
Abstract
Objective
To evaluate the effect of virtual group music therapy on apathy in people with Parkinson’s disease (PD).
Introduction
Apathy affects 40% of people with PD, lacks effective therapies, and independently predicts poorer quality of life and greater caregiver burden. Music therapy is the clinical application of music to address a person’s physical or emotional needs and is effective in treating apathy in dementia.
Methods
People with idiopathic PD and apathy (Movement Disorders Society-Unified Parkinson’s Disease Rating Scale, apathy item
Results
Sixteen PD participants (93.8% men, mean age 68.3
Conclusion
Group music therapy is an effective treatment for apathy in PD and may improve mood. The virtual format is a feasible alternative to in-person sessions with high adherence and satisfaction.
Introduction
Over 1 million people in the United States are currently living with Parkinson’s disease (PD), and 90,000 Americans are diagnosed with PD each year. 1 PD is the second most common neurodegenerative condition and is characterized by its cardinal motor features of bradykinesia, rest tremor, rigidity and postural instability. 2 However, nonmotor symptoms such as autonomic dysfunction, depression, anxiety, apathy, cognitive changes, and sleep disturbances have a greater impact on health-related quality of life than motor symptoms. 3 Apathy, or a lack of motivation to perform goal-oriented behaviors, is reported in 40% of people with PD and is often challenging to manage. 4 Due to apathy, people with PD make less effort to perform daily tasks, have reduced interest in things they used to enjoy, and take less initiative in dealing with personal or social issues. Neuroimaging studies of apathy in PD reveal abnormalities in the cortico-subcortical pathways including the ventral striatum, dorsal anterior cingulate cortex, medial and lateral prefrontal cortices, and the ventral tegmental area. 5 In PD, apathy is associated with older age, more severe motor impairment, executive dysfunction, and depression. 4 Additionally, apathy is associated with greater functional disability in performing activities of daily living, 6 independently predicts worse quality of life, 7 and contributes to caregiver burden. 8
There are currently no effective treatment options available for apathy in PD. Several pharmacologic agents have been studied and are used off-label to treat apathy. Clinical trials of dopamine agonists including pirebedil 9 and rotigotine 10 have found mixed effects on apathy. The cholinesterase inhibitor, rivastigmine, was found to reduce apathy and improve caregiver burden in people with PD and moderate to severe apathy, but the benefit was not sustained long-term. 11 Methylphenidate, which inhibits dopamine re-uptake, improved apathy in a subgroup of patients with freezing of gait. 12 There is limited research on non-pharmacologic approaches to apathy in PD.
Music therapy is the “clinical use of music interventions to address a patient’s physical, emotional, cognitive, and social needs.” 13 Music therapy is categorized as active when creating music, such as playing an instrument or singing, or receptive, when listening to music. Preferred music, which promotes dopamine release, may be more beneficial than non-preferred music for certain clinical goals. 14 Music preferences are often developed during an individual’s late teens to early twenties. Particularly within the dopaminergic mesolimbic system, music stimulates the nucleus accumbens, which regulates mood and motivation and mediates reward pathways. Furthermore, limbic structures including the hippocampus, amygdala, cingulate cortex and prefrontal cortex are also activated by music resulting in mood and cognitive changes. 15
Music therapy has consistently shown efficacy in treating apathy in dementia, including Dementia with Lewy Bodies (DLB), which shares prominent neuropsychiatric symptoms and pathophysiology with PD. 16 Previous studies on music interventions in PD have primarily focused on either motor symptoms or voice and communication.17-21 There are a few reports dedicated to nonmotor benefits of music-based interventions in PD. People with early-stage PD participating in dance therapy had significant improvements in executive function, episodic memory, anxiety, depression, and quality of life. 22 A pilot, feasibility study of a group guitar instruction program found improvements in depression, anxiety and quality of life. 23 As a secondary outcome, quality of life has been noted to improve with various music-based interventions.17,21 Limited studies have evaluated the impact of music therapy on caregivers of people with PD. In ParkinSong, a multi-arm controlled clinical trial of group singing for both people with PD and their caregivers, the caregivers showed improvements in stress and depression. 19
Given its consistent positive effect on apathy in patients with other neurodegenerative conditions and on caregiver mood and stress, we aimed to determine if group music therapy may be a suitable strategy to 1) reduce apathy in people with PD and 2) improve caregiver burden. In addition, we hypothesized that the virtual platform for music therapy would be feasible with strong adherence (>70%) and satisfaction.
Methods
Study Design and Participants
Participants were recruited along with their caregivers from September 2021 to January 2022 to this cohort study. First, patients seen in the Rush University Medical Center (RUMC) Movement Disorders Program were pre-screened for potential inclusion using any diagnoses of apathy (ICD-10 code R45.3) and PD (ICD-10 code G20) recorded in the electronic medical record. To confirm current apathy, the primary investigator (PI) (DSZ) telephoned potential participants and administered a single apathy question (item 1.5) from the Movement Disorders Society- Unified Parkinson’s Disease Rating Scale (MDS-UPDRS).
24
Those who scored
Medical history including PD duration, current stage of PD (Hoehn & Yahr (H&Y), 25 most recent Unified Parkinson’s Disease Rating Scale (UPDRS) scores, 26 medical and psychiatric comorbidities, active neuropsychiatric treatment regimen (including deep brain stimulation placement, infusion therapy, oral PD medications, cognitive medications, stimulants, antidepressants, and recreational drug use including marijuana and cannabidiol products) was obtained from the electronic medical record. Participants provided their age, sex, race, ethnicity, and employment status (for both the person with PD and the caregiver) by online survey.
This study was approved by the RUMC Institutional Review Board. The primary data was collected and managed using REDCap (Research Electronic Data Capture) hosted at RUMC.27,28 REDCap is a secure, Health Insurance Portability and Accountability Act of 1996-compliant, web-based software platform designed to support data for research studies. All paper copies of records were stored in a binder in a secure, locked location. Data was exported to and analyzed with “R” statistical software.29,30
Assessments
The following assessments were completed prior to the start of the music therapy intervention (January 2022) and at the end of the study (April 2022), except for the satisfaction survey that was completed only post-intervention.
Apathy Scale (AS)
is a validated 14-item questionnaire to screen for and measure severity of apathy.
31
A score of
Parkinson’s Disease Questionnaire – Short Form (PDQ-8)
is a validated 8-item questionnaire derived from the original 39-item Parkinson’s Disease Questionnaire and is used to measure quality of life in people with PD. 32 Lower scores reflect better quality of life.
Schwab and England Activities of Daily Living (SE-ADL)
scale is an assessment of an individual’s ability to perform activities of daily living. 33 Here it was used as a self-assessment completed by the person with PD. Ratings are in 10% increments ranging from 100% (completely independent) to 0% (vegetative).
Beck Depression Inventory (BDI-II)
is a self-administered 21-item scale that identifies behavioral characteristics of depression. 34 Higher scores reflect more severe depressive symptoms.
Montreal Cognitive Assessment-Blind (MoCA-B)
is a 22-point cognitive screening tool validated for phone administration by a trained professional. It omits the naming and visuospatial/executive sections of the original MoCA. 35
Zarit Burden Interview
- short form (ZBI-12) is a validated 12-item self-administered survey for caregivers to determine the extent of burden experienced while providing care to a loved one. 36 Higher scores suggest increased caregiver burden.
Multidimensional Caregiver Strain Index (MCSI)
Is a validated 18-item self-administered scale that measures six domains including physical strain, financial strain, social constraints, interpersonal strain, time constraints, and demanding issues. 37 Higher scores reflect increased frequency of caregiver strain.
A Satisfaction Survey
Designed by the study team had three questions with a 10-point Likert scale, five checkbox questions, and one open-ended question for overall study feedback (see Supplemental Material, Appendix 1). PD participants and caregivers individually completed this at the end of the study.
The music therapist recorded attendance at each session. All assessments were de-identified and self-administered in REDCap to reduce bias, except the cognitive and depression screens, which the PI (DSZ) administered by telephone, then entered into REDCap.
Intervention
Music therapy was delivered virtually in small groups of five to six pairs on a secure videoconferencing platform by a board-certified, neurologic music therapist for one hour each week for a total of twelve weeks (from January 2022 through March 2022). Participants with PD and their caregivers were each provided instrument kits including a harmonica, drum, tambourine, drumsticks, wrist bells and more. Each session followed a similar agenda as shown in Figure 1, with exercises increasing in complexity over the study period. A detailed description of a typical group music therapy session, which was designed by the music therapist based on prior similar research, is included as Supplemental Material, Appendix 2 to facilitate replication.17,38-41 The music therapist encouraged participants to recommend songs for inclusion in therapy and finalized songs based on participant preference.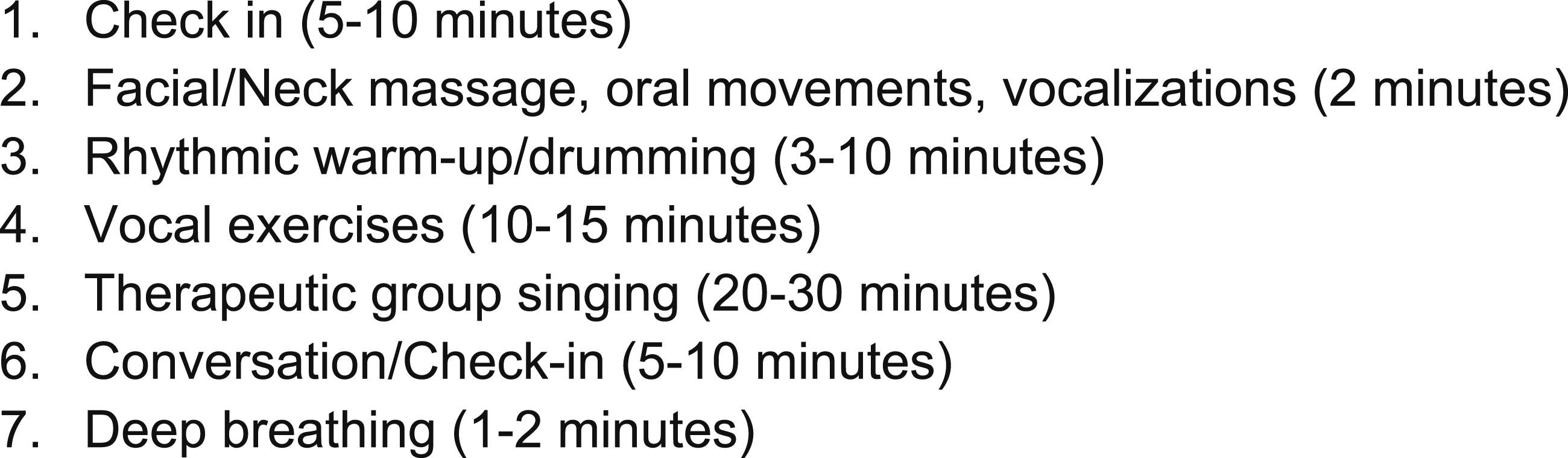
Statistics
Sample Size Determination
This pilot study was powered to detect a meaningful post-intervention change in the AS, where the minimum clinically important difference is five. 42 A sample size of 17 people with PD achieved 95% power to detect this within-group difference, yielding an effect size of 0.96 using a two-sided paired t test with a significance level of <0.05. Accounting for a 15% drop out rate, we aimed to recruit 20 participants with PD.
Analysis Approach
The analytic cohort included participants with PD and their caregivers who completed all pre- and post-intervention surveys. Changes in post-intervention scores on the AS, PDQ-8, BDI-II, SE-ADL, MoCA-B, ZBI-12, and MCSI were assessed with a nonparametric Wilcoxon signed-rank test due to the small sample size and assumption that that data would not be normally distributed. A two-tailed alpha level of <0.05 indicated significance. Attendance was described with frequencies. Subjective data from the satisfaction surveys were summarized as frequencies and percentages for categorical variables and median and interquartile range (IQR) for continuous variables.
Results
Participant Selection
We identified 80 potential participants based on diagnoses of PD and apathy in the electronic medical record, of whom, 20 people scored ≥2 on the MDS-UPDRS apathy item to qualify for the study. Of these 20 people, 16 completed the consent process and enrolled, as shown in the CONSORT diagram in Figure 2. Of those who did not enroll, one participant did not complete the consent form and was lost to follow-up, another reported anxiety about joining the study, one was no longer interested in the study, and another participant’s caregiver was unable to commit to the study’s time requirements. CONSORT Diagram. Abbreviations: PD, Parkinson’s disease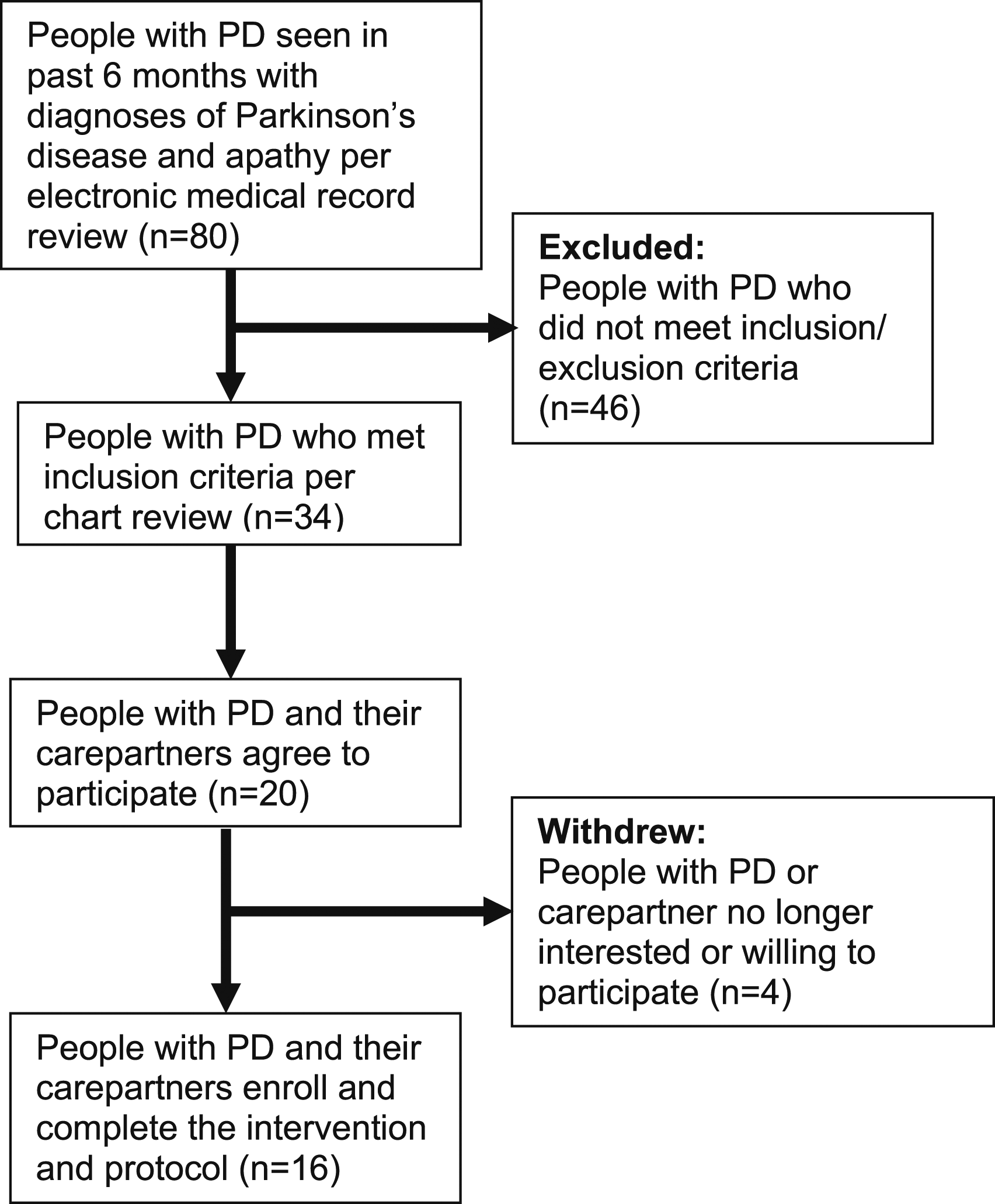
Demographics and Baseline Characteristics
Baseline Characteristics.
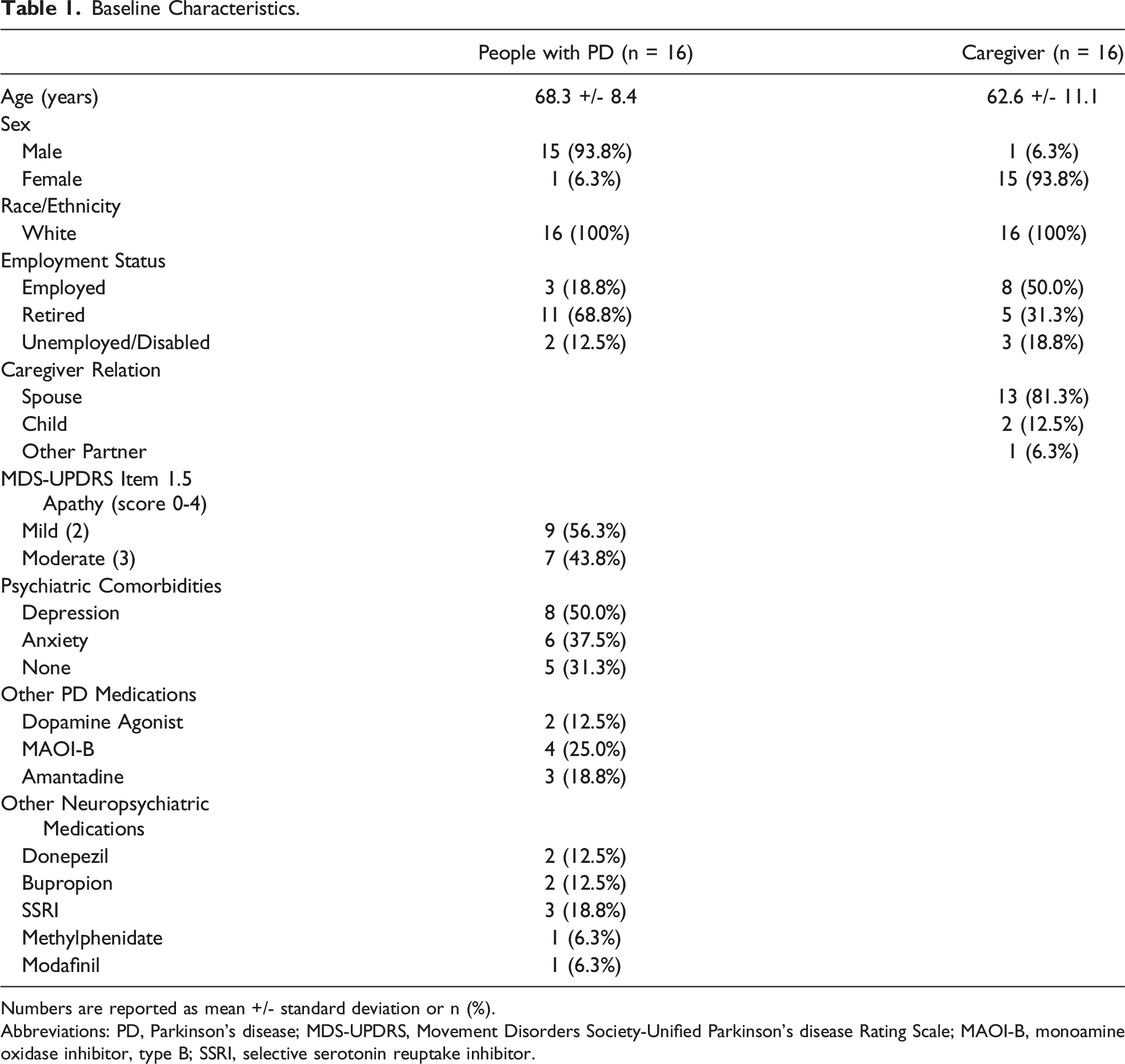
Numbers are reported as mean +/- standard deviation or n (%).
Abbreviations: PD, Parkinson’s disease; MDS-UPDRS, Movement Disorders Society-Unified Parkinson’s disease Rating Scale; MAOI-B, monoamine oxidase inhibitor, type B; SSRI, selective serotonin reuptake inhibitor.
Analysis of Participants with Parkinson’s disease
Parkinson’s Disease Participant Outcomes.
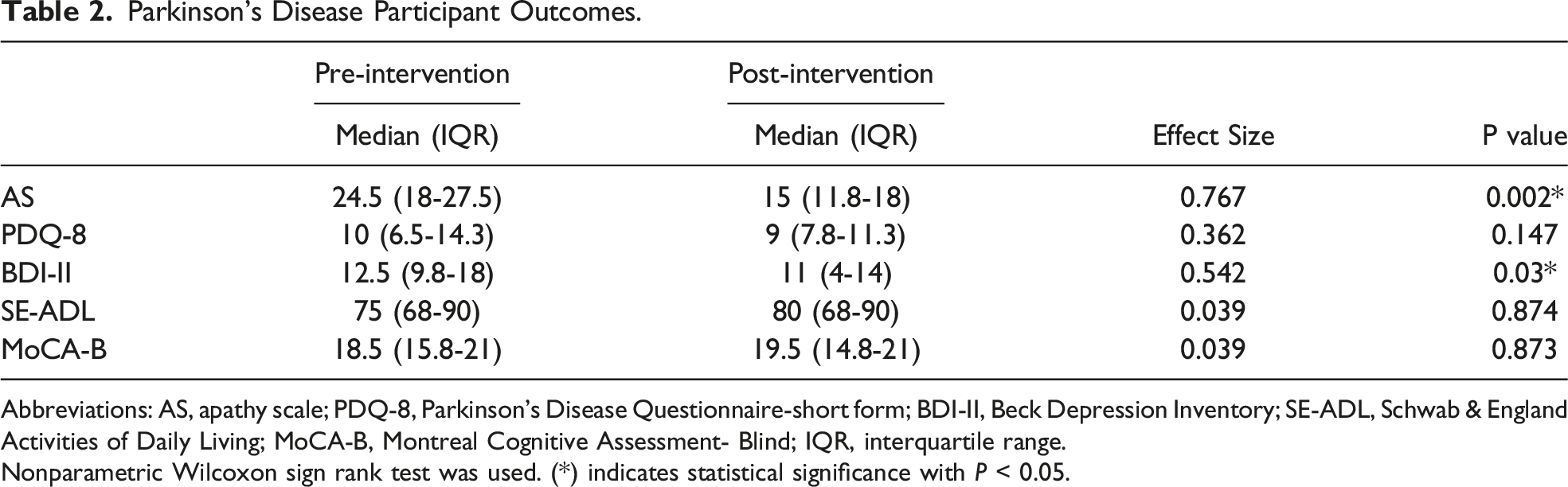
Abbreviations: AS, apathy scale; PDQ-8, Parkinson’s Disease Questionnaire-short form; BDI-II, Beck Depression Inventory; SE-ADL, Schwab & England Activities of Daily Living; MoCA-B, Montreal Cognitive Assessment- Blind; IQR, interquartile range.
Nonparametric Wilcoxon sign rank test was used. (*) indicates statistical significance with P < 0.05.
Analysis of Caregivers
Caregiver Outcomes.
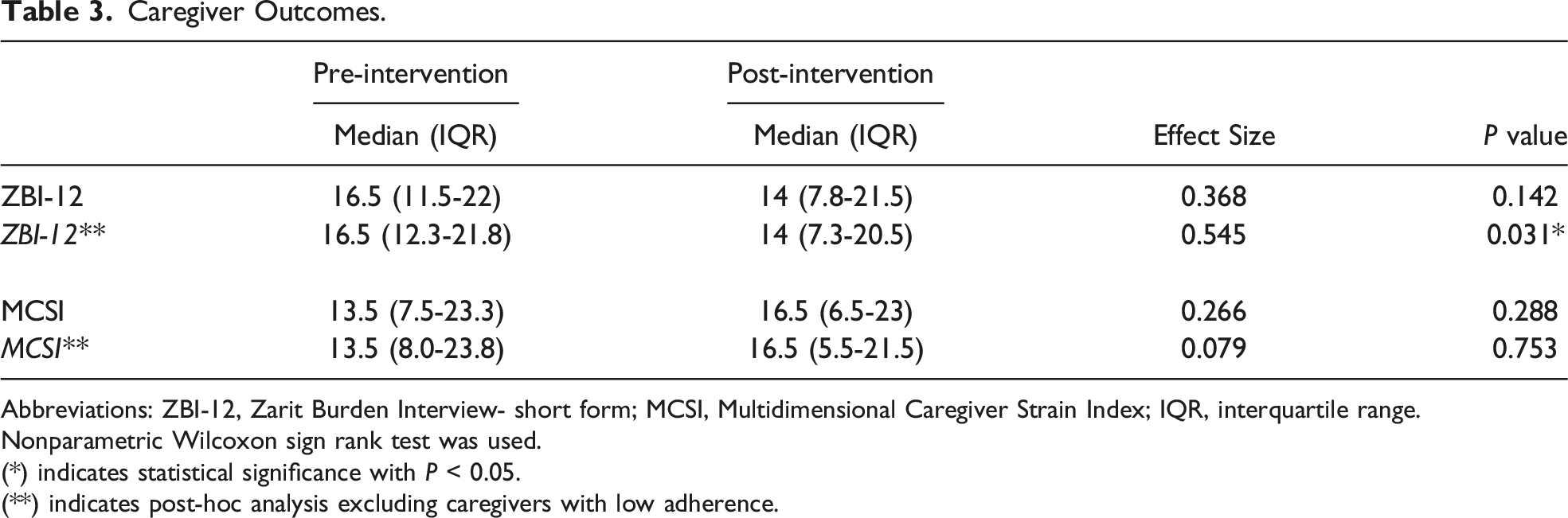
Abbreviations: ZBI-12, Zarit Burden Interview- short form; MCSI, Multidimensional Caregiver Strain Index; IQR, interquartile range.
Nonparametric Wilcoxon sign rank test was used.
(*) indicates statistical significance with P < 0.05.
(**) indicates post-hoc analysis excluding caregivers with low adherence.
Analysis of Adherence and Satisfaction
Participants with Parkinson’s Disease
All 16 participants with PD completed at least eight sessions (>70% adherence). Four participants asked to attend an alternate day due to scheduling conflicts. Reasons for absence from the sessions included vacation and personal or family illness.
There were high levels of satisfaction among people with PD on the post-intervention satisfaction survey. On a scale from 0 to 10, where 10 means very satisfied, the median satisfaction with music therapy was 9.5 (IQR 7-10, range 2-10) and with the virtual platform was 9.5 (IQR 8-10, range 2-10). The median likelihood of recommending music therapy to another patient with PD was 10 (IQR 7.8-10, range 2-10) indicating “very likely” to recommend.
The top three most enjoyed features of the intervention were interaction with the music therapist (81.3%, n = 13), social interaction (75%, n = 12), and musical activities, such as instrument playing (62.5%, n = 10). Over half of the PD participants (56.3%, n = 9) planned to either restart an old hobby (musical or non-musical) or start a new one. Half of the participants (n = 8) stated they would continue the exercises they learned from music therapy, and 50% planned to incorporate more music into their day. The most frequently reported benefits noted by PD participants were improved mood (62.5%, n = 10), improved voice quality (56.3%, n = 9), and increased interest in things (37.5%, n = 6). Five PD participants (31.3%) did not enjoy the music selection. The top three suggestions for improvement of the intervention were changing the music selected (37.5%, n = 6), adding in-person sessions (25%, n = 4), and changing musical activities performed (25%, n = 4). Eleven participants provided free text responses that were consistent with this feedback. Their responses are presented in Supplemental Material, Appendix 3.
Caregivers
All but two of the caregivers were >70% adherent with the music therapy sessions. Four caregivers asked to attend an alternate day due to scheduling conflicts. Reasons for absence from the sessions included vacation, personal or family illness, doctor’s appointments, family wedding, and work obligations.
The post-intervention satisfaction survey also revealed high levels of satisfaction among caregivers. The median satisfaction with music therapy was 9 (IQR 5.8-10, range 2-10) and with the virtual platform was 9.5 (IQR 7.8-10, range 4-10). The median likelihood of recommending music therapy to another PD caregiver was 10 (IQR 6-10, range 2-10).
The top three features of the intervention that caregivers most enjoyed were interaction with the music therapist (100%, n = 16), the musical activities (87.5%, n = 14), and the social interaction (68.8%, n = 11). As a result of their participation in the study, 68.8% (n = 11) of caregivers planned to incorporate more music into their day. Six caregivers (37.5%) reported an improvement in their mood. Three caregivers (18.8%) did not enjoy the music selection. The most frequently selected suggestion for improvement was adding in-person sessions (43.8%, n = 7). Three caregivers specifically noted their appreciation for the opportunity to participate in the intervention with their loved one with PD. Caregiver responses are presented in Supplemental Material, Appendix 4.
Discussion
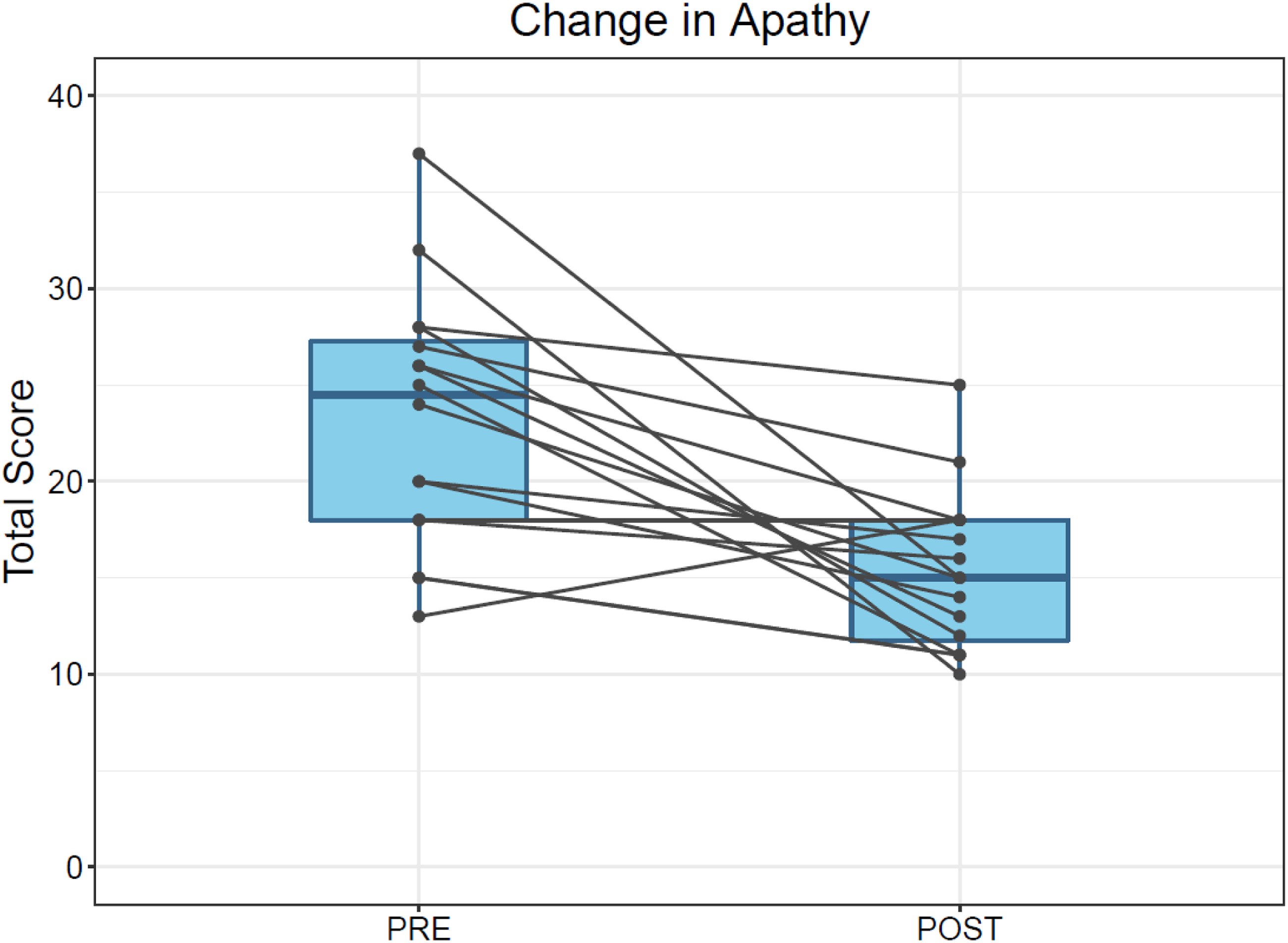
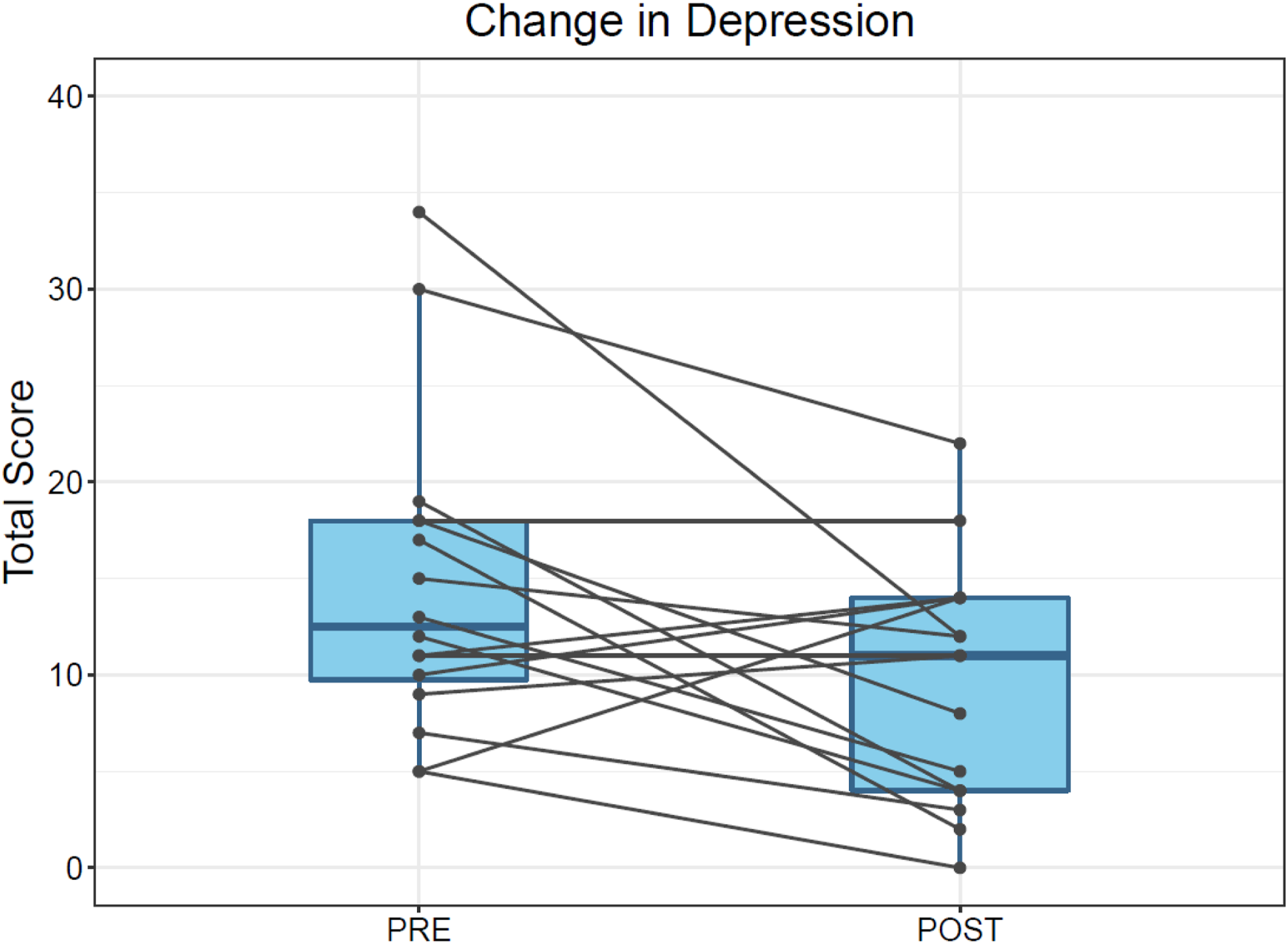
Music therapy appears to be an effective treatment for apathy in PD. There was marked improvement in apathy on the AS post-intervention. Subjectively, over one-third of people with PD reported increased interest in activities, and over half of the PD participants either restarted an old hobby or started a new one by the end of the study. Examples of hobbies included playing guitar and joining a local soccer club. Additionally, music therapy also reduced depressive symptoms in people with PD.
The effects of music therapy on apathy and mood in this study are consistent with prior research16,22,23 and can be explained by understanding the two primary effects of music-based interventions. 43 Music’s impact on mood and emotion gives it the ability to improve one’s quality of life and overall well-being. When the intervention also involves active music playing, such as playing an instrument or singing, there is repetition of movement and integration of auditory information, both of which are important for motor learning and neuroplasticity. Creation of music promotes intrinsic motivation for the individual to self-monitor and adjust, while the auditory information, or the music produced, provides extrinsic motivation. The activation of these reward pathways, which are impaired in apathy, is mediated by dopamine, the release of which is increased by music. Together, the mood and reward-based learning effects of musical interventions can promote self-efficacy and autonomy.
Quality of life, functional abilities, and cognition were not affected by music therapy in this study. However, other studies have reported improvements in quality of life with music therapy.17,21,22 This study may not have found similar results because it was not powered to detect change on the PDQ-8. Alternatively, the use of this abbreviated version of the PDQ-39, the music therapy curriculum, and the duration of therapy may also contribute to lack of improvements in quality of life. Increased disability is associated with chronic apathy in PD.4,6 Thus, changes in self-assessment of functional status by people with PD may only be detected if compared with a control group and after a longer duration of follow-up. Lastly, apathy has been associated with executive dysfunction. 4 The lack of effect of music therapy on cognition in this study may be due to the use of the MoCA-B, which is a screening tool that excludes visuospatial and executive function tasks, the latter of which is associated with apathy. Additionally, like the functional assessments, cognition may need to be reassessed after a longer duration of time and compared to the natural course of cognitive decline in a control group.
Caregivers did not show improvement on assessments of caregiver burden or strain in this study. Only when those with low adherence were excluded from analysis was there a slight reduction in burden. Subjectively, over one-third of caregivers reported improved mood after the music therapy sessions, and there were few critiques about the intervention. Caregiver burden and strain are more chronic states and may not be as responsive to short-term interventions. Scales measuring mood, loneliness, caregiver quality of life, or caregiver attitude may be more suitable and sensitive to change. However, these results must be interpreted with caution because the study was not powered to detect changes in caregivers.
The specific music therapy curriculum used in this study also may explain the lack of music therapy effect on the caregiver measures. The sessions were focused on achieving vocal and motor goals with indirect effects on apathy and mood in people with PD and not on reducing stress in caregivers. In their open-ended feedback, caregivers primarily commented on how the sessions helped their loved one rather than themselves (see Supplemental Material, Appendix 4). This suggests that caregivers may have been preoccupied in ensuring their loved one was adequately engaged. Therefore, caregivers and people with PD may need to participate in separate music therapy sessions so that goals of treatment are appropriately addressed and to allow caregivers to focus on themselves.
Overall, both people with PD and their caregivers reported high levels of satisfaction with the virtual group music therapy platform, and most would strongly recommend it to others. About one-third of participants suggested adding in-person sessions in future iterations of this study. Thus, virtual music therapy may be a useful alternative for some PD patients with limited mobility or who are homebound, but may not be a desired platform for all, especially caregivers. In this study, the music therapist reviewed the song selection with participants and requested recommendations to use during the sessions. However, the satisfaction survey feedback demonstrated that not all participants enjoyed the music used. This remains a challenging aspect of providing music therapy in a group setting. Additionally, qualitative feedback suggested that some participants found the motor and vocal exercises challenging. The music therapist had similar observations and had to modify the curriculum over the course of the study to improve participation and satisfaction in those participants. Due to the virtual format, the music therapist had to mute participants during certain activities and limit the incorporation of some of the instruments normally used like the bell and tambourine, which would cause technical issues.
There were several other limitations to this small pilot study. One major limitation to the study design was the lack of a control group. Prior studies assessing the effect of music therapy have focused on motor symptoms, in which control interventions included “standard of care” or physical therapy. There is no set standard for managing apathy in PD, and clinical approaches are highly heterogeneous between providers. Thus, a “standard of care” control arm would not be suitable. In order to select an effective control for music therapy to manage apathy, first the “active ingredient” of music therapy must be identified. At the time of study design, it was unclear whether the music therapist, the musical activities, the social interaction in a group setting, or the music itself was key to a successful intervention. The satisfaction survey feedback revealed that participants most enjoyed the social interaction, guidance from the music therapist, and the musical activities; these are likely core to the intervention used to manage apathy. The addition of a control group would also improve understanding of the impact of music therapy on the natural trajectory of this chronic disease. From the open-ended survey responses (see Supplemental Material, Appendices 3 and 4), several participants commented on enjoying the musical aspect of the therapy as well. Because interaction with the therapist and with other participants was reported as a positive attribute of the study by several participants and caregivers, there may have been a component of loneliness that was addressed by the intervention but was not assessed in this study.
This study was slightly underpowered due to greater than expected attrition between screening and enrollment, with restrictions on additional recruitment due to the timeline of funding, and it was only powered to assess for clinically meaningful change on the AS. The participants were homogenous in race and sex so these findings may not be generalizable to other populations. Additionally, requiring people with PD to enroll with their caregivers limited recruitment since some apathetic people with PD without a caregiver were unable to participate. While the requirement of a caregiver may have excluded some individuals, this was an intentional decision: poor motor function is associated with both apathy and disease progression, and caregiver dependence similarly increases with disease progression. Thus, we assumed that individuals with apathy would be more likely to have poorer physical mobility and accordingly, more likely to have a caregiver. The baseline UPDRS-III, H&Y, and SE-ADL scores indicated a range of motor disability and dependency for activities of daily living. Thus, while most participants were largely independent, some of this cohort had more significant immobility. On the other hand, caregiver involvement may have contributed to the high adherence among PD participants. The concurrent caregiver participation in the sessions may also have potentially confounded the results if caregivers provided encouragement or positive reinforcement to the PD participants during or after the sessions.
There were also limitations to the assessments used. As previously mentioned, caregiver measures may not have been responsive to short-term changes. The satisfaction survey did not adequately assess the desired outcomes for caregivers including reduced stress. The MoCA is only a screening tool, and furthermore, the MoCA-B excluded executive function tasks. A comprehensive evaluation of both motor function and cognition with formal neuropsychological testing would increase sensitivity in measuring change post-intervention. Finally, since the surveys and questionnaires were primarily self-administered and labeled with the survey name, there may have been both response and social desirability biases.
Future iterations of this study should include an appropriate control arm and a diverse cohort more representative of PD nationally. This may be achieved by leveraging community-based partnerships and support groups serving underrepresented minority populations of people with PD, as well as broader dissemination of recruitment material, to enroll a more representative cohort. 44 Based on the findings from this study, the control arm could use pre-recorded music to eliminate the social interaction and contribution of the music therapist. Additionally, an attention control arm including only social interaction could also be considered to better delineate the impact of music therapy itself. Virtual music therapy has been shown to be as effective as in-person sessions. 45 While the virtual format was enjoyed by most participants, based on constructive feedback from others, both formats could be offered in future iterations of this study. Due to the differing goals of participants with PD and caregivers, each cohort should undergo a separate intervention. The music therapy curriculum for participants with PD may be similar to what was completed in this intervention and include motor and vocal exercises, enjoyable music and direct guidance from a music therapist. They may, however, benefit from one-on-one sessions since each participant with PD’s ability to complete the exercises depends on motor symptom severity. Meanwhile, in order to improve caregiver stress, mood, and quality of life, a cognitive-behavioral approach of music therapy may instead be beneficial for them. For example, a study evaluating music therapy to reduce compassion fatigue in professional hospice workers used music therapy interventions such as guided meditation with live music, lyric analysis, and music and movement. 46 Regarding the scales and surveys used, in the future, formal neuropsychological assessments would allow for in-depth evaluations of mood and cognition and would be more sensitive in determining the impact of the intervention. Participant and caregiver loneliness and caregiver stress, quality of life, and mood measures should be included. While a full motor examination was impractical in this virtual pilot study, it is certainly indicated for future work to clarify the associations and interactions of mobility, apathy, disease duration and progression, and level of caregiver involvement. Furthermore, music therapy, like most pharmacologic, complementary, and rehabilitative therapies, must be maintained in order to remain effective and result in lasting changes. Thus, the duration of therapy and frequency of maintenance sessions should also be determined. Once this is understood, the long-term effects of music therapy on cognition, mood and motor functioning can be better assessed.
In summary, apathy is a common but under-recognized symptom in PD. There is no standardized treatment for apathy in PD despite its prominence as a predictor of poor quality of life. Thus, management of apathy remains an unmet need in the field. This pilot study is the first to demonstrate the effect of music therapy on apathy in PD. The findings from this study are promising and highlight the potential use of non-pharmacologic therapies in PD, particularly in the management of neuropsychiatric symptoms. Given the effectiveness of non-pharmacologic treatments and strong patient interest in these interventions, further research on the clinical uses of music and other complementary therapies in Parkinson’s disease is warranted.
Supplemental Material
Supplemental Material - Virtual Group Music Therapy for Apathy in Parkinson’s Disease: A Pilot Study
Supplemental Material for Virtual Group Music Therapy for Apathy in Parkinson’s Disease: A Pilot Study Deepal Shah-Zamora, Sharlet Anderson, Brandon Barton, Jori E. Fleisher in Journal of Geriatric Psychiatry and Neurology.
Footnotes
Acknowledgments
We thank the participants and caregivers who contributed to this study and generously offered their time. We also specifically acknowledge Linda Jedrzejek, the music therapist who organized and provided the music therapy intervention. We are grateful to the Rush University Division of Movement Disorders clinicians who referred patients to our study.
Authors’ Contributions
DSZ and JEF conceived the study; all authors designed the protocol; DSZ participated in recruitment, data collection; DSZ and JEF analyzed the data. DSZ drafted the manuscript and all authors provided critical reviews and approved the final version of the manuscript.
Conflicts of Interest
The authors declare that they have no competing interests with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Postma Family Research Program at Rush University Medical Center. JEF is supported by a research grant from the National Institutes of Health/National Institute of Neurological Disorders and Stroke (K23NS097615). The Sponsor had no role in the study design, collection, analysis, and interpretation of data, writing of the report and in the decision to submit the article for publication.
Ethical Approval
All procedures were approved by the Rush University Medical Center Institutional Review Board, IRB # 21-031212.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.