
Abstract
Background
Women with Parkinson’s disease (PD) are less likely to have a caregiver.
Objective
To determine factors contributing to gender disparities in PD caregiving.
Methods
We conducted a cross-sectional survey of people with PD and caregivers participating in the Parkinson’s Foundation Parkinson’s Outcomes Project and compared patient and caregiver characteristics by gender.
Results
Among PD patients, 20.7% of 1663 women and 14.2% of 3005 men had no caregiver (P < 0.001). Women without caregivers were older (69.1 vs 66.3, P < 0.001), less likely to be married (30.4% vs 54.7%, P < 0.001), and more likely to be taking an antidepressant (41.8% vs 30.9%, P = 0.002) than men. Using stepwise logistic regression models, gender differences in access to caregiving were explained by marital status. Among caregivers, women reported more strain (P < 0.001) and had less time for other family members (P < 0.001).
Conclusion
Fewer women with PD have caregivers because they are less likely to have a spouse.
Plain Language Summary
Caregivers play a vital role in the lives and health of people with Parkinson’s disease (PwP). However, women with Parkinson’s disease (PD) are less likely to have a caregiver and are more likely to be a caregiver themselves. Furthermore, women caregivers for PwP are more likely than men to feel burnout due to caregiving. This study examines potential reasons for these gender-related differences in PD caregiving. To better understand the experiences of caregivers, surveys were given to caregivers of PD patients who receive care at Parkinson’s Foundation Centers of Excellence in the United States. Our findings show that women without caregivers are older, less likely to be married, and have higher rates of depression. Marriage is by far the strongest predictor for having a caregiver. Among PD caregivers, women (1) care for PwP who are more disabled, (2) have more burnout, and (3) sacrifice more of their time with other family members. More research is needed to identify ways to better support PwP and their caregivers.
Introduction
Parkinson’s disease (PD) causes impairment in motor function as well as numerous non-motor symptoms such as dementia, depression, and psychosis. The motor and non-motor features collectively contribute to disability, particularly with advancing disease.1,2 People with Parkinson’s disease (PwP) need more help from others as the disease progresses, and informal (unpaid) caregivers are integral to the care of PwP.3,4 By late-stage PD, patients have complete loss of independence and are very dependent on caregivers for daily functioning. 5 Caregivers are an understudied part of the Parkinson’s disease care team, and more research is needed regarding caregiver responsibilities and needs.
There are 53 million informal caregivers in the United States. 6 They provide most of the care for individuals with serious illness living in the community and access to informal caregivers improves outcomes and delays time to institutionalization.7-9 Among PwP, caregivers are instrumental in tasks such as getting patients to appointments, managing medications, and reporting new issues to the medical team. However, caregivers typically have few resources and support to aid in this important task. 10
Furthermore, significant gender differences in caregiving exist. Disabled women are less likely to receive informal caregiving and have higher rates of nursing home placement than men.11,12 Women have less access to caregivers at the end-of-life and gender disparities permeate numerous aspects of end-of-life care. Women are more likely to outlive their spouses and live alone at the end of life, with fewer informal caregivers and resources left to care for them. Women are also more likely to accept formal care to avoid being a burden, a sentiment potentially influenced by prior life experience as a caregiver themselves. 13 Similarly, women with PD have less access to informal caregivers, with 88.4% of men vs 79.4% of women having a caregiver. 14 Women with PD are also more likely to hire paid caregivers and are more likely to be caregivers themselves; moreover, women caregivers report higher caregiver strain. 14 The mechanisms for these gender disparities are unknown though prior research suggests that differences in caregiver demographics may contribute. 11 Across cultures and health conditions, women provide most of the informal care for people with chronic medical conditions, and women may adopt this caregiving role due to societal and cultural expectations and demands traditionally placed on women.6,15,16 Most caregivers of elderly disabled patients in general are women, with children as the dominant caregivers for disabled women and wives as the dominant caregivers of disabled men.11,17
Determining contributors to gender disparities in PD caregiving can identify areas amenable to intervention and inform healthcare policy. We evaluated potential contributors to gender disparities by surveying PwP and their caregivers.
Materials and Methods
Standard Protocol Approvals and Patient Consents
The protocol was approved by the Institutional Review Board at each site prior to participant recruitment and written informed consent was obtained from both PwP and caregivers. Caregivers who participated in the additional sub-study signed an additional written informed consent form.
Study Design and Sample
We surveyed caregivers of PwP using participants drawn from the Parkinson’s Foundation Parkinson’s Outcomes Project (PF-POP), which is an ongoing, prospective, observational study of PD that annually assesses health outcomes among participants with PD and their caregivers. The study is conducted at 21 PF Centers of Excellence located in Canada, the Netherlands, Israel, and the United States. 18 Participant enrollment began in 2009, and new participants continued to be enrolled every year through 2023. For this cross-sectional sub-study, a caregiver survey was sent to caregivers of participants at 16 centers in the United States. Surveys were distributed at the discretion of each site by mail, email, and/or in person. A single caregiver was identified by each study participant. Completed surveys were collected during routine study visits from 2016-2018, providing a convenience sample among PF-POP participants. All patients seen at these participating sites for regular PD care were eligible to participate in the study. The primary goal of the study was exploratory, that is, to uncover patterns and relationships.
Measures
The PF-POP collects annual patient and caregiver data from study participants. The caregiver sub-study survey collected self-reported data on caregivers including basic information about the caregiver and patient, amount and type of caregiving provided, Center for Epidemiological Studies Depression Scale (CES-D),19,20 caregiver preparedness scale,21,22 support systems in place, specific needs of the PD patient, Multidimensional Caregiver Strain Index (MCSI), 23 Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) Part II, 24 and overall caregiving experience. Most questions were close-ended, with the exception of one open-ended question. Participants were asked to self-identify their gender by selecting either “Male” or “Female” on the survey. The survey (excluding the standardized questionnaires) is provided as Supplemental data. We used the STROBE cross sectional checklist when writing our report. 25
Analysis
Descriptive statistics were used to characterize the participants and quantify any missing data. Next, t tests were used for continuous variables with normally distributed data, Wilcoxon rank-sum tests for non-normally distributed continuous data, and χ2 tests for categorical variables, to compare demographic and caregiving characteristics by gender of caregivers and patients. The ANOVA test was used to compare normally distributed continuous data with greater than 2 categories and the Kruskal-Wallis test was used to compare non-normally distributed continuous data with greater than 2 categories. Individuals with missing gender data were omitted from analyses. Bonferroni correction was used to correct for multiple comparisons for the following analyses: (1) comparing baseline characteristics of PwP with and without caregivers, corrected P-value was 0.005; (2) comparing demographic data between men and women without caregivers, corrected P-value was 0.002; (3) comparing demographic data between men and women caregivers, corrected P-value was 0.005; and (4) comparing clinical data between men and women caregivers, corrected P-value was 0.003. Patient comparisons by caregiver gender were viewed as exploratory and a P-value of 0.05 was used. Once univariable correlations were determined, numerous significant individual variables were incorporated into a stepwise multiple logistic regression by iteratively adding meaningful groups of predictors, in order to determine which variables were the most important predictors of the gender disparity in access to a caregiver.
Results
Baseline Characteristics of PwP With and Without Caregivers.
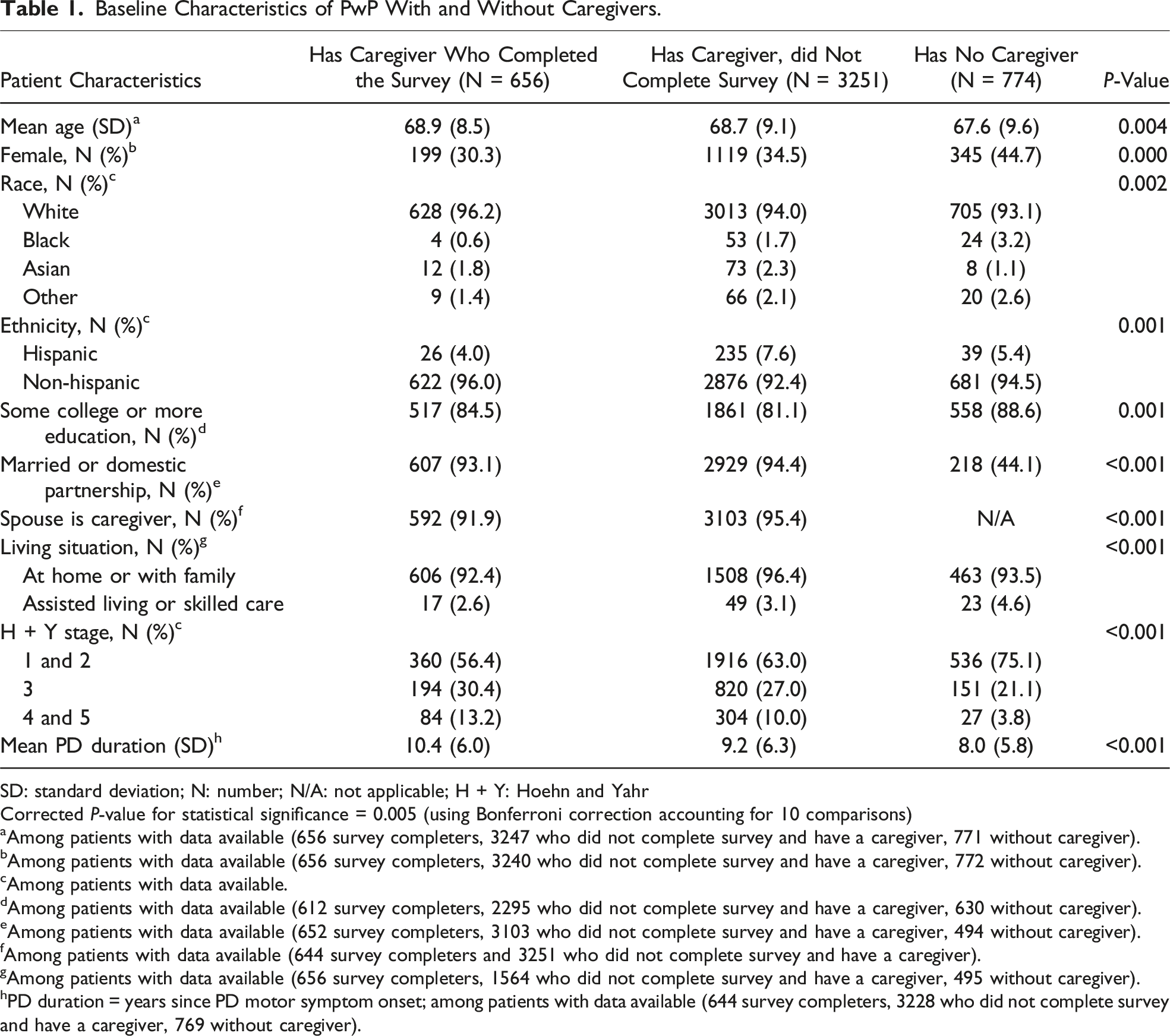
SD: standard deviation; N: number; N/A: not applicable; H + Y: Hoehn and Yahr
Corrected P-value for statistical significance = 0.005 (using Bonferroni correction accounting for 10 comparisons)
aAmong patients with data available (656 survey completers, 3247 who did not complete survey and have a caregiver, 771 without caregiver).
bAmong patients with data available (656 survey completers, 3240 who did not complete survey and have a caregiver, 772 without caregiver).
cAmong patients with data available.
dAmong patients with data available (612 survey completers, 2295 who did not complete survey and have a caregiver, 630 without caregiver).
eAmong patients with data available (652 survey completers, 3103 who did not complete survey and have a caregiver, 494 without caregiver).
fAmong patients with data available (644 survey completers and 3251 who did not complete survey and have a caregiver).
gAmong patients with data available (656 survey completers, 1564 who did not complete survey and have a caregiver, 495 without caregiver).
hPD duration = years since PD motor symptom onset; among patients with data available (644 survey completers, 3228 who did not complete survey and have a caregiver, 769 without caregiver).
Demographic Data of PwP without Caregivers
Characteristics of Female and Male PwP Enrolled in the PF-POP Who Have No Regular Caregiver.
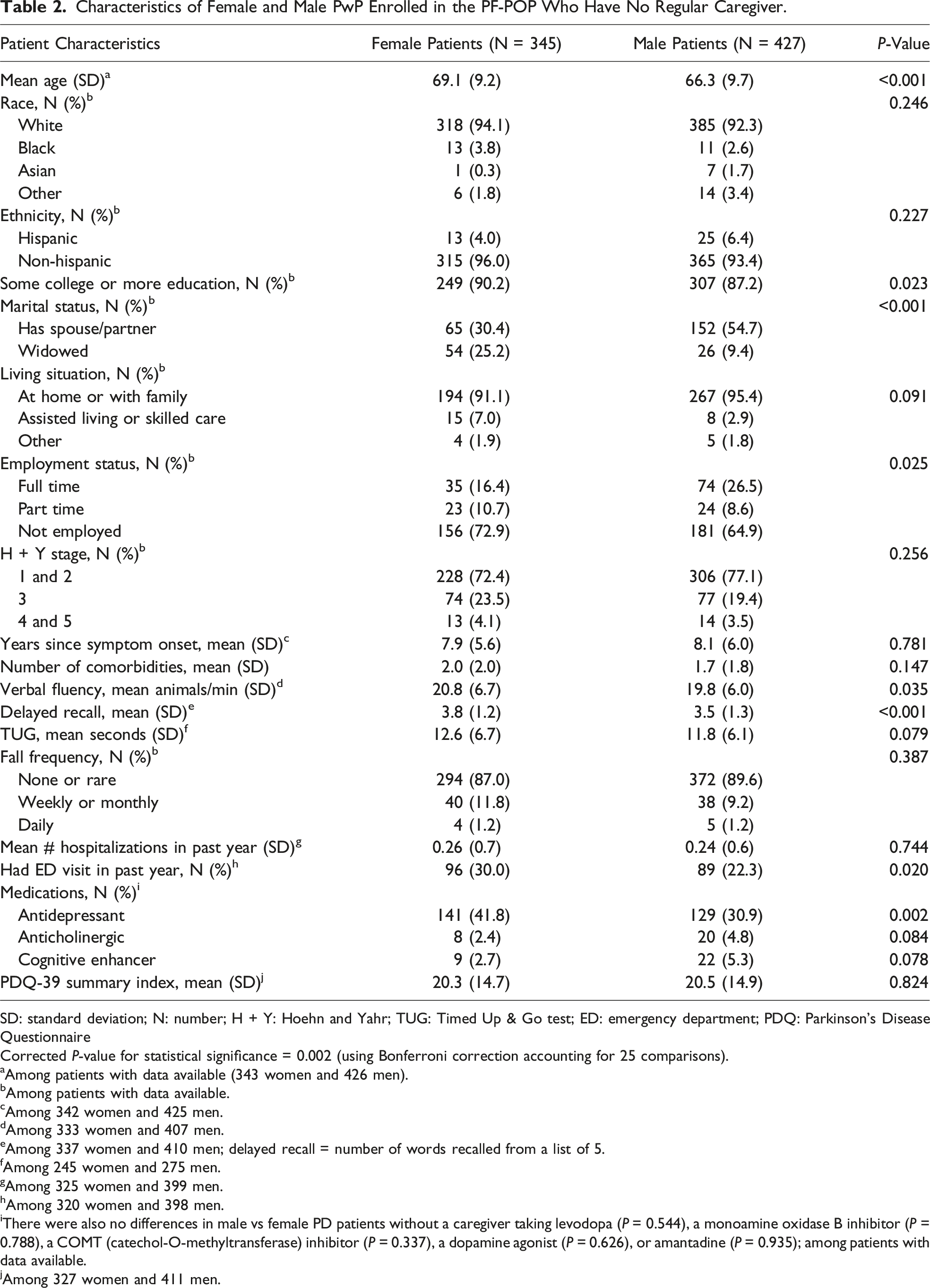
SD: standard deviation; N: number; H + Y: Hoehn and Yahr; TUG: Timed Up & Go test; ED: emergency department; PDQ: Parkinson’s Disease Questionnaire
Corrected P-value for statistical significance = 0.002 (using Bonferroni correction accounting for 25 comparisons).
aAmong patients with data available (343 women and 426 men).
bAmong patients with data available.
cAmong 342 women and 425 men.
dAmong 333 women and 407 men.
eAmong 337 women and 410 men; delayed recall = number of words recalled from a list of 5.
fAmong 245 women and 275 men.
gAmong 325 women and 399 men.
hAmong 320 women and 398 men.
iThere were also no differences in male vs female PD patients without a caregiver taking levodopa (P = 0.544), a monoamine oxidase B inhibitor (P = 0.788), a COMT (catechol-O-methyltransferase) inhibitor (P = 0.337), a dopamine agonist (P = 0.626), or amantadine (P = 0.935); among patients with data available.
jAmong 327 women and 411 men.
Demographic Data of PwP with Caregivers
Among the PwP enrolled in the PF-POP, 1317 women and 2575 men reported having a caregiver. Age is similar between men (mean 68.7 ± 8.8) and women (mean 68.6 ± 9.3) with caregivers (P = 0.621). Men with caregivers are more likely to be married (95.5% vs 90.3%) and less likely to be widowed (0.7% vs 5.1%) than women with caregivers (P < 0.001). While most caregivers are spouses for both men (96.8%) and women (91.1%), women are more often cared for by other relatives (6.5% vs 2.0%) or paid providers (2.2% vs 0.8%, P < 0.001). Men with caregivers are more likely to live at home or with family (95.8% vs 93.9%) and less likely to live in a skilled care or assisted living facility (2.4% vs 4.3%) than women with caregivers (P = 0.046). Women with caregivers have had PD longer than men (mean 9.8 ± 6.4 vs 9.2 ± 6.1 years, P = 0.008) and have poorer quality of life (Parkinson’s Disease Questionnaire (PDQ-39) Summary Index 27.1 ± 17.4 vs 24.0 ± 15.6, P < 0.001). There are no differences in race (P = 0.493), ethnicity (P = 0.147), number of co-morbidities (P = 0.316), or hospitalizations (P = 0.280) between men and women with caregivers.
Stepwise Multiple Logistic Regression
Stepwise Logistic Regression Models and Odds Ratios (95% CI).
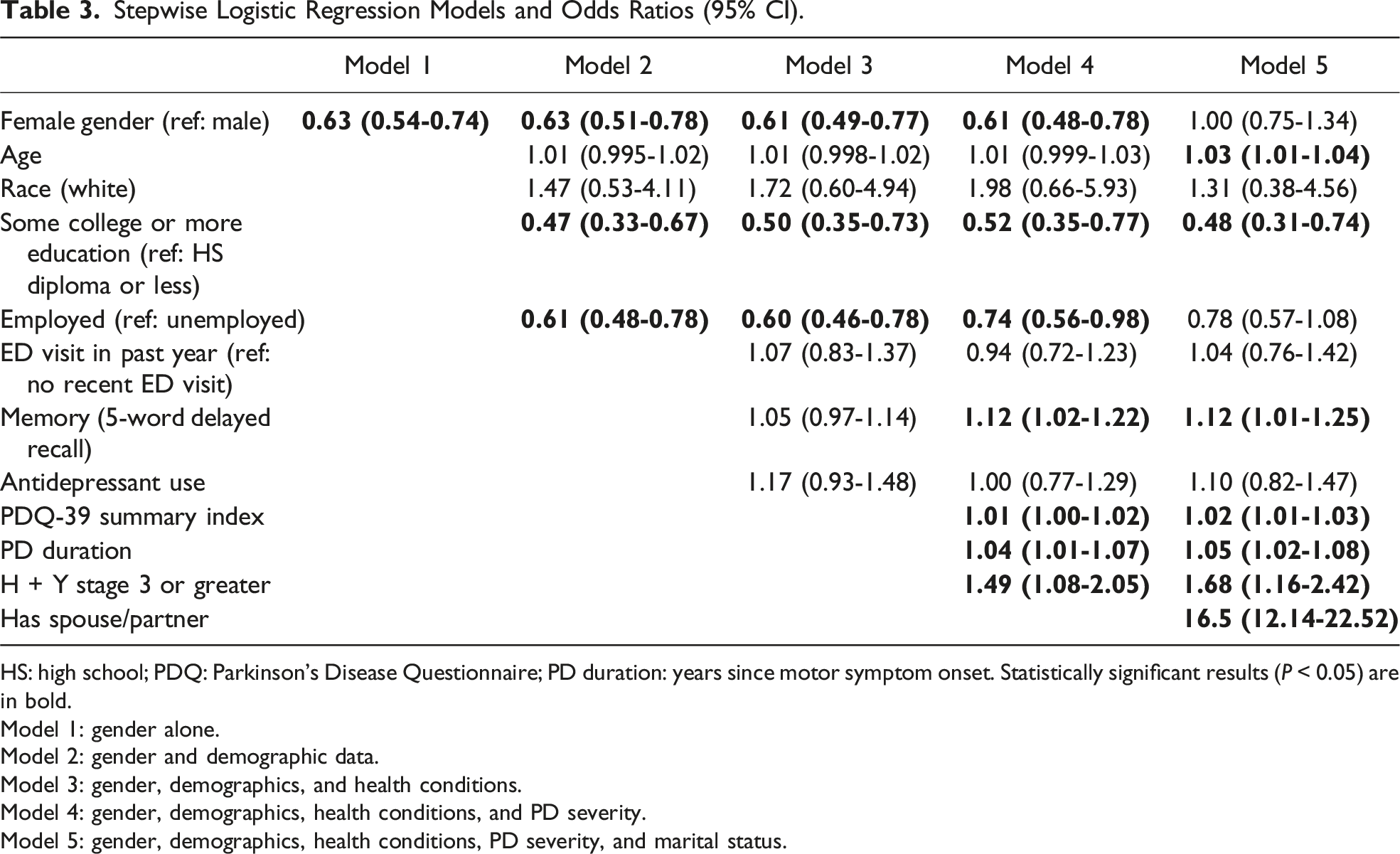
HS: high school; PDQ: Parkinson’s Disease Questionnaire; PD duration: years since motor symptom onset. Statistically significant results (P < 0.05) are in bold.
Model 1: gender alone.
Model 2: gender and demographic data.
Model 3: gender, demographics, and health conditions.
Model 4: gender, demographics, health conditions, and PD severity.
Model 5: gender, demographics, health conditions, PD severity, and marital status.
Demographic Data of Caregivers
Characteristics of Caregivers Who Participated in the Caregiver Survey Sub-Study.
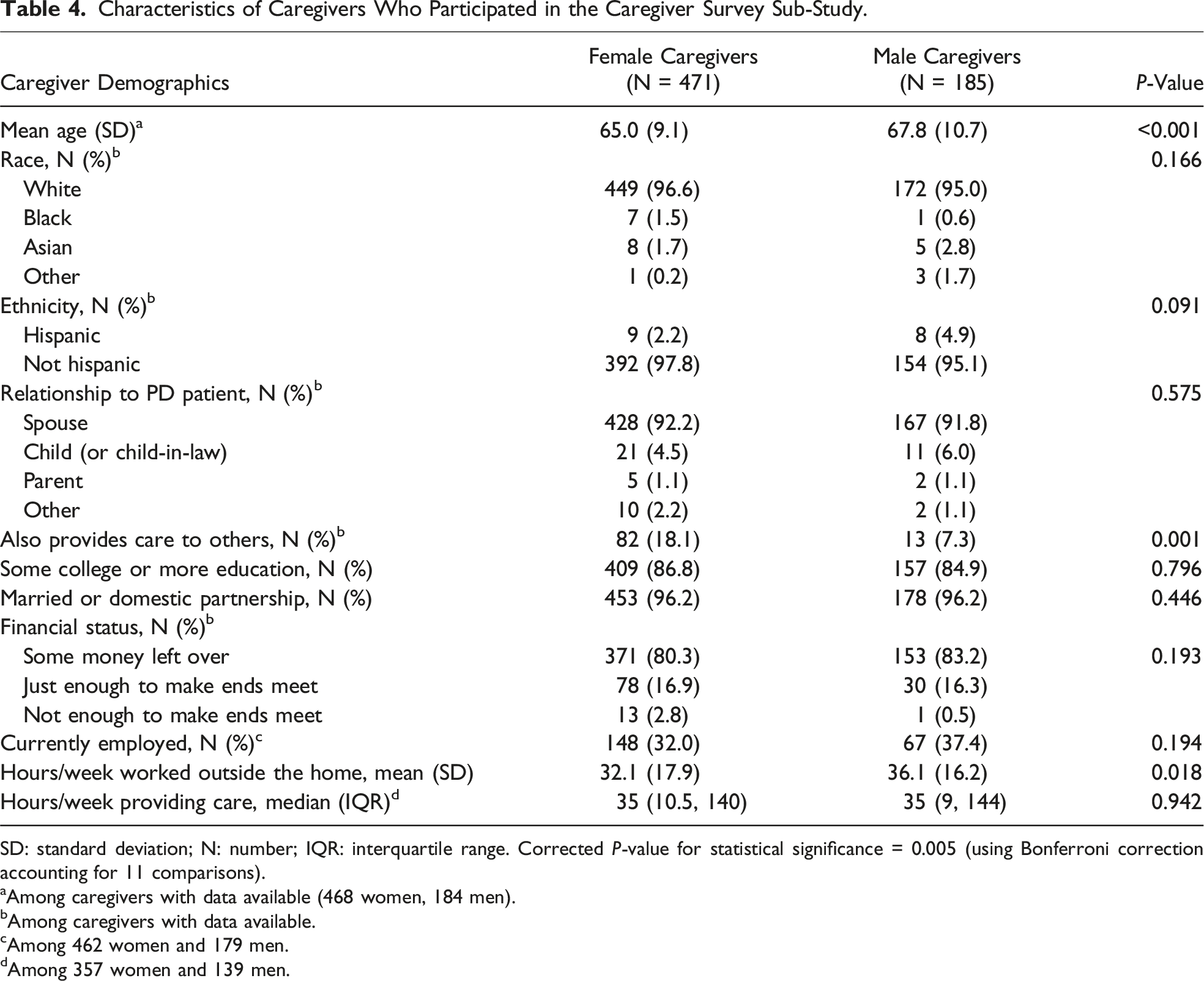
SD: standard deviation; N: number; IQR: interquartile range. Corrected P-value for statistical significance = 0.005 (using Bonferroni correction accounting for 11 comparisons).
aAmong caregivers with data available (468 women, 184 men).
bAmong caregivers with data available.
cAmong 462 women and 179 men.
dAmong 357 women and 139 men.
Differences in Patient Characteristics by Caregiver Gender
Female caregivers care for patients with greater disability (mean MDS-UPDRS Part II score 28.0 vs 23.9, P < 0.001). There are no differences in overall caregiving activities between men and women caregivers (mean activity help score 33.2 ± 11.3 for female caregivers vs 32.9 ± 11.34 for male caregivers, P = 0.494). However, male caregivers provide more assistance with mobility, both inside the house (mean help score 1.76 ± 1.08 vs 1.96 ± 1.10, P = 0.035) and outside the house (mean help score 1.87 ± 1.12 vs 2.15 ± 1.19, P = 0.004), while female caregivers spend more time doing chores inside the house, for example laundry (mean help score 2.93 ± 1.24 vs 2.54 ± 1.20, P < 0.001) and managing finances (mean help score 2.71 ± 1.31 vs 2.41 ± 1.33, P = 0.009).
Differences in Patient Characteristics by Caregiver Gender.
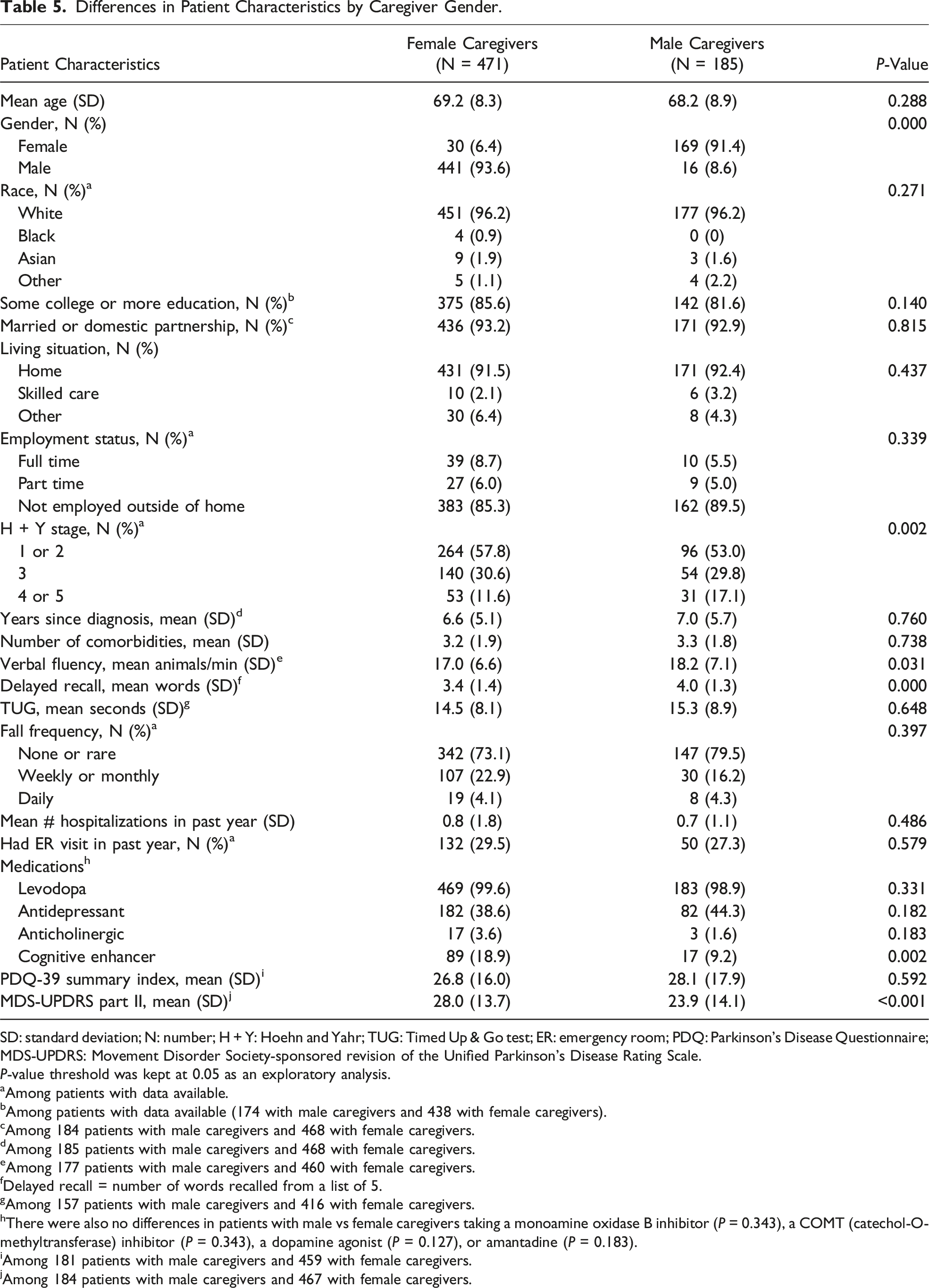
SD: standard deviation; N: number; H + Y: Hoehn and Yahr; TUG: Timed Up & Go test; ER: emergency room; PDQ: Parkinson’s Disease Questionnaire; MDS-UPDRS: Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale.
P-value threshold was kept at 0.05 as an exploratory analysis.
aAmong patients with data available.
bAmong patients with data available (174 with male caregivers and 438 with female caregivers).
cAmong 184 patients with male caregivers and 468 with female caregivers.
dAmong 185 patients with male caregivers and 468 with female caregivers.
eAmong 177 patients with male caregivers and 460 with female caregivers.
fDelayed recall = number of words recalled from a list of 5.
gAmong 157 patients with male caregivers and 416 with female caregivers.
hThere were also no differences in patients with male vs female caregivers taking a monoamine oxidase B inhibitor (P = 0.343), a COMT (catechol-O-methyltransferase) inhibitor (P = 0.343), a dopamine agonist (P = 0.127), or amantadine (P = 0.183).
iAmong 181 patients with male caregivers and 459 with female caregivers.
jAmong 184 patients with male caregivers and 467 with female caregivers.
Caregiver Health, Strain, Preparedness, Support, and Satisfaction
Caregiver Survey Results Regarding Caregiver Clinical Data and the Caregiving Experience.
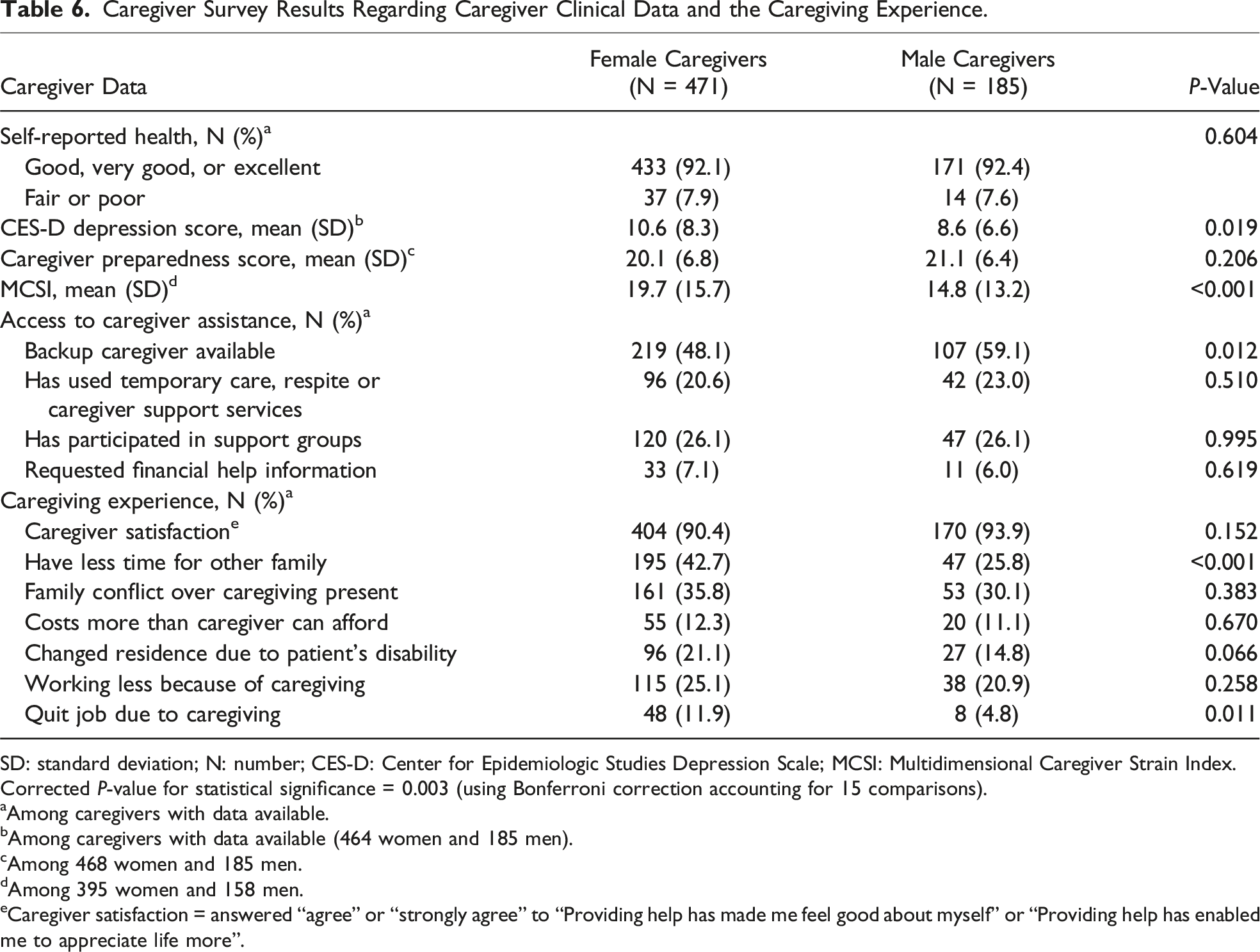
SD: standard deviation; N: number; CES-D: Center for Epidemiologic Studies Depression Scale; MCSI: Multidimensional Caregiver Strain Index.
Corrected P-value for statistical significance = 0.003 (using Bonferroni correction accounting for 15 comparisons).
aAmong caregivers with data available.
bAmong caregivers with data available (464 women and 185 men).
cAmong 468 women and 185 men.
dAmong 395 women and 158 men.
eCaregiver satisfaction = answered “agree” or “strongly agree” to “Providing help has made me feel good about myself” or “Providing help has enabled me to appreciate life more”.
Discussion
This national study examines potential explanations for observed gender differences in caregiving among PwP and shows that the relative lack of informal caregiver support for women with PD reported previously 14 is largely due to differences in demographics. Women with PD who don’t have caregivers are older and less likely to be married than men without caregivers. Stepwise regressions show that marital status is a strong driver of the gender disparity in caregiver presence.
As opposed to prior research of elderly disabled patients in general that shows wives play a dominant role in the care of disabled men and children (especially daughters, daughters-in-law, or granddaughters) play a dominant role in the care of disabled women, 11 the vast majority of caregivers in this study for both men and women with PD are spouses of the opposite gender. The high rate of male spouses as the caregiver for the married women with PD in this study may reflect changing demographics and evolving social structures and norms wherein men are increasingly assuming the caregiving role. 26 This finding may also further magnify the gender disparity in caregiver access in the PD population given that women with PD are less likely to be married and more likely to be widowed, and nearly half of those widowed have no caregiver. Widowhood disproportionately affects women for a variety of reasons; women are more likely to survive the death of their spouse and are less likely to remarry after their spouse dies. 27
Marriage and widowhood have been shown to affect numerous areas of health. Marriage has a positive impact on the health of older adults in general and widowhood is associated with cognitive decline.28,29 In cancer patients, marriage is associated with improved survival and widowhood is associated with the shortest survival rate. 30 Marriage may affect the health outcomes of men and women with PD differently, as has been shown in cancer patients wherein divorced/separated men have a worse survival rate than women. 30 This study shows that marriage strongly affects informal caregiver presence in PD, and prior studies indicate that the presence of a caregiver is associated with health outcomes in PD. 9 It is unknown to what degree marriage and widowhood may independently affect health outcomes in PD and whether the effects of marriage on health outcomes in PD may differ between genders and cultures. This area of research requires further investigation.
Because the PwP in this study are younger than the elderly disabled patients previously studied, 11 the lower rate of children acting as caregivers for people with PD could reflect the younger age of adult children in this population, who may be busy rearing children and establishing careers, with less time to devote to parental caregiving. Interventions that increase the participation and support of others, including men and women in their support system as well as paid caregivers, in the caregiving for women with PD may help address the relative lack of access to caregivers among women with PD.
The effect of gender differences in caregiving receipt on health outcomes for women with PD requires further investigation. A study of Medicare beneficiaries revealed that women with PD use more advanced nursing care resources (including nursing home placement, home health care, and hospice), have less direct physician contact, and have a higher incidence of hip fracture and depression than men. 31 Further study is needed to evaluate whether, and to what degree, gender differences in caregiving contribute to these or other adverse healthcare outcomes among women with PD.
Prior studies have also suggested that caregiving has adverse effects on the physical and psychological health of caregivers, particularly among caregivers for dementia patients, including higher rates of depression, stress, lower subjective well-being, and poorer health. 32 This study shows that female caregivers of PwP report higher rates of strain and have less time to spend with other family members than male caregivers. This may be due to greater cognitive decline among PwP with female caregivers, which has been shown to be more burdensome on caregivers than the motor symptoms of Parkinson’s disease. 33 Female caregivers also care for PwP with greater disability as evidenced by higher MDS-UPDRS Part II scores, which may contribute to higher caregiver strain. However, this scale could be affected by traditional gender roles; women with PD may score better on the MDS-UPDRS Part II in part because they might be more likely to continue household chores despite their impairment, due to social norms and expectations. 34 Female caregivers are also more likely to provide care for multiple people, which may reflect traditional gender roles and cultural expectations that shape caregiving responsibilities for women. 15 Despite this, self-reported health of women caregivers is not poorer than that of men. Addressing gender-specific needs of caregivers will be important for reducing burnout and increasing access to informal caregivers.
There were several limitations to our study. This study is cross-sectional in design, limiting the ability to establish causation. Data gathered for the study relied on self-report, which can lead to bias and missing data. The survey did not capture differences in how men and women caregivers define caregiving, which may be shaped by cultural gender norms. The survey did not account for patients and caregivers with non-binary genders. Participants of the PF-POP may not be representative of the general population, which may affect generalizability of the results. Although the baseline cohort is large, they still represent individuals who are seeking care at Parkinson’s Foundation Centers of Excellence. This cohort is mostly white, with mild disease (H + Y 1 or 2), more educated on average, and may have more resources than the general PD population. Additionally, we relied on a convenience sample of caregivers who chose to respond to the survey which may select for those more interested in or affected by caregiving, thereby creating participation bias. Respondents were mostly spouses of PwP living at home with mild disease, who accompanied the patient to their appointment. These cohort characteristics differ from PwP enrolled in the broader PF-POP who chose not to participate in this sub study (as shown in Table 1) and may differ from the general PD population. These cohort factors limit our ability to understand the caregiving experience of non-spouses and for PwP not living at home. Additionally, the sub-study only captures the experience of the primary caregiver for a patient and does not capture the caregiving experience of any potential secondary caregivers for the same patient. However, the large number of respondents and the detailed nature of the survey allows for the ascertainment of interesting and significant caregiving data that can inform Parkinson’s disease caregiving education and future interventions.
This study highlights the impact of demographic differences between men and women on access to informal caregiving in PD. Identification of factors driving gender disparities in caregiving is important for shaping health policy and implementing interventions to address the unmet needs of both caregivers and PwP without access to informal caregivers. Strategies to detect and address caregiver needs such as systematically screening for caregiver strain and increasing access to social workers are a first step to support existing caregivers. In addition, for all PwP, earlier assessment of needs could help trigger earlier involvement of community and family support networks to identify potential informal caregivers.
Supplemental Material
Supplemental Material - Contributors to Gender Disparities in Parkinson’s Disease Caregiving
Supplemental Material for Contributors to Gender Disparities in Parkinson’s Disease Caregiving by Sarah Horn, Yunfeng Dai, Samuel S. Wu, and Nabila Dahodwala in Journal of Geriatric Psychiatry and Neurology.
Footnotes
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Parkinson’s Foundation (#UP201). The funding source had no involvement in the study design; collection, analysis, and interpretation of data; writing of the report; or in the decision to submit the article for publication. Dr Horn also received support from the Edmond J. Safra Fellowship in Movement Disorders.
Ethical Statement
Data Availability Statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental Material
The caregiver sub-study survey instrument (excluding the standardized questionnaires). Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.