
Abstract
Background
Driving promotes independence in older adults, yet age-related changes in cognition and sleepiness may reduce driver safety. We examined associations between sleepiness and driving in older adults with subjective cognitive decline (SCD) and mild cognitive impairment (MCI).
Methods
A cross-sectional/observational study of older drivers (60-80 years), classified as cognitively healthy (n = 21), SCD (n = 26), or MCI (n = 13), completing the Manchester Driver Behaviour Questionnaire (DBQ), and a 2-week driving diary including the Sleepiness Symptoms Questionnaire (SSQ).
Results
For DBQ, MCI drivers reported 2.26x more driving lapses (eg, memory/attention failures) than healthy, while SCD reported 2.54x more driving violations than MCI. For diaries, SCD drivers reported 7.51x more inattention events than healthy, and higher SSQ (P = .002). Higher SSQ was associated with increased inattention events for SCD and MCI groups (P ≤ .018).
Conclusion
Sleepiness impacts poorer driving outcomes in SCD and MCI, providing an intervention opportunity to support continued driving.
Introduction
For older adults, driving a motor vehicle forms an important part of maintaining quality of life through continued independence and enabling access to multiple opportunities and needs. Dementia is characterised by significant impairments in cognition and daily functioning, with Alzheimer’s Disease (AD) as the most common cause, 1 and increasing severity is associated with greater likelihood of driving cessation. 2 Nonetheless, driving is rated as the second most valued instrumental activity of daily living (IADLs) for maintaining independence within the community 3 and is associated with greater engagement in social events. 4 In the 2024 Lancet Commission, 45% of dementia risk was attributed to modifiable factors, including 5% to social isolation. 5 Risk modifying interventions for dementia are essential for preventing and delaying the incurable disease, especially during early pre-dementia stages of Mild Cognitive Impairment (MCI) and Subjective Cognitive Decline (SCD) where subtle cognitive changes can occur 10 years before dementia onset.6-8 However, preserving driving abilities as a proactive strategy to reduce dementia risk may be an important target that remains unexplored. Road safety is a shared responsibility however, necessitating a need to balance continued independence with personal and public safety as driving abilities change.
While driving ability becomes significantly impaired in moderate to severe dementia, many individuals with MCI and mild AD preserve fitness to drive. 9 Individuals with MCI exhibit suboptimal driving performance relative to cognitively healthy older adults, however, this does not constitute impaired driving capacity as these reductions were considered to pose minimal threat to road safety.10-13 Only one study has investigated driving performance in older adults with SCD, which found a difference in a safety behaviour relative to those with MCI; however, the directionality was not reported. 14 In addition to objective measures, self-perceived driving abilities often form the basis by which individuals may decide to cease driving. 15 Older adults with MCI may overestimate driving risks as they report driving faster and shorter following distances compared to objective driving simulator measurements. 16 Furthermore, compared to those without cognitive impairment, older adults with MCI or mild AD are more likely to report self-regulation driving behaviours, such as avoiding making turns and driving at night.17,18 Together, these results suggest older adults with MCI can self-monitor driving abilities, and this is yet to be investigated in older adults with SCD.
Driving ability also requires optimal alertness. 19 Sleepiness is associated with impairment across a range of driving abilities 20 and greater likelihood of falling asleep whilst driving. 21 Together, this increases the risk of crashes and associated injuries.22,23 While sleep disturbances are linked to changes in sleepiness, 24 sleepiness is influenced by many additional factors and impairs driving ability regardless of its cause. 25 Nevertheless, little is known about sleepiness in older adults with early cognitive changes. Daytime sleepiness can accompany cognitive impairment in older adults with mild or moderate dementia, 26 though few studies have addressed daytime sleepiness in older adults with MCI. Of those, findings suggest that those with MCI may not differ in daytime sleepiness to their cognitively healthy counterparts.27-29 However, perceived cognitive decline appears to be linked to perceived sleepiness, with greater severity of perceived cognitive decline being associated with more daytime sleepiness. 30 As sleepiness is often the result of insufficient or disturbed sleep, including the effects of obstructive sleep apnoea (OSA), intervention strategies can be effective in reducing sleepiness,31-33 which in turn may improve driving outcomes. Although the relationship between sleepiness and driving has been investigated in cognitively healthy older adults, 34 the only study conducted in older adults with MCI found no associations between pre-drive sleepiness and simulator driving performance, 35 and this is yet to be studied in those with SCD.
Further work is required to characterise driving behaviours and to determine the interplay between sleep and driving in older adults with SCD or MCI who are at risk of future dementia diagnoses. To inform future driving interventions on the aspects of driving that may benefit from additional support to ensure continued independence and safety on the road, this exploratory study will characterise driving behaviours in older adults at various stages of cognitive decline. Specifically, this study examined the relationship between various stages of cognitive decline (ie, SCD, MCI, and cognitively healthy individuals) and adverse driving events based on self- and informant-reports. Additionally, we explored the association between self-reported sleepiness symptoms and incidences of adverse driving outcomes to understand awareness of impairment in this population of drivers.
Methods
Participants
Sixty-seven community-dwelling adults, aged 60 – 80 years were recruited through online advertisements, community-based flyers, or from a private geriatric clinic. To be eligible for the study, participants had to be fluent in English, have a Standardised Mini Mental State Examination score greater than 20, 36 and be an active driver at the time of participation. Exclusion criteria were a current mental health or psychiatric disorder (except depression and anxiety), a lifetime diagnosis of a neurodevelopmental disorder, neurological disorder, severe head injury, or neurocognitive disorder (except Minor Neurocognitive Disorder due to Alzheimer’s Disease); regular use of medications known to affect sleep (ie, sedatives, hypnotics, melatonin, opioids, mood stabilisers, antipsychotics, anxiolytics, or anticonvulsants), and anaesthesia in the past 3 months; consumed less than 14 standard drinks of alcohol per week, and no illicit substance use in the past 12 months.
Participants were recruited between March 2021 and May 2024. All participants provided written consent to participate in the study. The study was approved by the Monash University Human Research Ethics Committee.
Protocol
Following eligibility screening, the cross-sectional study included classification of cognitive status through completing an in-person neuropsychological assessment, completing driving questionnaires by the participant (and an informant, optional). Driving diaries were provided at the end of the neuropsychological assessment and were completed during a 2-week period that best represents their typical driving patterns.
Classification of Cognitive Status
Participants with SCD were classified according to the SCD-I working group recommendations,
6
whereby participants display no objective impairment on neuropsychological testing and self-reported declines in cognition beyond typical ageing. Perceived decline in cognition was assessed through 2 methods. First, the Subjective Cognitive Decline Questionnaire (SCD-Q)
37
is a 24-item questionnaire that assesses cognitive changes in daily functioning in the past 2 years through self-report (MyCog; scores
Neuropsychological Assessment
Participants completed a neuropsychological assessment battery that was sensitive to detecting early cognitive decline associated with dementia across different cognitive domains. Cognitive domains included learning, memory, language, visuospatial, processing speed, and executive functions. The test battery (described in detail elsewhere
42
) comprised of: • Global cognition: the Standardised Mini Mental State Examination (SMMSE)43,44 to screen for and describe global cognition. • Memory: The Rey Auditory Verbal Learning Test (RAVLT)
45
and the Logical Memory I and II subtests from the Wechsler Memory Scale - III
46
assessed verbal learning and memory. • Processing speed: The Trail Making Test, Part A (TMT-A)
47
and the colour-word interference task (colour reading and word reading conditions) from Delis-Kaplan Executive Functioning System (D-KEFS)
48
evaluated processing speed. • Executive functions: Several measures of executive functions were obtained. The Controlled Oral Word Association Test (COWAT)
49
measured verbal fluency. Digit Span subtest from the WAIS-III
50
assessed working memory. The Trail Making Test, Part B
47
evaluated mental flexibility. Response inhibition and switching were measured using the inhibition (commonly known as STROOP task) and inhibition-switching conditions from the D-KEFS colour-word interference, respectively.
48
• Language: The 60-item Boston Naming Test (BNT)
51
assessed confrontation naming; however, the BNT was not used for classification in non-native English speakers.52,53
Driving Outcomes
Driver Behaviour Questionnaire (DBQ)
The 28-item Manchester Driver Behaviour Questionnaire (DBQ) 54 was used to assess self-reported driving behaviours in the past year, such as disregarding speed limits and hitting something while reversing. Items were rated on a Likert scale from 0 (Never) to 5 (Nearly all the time), which were summed to provide scores across driving lapses, aggressive violations, violations, and errors. Driving lapses are behaviours due to involuntary attention or memory failures (eg, forget where you left your car in a car park). Violations are intentional breaches of safe driving practices (eg, speeding), where aggressive violations are deliberate hostility towards other road users (eg, getting angry at another driver). Errors are unintended errors in judgement or decision-making, where planned action did not result in the achieved outcome (eg, missing a give way sign). This was also completed by informants as an optional component.
Driving Diary
The driving log (adapted from Anderson et al., 2018 55 ) was completed after each trip that was 15 minutes or longer (Supp 1). The driving diary collected information on duration, type of commute, and adverse driving events that were classified into 4 categories56,57: sleep related (fell asleep at stop light, resting your eyes), inattention (fixation on internal/external object, lack of awareness, being distracted), hazardous (braked sharply, hit the curb, swerved violently, missed your turn), or violations (drove through stop light, shouting at another person). Violation events were transformed into a binary variable (ie, 0 or 1) as there was only one instance of more than one event.
Sleepiness Symptoms
Two measures of subjective sleepiness were incorporated in the driving diary. The Karolinska Sleepiness Scale (KSS) 58 measured subjective sleepiness symptoms at the start and end of the driving session, and it was rated on a Likert scale from 1 (Extremely alert) to 9 (Very sleepy, fighting sleep, great effort to stay awake). The 8-item Sleepiness Symptoms Questionnaire (SSQ) 59 assessed sleepiness symptoms specific to driving performance, such as difficulty keeping to the middle of the road. A Likert scale from 1 (Not at all) to 7 (Most of the time) was used. Item scores were summed, and higher total scores indicate more severe sleepiness symptoms.
Data Analysis
Data analysis were conducted in R-Studio 60 with R version 4.0.5. 61 Between group differences in demographic variables were assessed using Kruskal-Wallis test for continuous variables, and Fisher’s Exact test for categorical variables. Within group differences between self- and informant-reported scores were evaluated using Wilcoxon signed-rank test.
There was data loss of 10 participants (16.7%) on self- and informant-reported lapses, violations, and errors DBQ factors due to administrative revisions on the DBQ items included. Given that the informant DBQ was optional, items with missing data were excluded from analysis. This resulted in n = 6 informant reports being excluded from lapses, n = 4 excluded from aggressive violations, n = 3 from violations, and n = 10 from errors analyses. To examine whether cognitive status groups predicted DBQ driving behaviours (ie, lapses, aggressive violations, violations, and errors), negative binomial regressions were conducted, accompanied by incidence rate ratio (IRR), 95% confidence intervals (CI), and McFadden’s R2 as effect size. Unadjusted and adjusted (for age, sex, and recruitment setting) model estimates are reported. Benjimini-Hochberg false discovery rate (FDR) was applied to covariate adjusted models to correct for multiple comparisons (p FDR ). IRRs with 95% CIs that are wide or incongruent with the P-value will not be considered as a valid result due to instability in the estimate.
To investigate whether cognitive groups could predict adverse driving events and subjective sleepiness symptoms on the KSS and SSQ from driving diaries, repeated-measures generalised linear mixed effects models were conducted. Driving events, KSS, and SSQ scores were individually entered as outcome variables, group as predictor (modelled as fixed effects), and within participant variability was modelled as random effects (1|ID). Poisson distribution was specified for inattention, hazardous, and total driving events. Binomial distribution was specified for violation events, and gamma distribution was used for KSS and SSQ. As low number of near-misses were reported across the whole sample (n = 8), binary logistic regression was conducted. Unadjusted and adjusted (for drive duration) estimates will be included, and models with sleepiness symptoms (KSS or SSQ) as the outcome variable were additionally adjusted for number of self-reported sleep disorders. If analysis revealed significant associations in sleepiness symptoms and driving events, follow-up analyses were conducted to examine the contribution of sleepiness to driving events. P < .05 for statistical significance was used for all analyses.
Results
Participant Demographic Information by Cognitive Status Group
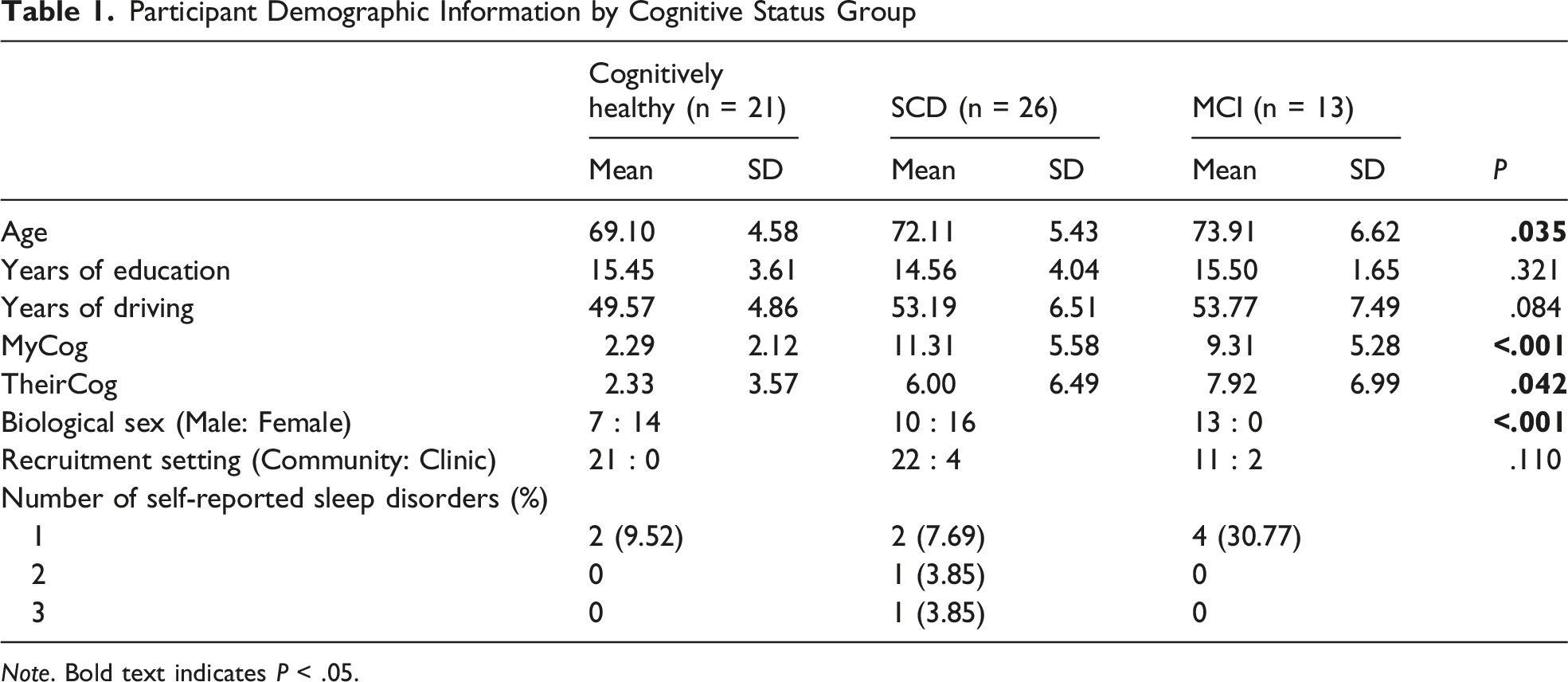
Note. Bold text indicates P < .05.
DBQ and Driving Diary Summary Statistics

Note. DBQ: Driver Behaviour Questionnaire; SSQ: Sleepiness Symptoms Questionnaire; KSS: Karolinska Sleepiness Scale. DBQ measures driving behaviours in the past year.
Associations Between Cognitive Status and Driver Behaviour Questionnaire (Self- and Informant-Reported)
Associations Between Cognitive Status and Driving Lapses, Aggressive Violations, Violations, and Errors on the DBQ

Note. IRR: Incidence rate ratio; p FDR : FDR corrected P-value based on adjusted model. Adjusted model controlled for age, sex, and recruitment setting. *P < .05; **P < .01; ***P < .001. Bold text indicates P < .05 for adjusted models that withstood FDR correction. Negative binomial regression was used for all models.
aReference group.
bResult not valid due to wide and incongruent 95% CI.
No significant differences were found between self-report and informant-report DBQ scores for any outcomes (p adj ≥ .065). There were, however, slight differences in group risk in informant-reported outcomes (see Table 3). SCD was associated with approximately 3 times more violation events compared to both cognitively healthy and MCI groups (p FDR < .016) that was small in effect (McFadden’s R2 = 0.07). Although SCD was also associated with 5.76 times more driving errors relative to the MCI group (P = .041), the 95% CI was wide and incongruent with the P-value, and therefore not considered a valid result. No associations were found between cognitive status and lapses or aggressive violations (p adj ≥ .394).
Associations Between Cognitive Status With Self-Reported Actual Driving Events and Sleepiness Symptoms (Driving Diary)
A subset of 59 participants completed driving diaries for 2 weeks. From 804 potential diary entries, there were 789 completed entries, resulting in a 2% data loss and exclusion of 3 participants with SCD (due to incorrectly completed entries). The final sample consisted of 56 participants (N = 21 who were cognitively healthy, N = 22 with SCD, and N = 13 with MCI).
Descriptive statistics for number of diary entries, drive duration, subjective sleepiness measures, and frequency of driving events by cognitive groups are shown in Table 2. There were no differences in the number of diary entries across groups (P = .177). Significant difference in drive duration was found (P < .001), where the MCI group drove longer per trip compared to the cognitively healthy (P = .016) and SCD groups (P < .001). Mean SSQ and KSS scores (averaged within participants) did not significantly differ between groups (P > .084). Drive duration was therefore entered as covariates into all subsequent models. As no crashes and only one sleep related event was reported, these variables are excluded from analysis.
Cognitive Status and Actual Driving Events
Relationship Between Cognitive Status Group (Cognitively Healthy, SCD, and MCI) and Driving Events and Sleepiness Symptoms on Driving Diaries

Note. IRR: Incidence rate ratio; OR: Odds ratio; ICC: Intraclass correlation coefficient; p FDR : FDR corrected P-value based on adjusted model. Adjusted model controlled for drive duration (standardised).*P < .05; **P < .01; ***P < .001. Bold text indicates P < .05 for adjusted models that withstood FDR correction.
aPoisson distribution.
bBinomial distribution.
cGamma distribution.
dAdditionally adjusted for number of self-reported sleep disorders.
Cognitive Status and Sleepiness Symptoms
The associations between cognitive status and sleepiness symptoms (KSS and SSQ) are shown in Table 4. The SCD group reported approximately 1.10 times greater sleepiness symptoms on the SSQ per unit of standardised drive duration compared to the cognitively healthy group in the unadjusted (P = .006) and adjusted models (p adj = .002, p FDR = .012). No other significant group associations were found for SSQ (p adj ≥ .085) or pre-drive KSS ratings (p adj ≥ .805).
Association Between Sleepiness Symptoms and Inattention Driving Events for SCD
As SCD was independently associated with SSQ and inattention driving events, we examined the association between sleepiness symptoms (SSQ) and inattention driving events within the SCD group, using generalised linear mixed effects models with Poisson distribution. Here, each unit of increase on the SSQ was associated with 1.34 times greater rates of inattention driving events, adjusted for drive duration (95% CI [1.10 – 1.63], p adj = .004). Intraclass correlation coefficient (ICC) of 0.43 indicates that 43% of variance in inattention events was attributed to between participant differences within the SCD group. Marginal R2 of 0.07 and conditional R2 of 0.47 indicate that fixed effects accounted for 7% of the variance, while the full model accounted for 47% of the variance, respectively. As a check on specificity within the SCD group, analyses were repeated for cognitively healthy and MCI groups. While each unit of increase in the SSQ was associated with 2.32 times more inattention events in the MCI group (random effect was removed due to insufficient sample size; 95% CI [1.16 - 4.63], p adj = .018), no significant association was observed for the cognitively healthy group (p adj = .099).
Associations Between SSQ Items and Inattention Driving Events Reported on Driving Diaries in Participants With SCD

Note. IRR: Incidence rate ratio; ICC: Intraclass correlation coefficient; p adj : Adjusted for drive duration (standardised). Bold text indicates P < .05.
Discussion
This cross-sectional study systematically examined self and informant reports of driving behaviours across the prodromal stages of dementia (ie, SCD and MCI) relative to cognitively healthy individuals. We found that SCD was associated with more inattention events and increased sleepiness symptoms while driving, and sleepiness symptoms were associated with greater inattentive driving events in older adults with SCD and MCI. Our findings suggest that sleepiness may have safety implications for driving in the prodromal stages of dementia (SCD and MCI). Early changes in driving ability and/or sleepiness while driving may serve as useful targets to identify at-risk older drivers and to support continuation of driving for social engagement as a dementia risk reduction strategy.
Sleepiness symptoms while driving (SSQ) was significantly associated with greater self-reported inattention driving events on driving diary in both the SCD and MCI groups. This is expected as sleepiness can reduce vigilance and sustained attention,62,63 further exacerbating inattention and distractibility.64,65 Given that this relationship was not found in participants who were cognitively healthy suggests that older adults with early cognitive changes (SCD and MCI) may be particularly vulnerable to the depletion of attentional resources associated with sleepiness, leading to greater inattention during driving. For specific sleepiness symptoms (derived from the SSQ), we found that self-reported slower reactions had the strongest association with inattentive driving in older adults with SCD (5x), followed by difficulty keeping to the middle of the road (4x). Both these symptoms have been shown as predictive of drowsiness-related near-crash events.66,67 These results suggest that monitoring of sleepiness symptoms while driving is important for individuals with SCD and MCI to support safer driving outcomes.
Compared to cognitively healthy older adults, SCD was associated with more self-reported inattention driving events and greater self-reported sleepiness symptoms whilst driving (SSQ) for drives of equivalent duration. Inattention events were characterised by distractibility and reduced situational awareness, which aligns with previous findings that older adults with SCD demonstrate less efficient attention allocation, spatial attention, and inhibitory control68-70 than healthy older adults. Additionally, earlier evidence described that greater severity of perceived cognitive decline was associated with higher self-reported daytime sleepiness and need of more sleep.30,71 Of interest, this enhanced sleepiness in SCD was not observed for KSS, which is consistent with previous findings in older driver with and without MCI. 35 This suggests that the sleepiness symptoms may have emerged while driving and/or are only evident when concrete behavioural anchors such as those in the SSQ are used. 67
While the association between sleepiness and inattention was observed for older adults with MCI, MCI was not independently associated with sleepiness or inattention events when compared to other cognitive groups (unlike SCD). Moreover, older adults with SCD reported more driving violations on the DBQ than those with MCI (eg, speeding, running red light). Although this was corroborated by informant reports, it did not withstand multiple comparisons correction and thus should be interpreted with caution. There are several explanations for these observations. Firstly, older drivers with MCI may utilise compensatory behaviours. For instance, in a recent study of real driving, individuals with cognitive impairment were less likely to drive after a night of poor sleep. 72 Drivers in our study (with MCI) may therefore have been less likely to drive when sleepiness was high. Secondly, the MCI group may have reduced insight and therefore under-report impairment. Specifically, impaired retrospective memory recall in those with aMCI 73 may lead to inaccurate reporting of adverse driving outcomes. However, under-reporting is less likely given that informant-reports did not significantly differ to self-reported scores. Thirdly, it is possible that the SCD group exhibit hypervigilance around functional concerns. This is supported by their significantly elevated self-reported cognitive concerns (MyCog) relative to the informant (TheirCog) that was unique to the SCD group. It is possible then that over-reporting of decline may also extend beyond cognition to sleepiness and driving abilities. Finally, this finding may be influenced by the small sample size in the MCI group, which may not have sufficient power or adequately capture representative population characteristics.
Those with MCI reported more driving lapses on the DBQ relative to healthy controls; however, this finding did not withstand multiple comparisons correction, likely due to small sample size. Notwithstanding, driving lapses largely comprised of behavioural errors resulting from memory or attentional failures (eg, forgetting where the car was parked), which is consistent with literature showing impaired sustained attention, executive attentional control, and working memory in older adults with MCI.74-77 Taken together, our results suggest that (a) SCD may represent a transitional stage where drivers can recognise subtle changes in cognition, driving, and sleepiness, highlighting this as an optimal stage for early driving interventions, but importantly (b) future work with a larger sample size should examine the incidence of adverse driving and sleepiness in those classified with MCI, extending both our work and that recently described by Chang and colleagues. 72
Our data should be interpreted with the following caveats in mind. Firstly, the DBQ has limited capacity in predicting objective crash data 78 despite correlating closely with objective on-road or simulator driving behaviours. 79 To improve accuracy and insight, the informant DBQ was included to provide more objective insight into driving behaviours. 80 Secondly, the relatively small sample size may have implications for our results. For the MCI group especially, lack of significant findings should be interpreted with this in mind. For the SCD group, a relatively small sample size may have led to instability in model estimates for group comparisons. However, most significant relationships were preserved after correction for multiple comparisons and mixed effects models obtained a minimum conditional R2 of 0.46 that indicate an overall substantial degree of explanatory power. Thirdly, oxygen saturation as an objective indicator of OSA was not assessed despite previous work showing a negative impact on driving in those with MCI. 35 We therefore acknowledge OSA as a possible contributing factor in the relationship between cognitive groups and driving behaviours. Lastly, the exclusively male composition of the MCI group limits the generalisability of our results to females with MCI, despite adjusting for sex as a covariate in analyses.
In conclusion, the current study found that sleepiness symptoms were associated with inattention during driving in older adults with SCD and MCI. SCD was associated with more inattention driving events, possible driving violations, and sleepiness symptoms during driving, while older drivers with MCI may have more driving lapses. Our findings suggest that implementation of early interventions that encourage monitoring driving behaviours and sleepiness may support continued safe driving and can begin as early as SCD, that is, at least 10 years prior to the development of dementia. 7 Such an intervention could promote maintenance of functional and social independence that may, in turn, reduce social isolation as a dementia modifiable risk factor. Further research with larger sample size is required to clarify the effects of cognitive status and sleepiness on objective driving performance, and the potential effectiveness of early driving interventions on longitudinal cognitive functioning and eventual dementia progression.
Supplemental Material
Supplemental Material - Self-Reported Driving Behaviours and the Relationship With Sleepiness in Subjective Cognitive Decline and Mild Cognitive Impairment
Supplemental Material for Self-Reported Driving Behaviours and the Relationship With Sleepiness in Subjective Cognitive Decline and Mild Cognitive Impairment by Tiffany Y. T. Lo, Jessica E. Manousakis, Melinda L. Jackson, Michael Woodward, Sharon L. Naismith & Clare Anderson, PhD in Journal of Geriatric Psychiatry and Neurology
Footnotes
Acknowledgements
The authors would like to thank the participants for their time and dedication to the research. We would also like to thank Dr Anna Cai and Malisa Burge for assistance with neuropsychological assessments and statistical analysis, respectively.
ORCID iDs
Ethical Considerations
This study was approved by the Monash University Human Ethics Committee (approval no. 26176) on November 20, 2020. This research was conducted in accordance with the Declaration of Helsinki.
Consent to Participate
All participants provided written informed consent to participate.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sharon Naismith is supported by an NHMRC Leadership Fellowship: 2008064.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be available on request in writing to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.