
Abstract
To encourage buy-in and manage resistance, change managers utilize participatory strategies. This study examined the communication practices and perspectives of implementers and employees as they negotiated the change participation process to better understand resistance dynamics. Data were collected through interviews (n = 37) and observations (n = 2) with nurses and change implementers in a medical center. Grounded practical theory was used to reconstruct the stakeholders’ normative theories of participation in which multiple and often contradictory perspectives emerged. Asking employees to participate reduced implementers’ perceptions of control and increased their feelings of vulnerability. Implementers often equated participation with resistance and used different communication techniques to shape how nurses shared ideas, influencing their participation. Theoretically, this article adds to the study of participation and resistance by showing how resistance is constituted through communication by both implementers and change recipients as they attempt to navigate the inevitable contradictions that arise during the change process.
Introduction
Organizational change has become ubiquitous and is often framed in positive terms, as it is expected to offer competitive advantage and the ability for an organization to improve and maintain its position in the environment in which it functions (Lewis, 2019; Zorn et al., 1999). A common point of discussion in many change contexts centers on identifying the methods for successful change implementation for management (Tam, 1999), which often include offering employees the opportunity to participate by soliciting their feedback (Baker, 2007; Lewis, 2019; Sahay, 2021). Broadly speaking, successful change implementation is often evaluated from the perspective of management in terms of compliance with their original plans. This approach may, however, undervalue employees’ perspectives and their interaction with the change process, which can influence outcomes and have consequences for the organization (Jian, 2007; Lewis, 2019; Thomas et al., 2011). Therefore, it is important to understand how employees interact with the participatory processes during change, because their reactions and perspectives can influence the overall organizational climate and the success of the change (Lewis, 2019; Sahay, 2017).
Participation practices and techniques used during change may be selected based on change-specific needs and problems that implementers are trying to address, or they may be adopted simply because of best practices disseminated through the popular press and scholarly research (Lewis et al., 2006; Sahay & Dwyer, 2021). For example, soliciting input from nonmanagerial employees (Lewis, 2019) is common during change as a way to increase buy-in, curb resistance, reduce uncertainty, and help stakeholders such as employees feel included in the process (Bordia et al., 2004; Ford & Ford, 1995; Lewis, 2019). In prominent change management studies, participation is considered to be a beneficial strategy that reduces resistance to change (Giangreco & Peccei, 2005; Lines, 2004). Participation provides a sense of agency to employees or other stakeholders, thus making it easier for individuals to accept the change (Oreg et al., 2011).
However, as communication scholars have noted, effective participatory mechanisms can be difficult to implement and ultimately may be more peremptory than inclusive, depending on the implementers’ ideals about participation and their practical theories about how communication works (Aakhus, 2007; Sahay, 2021). Managing participation therefore requires confronting inherent contradictions and paradoxes; for example, empowerment-based strategies may, in fact, diminish participant agency and compel employees to follow dominant views (Stohl & Cheney, 2001). In this study, we explore how different stakeholders with different interpretive schemes navigate their participation through the evolving contradictions and paradoxes of change (Jian, 2007; Ford et al., 2008). Most notably we highlight how the participation interventions change managers design and implement to manage stakeholder resistance are viewed as a form of resistance by other stakeholder groups.
This study observed and explored the perspectives of nursing employees and change implementers in a medical center that was undergoing transformational change targeted toward nurses. The medical center was in the process of attaining an accreditation that is awarded to healthcare organizations that support nursing excellence (NE) (i.e., a culture that supports the contribution of nurses toward clinical research and leadership and motivates acquisition of advanced degrees). Such programs are often developed to make nursing work more equitable and to overcome the challenge of retention (Stimpfel et al., 2014). Participation, therefore, was an important strategy, as this change was based on the principle of shared governance (Stimpfel et al., 2014).
The study uses a grounded practical theory (GPT; Craig & Tracy, 1995; 2014) approach, which provides a metatheoretical lens for investigating communication practice through three interrelated theoretical levels—the problem level, the technical level, and the philosophical level. This approach enabled us to reconstruct member practices by identifying the contradictions, paradoxes, and dilemmas participants experienced (i.e., the problem space) and the communication techniques participants employed to manage these (i.e., technical aspect). We further explored the philosophical positions that guide these communication techniques for implementers and other employees (Ashcraft, 2000).
The theoretical contributions in this article highlight how ideologies around participation (i.e., what ought to be) can vary for different stakeholder groups. Communication techniques used to resolve implementers’ participation problems can generate a new problem space (i.e., paradoxes) for other stakeholders (i.e., employees and middle management) based on their ideals of participation. These ideals are motivated by different perceptions of vulnerabilities resulting in the emergence of resistance all around. This study demonstrates how resistance is emergent and fluid, constituted and negotiated through communication practice, not just an objective fact of change recipients’ behavior (Giangreco & Peccei, 2005; Lines, 2004). GPT analysis provides a more nuanced understanding of how participation and resistance are constituted through communication and interact in unanticipated ways due in large part to competing ideas around participation (Jian, 2007; Stohl & Cheney, 2001). Next, we review the literature on change, participation, and resistance.
Change Implementation and Participation
There exist widely propagated assumptions and advice concerning soliciting input during planned change initiatives for controlling resistance and increasing change implementation success (Bordia et al., 2004; Lewis et al., 2006). For example, Msweli-Mbanga and Potwana (2006) highlight the importance of individuals having access to participation (i.e., ability and opportunity to participate with appropriate information) and having some say in the decision-making during change efforts in order to reduce resistance. However, participation is a broad and indeterminate concept because the scope, form, and depth of participation differ across and within interventions (Abildgaard et al., 2018).
Not every intervention that is labeled participatory affords the same degree and type of participation. For instance, employees may have some influence over how a goal is achieved (i.e., the process) but not over the goal or content of the change itself. The type and form of representation matter, too, because individuals may be asked to participate directly or through appointed representatives, which may alter feelings of control and agency. The goal of participation is also important to consider; it may simply be to enhance the psychosocial work environment by helping employees feel involved, or it may be more holistic, such as establishing long-term participatory practices to genuinely create an inclusive workplace. However, as Aust et al. (2010) note in their analysis of an intervention process, stakeholders can have different implicit theories about how they define meaningful improvements to work environments, and this may create conflict that contributes to failed participatory interventions. These failures may be perceived to be a breach of psychological contracts, when employees believe that no remedial action is taken in response to their feedback during change (Harlos, 2001). This chain of events can cause greater frustration and damage perceptions of fairness.
While there are various perceived benefits of participation, there may also be inherent paradoxes that create tensions and contradictions arising from conflicts of ideas, principles, and actions, which organizational members must attempt to resolve (Stohl & Cheney, 2001). At times, the pursuit of one goal is undermined by the pursuit of another competing goal; this often occurs unintentionally but requires organizational members to confront the resulting problem space. These tensions, contradictions, and paradoxes have received considerable attention in the communication and change literature (Barge et al., 2008; Fairhurst et al., 2002; Stohl & Cheney, 2001). Paradoxes, in particular, are inherent to participatory designs due to factors associated with structure, agency, identity, and power. To name a few, the paradox of design (i.e., imposing mandates for empowering employees), the paradox of formalization (i.e., routinizing participation, which eliminates spontaneity), the paradox of representation (i.e., becoming co-opted by dominant interests), and the paradox of homogeneity (i.e., valuing agreement over disagreement while supporting diversity of opinion) are embedded in participation (Stohl & Cheney, 2001). Recent literature urges scholars to explore interactional foundations of paradox (i.e., how and why paradoxes are constructed in organizational interactions; Lempiälä et al., 2022). These tensions, contradictions, and paradoxes are a critical reality of organizational life; they influence how change is experienced (Fairhurst et al., 2002; Jian, 2007) and pave the way for unintended consequences (Jian, 2007) that can be expressed in the form of resistance and reactions from stakeholders.
Stakeholder Reactions and Resistance in Organizations
Stakeholder and employee reactions to change have been examined across literature in management, leadership, and communication (Lewis, 2019; Visagie & Steyn, 2011). In general, management and leadership literature centers around stakeholders’ commitment or resistance to change, change readiness, the fulfillment of personal values influencing employees’ commitment to change, and organizational benefits (Visagie & Steyn, 2011).
Resistance is often understood as a taken-for-granted consequence of power relationships in organizations (Mumby et al., 2017). Ironically, those who resist the rules and procedures that form the broad organizational structures are often complicit in recreating the very same structures they were opposing (Mumby et al., 2017). This perspective cautions us against oversimplifying resistance that treats employees as victims and management as perpetrators (Deetz, 2008). In fact, resistance has almost always been seen as a bottom-up concept, where employees resist the change implemented by management. However, scholars rarely discuss how management is also resistant to many things during change. A key observation from critiques regarding resistance is that it both challenges and reproduces power struggles (Mumby et al., 2017) and may be uniquely expressed by different stakeholder groups as they identify, negotiate, and advance their stakes in an attempt to maintain power. For instance, Thomas et al. (2011) discussed how senior management’s framing of change was often resisted by middle managers. And as Ford et al. (2008) note, “change agents contribute to the occurrence of resistance through their own actions and inactions” (p. 362).
Furthermore, literature on organizational resistance also considers different expressions of resistance (Dick, 2008), including sarcastic, cynical, or ironic communication or no response at all (Fleming & Spicer, 2008). Voice and silence are also closely tied to resistance, where voice is a choice employees make regarding communicating their ideas, suggestions, or concerns to improve organizational functioning, and silence suggests withholding those ideas (Morrison, 2011). Silence may also be viewed as a defensive measure used to avoid negative repercussions and provide self-protection (Van Dyne et al., 2003). Vulnerability and resistance often coexist, because feelings of vulnerability may motivate individuals to mobilize resistance efforts to oppose forms of power and control (Butler, 2016).
Critics suggest that resistance is typically examined as an independent event situated at one point in time rather than as a process that shifts as the change process unfolds (Erwin & Garman, 2010). Others have noted that there is a tendency to ignore how change agents view resistance as an objective truth and how they actually contribute to its existence (Ford et al., 2008). Furthermore, studies have not simultaneously accounted for both individual and social aspects of resistance (Erwin & Garman, 2010). Moreover, scholars have drawn an overly simplistic connection between resistance and participation, where participation is considered an acceptable solution to curb resistance; this is an area that requires further examination (Sahay, 2021). In exploring these gaps, greater insight into managing participation and understanding resistance will help develop an actionable knowledge base for change management.
With the above-citied literature in mind, the current study uses a GPT approach to reconstruct a normative theory of participation during a nurse-related change in a medical center by examining how participation techniques are selected, implemented, and responded to and the consequence thereof over the course of a change initiative. Our research questions are thus GPT-oriented:
Methodology
Introduction to the Case
This case investigated in this research involved a planned change initiative in a large suburban hospital with more than 850 staff registered nurses. The data presented here were part of a larger study examining a planned change initiative aimed at achieving the NE (pseudonym) accreditation, which would directly affect the day-to-day activity of nurses. NE is a prestigious designation awarded to healthcare systems that support NE and innovation through nurse empowerment.
According to the nursing literature, nurses face various obstacles at work (Sahay, 2021; Trinkoff et al., 2008) that contribute to increased nurse burnout and retention issues (Baker et al., 2007; Efendi et al., 2019; Trus et al., 2018). To enhance retention and empower nurses, several accreditation programs and initiatives have been developed. We studied the implementation of one such program that recognizes organizations that support nursing work, innovation, and patient care excellence. The journey to achieving these recognitions requires transformational changes, warranting time, awareness, knowledge exchange, and reinforcements by valuing nurses’ perspectives (Arthurs et al., 2018).
To be awarded these recognitions, healthcare organizations must demonstrate their commitment to cultural transformation by carrying out several activities. The NE accreditation consists of completing steps—including applying for the accreditation, documenting narratives and evidence supporting nurse innovations across medical center units, and planning for and undergoing the site visit by accreditors—before a final decision is made. The idea to seek the NE initiative in this organization was initially proposed by some nurses and was subsequently adopted by the organization.
The principal investigator entered the site when the organization was collecting narratives from different units to support the organization’s claims that it was an empowering workplace for nurses. These narratives identified innovative clinical work and involvement of nurses in important organizational activities. To document innovative practices and collect feedback from nurses about the change, the change implementers had created a steering committee. The NE accrediting body approved the documentation within a couple of months, at which point the hospital began to prepare for the final NE accreditor site visit. The principal investigator exited the field before the final decision of the NE accreditors was shared with the organization.
Study Participants
The study involved interviewing and observing individuals from three broad levels of the medical center who were directly affected by the change, including (1) executives and implementers (i.e., individuals responsible for implementing and managing the change); (2) steering committee members [SCMs] (i.e., nurses who were handpicked by their managers or those who volunteered to champion the change and collect feedback and narratives about the change from their units); and (3) frontline unit nurses [UNs] (i.e., stakeholders who were not directly responsible for the implementation even though it would impact their work). These SCMs and UNs held associate’s, bachelor’s, or more advanced degrees.
Sampling and Data Collection
The larger study adopted a mixed methods approach consisting of observations, semi-structured interviews, and a questionnaire. This article is based on the observational and semi-structured interview data. The principal investigator observed two steering committee meetings held in consecutive months and obtained access to the minutes of prior meetings. Semi-structured interviews were conducted with the five key implementers of this change and 32 nonmanagerial nurses (six SCMs and 26 UNs). Names of implementers (n = 5) were shared by the organization. The nurse participants were recruited from a list provided by the organization that contained names of prospective candidates (n = 14). These candidates helped recruit additional participants (n = 18) through snowball sampling.
Interviews began with the implementer, followed by the first observation of the first steering committee meeting, which was attended by both implementers and SCMs. After this observation, the principal investigator was able to conduct interviews with some SCMs and other nurses. Additional interviews were conducted through snowball sampling via phone calls later that month. The principal investigator then attended the second meeting, and more interviews followed that month.
Because these committee meetings were held once a month, the principal investigator was only able to attend two consecutively held meetings before the accreditor’s site visit. These two-hour meetings were attended by more than 20 SCMs and the implementers. The meetings consisted of updates on the change, discussions around challenges the units faced, concerns the nurses brought to light, talks regarding how implementers could support the effort, and information on next steps. SCMs and implementers sometimes discussed their perspectives regarding the meetings during the interviews that followed. The principal investigator attended these meetings as a nonparticipant observer and recorded jottings and preliminary field notes with a focus on how interactions unfolded. Field notes totaled about 24 pages and included both discrete moments and more in-depth descriptions of the attendees’ interactions. The field notes and jottings were continuously analyzed, and memos were developed by the principal investigator.
The interview protocol explored nurse perspectives regarding participation and voice in the change. Because GPT was used as the metatheory to analyze the data, the interview questions asked for both strategies and stakeholders’ accounts of those strategies. Most interviews ranged from 30 to 54 minutes and included one male and 36 females. All interviews were recorded with participants’ permission in accordance with our Institutional Review Board and were then transcribed.
Data Analysis
This analysis was informed by GPT (Craig, 2015; Craig & Tracy, 1995), which focuses on the beliefs and assumptions about what is deemed to be valuable and appropriate communication (Craig & Tracy, 2014). This approach highlights how underlying ideas and principles regarding communication practices such as participation or input solicitation are constituted through discursive strategies, creating conditions for stakeholders and implementers who must negotiate their responses.
Coding Example.
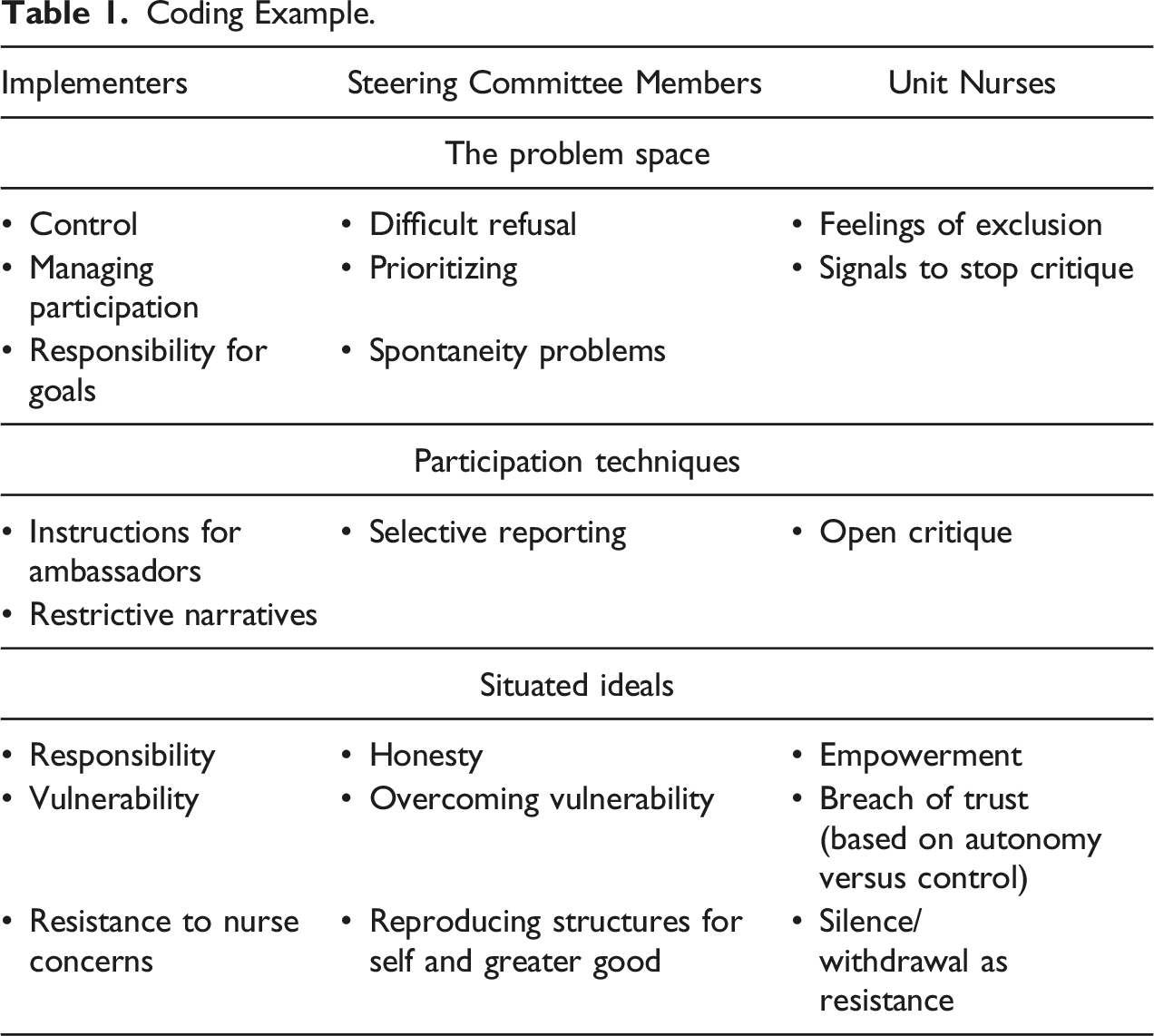
The next round of data analysis consisted of more focused coding; the principal investigator and the co-author focused on identifying techniques used by different stakeholder groups. For instance, SCMs often discussed their approach of reserving “full concerns” or sharing “limited issues,” which was labeled a technique of “selective reporting” through which members would share some concerns but not others to appease implementers.
In the third round of coding, the principal investigator and the co-author specifically explored the situated ideals in greater detail and made connections through a constant comparative method (Glaser & Strauss, 1967) in which incidents were compared for similarities and differences in and across interviews (Corbin & Strauss, 2008). This also helped us connect ideals to the techniques used. For instance, we noted that those nurses who were exiting the organization decided to speak up for several reasons, including the fact that they had nothing to lose, or they were setting examples for others to follow; both of these reasons established the importance of empowerment for nurses and their frustrations with the system. A final round of coding helped to refine our ideas during the revision process of this article.
Findings and Interpretations
This section first focuses on identifying the multifaceted problem space around change participation that emerged in part from the inherent dilemmas associated with participation. We then discuss the strategies and communication techniques these stakeholders employed to navigate the problem space. These communicative techniques often emerged as unplanned consequences based on the situated ideals change implementers and stakeholders held regarding change, participation, and culture. In the following discussion, implementers are designated as (I), SCMs as (SC), and unit nurses as (UN).
The Problem Space—Contradictions and Paradoxes Around Participation
In general, implementers spoke about participation being essential for managing the change process, as it would signal the required involvement of nurses in this process. This change was meant to empower nurses, “and thus it was important to hear from them about what they thought about it” (I1). At the same time, however, implementers had to follow rules set by the external accreditors, which required them to design the change process in particular ways. As one implementer posited, “we had to follow the rules and manage this change. While participation was necessary for the change, there was so much that could not change” (I2). Therefore, according to the implementers, the rules around this accreditation program did not afford any flexibility to modify the change based on nurses’ feedback. Subsequently, SCMs and UNs had less influence on the content of the change. Participation presented the main contradiction for implementers, as one implementer described: “sometimes it is like walking this weird line, if you listen to everyone, then you are giving up your control, and this was our job to get the accreditation, so we had to be in control” (I3). Implementers spoke about this contradiction in which including employee voices could lead to reduced control for the implementers, who would struggle to implement the change they were tasked with. This inevitable redistribution of power was problematic for the implementers.
Implementers created a steering committee to respond to questions, control negative feedback, and educate the nurses about the program; it was hoped that this committee would prepare the organization for the site visit. As noted by one implementer, the steering committee offered a sense of “shared governance.” She added, “we were also collecting feedback on what was not working and used that to provide more information to help clarify the doubts” (I1). Therefore, while the steering committee was formed to offer representative participation to individuals, implementers established various techniques to ensure that they were able to control the change and see it through.
The role of the steering committee was shaped by the implementers’ perspectives regarding participation and the contradictions they felt. The SCMs were asked to collect feedback from their units, share it with the implementers, and bring the information from the monthly steering committee meetings regarding the initiative back to their units. As one SCM posited, “our job was to include our units, and since we have to be ambassadors of this change, I am positive about this program. But not everyone understands that or is happy about it” (SC5). The SCMs, too, were left in an “uncomfortable space sometimes, where I was tasked with collecting feedback and informing my unit, but I couldn’t always take the issues back to the meetings because ultimately we were responsible for the change” (SC4). The contradictions implementers felt were, in a sense, transferred to these SCMs and even amplified by their roles as middle managers trying to mediate the participatory space for the implementers and the UNs. Within the larger participatory problem space, SCMs were faced with two distinct paradoxes: one in which they could not refuse their selection to the committee, as they were sometimes handpicked by their managers (i.e., the paradox of design), and another where the SCMs’ interest in supporting their UNs was overshadowed by the interest of the implementers, which was to wield control to ensure the change was implemented as defined by the program (i.e., the paradox of responsibility; Stohl & Cheney, 2001). As this SCM commented, “I just had to say yes because my manager had asked me and also because it was about empowering us” (SC6). Another member said, “My manager had trusted me with this. … I understand the value of participation, but I also realized that they [implementers] were not looking for negative information” (SC4). These quotations delineate the paradoxes that were part of steering committee participation, especially those associated with member selection and the expectations to conduct participation in specific and restrictive ways.
There were other committee members who had volunteered to be part of this committee because they wanted to “move up the ladder,” but they, too, understood the dilemmas associated with balancing the nurses’ voices with following the rules set by the implementers: “It is just expected that we ensure that this change happens. When I see how it [implementation] is being done. It can be difficult, when nurses tell you it is not working for them” (SC3). This excerpt reflects how rules around participation were not always codified but were implied through different communication techniques; this will be discussed later.
In general, UNs believed that their “feedback could be used to make knowledgeable efforts in modifying the course of the change” (UN4). They believed that they should have a say in the content and process of the change as they understood the day-to-day obligations and identified several problems associated with the change that should be addressed: “We have other issues that need our attention and resources, and to add to those expectations by expecting us to follow the [NE] level of work requires a conversation that we are missing” (UN2). However, given the participatory strategies and techniques implemented by the organization and the general inequity of voice in nursing work, they also understood that these structures of participation were there primarily to control the conversations. As one nurse points out, “this is nursing work. We don’t get to speak up, but we need to. They will get feedback from us but then you know the intentions behind when they use particular strategies” (UN6). Therefore, design contradictions resulted when nurses recognized that their feedback was important but their nursing work experiences and the current process felt inauthentic, leaving them feeling vulnerable, thus influencing their willingness to provide feedback. As one nurse posited, “I can give you my feedback, but then if you don’t do anything with it, or see me as a cynic, then I feel even more exposed” (UN16). Through their past and current experiences in which management failed to take remedial action in response to nurses’ concerns about the change or other matters, nurses were hesitant to provide feedback, even though they recognized it was important. Therefore, the contradictions and paradoxes shaping the management’s and SCM’s strategies created the conditions for nurses to also experience contradictions regarding participation.
Additionally, the lack of clear criteria regarding how committee members were chosen signaled to the nurses that meaningful participation would not be possible. One nurse spoke about the importance of participating in changes relevant to them, which was essentially “the tagline of the [NE] program, but the way this [steering] committee was selected and how it did not really take our concerns seriously, showed us that we were not valued” (UN4). This inclusion-exclusion tension created an additional contradiction for nurses.
The Technical Level—Navigating Participation
We next identify how stakeholders navigated participation and managed the problem space through the use of various communicative techniques. Sometimes these techniques emerged as unintended consequences and exacerbated the contradictions each group was facing.
Beginning with the implementers, while the formation of the steering committee was a strategy used to solicit feedback and educate units, implementers used communication techniques to establish control. As discussed earlier, the selection technique for the committee was based on recruiting either those handpicked by their unit managers or those who wanted to advance their careers in management. As one implementer explained, “it was important to have representatives who understood the management views, which would make it easier for us to translate the NE’s expectation” (I2). Those who closely aligned themselves with management would likely show less resistance, accept expectations, and follow rules.
While the selection process was one technique, there were other communication techniques that signaled control and helped the implementers set participatory boundaries. These included developing a grand narrative around what it meant to be an ambassador of the change, selectively responding to comments, setting a rigid agenda for steering committee meetings, regulating turn-taking, asking members to find their own solutions, making light of difficult issues, and, importantly, evading questions regarding resistance.
Developing a Grand Narrative of Ambassadorship
The implementers developed grand narratives around what it meant to be SCMs. Implementers used words like “bridge” and “bonding” along with “credibility” to describe the ideal SCM. This implied that “nurses could approach their representatives to talk about the NE initiative” (I2), but it also meant “they did not have to come to us [implementers] directly” (I3). Implementers organized kickoff events and discussed the role of representatives in aiding their units in “bridging the knowledge gap related to the NE initiative” (I2). But this grand narrative magnified the distance between the nurses and the implementers, making implementers appear unapproachable. It also generated expectations around what SCMs were supposed to do: “they were drivers of this initiative who had to convince their units this change was good for them” (I1). Therefore, this discursive technique had implications for both nurses and SCMs.
Selective Listening
Implementers spoke about the role of the steering committee as “collecting and bringing most frequently discussed concerns to us” (I1). Implementers used these comments to create a “Mythbuster” campaign, yet, as they suggested, “it was helpful to hear about the frequent issues, but of course we can’t make everyone happy and not every comment will have value, so the steering committee can help us sift through this” (I4). Therefore, the steering committee helped to filter out some comments and create the Mythbuster fact sheet to address only the most common concerns. However, this also meant that some of the nurses’ concerns were filtered out in the process.
Rigid Meetings and Regulated Turn-Taking
A meeting agenda was always sent out before the tightly-run steering committee meetings. As one implementer explained, “we always provide an agenda a few days in advance. It helps us keep focused on how to move forward” (I2). This left little room for discussion beyond the specified topics. During the observations, it was noted that the steering committee meetings were strictly conducted with regulated turn-taking, thereby making it a restrictive participatory technique. For instance, implementers would ask the members to talk for a limited time in small breakout groups about new ways of educating nurses. This enabled implementers to maintain power and control, thus illustrating the paradox of formalization (Stohl & Cheney, 2001), which detracts from genuineness and spontaneity.
Finding Your Own Solutions
In a handful of cases when SCMs or breakout groups reported on a problem during the meeting, implementers would respond by telling them to “come up with their own creative solutions” (I2). This response dampened participation, as one SCM noted how this technique affected “any honest conversation around the real issues present here” (SC3), again highlighting the paradox of formalization.
Making Light of a Situation
Making light of the difficulties associated with imparting program-specific knowledge was observed during a discussion between the implementers and the SCMs regarding a “Flashcard Campaign.” During this steering committee meeting, implementers opened the floor to committee members, asking their opinions on how they might educate the UNs about relevant content prior to the site visit. The SCMs suggested creating flashcards held on a ring that nurses could easily flip through during huddles (i.e., brief meetings held at shift changes to transfer patient information to incoming nurses) and breaks. An implementer agreed that this was a practical way to gain attention, adding, “we can also, say, dress up like clowns during the socials and start quizzing random people.” Power differentials were maintained through these proposed strategies (i.e., quizzing nurses), which sometimes made SCMs feel devalued. As one member commented, “at least it was an innovative idea that would work for our units, but I don’t want to play a clown” (SC5).
Denying Resistance
When asked about current resistance in the organization, implementers often denied its existence or deflected the topic. For example, when asked about resistance they had encountered leading up to the change, one implementer responded: “I guess we haven’t encountered something like that yet” (I2). Implementers failed to see the value of oppositional voices—in fact some even denied their existence—while still supporting the NE initiative that valued diversity of opinions. Additionally, implementers rationalized nurses’ negative feedback by denying personal responsibility for the consequences of the change, as illustrated by this implementer’s statement: “I am essentially helping conduct this change and was primarily expected to do this. Deciding whether we need this or not is not my responsibility” (I4).
Most SCMs followed the practices established by the implementers but altered them slightly. For example, they edited the nurses’ feedback by taking only selective concerns directly to the implementers. Many SCMs chose to protect the confidentiality of their unit members because they recognized the contradictions around participation emerging from how implementers conducted the meetings. Finally, many members used the brief huddle meetings with nurses to share knowledge from steering committee meetings or to solicit additional feedback as a way to limit discussion, enabling them to report to the implementers that there was no discernable resistance.
Selective Reporting
SCMs often spoke about how they did not always convey the full details of a nurse’s concern because it would hurt the change process and their standing as an ambassador, which highlights the paradox of responsibility. As one nurse explained: I think there is a general understanding between us [reps], we don’t always have to get the full concern to the [name of the executive]. … I did tell them [implementers] about the issue [brought up by the nurse] but kept out the emotions. I think they too understand this … she said we have to make these hard choices. (SC3)
This SCM understood that there were difficult choices to be made and downplayed the UNs’ concerns using a selective reporting technique that omitted emotions to share an acceptable version of the concern with the implementer.
Preserving Confidentiality
Almost every SCM spoke about the importance of protecting the confidentiality of UNs who shared feedback with them. Preserving confidentiality was a communication technique that did two things: first, it protected the nurse who shared a critique; and second, it made the concerns less likely to be taken seriously by implementers because no names were attached to them. For instance, one SCM noted: “We just have to see this change through, so I am hesitant to share names [of colleagues]. I think the higher ups are also happier because they are not answerable to a person they don’t know” (SC5).
Selection of Restrictive Channels
While the change initiative was supposed to embrace a shared governance approach, SCMs utilized top-down restricted channels of communication to limit listening. In fact, some SCMs mimicked the implementers’ techniques that generated contradictions. For example, one steering committee nurse said, “yes, I inform my unit and keep it short and formal, like our monthly meetings, because again not much can be done, so this works” (SC5). This restrictive participation spread to others, with some SCMs adopting the same approach. Even though they recognized that this behavior did not enable genuine participation, it was nonetheless deemed appropriate for this situation, thus magnifying the problem space. Others spoke about using “huddles to give quick updates” about the change, which did not leave any time for questions and answers (SC3, SC4). Therefore, during the huddles, “the focus was on changing hands, discussing what the patient needs were, and not as per se the issues about the change” (SC1). Using this time to solicit feedback about the change trivialized any concerns nurses had. Nurses also reflected on being asked to provide feedback in hurried instances like huddles, stating, “These huddles are short. … I don’t think our committee members have time to listen to the negatives, so I let it be” (UN18). Thus, how participation was conducted created doubt and caused frustration and potential resistance. UNs experienced these contradictions and selected techniques as a response to how participation was conducted and the culture at large “that was not open to voice” (UN5).
Open Critique
Not all nurses reacted in the same way. Some, especially those who were going to exit the organization soon due to retirement or job change, were more forthcoming about their perspectives and more openly critiqued the change. As one nurse posited, “I spoke up in the townhall meeting … It was in front of the CNO and everyone else. I told them this was not the right time, and building this steering committee was not helpful … ” (UN4). Nurses who had less to lose recognized the value of providing feedback and openly critiqued the change and the way participation was handled.
Withdrawal and Silence
In some cases, nurses censored their feedback as they realized that their input would not influence the process. Subsequently, many of the nurses resorted to withdrawal and silence as communicative techniques to navigate their participation. Many UNs came to believe that providing feedback was a “waste of time” (UN18), because any substantial input provided was not used or addressed, and because the participation strategies offered seemed inauthentic. As one nurse questioned, “what is the point of speaking up if they don’t listen?” (UN14). Another commented, “maybe if I stopped saying things, they would actually wonder why and try to listen” (UN10), thus highlighting how silence can be a form of resistance. Nurses also chose silence in response to the SCMs’ enthusiasm for the change. As one nurse explained, “our rep only had positive answers and it became difficult to approach her with any questions” (UN3). Moreover, nurses spoke about how not being permitted to speak directly to the implementers negatively affected the culture further. For example, one nurse stated: “That shows the level of trust they have in us or how we have been distanced from the real effort” (UN8). Thus, these nurses viewed the restrictive communication techniques and the steering committee as detrimental for developing an open culture.
Situated Ideals: The Rationale Behind Using Techniques
Next, we turn to the situated ideals that were implied in these efforts to manage the contradictions. Importantly, these represent the underlying philosophy that each group contemplated as they used specific techniques and reflected on the reasons for doing so. This section also establishes how situated ideals do not exist in isolation but rather are often discussed and transferred between individuals, who individually and collectively navigate the problem space.
For the implementers, the situated ideal was a belief that they should be in control of the change and that to do so they must control any negative voices. However, because implementers were expected to provide participation as indicated by the shared governance model, they felt vulnerable to losing their power and control over the change and the implementation process. Nevertheless, some also recognized they had some privilege in that vulnerability, stating “we had the power to control how vulnerable we would allow ourselves to become” (I1). This may be why many implementers denied the existence of resistance as a way to avoid any negative information that might derail their effort and prevent them from fully controlling the situation. As one implementer noted, “changes will leave some people unhappy or resistant, so we can’t address every concern” (I2). Therefore, nurses’ concerns were viewed as resistance that could be overlooked to maintain control, which led to the development of restrictive techniques.
Many SCMs were either invested in climbing the ladder or pleasing their managers, as they had been handpicked by those managers. In either situation, the prominent ideology that guided their stance was, “Nurses have been in this powerless situation for a long time, and for us to get out of this, we have to grow. I can only get myself out and set examples for others” (SC2). Thus, the SCMs often reproduced the unequal systems of which they were a part in order to establish themselves and move out of those vulnerable positions of uneven power dynamics. To overcome feelings of vulnerability, they justified reproducing inequities in the short term for an imagined greater good in the long term. However, they modified the participation techniques used by implementers to create more realistic expectations for their nurses. As one SCM pointed out: They [my UNs] fully support me, but we all know in order to live in the system we have to do what we are asked to do, but we can always change it up a little bit, like anonymize names or not waste my nurses’ time if I am honestly not going to take their feedback. (SC6)
Thus, this SCM discussed the importance of and reproduction of rules but with modifications. By tweaking the techniques, she could set realistic expectations for nurses, creating a more authentic way to conduct limited participation. As another SCM noted, “I think honesty goes a long way” (SC3). This nurse chose to tell her UNs about the restricted participation technique, thus setting a realistic expectation and increasing the trust her nurses had for her.
UNs, those who participated and those who held back, had similar situated ideals, believing that “nurses needed to be empowered, but the culture underlined the existing issues with control” (UN2). One nurse spoke about how the participatory tools used had enabled her to see the contradictions more clearly: “Would it have been an issue if you had not made so much rah rah about [how] we need you to participate? No. But now, I pay attention to what that committee does and it doesn’t look like participation” (UN12). As this nurse suggests, showcasing participation backfired and instead attracted greater scrutiny. The very talk of participation and the techniques used instead accentuated the inauthentic approach, thus highlighting the contradiction between autonomy and control. As one nurse posited, “They wanted me to believe I had power, but they were controlling it for me.” She added, “it is like a breach of trust when you do that” (UN8). Therefore, psychological contracts played an important role here as nurses felt that their trust was breached, and they perceived the system to be unjust as they were promised things that never materialized.
Nurses spoke informally about their communication techniques with other nurses. For instance, as one nurse explained: She (my colleague) asked me what I thought about the NE program, and I had given my feedback to my unit [rep], but they made a FAQ [“Mythbuster”] from this. My friend was like, I knew this was going to happen from the very beginning. … Anyway, I was already upset … and talking to my friend made me realize how important it was to withdraw from this, hopefully show our discontentment. (UN21)
As illustrated here, resistance did not emerge as a concrete consequence of an event gone wrong; rather, it emerged sequentially as individuals reacted to techniques and shared their opinions with others who experienced similar issues. Resistance efforts became more prominent as time passed: “Just throughout the process things were not fair, I know me and other girls in the unit, we don’t even react anymore [regarding the NE initiative]” (UN20). This reveals how resistance and silence were intertwined and how resistance grew as trust was broken.
Only the nurses who were planning to quit or retire from the organization spoke out, even if they were not being heard: “I have given 30 years and I want to leave behind a legacy where nurses know they can stand up for themselves … We cannot be vulnerable anymore” (UN22).
In summary, resistance did not form in the aftermath of a singular event but emerged over time as individuals navigated the problem space and coped with contradictions that created perceptions of injustice. These perceived injustices were often the difference between what is and what ought to be, fueled by the inherent contradictions associated with participation that can influence how vulnerable one feels. Resistance was assumed to be a natural part of participation and expanded through informal networks as individuals discussed their experiences and techniques with others. Importantly, however, implementers also resisted, choosing not to see the resistance of SCMs and UNs to minimize the implementers’ vulnerabilities.
Discussion
This study makes key theoretical contributions to organizational communication in relation to participation and resistance during organizational change. The GPT analysis helped us reconstruct a normative theory of participation and resistance by shedding light on paradoxes that emerged during the participatory process. It highlights the complicated relationship between problem spaces, situated ideals, and techniques, where management of a problem space by one stakeholder group using a particular communicative technique can generate new problem spaces (i.e., paradoxes) for other groups (see Figure 1; Giangreco & Peccei, 2005; Oreg et al., 2011). These paradoxes and contradictions are unintended consequences of managing participation (Jian, 2007). Example of relationship between problem space, techniques, and situated ideals.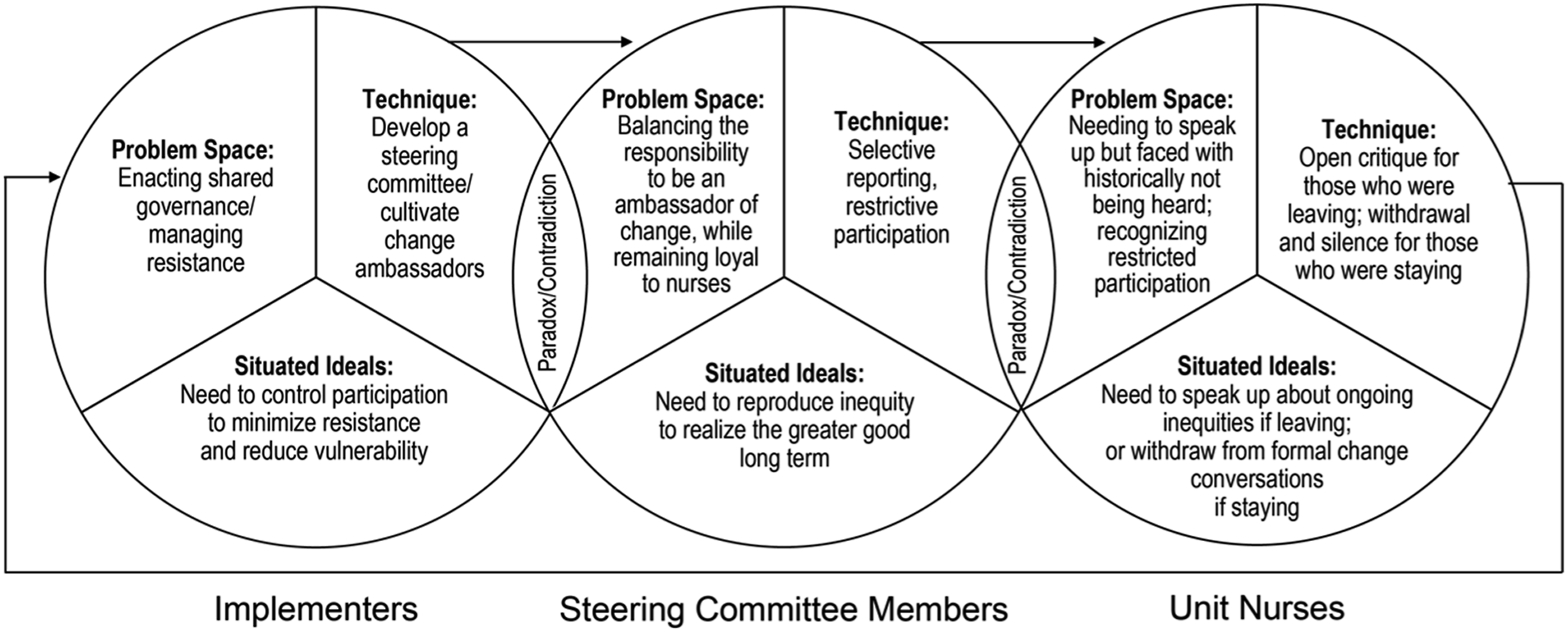
First, this study helps us unpack the nuances between participation and resistance and signals that resistance occurs at all levels and is interactional in nature (Ford et al., 2008; Lempiälä et al., 2022; Thomas et al., 2011). Resistance is constituted through communication as both implementers and employees (i.e., participants) construct and negotiate the meaning of participation that is embedded in their ideals of participation (i.e., what ought to be) (Aust et al., 2010) that are often motivated by their vulnerability (Butler, 2016). For instance, implementers used certain techniques of participation to maintain their control over the change process because they felt vulnerable to losing that control. In doing so, they limited the very meaning of participation, and viewed concerns and questions that did not fit their definition of participation as concerns that needed to be curbed. The findings have thus helped us unpack the complex relationship between participation, paradoxes, vulnerability, and resistance. When participation is planned with certain goals in mind (i.e., to limit one’s vulnerability), the specific techniques used to meet those goals can create and signal resistance toward valid employee feedback, the very thing it sought to support. This could breach employees’ psychological contract and trust in their organization (Aust et al., 2010), generating greater resistance from the employees toward their management’s practices. Employees may respond by resisting in specific ways or by withdrawing their participation. This paints a complex picture of resistance in which resistance is no longer a bottom-up concept and can be started by implementers themselves. Employees evaluate and interact with individuals and restrictive participatory mechanisms that can further generate a chain reaction of resistance at multiple levels, especially as employees navigate their participation.
Second, it is important to note that resistance emerges throughout the change process, especially as the change progresses; therefore, resistance is not the result of a single event and is quite emergent in nature (Erwin & Garman, 2010). Resistance, whether it is toward employee concerns or is a reaction by the employees toward their implementer’s management of change, emerges in the change process. The findings thus suggest a revised theory of participation and resistance grounded in the idea of shifting paradoxes. The findings suggest that paradoxes embedded in participatory practices are not concrete or situated and that (a) different stakeholders perceive these paradoxes differently; (b) these paradoxes and contradictions motivate conversations about the problematic participatory space; and (c) through the interactions, the meanings assigned to these paradoxes and contradictions change. This paves the way for emergent resistance as individuals adopt different strategies to navigate and/or challenge their perceptions of management’s ideals and reasons for offering participation and vice versa. Therefore, resistance and perceptions of resistance are not fixed concepts and change over the course of the change.
A third and final theoretical implication involves interventions or programs that promise empowerment to employees. As investigated by Aust et al. (2010), these programs can actually fail to fulfill promises made to the employees for a number of reasons including increased pressure on employees to change, unsuccessful coaching, unrealistic expectations from leadership, or simply having different meanings of what it takes to change. In the change considered here, participation meant very different things for the different groups. Stakeholders had to be very strategic about how they labeled and managed resistance (Ford et al., 2008). For a program that was promising hospital-wide nurse empowerment, the restricted participatory efforts countered the main ideology of the change (Abildgaard et al., 2018). This makes us question whether programs that promise their employees empowerment, such as the NE accreditation, are at best superficial because the implementation is often highly structured and limits participation. Does the way such programs ritualize participation only use it as a tool to achieve the end goal of conferring accreditation, which then becomes its own paradox?
Practical Implications
For change programs implemented to empower employees, such as nurses who suffer inequities (Baker et al., 2007; Efendi et al., 2019; Trus et al., 2018), or organizations that are attempting to improve the employee experience and management quality more generally, it is important to recognize the differences between what such change initiatives require and how changes are implemented. And while there can be no set or prescriptive formula because every organization is different, our findings highlight the need for change implementers to be attentive to how their own behaviors during the change process may resemble resistance. Additionally, implementers must consider how participation may fit with a particular organization by first understanding the perspectives and ideals of those at the receiving end of the change and plan the change and participatory processes accordingly. Implementers should not interpret silence as acceptance of change; and, if they wish to have a real picture of the situation, should make an effort to listen to the critiques.
Most important, the analysis helps us to propose techniques that can contribute to successful participatory efforts. These include working to create an open culture that cannot be developed over the course of one change event and must be developed long before the change process begins. However, even during the change process, implementers can adopt techniques that engender trust and honesty, as in this case when the nurses appreciated steering committee efforts to be honest about the restricted participation. Having empathy for peers and coworkers can help develop a culture in which a candid approach toward what individuals can expect from their participation may help to develop trust in relationships and mitigate negative impressions of the organization. Managers must avoid making promises that will set unrealistic expectations that can cause psychological breaches (Harlos, 2001).
Limitations and Future Research
A limitation of this study is that the original list of prospective participants for the interview was provided by the organization; therefore, it may have come with some selection bias. However, additional interviews were conducted through snowball sampling along with observations to overcome this limitation. Second, during our analysis, it sometimes became difficult to separate the change-related experiences from broader conversations about the organization’s culture, past experiences, and the overall assumptions around the nurses’ work and occupation. We believe that these experiences, which consist of intersecting identities, learning, and sensemaking, shape the understanding of communication strategies. Future studies can focus on exploring how these experiences help create an understanding of what these strategies should be. Moreover, studies can add to the application of GPT analysis, to further explore how current strategies used for resolving problem spaces can shape future problem spaces in changes that are conflicted or generate contradictions.
Conclusion
This study explored participation during an organizational change initiative in which there were multiple problem spaces associated with participation that implementers and employees attempted to resolve. Implementers and employees used different communication techniques informed by their ideals and also reflected on others’ strategies as creating challenges for participation. Implementers faced the contradictions of providing participation to empower employees consistent with the change, but also struggled to educate nurses about the change while controlling resistance. The steering committee was caught between loyalty for the change effort and the concerns posed by their unit members. UNs wanted to provide their feedback, which they felt was essential for this change, but understood that the strategies provided by implementers were too restrictive for authentic participation. This shifted the focus from the change to the participatory mechanisms or communication techniques provided by the implementers.
This study explains that the relationship between participation, vulnerability, and resistance is quite complex. Participation does not always quell resistance during change; rather, participation can be construed as resistance by those who do not want to give up their status quo. Resistance emerges in relation to how techniques of participation are negotiated over the course of the change.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.