
Abstract
Background
Mobility impairments in Parkinson’s disease (PD) significantly impact individuals’ physical health, independence, and psychosocial wellbeing. In this review, mobility loss is used to refer to altered or impaired mobility (eg, reduced gait, balance difficulties, freezing of gait), rather than a complete loss of mobility. These changes affect daily functioning and quality of life. Carers also experience significant burden as they manage mobility issues. Understanding the implications of mobility loss in PD is essential for improving support for both people with PD and carers. This review explores impact of mobility loss on perceived independence and psychosocial wellbeing in people with PD and carers, providing deeper insight into the broader emotional and social consequences of the condition.
Methods
A systematic search of six health databases (Medline, Embase, PsycInfo, CINAHL, Scopus, Web of Science) was conducted using key terms related to mobility loss, independence, and psychosocial wellbeing in PD. Studies were included if they employed qualitative methods to explore experiences of mobility from people with PD and/or carers. The methodological quality of studies was assessed using the NICE qualitative checklist, and reporting adhered to PRISMA guidelines. A meta-ethnographic approach was used to extract key themes and construct a comprehensive understanding of the findings.
Results
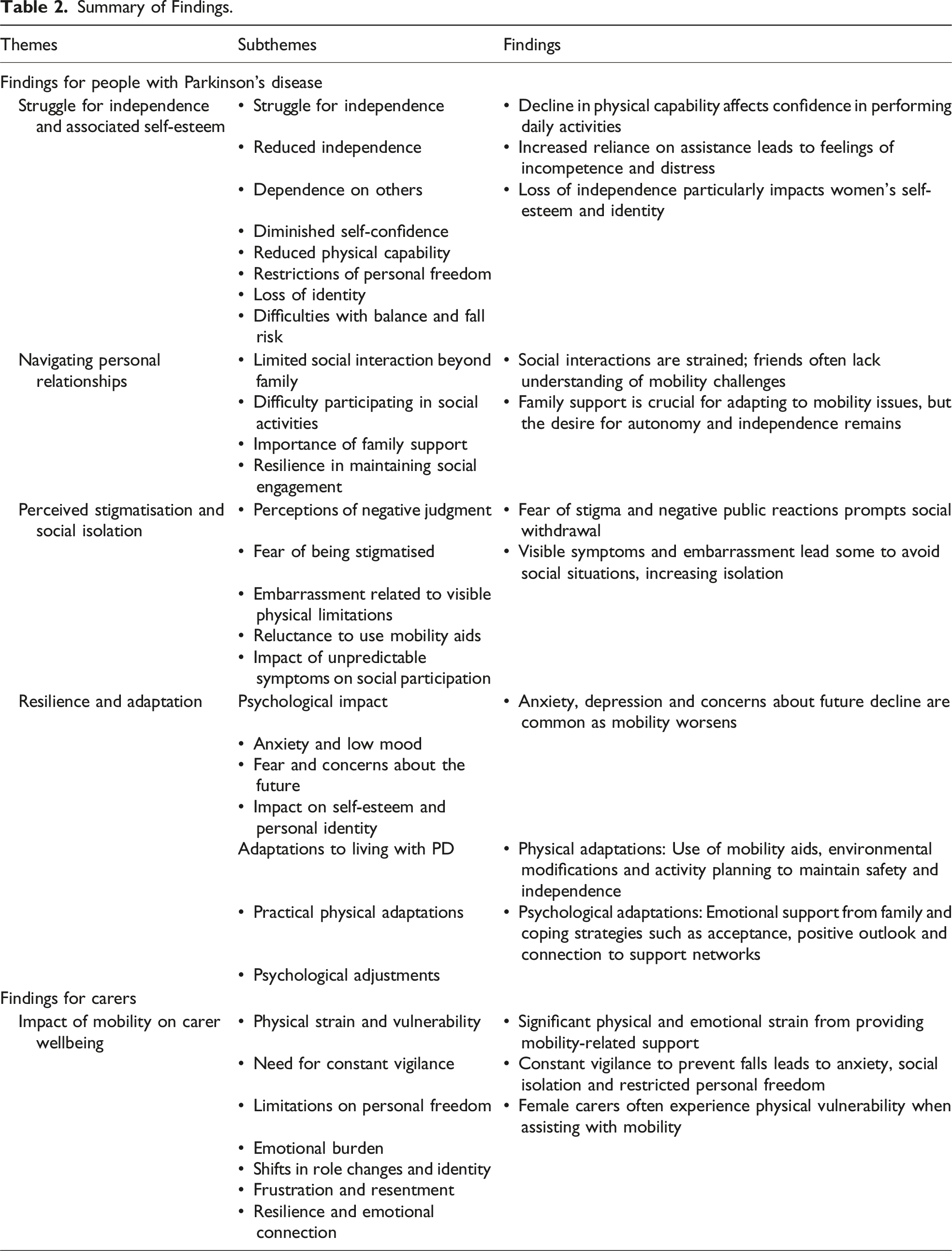
Five key themes emerged: the struggle for independence and associated self-esteem, navigating personal relationships, perceived stigmatisation and social isolation, resilience and adaptation, and impact of mobility on carer wellbeing.
Discussion
Findings highlight the need for comprehensive support systems that address the challenges of mobility loss in PD. Wearable technology presents a promising solution for personalised interventions. Future research should explore diverse populations of people with PD and include formal carers to develop a more holistic perspective of mobility-related challenges in PD caregiving.
Introduction
Functional abilities may decline during ageing, leading to some degree of functional dependency. 1 Physical mobility, defined as the ability to move independently from one place to another through functional movements like walking, is a central function in maintaining overall wellbeing.2-6 Mobility is associated not only with physical health but also mental, emotional, and psychological wellbeing, and is pertinent to one’s identity and sense of self. 6 While mobility limitations are often identified in older adults, certain clinical populations with mobility-related impairments experience a relatively early and accelerated decline.7,8 For instance, Parkinson’s disease (PD) is a neurodegenerative condition characterised by progressive motor dysfunctions which impair mobility and cause rigidity in one’s movement, significantly impacting quality of life.9-11 These mobility limitations have significant social and emotional consequences for people with PD, such as reduced quality of life, increased depressive symptoms, and restricted social participation.12-14
The impact of mobility loss in PD extends beyond the individual, profoundly affecting carers as well. PD is a complex condition that encompasses multiple limitations, including cognitive impairments, autonomic dysfunction, and mobility loss.15,16 Caring for someone with PD can place significant burden on carers, often resulting in psychological distress.17,18 Research shows that 40-50% of PD carers report symptoms of anxiety and depression, 17 and that the prevalence of depressive disorders among carers increased from 11.6% to 17.8% over a 12-month period 18 ; these statistics demonstrate the considerable psychological strain associated with caregiving. The burden is particularly pronounced when caring for people with more severe mobility impairments, as these cases often require increased physical assistance and heighten emotional stress due to higher dependency,19-21 further demonstrating that mobility loss plays a central role in the caregiving experience. Carer burden not only diminishes the carers’ quality of life but can also lead to reduced care capacity or increase the likelihood of an earlier transition to formal care for the person with PD. Such transitions not only pose wider economic and public health challenges,22-24 but also impact the person’s independence and wellbeing, and can place added emotional strain on families. While some syntheses have addressed carer burden in PD, they often consider the condition in its entirety. Several reviews have already explored important aspects of the lived experience of PD, including stigma, 25 psychosocial impact, 26 relationships, 27 identity and quality of life. 28 These reviews demonstrate the breadth of challenges faced by people with PD and carers; however, mobility loss is often treated as one theme among many rather than the central analytical focus. Despite existing research, there is a need for a more targeted analysis that looks at the experience of mobility loss as a defining feature of the PD experience. Understanding mobility-related challenges could not only highlight the specific burdens faced by carers but also ensure we monitor meaningful aspects of mobility for both people with PD and carers. This insight is essential for guiding timely and targeted interventions that support mobility, potentially alleviating carer strain and improving quality of life for both groups.
The value of exploring lived experience is being increasingly acknowledged in health and care research. 29 It illuminates both the perspectives and experiences of affected communities and is perhaps one of the most useful forms of research in this context, as those impacted by PD understand most about the complications of dealing with it.30-32 Therefore, investigations into the lived experience of PD have increased, demonstrated by two recent meta-ethnographies.33,34 While these reviews offer valuable insights and informs us of factors that contribute to the PD experience, their primary focus was on the broader impact on quality of life. Despite touching on psychological distress and social challenges, they did not fully identify how mobility loss specifically relates to these wider challenges. Interestingly, none of the existing reviews define mobility loss clearly or explore the psychosocial impact in detail.
Psychosocial wellbeing and independence are particularly important in this context; psychosocial wellbeing reflects the broader emotional and social consequences of PD, capturing changes in quality of life and identity over time,35,36 while independence reflects autonomy and functional capability, both of which can shape daily functioning and place a heavy burden on both people with PD and carers.37,38 Yet, despite their importance, current reviews do not provide a well-defined focus on mobility loss, a central aspect of PD, that underpins both psychosocial wellbeing and independence. Similarly, reviews examining the carer experience19,39-41 have not explored mobility-related challenges both for those with PD and carers. This leaves a clear gap for a focused synthesis that places mobility loss as the primary analytical lens.
Given the above, synthesising qualitative literature that explores how mobility loss affects independence and psychosocial wellbeing in people with PD and carers could offer valuable insights. This would address the current lack of a focused, in-depth exploration of mobility-related challenges in PD and provide a more comprehensive qualitative account that is currently missing. Therefore, this meta-ethnography aims to capture the impact of physical mobility loss on perceived independence and psychosocial wellbeing in people with PD and carers.
Methods
This synthesis consists of a systematic review and a following meta-ethnography. Methods will be reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and the reporting guidelines for meta-ethnography (eMERGe).42,43
Phase 1: Getting Started
Meta-ethnography was selected as the most appropriate methodology because it allows both the interpretation and conceptualisation of how people experience a phenomenon and to build a theoretical understanding that extends beyond findings of individual studies, retaining the original interpretations within its analysis.43-45 This method distinguishes itself from other qualitative synthesis methods by re-interpreting authors’ conceptual constructs alongside primary participant data through a synthesis process, enabling the development of higher-order themes that extend beyond individual study findings. 46 It is therefore particularly congruent with our focus on people with PD and carers, as it allows us to capture the complex and relational realities of mobility loss and its intrinsic link to the experience of PD. Our focus is on the lived experiences of PD and mobility loss from the perspective of the person with PD and carers. This method is well suited to synthesising lived experiences as it preserves the interpretive depth and contextual richness of qualitative studies.
Phase 2: Deciding What is Relevant
Studies were included if they explored the lived experience of mobility loss in PD from the perspective of people with PD and/or the experiences of cares supporting a person with Parkinson’s-related mobility loss. The phenomenon of interest was defined as the impact of mobility loss on independence and/or psychosocial wellbeing in people with PD and carers. For the purpose of this review, mobility loss was considered as factors directly affecting freedom of movement, such as impaired walking, freezing of gait, balance difficulties, falls, and related challenges in physical movement. Eligible participants included people diagnosed with PD and carers of people with PD. Studies where mobility loss was attributable to conditions other than PD were excluded. Methodologically, qualitative studies and mixed-methods studies with a predominant qualitative focus were considered. Mixed-methods studies were included only when qualitative findings were reported separately. Exclusively quantitative studies, systematic reviews and meta-analyses were excluded. Only studies in written in the English language were considered.
A comprehensive search strategy was developed by the research team with no specialist involvement and was explicitly guided by the research question. Key concepts included Parkinson’s disease, caregiving, mobility impairment, psychosocial wellbeing, independence, and lived experience. Searchers used different variations of vocabulary to capture population, including combinations of Parkinson with caregiver, carer, and related variants. Additional search terms captured context such as mobility-related constructs (eg, mobility, gait, walking, combined with issues, impairment, or loss) and psychosocial outcomes (eg, psychosocial wellbeing, psychosocial functioning, independence, activities of daily living and quality of life). All qualitative study designs and methodologies were eligible, as were the qualitative components of mixed-methods studies provided that qualitative findings were reported distinctly. This included search terms such as qualitative, interview, focus group, mixed-methods, perception and lived experience.
A systematic search was then conducted by one reviewer (MH) across six health databases: Medline, PsychInfo, Embase, Web of Science, Scopus and CINAHL. The search was not limited to a specific timeframe and all relevant studies conducted up until November 2024 (ie, date of the search) were considered.
Methodological quality of eligible studies was assessed using the NICE quality appraisal checklist. 47 This was done to assess conduct, content, utility of findings within each study, and to make the strength and weaknesses of the evidence based transparent. Appraisal was not used as a basis for exclusion but rather to provide a framework for interpreting findings. This approach was chosen because methodological limitations in reporting does not necessarily indicate low-quality research, and excluding studies based on strict appraisal criteria would have risked omitting valuable insights. 48
Phase 3: Reading Through the Studies
Study Characteristics.
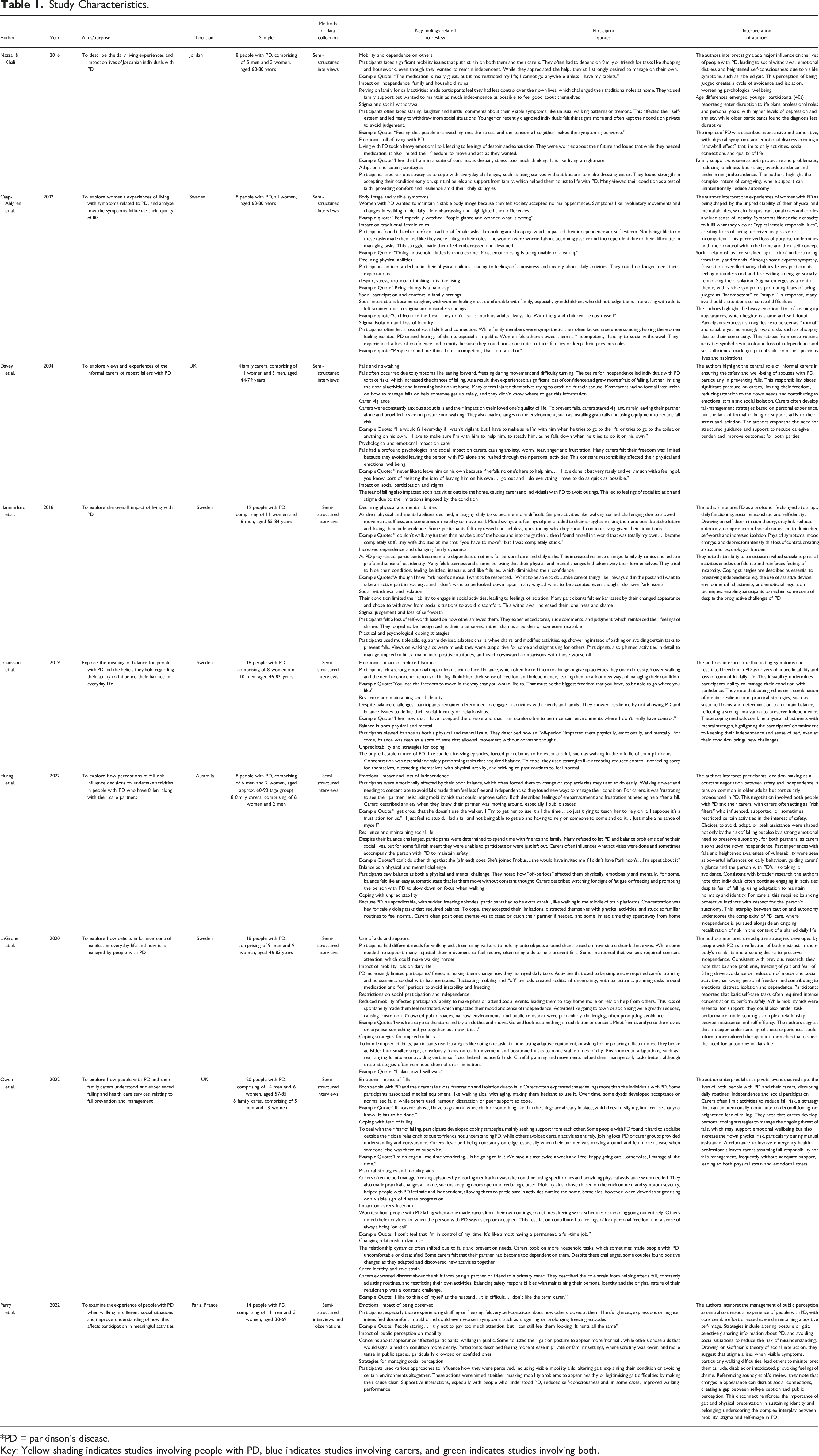
*PD = parkinson’s disease.
Key: Yellow shading indicates studies involving people with PD, blue indicates studies involving carers, and green indicates studies involving both.
Phase 4 and 5: Determining How Studies Are Related and Translating the Studies Into One Another
We aimed to establish how the included studies are related by systematically comparing their findings. One reviewer (MH) identified first-order constructs (ie, direct participant quotes) and second-order constructs (authors’ interpretation). This involved exploring and grouping together recurring themes and perspectives that emerged across studies, focusing on mobility loss and its impact on people with PD and carers. The emerging constructs were then discussed within the wider team to support triangulation, enhance credibility and ensure rigour in interpretation. Once we identified concepts that aligned with each other, we integrated findings to create a broader, shared understanding of mobility loss on PD. Where studies presented differing or contradictory interpretations, the inconsistencies were explored, and we included a more nuanced understanding of the phenomenon.
Phase 6: Synthesising Translations and Expressing the Synthesis
After translating the studies, MH synthesised the key constructs to create third-order constructs, with iterative review and feedback from the wider research team, that represented new interpretations that extend beyond the original findings. This phase focused on detailing the varying perspectives, both from people with PD and carers, to generate a shared understanding of the physical, emotional, and social effects of mobility loss. We identified overarching themes which are articulated below in a comprehensive account of the impact of mobility loss in PD.
Results
Following database search, 841 records were identified. Nine qualitative studies were included in the meta-ethnography, following the screening process (see Figure 1). Regarding methodological quality, the included studies were deemed appropriate (see Appendix A). PRISMA flow diagram.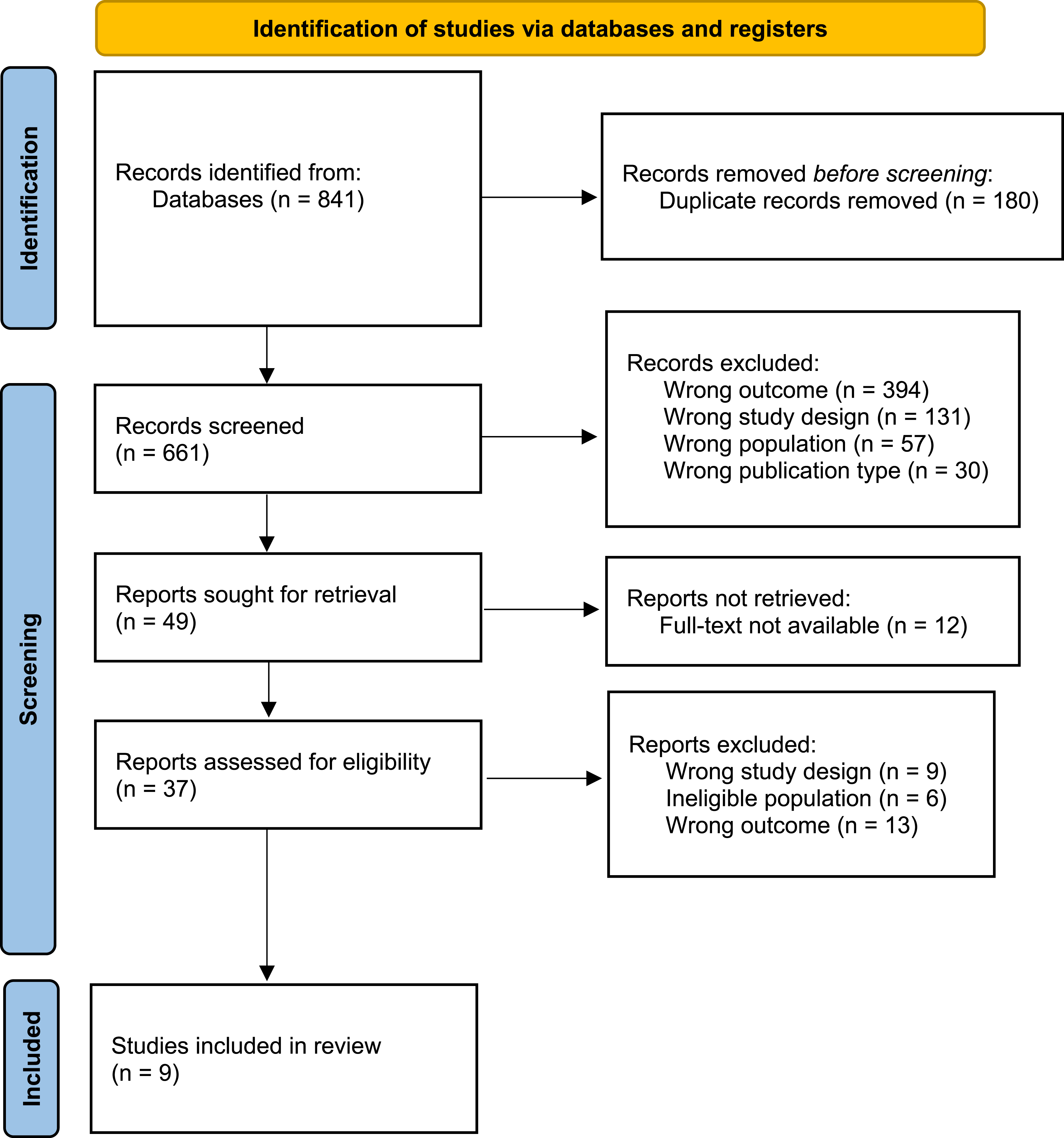
All studies covered the experience of mobility in PD, and three included perspectives from informal carers. Among the 153 participants, 113 were people with PD and 40 were family carers, ages ranged from 30-90 years, with an equal representation of men (48%) and women (52%). Ethnicity was scarcely reported; most represented primarily Western or European populations, with one study focusing on a Middle Eastern (Jordanian) group. See Table 1 for further details.
Analysis of Findings
Summary of Findings.
Findings for People With PD
The Struggle for Independence and Associated Self-Esteem
Across studies, the impact of mobility loss on diminished independence emerged as a central theme.49-56 As mobility declined, participants expressed a growing lack of confidence in their ability to perform even basic activities of daily living, which directly affected their sense of independence. This decline in physical capability often led to feelings of incompetence and emotional distress.54,56 The reliance on assistance for routine tasks was frequently experienced as a direct challenge to their identity and self-perception as capable people. 52
As participants with PD faced increasing difficulty with functional movements such as walking, standing, and moving around the house, household and self-care responsibilities gradually shifted to family members. 53 Mobility limitations were frequently cited as the main reason for this shift, as participants grew to distrust their body’s reliability, leading to feelings of restricted freedom and a loss of identity, especially when mobility aids or assistance became necessary for safety.50,52,56 Impaired balance and the associated risk of falls also led people with PD to modify or avoid activities which, though necessary for safety, highlighted the progressive nature of their condition and diminished their sense of autonomy.50,51 This loss of independence was especially challenging for women, as relinquishing control over household tasks affected their self-esteem and self-worth. 54 This challenged their sense of femininity, as they could no longer maintain the household or their physical image in the way they once had.
The desire to maintain independence sometimes led participants to take risks, such as attempting to perform certain activities without assistance. While this may have temporarily boosted self-esteem, it also increased the risk of falls, posing both physical and emotional risk such as feelings of helplessness and dependency. 56 Conversely, in other cases, the fear of falling resulted in a reluctance to engage in physical activities altogether, whether by personal choice or following advice from their carer. This fear further intensified participants dependency on others,49,55,56 creating a cyclic relationship between mobility loss, dependence, and reduced self-esteem.
Navigating Personal Relationships
Social interactions, particularly beyond the immediate family, were often limited. Some participants mentioned that their friends lacked an understanding of the physical challenges posed by PD, which made socialising difficult and strained friendships.49,54 However, for many, family support was instrumental in helping them adapt to their mobility challenges. 53 That said, the desire to maintain independence persisted; participants tried to balance between seeking support while striving for autonomy. 53 This balancing act was complex, as mobility impairments often fluctuated, causing frequent adjustments in the level of support needed.
Despite these difficulties, people with PD showed resilience in their efforts to engage socially. 51 Some found that the emotional support provided by family and friends could temporarily ease their mobility difficulties, such as reducing anxiety during social interactions, which in turn improved their gait and confidence in their mobility. 57
Perceived Stigmatisation and Social Isolation
Mobility impairments in PD often lead people with PD to feel perceived differently by society due to visible symptoms such as impaired gait, tremors, and other motor dysfunctions. This fear of stigma was a recurring theme, with many participants reporting social withdrawal and psychological distress due to the public’s reaction to their symptoms, such as staring, laughing, or hurtful comments.50,52-57 Embarrassment over their physical limitations led some participants to avoid social situations, fearing judgment or misunderstanding, while others actively tried to conceal their condition or avoided mobility aids like walking sticks, despite the increased fall risk.51,57 The effort to manage how others perceived their mobility became a constant challenge, with some participants adopting strategies such as using a cane to ‘legitimise’ their walking problems,50,57 which they found emotionally difficult to accept. For many, the stigma attached to these visible symptoms was isolating, with participants describing how being seen as “incompetent” or even “like an idiot” diminished their self-worth. Some even adjusted their posture or “gait image” to manage perceptions yet still struggled with feelings of shame and a loss of identity. 54
The unpredictability of symptoms, such as the sudden shift between “on” and “off” periods, further complicated social participation. People with PD worried about the possibility of freezing or falling in public, which often left them feeling excluded or isolated. 54 This led many to avoid social events altogether, creating a cycle of isolation that had a profound impact on the psychosocial wellbeing.
Resilience and Adaptation
Psychological Impact
People with PD frequently reported heightened anxiety, depression, and a persistent sense of loss as their mobility declined. The physical limitations imposed by PD often led to significant psychological toll, with concerns primarily focused on the progression of the condition, the physical deterioration comes with it and worries about what the future may hold. 52 The fear of losing the ability to walk independently, the increased risk of falls, and the dependency on others for basic mobility-related tasks contributed to feelings of helplessness and despair.
For many participants, their self-esteem and sense of identity were closely tied to their ability to move independently, and the gradual loss of this ability amplified feelings of anxiety and depression.50,53 Mobility impairments were a constant reminder of the progressive nature of PD, leading to persistent worries about how their condition would affect their future quality of life, ability to engage in social activities, and maintain independence.50-53
Adaptations to Living With PD
For people with PD, developing adaptation strategies was essential for maintaining a sense of independence and quality of life, especially amid increasing mobility challenges. These adaptations were both physical and cognitive, designed to help manage with daily activities and minimise the risk of falls, while also addressing the emotional challenges that come with the progressive decline in mobility.
Physical Adaptations
Mobility aids, such as walking sticks, walkers, and wheelchairs were commonly used by people with PD to assist with daily activities and provide stability during movement.50,52,57 These aids were vital for preventing falls and maintaining a level of independence, especially when navigating uneven terrain or crowded spaces. 49 Additionally, people with PD would often plan their activities around their “on” periods, when their mobility was less restricted due to the effects of the medication, ensuring that more physically demanding tasks were done when their movement was more reliable.50,51 For many people with PD, modifying the environment, such as rearranging furniture to create clear walking paths or installing grab rails, was another important strategy to help reduce the risk of falls within the home.49,55
However, while these physical adaptations were necessary for safety and functionality, they also served as a reminder of the progressive nature of PD. The constant need for aids and adjustment often reinforced the reality of declining physical abilities. 56 For some people with PD, using mobility aids, although beneficial, was perceived negatively because it signalled their disability, impacting their self-esteem and psychological wellbeing.49,52,56 This strain between the need for physical assistance and the desire for independence was a recurring emotional challenge for people with PD.
Psychological Adaptations
To cope with the emotional toll of mobility loss, people with PD often adopted various psychological strategies. Maintaining a positive outlook and accepting their physical limitations were key factors in preserving emotional resilience. 52 People with PD who were able to find comfort in spirituality, family support, or social networks were better equipped to manage the psychological impact of their condition. 53 The involvement of family members, who often provided both emotional and practical support, played a crucial role in helping people with PD navigate daily life, even as they sought to maintain their independence.53,56
For some participants, continuing to engage in physical activities that were once part of their daily routine, albeit adapted, provided a sense of normalcy, and helped counteract feelings of helplessness. 57 These adaptations allowed them to continue participating in meaningful activities while minimising the risk of falls. However, despite these adjustments, many people with PD still experienced ongoing frustration and emotional distress due to their progressive mobility impairments. 52
Findings for Carers
Impact of Mobility on Carer Wellbeing
Mobility impairments in people with PD significantly increase the burden on carers, creating both physical and emotional strain. The physical demands of assisting their care partner, particularly in preventing or responding to falls, place carers under immense pressure. Many carers felt they had to remain constantly vigilant, always on alert to prevent falls, which created ongoing anxiety and worry. 55 This constant state of alertness restricted their own personal outings, contributing to a sense of loss and isolation, as carers often felt they could not possibly leave the person with PD one alone for extended periods due to fear of falls.49,56
Falls or the risk of falling were a primary concern. Carers, especially female carers, reported feeling physically vulnerable when trying to assist their care partner, particularly after a fall. The task of lifting or supporting someone with impaired mobility often felt overwhelming, and some feared injuring themselves in the process. 49 This concern was further compounded by the unpredictable nature of PD symptoms, such as freezing episodes, which often necessitated immediate physical assistance, placing both the carer and the person with PD at risk of injury. 55
The emotional toll of this constant vigilance was significant. Carers frequently expressed feelings of exhaustion and emotional depletion, worsened by the lack of personal time or breaks from their caregiving role. Adjusting daily activities to prevent falls, such as modifying the home environment by keeping doors open or reducing clutter, became routine but also deepened the sense of responsibility. 49 While these adaptations were necessary, they often reinforced feelings of dependency for the person with PD and heighted the emotional burden for the carer. Carers experienced frustration and isolation as their social activities and daily routines were increasingly shaped by the need to manage mobility-related challenges. 56
This constant management of mobility impairments not only reshaped daily activities but also strained the emotional dynamics within the dyadic relationship. For many carers, the increasing physical demands of assisting with mobility, such as helping with walking or preventing falls, reshaped their sense of identity, making them feel defined by their caregiving role. As they took on more domestic responsibilities and focused on the mobility needs of the people with PD, carers often experienced feelings of resentment, particularly when they perceived that the person with PD was overly dependent on them. 49 Despite the challenges, some carers found moments of resilience and emotional connection, especially when adapting activities to maintain a sense of normalcy and shared time together. 49 However, these positive moments were less frequently reported and were dominated by the overwhelming demands of caregiving.
Comparison of Experiences Between People With PD and Carers
The experiences of people with PD and carers showed notable commonalities as well as important difference, reflecting the interconnected yet distinct ways mobility challenges shape daily life. These relationships are brought together in Figure 2, which exhibits a model of mobility-related impact in PD integrating the perspectives of both groups into a single conceptual framework. In this model, people with PD and carers experience shared impacts, such as loss of independence, emotional strain, social isolation, adaptation and resilience. This also highlights the reciprocal influence between both groups; for example, as people with PD lose independence through mobility loss, carers take on greater responsibility, which could then restrict the autonomy of the person with PD. Dyadic model of mobility-related impact in PD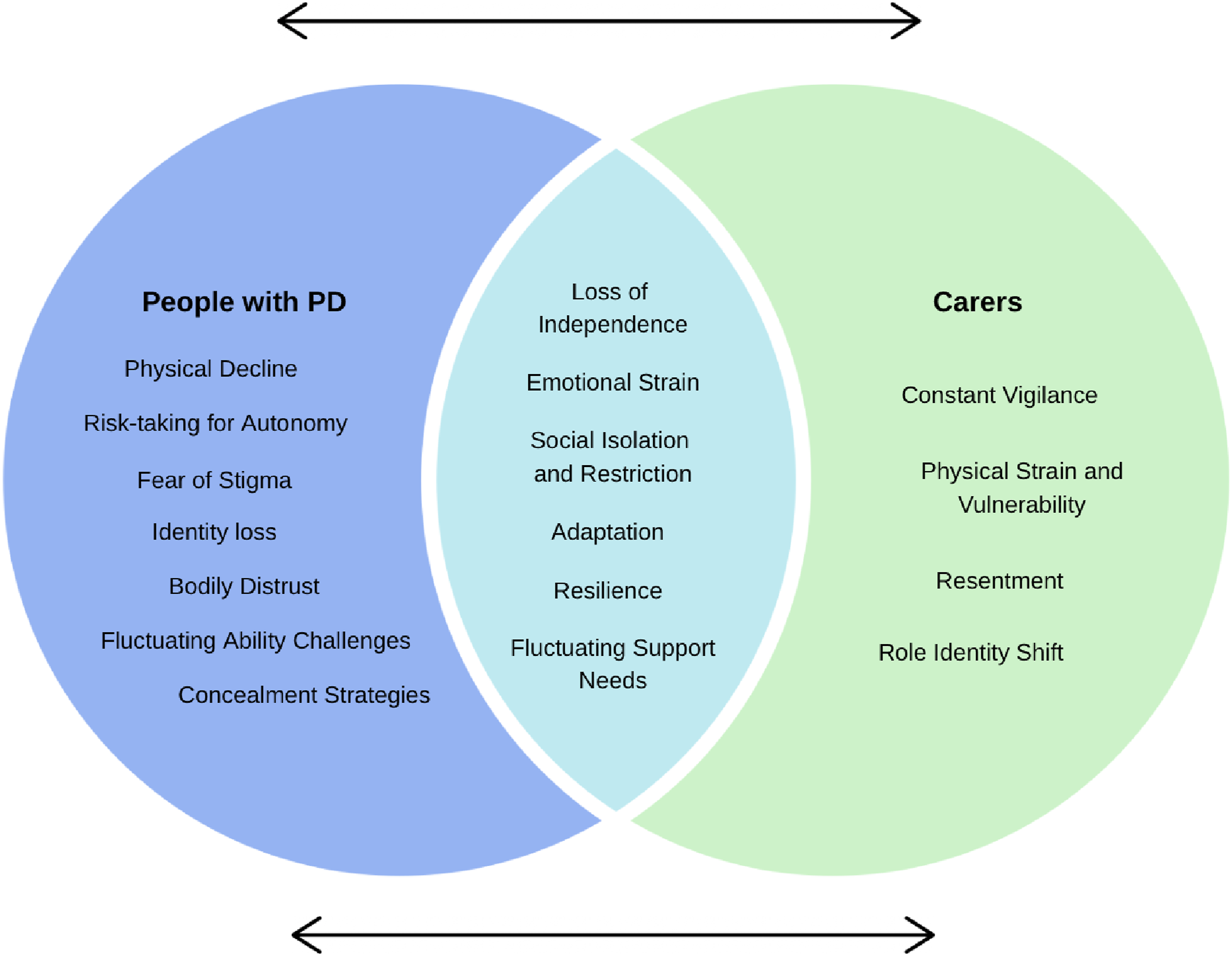
Despite these commonalities, the underlying source and how they were experienced varied. For people with PD, the impact stemmed primarily from mobility loss, fear of stigma, and the tension between maintaining autonomy and managing safety. Whereas for carers, the strain was caused by constant vigilance, physical demands, and a shift in role identity. Risk was also perceived differently, people with PD sometimes took physical risks to preserve their autonomy, while carers were more likely to limit activities to reduce fall risk. Gendered patterns emerged in both groups; women with PD often linked mobility loss to the loss of traditional household roles and self-image, and female carers described physical vulnerability when providing assistance with mobility.
Although a refutational synthesis identified few direct contradictions across participants, some differences emerged within the accounts of people with PD. These included responses to fall risk, with some participants taking physical risks to preserve independence and self-esteem, while others avoided certain activities altogether due to fear of falling or advice from carers. Perception of mobility aids also varied, as some participants viewed them as tools to maintain safety and independence, while others perceived them as stigmatising symbols of disability which negatively affected self-image. Approaches to social participation also slightly differed. Many withdrew completely from social settings due to embarrassment or stigma, whereas others remained active in the community, but often making efforts to conceal their symptoms. Similarly, experiences were quite consistent across carers, however some differences still emerged. The experience of physical strain only came up with female carers, they described feelings of physical vulnerability when assisting with mobility or after a fall, while others focused more on emotional or practical challenges. Emotional responses to the carers’ role also differed, with some expressing frustration, exhaustion or resentment, while a few focused on resilience and emotional connection. So, while the overarching impacts of mobility change are widely shared, the ways in which people experience and respond to these challenges can differ considerably.
Discussion
This meta-ethnography is the first to synthesise literature that provides a detailed account of the impact of mobility loss in people with PD and the experiences of carers managing the associated physical and emotional challenges. Across studies, findings consistently emphasised that mobility loss has significant consequences for both the independence and psychosocial wellbeing in people with PD. Common themes included loss of autonomy, increased reliance on carers, and the emotional strain associated with mobility loss. These findings echo earlier research linking reduced mobility to diminished quality of life and increased emotional distress in people with PD, due to the growing dependency on others for everyday activities.58,59 However, our synthesis extends existing knowledge by integrating the perspectives of carers, who described constant vigilance, physical strain and restrictions to their own independence as key consequences of supporting a person with mobility loss. Previous studies have found that the carers’ psychosocial wellbeing is associated with the person with PD’s ability to remain mobile. 60 Studies examining the caregiving experience in PD also highlight the significant influence of non-motor symptoms, particularly cognitive impairment and the burden of treatment on carer wellbeing. 61 Taken together, these findings highlight mobility loss as a shared challenge; however, less is known qualitatively about how mobility is experienced by these groups and how it impacts the quality of life of both the person with PD and the carer.
The unpredictability of PD symptoms, such as the sudden shift between “on” and “off” periods, emerged as a persistent challenge that complicated social participation and highlighted a distinctive aspect of PD compared with other progressive conditions. This unpredictability is evident throughout the themes, impacting both the person with PD and the carer. For people with PD, abrupt mobility changes made it challenging to engage in social and everyday activities with confidence, often contributing to social withdrawal. For carers, fluctuating care demands required continuous adaptation and resulted in cumulative physical and emotional burden. These findings underline the need for flexible, dyadic care models that challenge traditional patient-centred approaches and adapt to the unpredictable nature of PD whilst also supporting both people with PD and their carers. Models that recognise the person with PD and the carer as an interconnected unit in which changes in mobility directly influence carer burden, emotional wellbeing, physical health and social participation. 62 And further, care models that extend beyond physical symptom management to incorporating more holistic support.62,63 This would require health care professionals to acknowledge reciprocal impacts within the dyad, support people with PD to remain socially engaged despite mobility fluctuations and also recognise carers as care recipients alongside patients within care planning. To capture these interlinked experiences, we developed a model demonstrating mobility-related impact in PD, which integrated the perspectives of both people with PD and carers. This model illustrates the shared impacts, eg, loss of independence, emotional strain, social isolation and adaption, as well as the unique challenges faced by each group. It also highlights the reciprocal influence between people with PD and their carers.
Clinically, the findings support the need for holistic, person-centred approaches that address not only the physical challenges of mobility loss but also the psychosocial impacts that accompany it. For people with PD, mobility loss is intertwined with identity, social participation and emotional resilience. There is a significant proportion of interventions targeted at people with PD, through national (eg, Parkinsons UK) and international (eg, Michael J Fox Foundation), third sector organisations, and self-management programmes through the digital sphere. 64 However, carers of people with PD appear not to receive the same attention and opportunities, despite evidence of carer burden, and in contrast to other neurological conditions (eg, dementia) where national care guidelines include specific recommendations for carer wellbeing and support.65,66 And yet, we know that carers play a dynamic and imperative role within the care plan for someone with PD. 65 As this meta-ethnography has shown, mobility loss alone leads to a significant burden for carers coupled with previous reports in the literature of the impact of non-motor and other components of PD and its impacts.19,25-28,39-41 These findings show the need for targeted interventions for carers, including education on managing mobility related risks in their care partner, for example falls and falls related consequences and psycho-social support addressing their own health and social isolation.
This review highlights how mobility loss and its fluctuations shape the daily lives of people with PD and carers, influencing independence, safety, social participation and emotional wellbeing. While the included studies did not examine technological solutions directly, the challenges identified, particularly the unpredictability of mobility changes and the impact on planning and safety, suggest potential value in tools that monitor and communicate mobility patterns over time.67,68 For example, wearable devices have been explored in other contexts to provide continuous, objective data on movement, supporting more complex assessments. 69 If designed in collaboration with people with PD and carers, such tools could help better anticipate periods of reduced mobility, support carers in planning assistance and inform more responsive clinical care. 70 Further qualitative research could explore the acceptability and perceived usefulness of these approaches, ensuring that any future digital innovations are grounded in lived experience.
While most of the included studies focused on the perspectives of people with PD, a smaller number explored carers’ experiences. This imbalance mirrors a broader trend in PD research, where the focus on informal carers is often limited despite their essential role in supporting people with PD. 71 This pattern is further consistent with wider structural under-recognition of carers within PD care pathways. 65 Practical and emotional barriers may also contribute to this underrepresentations, as carers frequently report time constraints, stress and priority of caregiving over research involvement. 72 Together, these challenges likely contribute to the limited qualitative evidence base. Given that mobility loss in PD affects the entire caregiving dynamic, the lack of carer-focused evidence represents a significant gap in the literature and an important area for future research.
Limitations
The primary limitation of this review is the predominance of studies from Westernised contexts and lack of reporting on inclusion of under-served groups such as ethnic minorities and low socio-economic status, which may not fully capture the diverse cultural and economic dynamics that influence caregiving and the experience of mobility loss in PD. Cultural variations and economic disparities in caregiving roles, health care access, and societal support systems are likely to shape the experience of both people with PD and carers differently.73,74 Thus, future research should aim to incorporate a broader range of cultural contexts to gain a more comprehensive understanding of the challenges posed by mobility loss across different populations. Additionally, there is a notable lack of studies involving formal carers, such as professional health care workers. Their perspectives are critical, as they frequently manage mobility impairments in more advanced stages of PD in clinical settings, offering insights into how mobility loss is addressed differently in institutional care environments compared to home settings. 75 Including formal carers in future research could provide a more complete picture of the caregiving experience and lead to better-informed interventions for both informal and professional carers. We also note that some included studies were published over 20 years ago, and may therefore capture perspectives that do not reflect the current day’s experience of PD. However, including all relevant studies without date restriction allows us to understand the full breadth of literature, and older studies can provide valuable and foundational insights into experiences that remain relevant today.
Conclusion
This meta-ethnography highlights the significant and multifaceted challenges associated with mobility loss in PD for both people with PD and carers. Mobility impairments not only diminish independence of people with PD but also place a considerable emotional and physical burden on carers. The findings emphasise the interconnected nature of these challenges, revealing that the loss of autonomy and increased dependency due to mobility limitations severely affect the psychosocial wellbeing of both groups. These insights reaffirm the need for capturing real-time data on mobility comprehensive, individualised interventions that address both the physical and emotional aspects of caregiving and patient care in PD. Wearable devices, such as those that monitor DMOs, offer promising avenues to enhance care by providing real-time data on mobility patterns, enabling personalised interventions, and supporting both carers and people with PD in managing mobility fluctuations more effectively. Exploring their potential offers an exciting direction for future research. This review also identifies notable gaps, particularly the lack of representation of non-Western cultural contexts and the absence of perspectives from formal carers. Addressing these gaps in future research is crucial to develop a more globally relevant understanding of caregiving in PD.
Supplemental Material
Supplemental material - Impact of Mobility Loss on Independence and Psychosocial Wellbeing in People With Parkinson’s Disease and Carers: A Meta-Ethnography
Supplemental material for Impact of Mobility Loss on Independence and Psychosocial Wellbeing in People With Parkinson’s Disease and Carers: A Meta-Ethnography by Megan Hanrahan, Cameron Wilson, Lynn Rochester, Alison Keogh, Ríona Mc Ardle and Katie Brittain in Journal of Geriatric Psychiatry and Neurology
Footnotes
Author Contributions
MH was involved in the conceptualisation, methodology, investigation, data curation, formal analysis, and writing – original draft. CW was involved in the conceptualisation, methodology, investigation, data curation, and writing – review and editing. AK, RMA and KB were involved in conceptualisation, supervision, funding acquisitions and writing – review and editing. LR was involved in in conceptualisation, funding acquisitions and writing – review and editing.
Declaration of Conflicting Interests
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by the NIHR Newcastle Biomedical Research Centre (BRC) and The Michael J. Fox Foundation for Parkinson’s Research (100000864-MJFF-022736). RMA is funded by the National Institute for Health and Care Research (NIHR) (NIHR301677, 301677). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, the Department of Health or any other funder.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analysed for this study.
Supplemental Material
Supplemental material is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.