
Abstract
Introduction:
Pediatric kidney stone disease is on the rise, and high recurrence rates necessitate consistent postoperative follow-up. Identifying social determinants of health is a key step in understanding the factors that influence adherence to follow-up after operation. This study examines socioeconomic associations with adherence after kidney stone procedure in children and evaluates whether enrollment in a multi-center clinical incentivized trial was associated with adherence. We hypothesize that those who lived farther from our hospital, lived in areas of higher deprivation, or were not enrolled in the trial were less likely to follow-up.
Methods:
We conducted a retrospective review of patients under 18 years old who underwent kidney stone operation from August 2019 to July 2023. Demographics, medical history, Area Deprivation Index (ADI) scores, and surgical details were analyzed. The primary outcome was follow-up clinic attendance within 16 weeks postoperation. ADI was calculated using patient home address to rank against other neighborhoods in the United States. Higher ADI score indicates more socioeconomic disadvantage. Variables were analyzed using chi-square tests for categorical variables and independent t-tests for continuous variables.
Results:
A total of 120 patients were identified: predominantly female (75/120, 62.5%), White (102/120, 85.0%), with median age of 15.7 years (interquartile range 11.5–17.2). Median travel distance to hospital was 51.0 miles. Of the 120 patients, 66 (55.0%) followed up within 16 weeks. Adherence was higher among patients with private insurance (p = 0.03) and lower ADI scores (less neighborhood-level deprivation) (p < 0.01). Prior surgical stone removal was also associated with lower adherence (p < 0.01). Enrollment in a clinical trial did not significantly impact imaging adherence (p = 0.98).
Conclusion:
Private insurance and lower ADI scores were associated with improved follow-up adherence, emphasizing the association of socioeconomic factors with adherence after kidney stone procedure. Clinical trial enrollment did not affect follow-up adherence, suggesting a need for targeted strategies to support high-risk pediatric patients.
Keywords
Introduction
The incidence of pediatric kidney stone disease is increasing, posing significant challenges for patients, families, and health care systems.1,2 For patients who have already had a kidney stone necessitating operation, major goals of postoperative follow-up include identifying residual stone burden that may result in future symptomatic events, ruling out postoperative complications such as “silent” hydronephrosis on postoperative imaging, and initiating kidney stone prevention counseling. Therefore, understanding drivers influencing adherence to care after stone operation can guide efforts to reduce risk of recurrence and additional procedure.
This study examines associations between various socioeconomic and clinical factors with adherence after kidney stone operation. Utilizing the Area Deprivation Index (ADI), this study seeks to better understand the impact of social determinants on adherence. In addition, this study evaluates the influence of enrollment in the Pediatric KIDney Stone (PKIDS) Care Improvement Network, a clinical trial created to study the comparative effectiveness of surgical interventions in kidney stone disease. 3 As PKIDS provided participants with structured reminders, research coordination, and financial compensation for participation, it offered a real-world model to examine whether such systems might improve adherence. We hypothesize that patients from disadvantaged backgrounds exhibit lower adherence and that adherence to postoperative follow-up care is associated with socioeconomic factors, such as insurance and ADI. In addition, we hypothesize that PKIDS trial enrollment is positively associated with imaging adherence.
Materials and Methods
Study design and population
This was a retrospective cohort study of patients less than 18 years who underwent surgical kidney stone removal at our tertiary pediatric hospital from August 2019 to July 2023 (IRB# X160923001). Patients were identified using operating room schedules and Current Procedural Terminology codes. We only included patients who underwent ureteroscopy with stone extraction and/or lithotripsy and percutaneous nephrolithotomy. There were no specific exclusion criteria; patients with complex medical comorbidities (e.g., spina bifida, anorectal malformations) were included to preserve generalizability and avoid artificially narrowing the study cohort.
Variables
Covariates analyzed for their association with adherence included medical history, socioeconomic factors, and surgical characteristics. Demographics included sex, race, ethnicity, age, and distance to the hospital. Medical history included previous stone diagnoses, prior surgical stone surgeries, and insurance status. Presentation characteristics included intervention type and whether multistage surgeries were required. Socioeconomic factors were assessed using insurance and single- vs dual-parent household status, which was obtained from clinic intake forms. Distance to hospital was calculated using the patient’s home address to the location of scheduled postoperative visit on Google Maps. We excluded all patients who had a telehealth visit from distance analysis.
ADI, a validated tool based on 17 U.S. Census variables, including education, income, employment, and housing characteristics, was used to evaluate socioeconomic challenges.4,5 Each patient’s ADI national percentile was calculated at the census tract level based on home address, with one representing the least disadvantaged and 100 the most disadvantaged. ADI reflects broader community-level socioeconomic disadvantage, offering a standardized way to quantify the socioeconomic context of a patient’s living environment. 6
Enrollment in the PKIDS clinical trial and postoperative imaging acquisition
The PKIDS Care Improvement Network is a multi-institutional initiative aimed at improving the care of children and adolescents with kidney stone disease. 3 Our hospital joined PKIDS in January 2021. The PKIDS protocol also specified for postoperative imaging within 16 weeks after operation. Enrolled patients were compensated for completing patient-related outcomes questionnaires, not specifically for adherence to postoperative follow-up or imaging. There were no penalties for nonadherence. Reminder mechanisms included scheduled phone calls coordinated by a dedicated research coordinator who was responsible for tracking adherence and acted as liaison for the patients.
Patients who participated in the PKIDS trial were identified through the trial enrollment log, whereas patients who did not participate in the trial were identified using operating room schedules from the same time period. The non-PKIDS cohort was composed of patients who did not want to participate in PKIDS, were not screened, or did not meet the inclusion criteria.
Outcomes and statistical analysis
The primary outcome was patient adherence to care within 16 weeks after stone operation, defined as completing a follow-up visit with postoperative imaging 110 days postprocedure. Patients were considered adherent if they completed at least one postoperative urology clinic visit within this 16-week window, regardless of whether additional follow-ups were recommended. For patients undergoing multistage operation, 16 weeks were measured from the final procedure.
In addition, we investigated the influence of PKIDS clinical trial enrollment on adherence to imaging acquisition within 16 weeks, comparing adherence and characteristics between PKIDS and non-PKIDS participants.
Pearson’s chi-square test and Fisher’s exact test were used for categorical variables, whereas the Mann–Whitney U test and independent t-test were applied to continuous variables, as appropriate. All statistical analyses were performed using IBM SPSS version 29.0.1.1, with significance set at p < 0.05.
Results
Patient population
A total of 120 patients were included, with patient demographics displayed in Table 1. The patients were predominantly female (75/120, 62.5%) with a median age of 15.7 years (interquartile range [IQR]: 11.5–17.2). Most patients were White (102/120, 85.0%), and 3.3% (4/120) were Hispanic/Latino. The median travel distance was 51.0 miles (IQR: 19.4–93.7).
Characteristics of Study Population (n = 120)
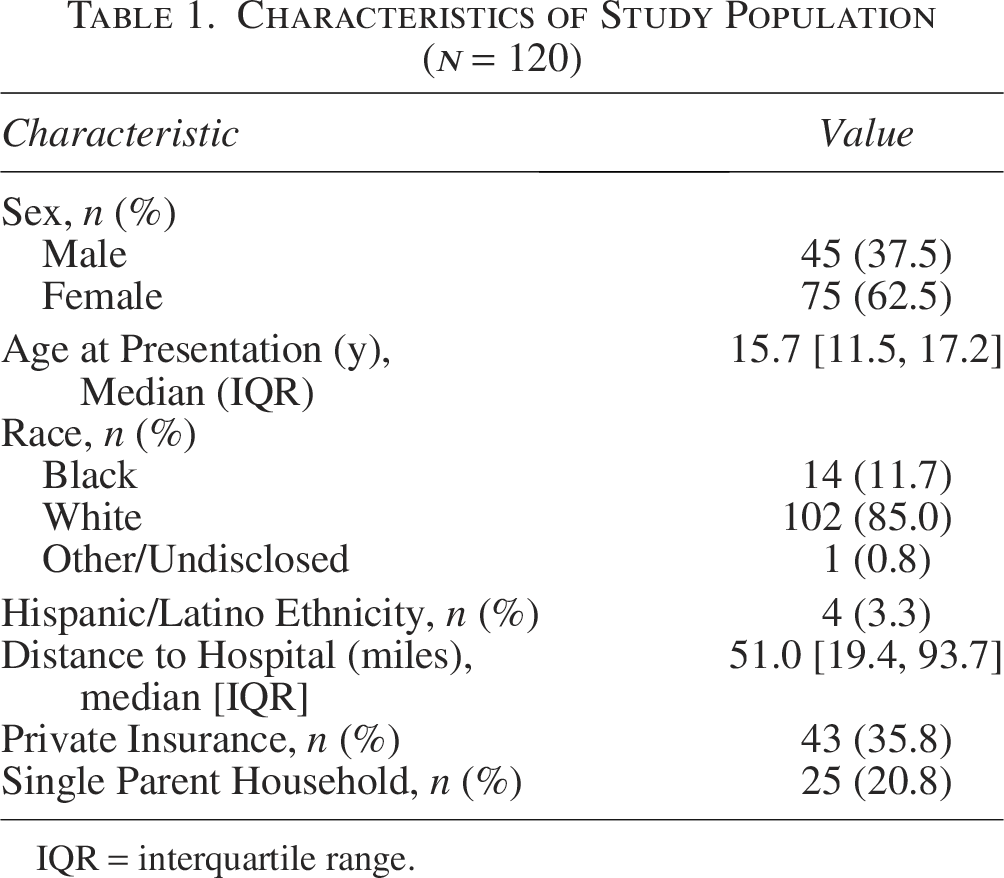
IQR = interquartile range.
Factors associated with adherence to postoperative follow-up
There were 66/120 (55.0%) patients who were adherent compared with 54/120 (45.0%) who were not adherent to clinic follow-up visit within 16 weeks of procedure (Table 2). Nonadherent patients (12/54, 22.2%) were statistically more likely to have had a prior stone removal compared with adherent patients (3/66, 4.5%, p < 0.01). Sex, age, family history of stones, initial presentation in the emergency room, and surgical intervention type showed no significant associations.
Comparative Analysis of Variables Influencing Patient Adherence to Postoperative Follow-Up
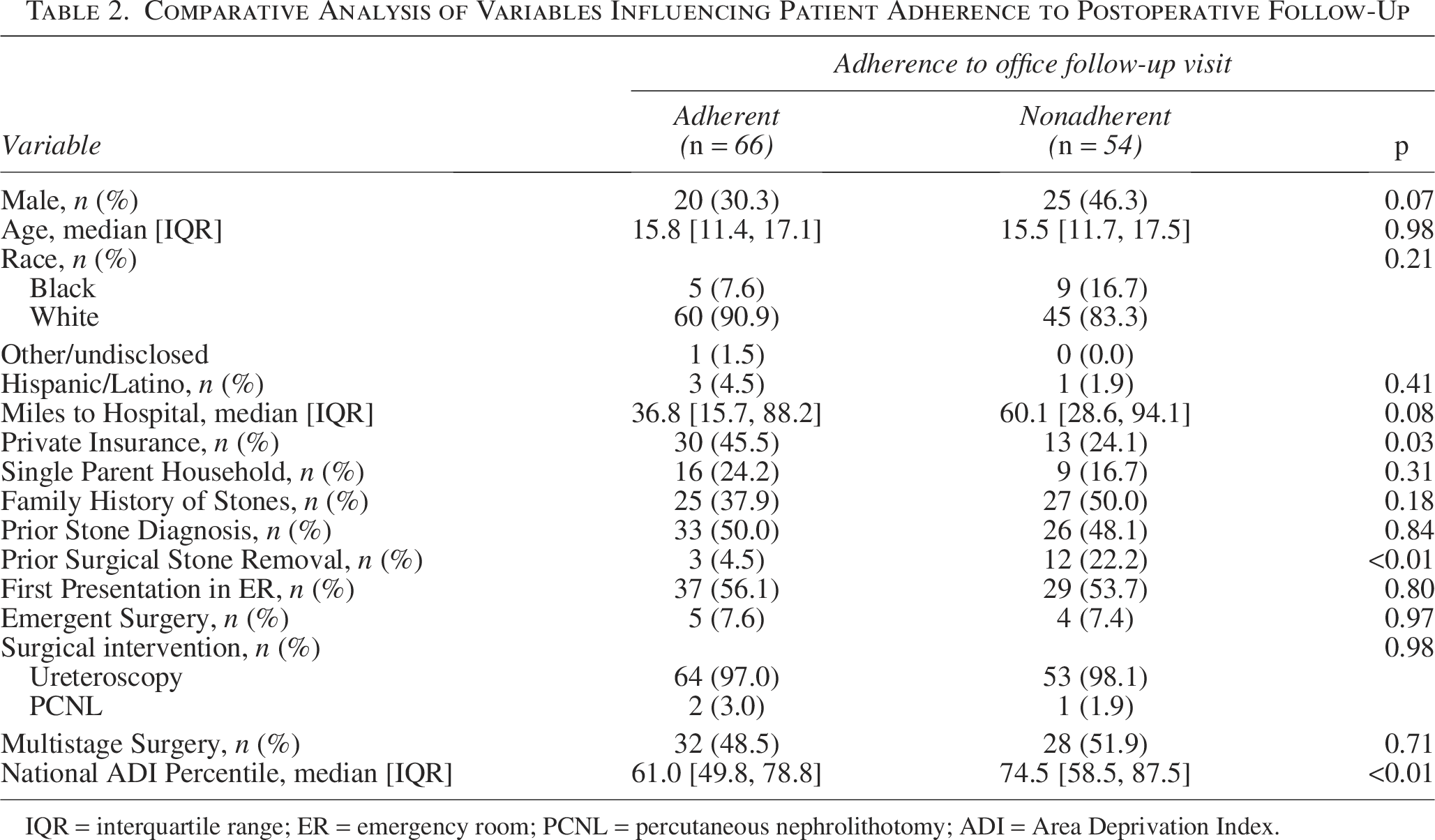
IQR = interquartile range; ER = emergency room; PCNL = percutaneous nephrolithotomy; ADI = Area Deprivation Index.
Private insurance was significantly more common in those who were adherent to follow-up visits than those who were not (45.5% vs 24.1%, p = 0.03). In addition, patients who adhered to follow-up had a lower median national ADI percentile (median = 61.0, IQR: 49.8–78.8) compared with nonadherent patients (median national ADI percentile = 74.5, IQR: 58.5–87.5; p < 0.01). Spearman’s correlation revealed a significant negative association between ADI and private insurance (ρ = −0.370, p < 0.001), suggesting that as ADI National Percentile increases, the likelihood of having private insurance decreases in a monotonic manner.
Influence of PKIDS enrollment
Seventy-one patients met criteria within the PKIDS trial time frame (January 2021 onwards): 30/71 (42.3%) enrolled in the PKIDS cohort, whereas 41/71 (57.7%) did not (Table 3). No significant difference in adherence was found between the two groups, with 18/30 (60.0%) of PKIDS cohort acquiring imaging within 16 weeks compared with 19/41 (46.3%) in the non-PKIDS cohort (p = 0.26). Additional variables, including sex, age, hospital distance, insurance type, and ADI indices, were not significantly associated with imaging adherence.
Overview of Patient Demographic During Pediatric Kidney Stone Enrollment and Comparative Analysis on Patient Acquisition of Imaging
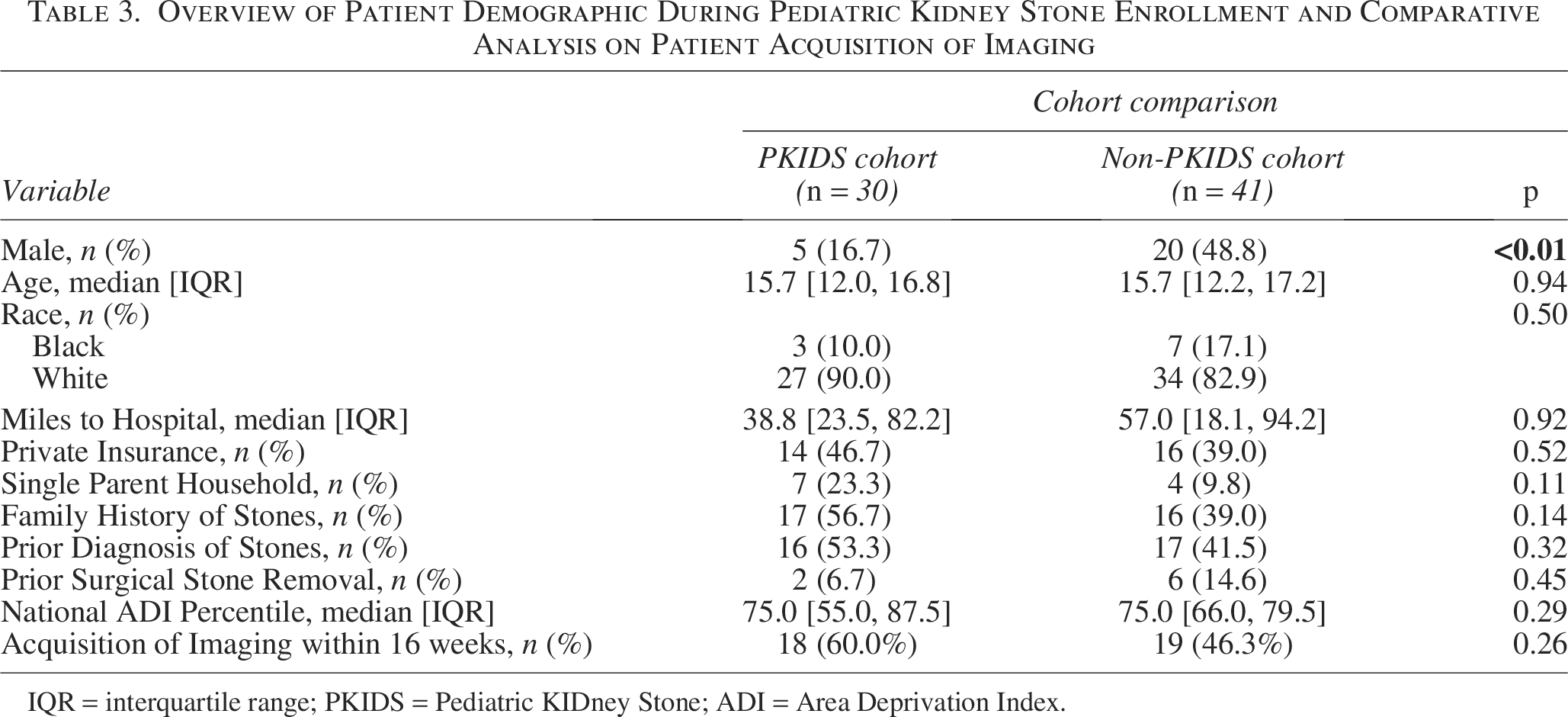
IQR = interquartile range; PKIDS = Pediatric KIDney Stone; ADI = Area Deprivation Index.
Discussion
This study aimed to provide insights into factors associated with adherence to postoperative follow-up among pediatric patients undergoing kidney stone removal at a tertiary care children’s hospital. Our findings suggest that insurance status and ADI scores may influence adherence to postoperative appointments. Although ADI has been extensively studied in the context of socioeconomic challenges and their associations with various health outcomes, it has not been previously utilized to examine associations with postoperative adherence in the pediatric population.
Association of insurance type with adherence
Our association between insurance type and adherence in pediatric kidney stone patients aligns with findings in other pediatric populations, where private insurance often correlates with better access to health care services. Findings from studies comparing Medicaid and commercial insurance similarly highlight that private insurance is associated with improved access to outpatient care and higher utilization of office visits. 7 Byrd and associates observed that children insured through publicly funded programs were significantly less likely to adhere to recommended well-child care visits compared with those with private insurance, even when financial barriers were minimized. 8 Private insurance is often associated with increased access to a wide range of outpatient services, but it may also come with unexpected financial burdens like high deductibles or co-pays, costs that do not apply to public insurance like Medicaid. Unfortunately, our dataset did not include detailed information relating to insurance costs, limiting our ability to directly assess their role in adherence. Future research incorporating these financial data points will be valuable in disentangling the different components of insurance coverage.
Although insurance status is often used as a proxy for socioeconomic status, a previous study has shown that it misclassifies socioeconomic status in over 20% of pediatric patients. 9 ADI and insurance status capture different but complementary dimensions of socioeconomic status—ADI reflects neighborhood-level deprivation, whereas insurance reflects individual-level access and financial resources. Both measures offer valuable and distinct insights into disparities in health care access, and using them in tandem may provide a more nuanced understanding of adherence-related barriers.
Our cohort supports this finding as well, where Spearman’s correlation between ADI and insurance was of moderate strength, implying a meaningful but not overwhelming relationship between these variables. This suggests that ADI may be a better marker for socioeconomic status than insurance status and should be considered for health disparities research in the pediatric population. Future studies using multi-institutional data (such as the PKIDS database) are needed to better validate the use of ADI in understanding barriers to postoperative care for children. 3
Stout and colleagues similarly examined adherence after kidney stone operation and found that private insurance and single-parent household status were significantly associated with increased adherence. 10 Although our study did not find single-parent household status to be significant, these findings align with broader trends that highlight the role of social determinants of health, such as insurance and household structure, in continuity of care. Denning and coworkers demonstrated that outpatient follow-up rates after pediatric operation were higher among patients with private insurance compared with those with Medicaid. 11 They also noted that follow-up was associated with significant reductions in 30-day emergency department visits and readmissions. These findings underscore a strong association of insurance type in facilitating continuity of care.
The role of ADI in adherence
The use of ADI as a socioeconomic measure provided further insight, with lower ADI scores correlating with higher adherence. ADI has been well studied in urologic literature, particularly in relation to cancer outcomes, where it has been shown to influence access to care, treatment decisions, and overall patient outcomes.12–14 Studies on bladder irrigation, antimicrobial prophylaxis for vesicoureteral reflux, and enuresis management have shown that adherence rates are significantly influenced by patient and family characteristics and access to health care resources.15–18 Children residing in socioeconomically deprived neighborhoods utilize more primary care services, but face challenges such as reduced continuity of care, particularly when residential mobility is involved.19,20 Although other validated neighborhood-level socioeconomic status metrics exist (i.e., the Social Vulnerability Index and Distressed Communities Index), we selected the ADI given its more established use in pediatric and urologic research, as well as its fine geographic resolution and validation across diverse clinical outcomes.
Within pediatric surgical literature, neighborhood-level deprivation has been linked to adverse postoperative outcomes. For instance, Cockrell and associates found that children from socioeconomically disadvantaged areas experienced worse surgical outcomes, independent of clinical factors.21,22 Similarly, Solomon and colleagues reported that social determinants of health influenced adherence to follow-up after orchiopexy. 24 Stephens and coworkers further highlighted the growing interest in geospatial measures of social determinants of health, including the ADI, noting their predictive value across multiple pediatric surgical domains. 25 These findings underscore the importance of considering intersecting barriers—such as health literacy, income instability, and transportation access—when designing interventions to improve adherence.
Prior surgical stone removal
Our study showed that patients with a history of prior surgical stone removal may influence adherence to follow-up. This may reflect a variety of factors, such as caregiver fatigue or the perception that follow-up is less critical once the acute episode has been managed. Prior work by Lee and associates suggests that symptomatology at presentation may influence follow-up behaviors, with higher adherence observed among patients presenting with symptomatic stones. 24 Because of documentation limitations, we were unable to reliably assess symptom severity or presentation characteristics in our study, but this remains an important area for future research. These speculations underscore the need for further investigation into motivational and psychosocial factors influencing adherence in this high-risk group.
PKIDS enrollment and acquisition of postoperative imaging
Finally, no significant difference in imaging adherence was observed between PKIDS-enrolled and nonenrolled patients. It has been thought that participation in clinical trials can lead to deviations in patient behavior that can lead to increased awareness of their medication conditions and improved adherence to care, a phenomenon known as the Hawthorne effect. 20 However, our results did not demonstrate this, despite the use of dedicated administrative support as well as financial renumeration. This suggests that although general reminders and incentives are beneficial, they may not fully address underlying barriers to adherence, suggesting that individualized interventions are necessary to address specific barriers faced by families.
Based on these findings, future clinical strategies could include the use of care navigation services to assist with scheduling and transportation, as well as expanded use of telehealth follow-up to reduce geographic and socioeconomic barriers to adherence. In addition, integrating social risk screening tools such as ADI into electronic health record systems (e.g., through automatic scoring at intake) could help providers proactively identify patients at higher risk for nonadherence. This may allow for earlier, tailored interventions to reduce the financial and logistical burdens on families and improve continuity of care. For example, if ADI scores were visible alongside clinical intake data, providers could flag patients who might benefit from social work consultation, transportation assistance, or prioritized telehealth scheduling.
Limitations
Several limitations of this study should be acknowledged. Alabama ranks among the lowest states for health literacy, socioeconomic status, and access to health care.23,26 Moreover, the demographic composition of our cohort reflects the patient population of our single institution and limits the generalizability of these findings to more diverse pediatric populations. As such, our findings may not be generalizable to broader or more diverse populations; a larger, prospective, multi-center study would better capture adherence barriers. The limited sample size, driven by the short study time frame, may have restricted the power of the analyses and the ability to conduct subgroup analyses, including use of multivariable regression to adjust for confounding and identify independent factors associated with adherence. Follow-up adherence could be underestimated, such as patients who followed up locally with pediatricians or obtained undocumented imaging studies elsewhere. The retrospective design limited our ability to collect detailed socioeconomic data—such as household income, food insecurity, and transportation access—as these variables were not available in either the electronic health record or the PKIDS dataset. In addition, we were unable to control for potential confounders such as comorbidities, family structure, or other barriers to care. Addressing these limitations will enhance the generalizability and depth of these findings.
Conclusion
This study highlights the role of socioeconomic factors in postoperative adherence among pediatric kidney stone patients. The limited impact of the specific compensation and reminder strategies used in the PKIDS trial suggests that such methods alone may not be sufficient to improve adherence in this population. Future research should explore multicenter studies that examine a broader range of adherence measures to develop more comprehensive and effective interventions.
Authors’ Contributions
B.T.B. and C.M.C.T.: Research conception and design. B.T.B., J.G., and C.M.C.T.: Data acquisition. B.T.B. and J.G.: Statistical analysis. B.T.B., J.J.C., J.G., and C.M.C.T.: Data analysis and interpretation. B.T.B. and C.M.C.T.: Drafting of the article. B.T.B., J.J.C., T.B., J.G., D.K., D.J., S.T., G.T., and C.M.C.T.: Critical revision of the article. J.J.C. and C.M.C.T.: Supervision. B.T.B., J.J.C., T.B., J.G., D.K., D.J., S.T., G.T., and C.M.C.T.: Approval of the final article.
Footnotes
Acknowledgments
The authors would like to thank Josh Cummins for his valuable assistance with data collection. Portions of the abstract were previously published in the Journal of Endourology, Vol. 38, No. S1 Abstracts of the 41st World Congress of Endourology and Urotechnology WCET 2024 ![]() .
.
This work was supported in part through a Patient-Centered Outcomes Research Institute (PCORI) Program Award (CER-2018C3-14778). All statements in this report, including its findings and conclusions, are solely those of the authors and do not necessarily represent the views of the PCORI, its Board of Governors or Methodology Committee.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported, in part, through a Patient-Centered Outcomes Research Institute (PCORI) Program Award (CER-2018C3-14778). All statements in this report, including its findings and conclusions, are solely those of the authors and do not necessarily represent the views of the PCORI, its Board of Governors, or Methodology Committee.
Ethics in Publishing
Ethical approval was granted by the quality improvement department of Children’s of Alabama as well as the Institutional Review Board of the University of Alabama at Birmingham (IRB#−300012330).
Submission Declaration and Verification
This work has not been published previously and is not under consideration for publication elsewhere. This work is approved by all authors and tacitly or explicitly by the responsible authorities of the clinic where the work was carried out.