
Abstract
Background
Orthostatic hypotension (OH) is multifactorial in Parkinson’s disease (PD). Antiparkinsonian medication can contribute to OH, leading to increased risk of falls, weakness and fatigue.
Methods
We conducted a systematic review and meta-analysis of randomised controlled trials (RCTs) of antiparkinsonian drugs associated with OH as an adverse effect, compared to placebo. We searched EMBASE, MEDLINE and Web of Science databases until November 2020. Analysis used fixed-effects models and the GRADE tool to rate quality of evidence. Meta-analysis was performed if 3 or more studies of a drug group were available.
Results
Twenty-one RCTs including 3783 patients were included comparing 6 PD drug groups to placebo (MAO-B inhibitors, dopamine agonists, levodopa, COMT inhibitors, levodopa and adenosine receptor antagonists). OH was recorded as an adverse event or measurement of vital signs, without further specification on how this was defined or operationalised. Meta-analysis was performed for MAO-B inhibitors and dopamine agonists, as there were 3 or more studies for these drug groups. In this analysis, compared with placebo, neither MAO-B inhibitors or dopamine agonists were associated with increased risk of OH, (OR 2.28 [95% CI:0.81–6.46]), (OR 1.39 [95% CI:0.97–1.98]).
Conclusions
Most studies did not specifically report OH, or reporting of OH was limited, including how and when it was measured. Furthermore, studies specifically reporting OH included participants that were younger than typical PD populations without multimorbidity. Future trials should address this, for example,, by including individuals over the age of 75, to improve estimations of how antiparkinsonian medications affect risk of OH.
Introduction
Orthostatic hypotension (OH) is common in Parkinson’s disease (PD), with a prevalence ranging between 9.6–64.9%. 1 This wide range reflects heterogeneity of studies, differences in OH definition used and population included. The classical definition of OH is ‘a sustained reduction of at least 20 mmHg of systolic blood pressure (BP) and/or 10 mmHg of diastolic BP within 3 minutes of standing or head-up tilt-table testing’.’ 2 However, OH can be difficult to detect, as symptoms such as dizziness, sweating and light headedness are non-specific or may be absent.
The prevalence of OH increases with age 3 and can be divided into 3 categories that may co-exist: drug-induced, related to depletion of intravascular volume and neurogenic. 4 In PD, neurogenic OH is a consequence of autonomic dysfunction, which is mainly a result of cardiac sympathetic denervation and reduced activation of noradrenergic pathways. Parkinson’s disease patients with OH experience worsening of OH over time that correlates with disease duration. OH also affects quality of life and increases the risk of falls, weakness, fatigue 3 and cognitive impairment. 5
Previous studies also reported associations between OH and PD medications, complicating management of PD. This includes levodopa,6-8 dopamine agonists 9 and monoamine oxidase inhibitors. 10 Studies have also reported that patients diagnosed with OH before starting these treatments are likely to experience a worsening of hypotension when these drugs are started. 11 Furthermore, when these medications are used in combination with each other or with other medications, OH can be potentiated. However, one systematic review and meta-analysis of randomised controlled trials (RCTs) comparing tolerability and safety of ropinirole in monotherapy and adjuvant therapy with levodopa vs other dopamine agonists found cabergoline to be the only dopamine agonist associated with a higher risk of OH compared to placebo. 12
There are few systematic reviews or meta-analyses exploring the association between OH and antiparkinsonian medications. However, this is important to understand as it may aid clinical decision making in PD. Observational studies can be subject to unmeasured confounding, including confounding by indication, compared to RCTs. 13 Therefore, the aim of this systematic review and meta-analysis was to understand the association between OH and antiparkinsonian drugs compared to placebo, using randomised controlled trial evidence.
Methods
Study Design
A systematic review and meta-analysis of randomised controlled trials was conducted following the Preferred Reporting Items for Systematic Reviews and Meta Analyses (PRISMA) guidelines. 14 This review was conducted as part of a broader review exploring drugs causing OH, and a protocol was registered on PROSPERO (CRD42020168697). 15 Parkinson’s disease was explored separately, since mechanisms of OH and demographics are potentially different in this population compared to the general population. Ethics approval was not warranted.
Data Sources and Searches
The search strategies were developed with an information scientist (Appendix 1) without language restrictions and included a systematic literature search of EMBASE, MEDLINE and Web of Science from inception to November 23, 2020. The search strategy included drug terms, individual drug names (identified by the international non-proprietary name (INN) in the British National Formulary (BNF) and U.S. National Library of Medicine) and accounted for drugs with name changes. 16 A macro was developed to automate searches and facilitate the search strategy (Pulover’s macro creator version 5.2.8). Reference lists of eligible reports were reviewed, and authors contacted to supplement incomplete reports of the original papers.
Eligibility Criteria
Included studies were RCTs comparing any drug used in the management of motor features of PD with placebo, reporting incident OH as an adverse effect or outcome in adults ( ≥ 18 years). Studies comparing a drug to another drug were excluded, and if the population had a diagnosis other than PD (e.g. depression or restless legs syndrome). This was because the participant characteristics, such as age, were very different in these populations.
Study Selection
One reviewer (CB) screened all titles, abstracts and full-text articles reporting potentially eligible studies. A second reviewer (DN) screened 10% of titles and abstracts, and 3 reviewers (DN, HH and SM) screened 10% of all full-text articles. We calculated the Cohen’s κ statistic to assess interrater agreement regarding eligibility. Disagreements were arbitrated by a third reviewer (KW) when necessary. An online systematic review software (Rayyan, QCRI) facilitated literature screening. 17
Data Extraction
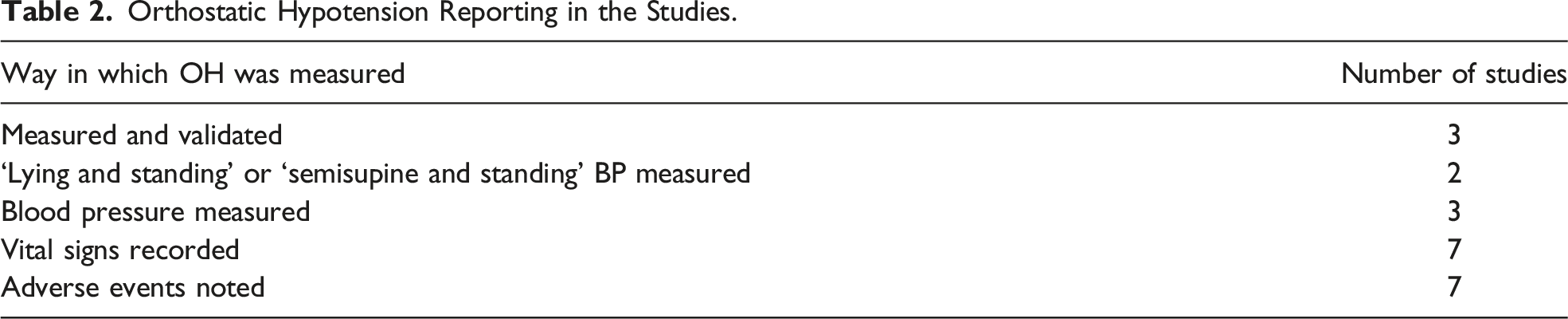
DN used a data extraction table for included studies, including patient demographics, length and severity of PD, drug characteristics, adjunct PD medication permitted, number of adverse events and method of reporting OH. Reporting of OH incidence was grouped into categories following expert consensus: • ‘measured and validated’ (a documented postural BP examination performed using a threshold of ≥ 20 mmHg systolic and/or ≥ 10 mmHg diastolic drop); • ‘Lying &Standing BP measured’ or ‘Semisupine &Standing BP measured’ (a documented postural BP examination performed without a specified threshold); • ‘BP measured’ (a documented BP examination only – but implied as postural since the study reports OH); • ‘physical examination’; • ‘vital signs recorded’; • ‘adverse events noted’; • ‘symptom report’.
We included all RCTs in the meta-analysis that compared drug to placebo and reported OH in any of the above categories.
Risk of Bias Assessment
DN assessed all included articles for risk of bias using the revised Cochrane risk of bias tool for randomised trials (RoB 2), 18 and CB independently assessed 20% of articles. Studies were assigned an overall score: ‘low’, ‘some concerns’ or ‘high’.
Data Synthesis, Analysis and Quality of Evidence
All RCTs comparing drug vs placebo with reporting of OH were grouped according to drug class, and results were pooled if 3 or more studies of a drug group were available. Further subgroup analysis was done according to individual drug. We estimated summary odds ratios for incident OH as a dichotomous outcome using fixed-effects Mantel–Haenszel statistics. Heterogeneity was assessed using the χ2 test and I2 statistic with an I2 > 50% representing substantial heterogeneity. We used Review Manager software version 5.4 (Cochrane). The Grading of Recommendations Assessment, Development and Evaluation was used to summarise the quality of evidence. 19
Results
Study Characteristics
36 940 citations were identified by the search related to OH as a side effect in any drug (not restricted to PD, as part of the original searches
15
). Out of these, 31 potentially eligible articles were retrieved in full-text related specifically to OH in PD (Figure 1). Ten full texts were excluded; as they were related to drugs not used to treat PD motor features or investigated drugs used to primarily treat other conditions in non-PD populations. There was substantial agreement between reviewers at the title and abstract stage (κ = .88) and full-text review stage (κ = .81). Results of the searches.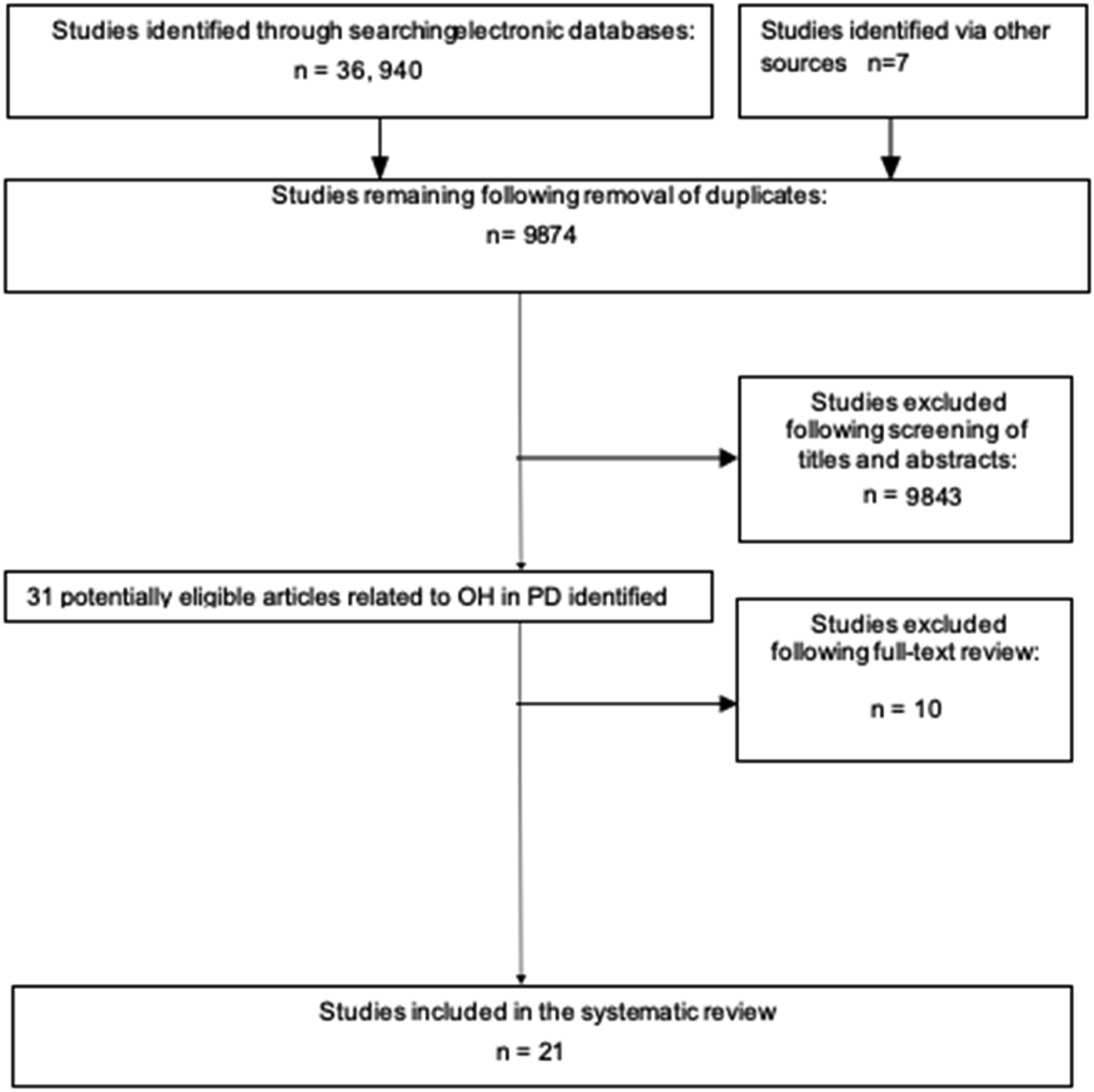
Study Characteristics.
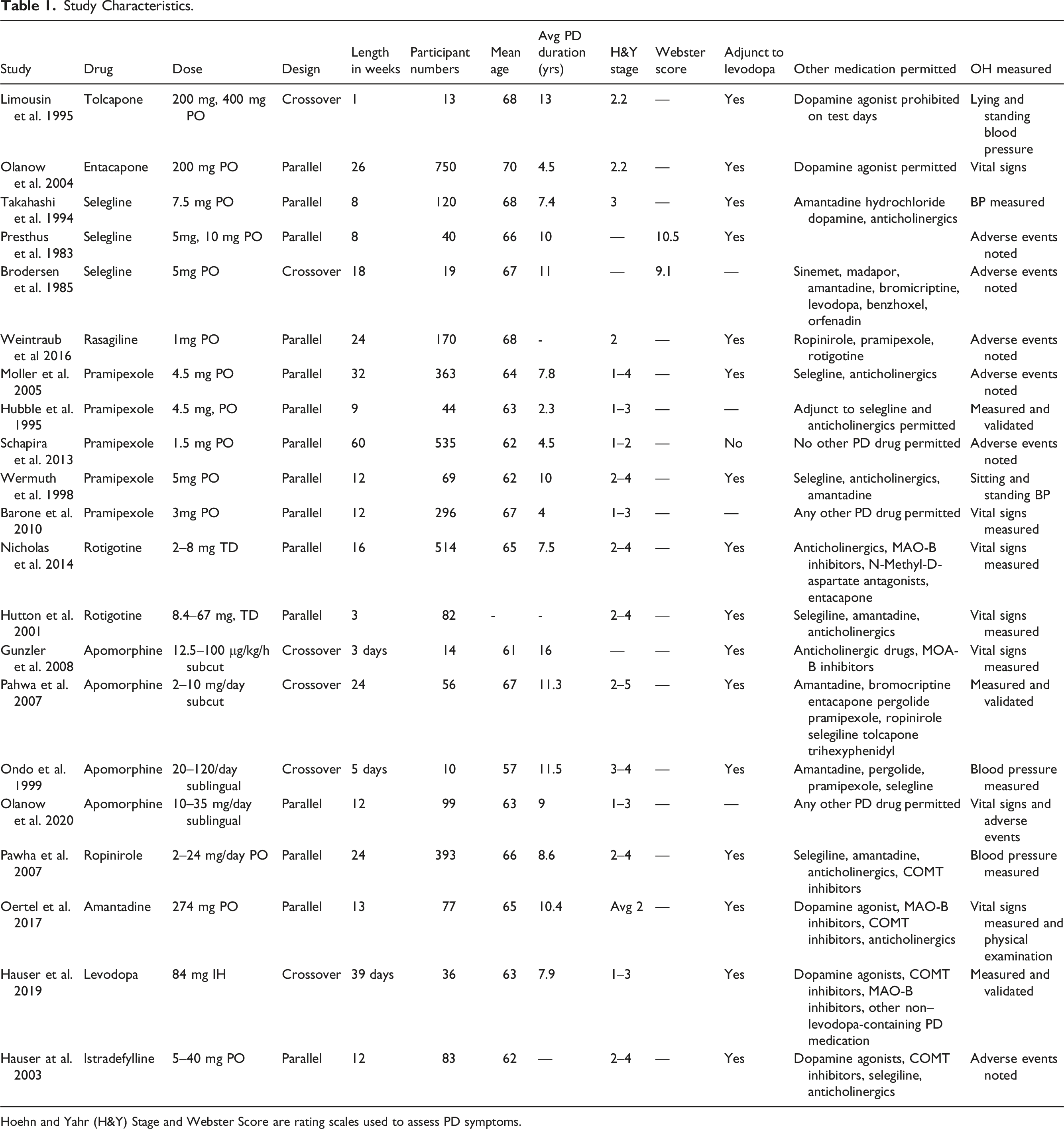
Hoehn and Yahr (H&Y) Stage and Webster Score are rating scales used to assess PD symptoms.
Orthostatic Hypotension Reporting in the Studies.
Sixteen out of 21 studies investigated the study drug as an adjunct to levodopa and 20/21 permitted the use of other PD medications. Only one study investigated the drug as monotherapy compared to placebo and did not permit the use of any other PD medication. 28
Risk of Bias and Quality of Evidence
According to Rob 2, 6/21 studies had an overall ‘low’ risk of bias and 15/21 studies scored either ‘some concern’ or ‘high’. This was mostly due to studies not describing the method of measuring OH and lacking a pre-specified plan for analysis (Appendix 2).
The GRADE judgements are outlined in Appendix 3 for drug groups with 3 or more studies suitable for meta-analysis (MAO-B Inhibitors and dopamine agonists). The certainty of evidence varied. It was low for dopamine agonists and very low for MAO-B Inhibitors. This was due to high risk of bias in many studies, and it was unclear how and when OH was measured.
MAO-B Inhibitors
Four RCTs investigated MAO-B inhibitors.22-25 3 RCTs investigated selegiline (5–10 mg) and 1 rasagiline (1 mg). Three were parallel and 1 was a crossover trial. Participant numbers ranged from 19 to 322 and mean age 67 years. Study duration ranged between 8 and 24 weeks. The average disease duration was not available for Weintraub et al., but for the remaining 3 studies, it was 8.4 years. In the study conducted by Takahashi et al., OH was determined by measuring BP at visits, while in the others adverse events were noted. In the meta-analysis, MAO-B Inhibitors for treatment of PD were not associated with an increased risk of OH compared with placebo (OR 2.28 [95% CI .81–6.46]) (Figure 2).
Dopamine Agonists
Thirteen RCTs investigated the association of dopamine agonists with OH in PD:
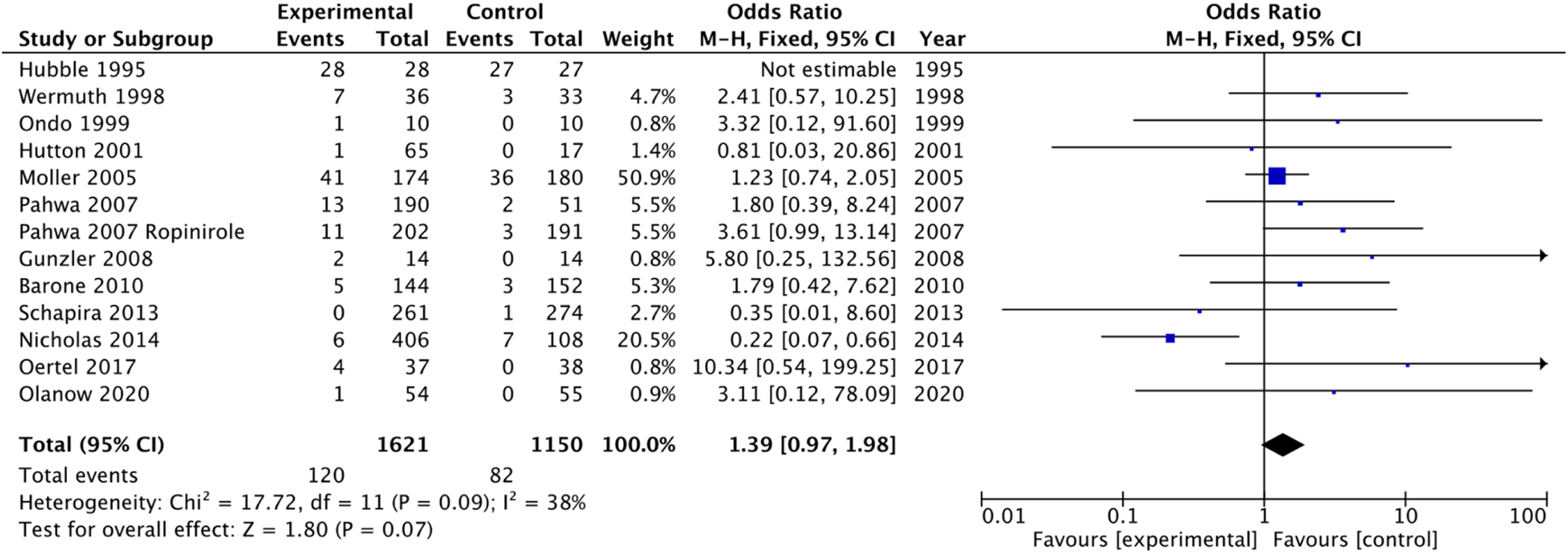
The meta-analysis of these studies did not demonstrate an increased risk of OH with dopamine agonists treatment compared with placebo (OR 1.39 [95% CI .97–1.98]) (Figure 3).
Pramipexole
Five parallel RCTs investigated pramipexole 1.5–5 mg. Participant numbers ranged from 44 to 535. The mean age was 64 years and mean disease duration was 5.5 years.26-30 OH was determined in a range of ways (Table 1) and study duration ranged between 9 and 50 weeks. Of interest, the study that used a measured and validated method for assessing BP found all patients had at least 1 episode of OH during the study period. 27 However, only 7/28 in the treatment group (25%) and 5/27 in the placebo group (18.5%) experienced symptoms – these did not require any treatment, nor were they dose limiting. Meta-analysis showed pramipexole did not demonstrate an association with an increased risk of OH, compared with placebo (OR 1.33 [95% CI .85–2.07]) (Figure 4).
Apomorphine
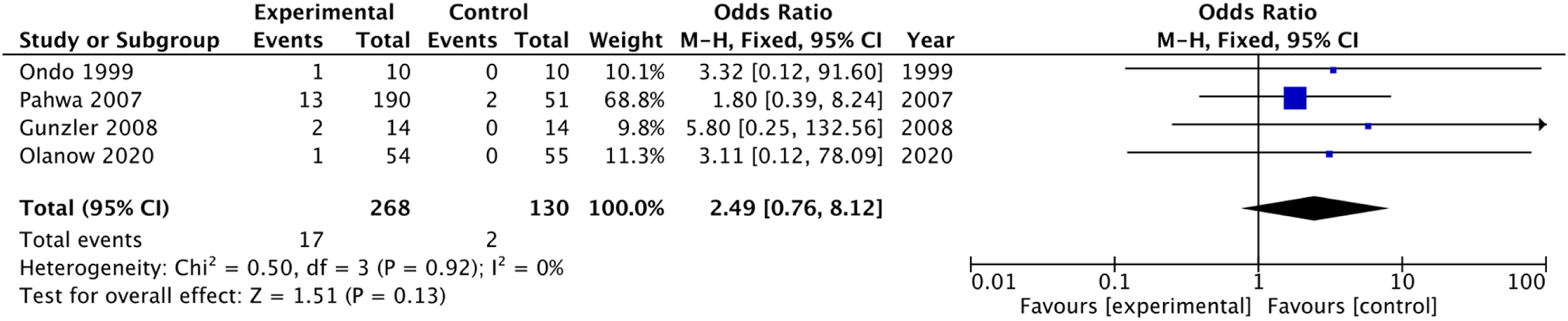
Three crossover and one parallel RCT investigated apomorphine, with study periods ranging between 3 days and 24 weeks with 10–99 participants, mean age 63 years and disease duration was 10.4 years.33-35,40 In 2 studies, vital signs were recorded,33,40 while BP was measured in another, 35 and 1 study described a postural BP examination performed using a threshold of ≥20 mmHg systolic /≥ 10 mmHg diastolic drop. 34 Meta-analysis did not demonstrate an association of apomorphine with an increased risk of OH, compared with placebo (OR 2.49 [95% CI .76–8.12]) (Figure 5).
Rotigotine
Two parallel RCTs investigated rotigotine at doses of 2 to 76 mg in participant numbers ranging from 82–514 and study duration ranging between 3 and 16 weeks.31,32 Nicholas et al. reported disease duration and age of participants; and the average was 7.5 years and 65 years respectively. In both studies, OH was determined by measuring vital Figure 2 signs at study visits. Hutton et al. found the incidence of OH events was 2% in the treatment group (1/65) compared to 0% in the placebo group (0/17).
32
While Nicholas et al. found the incidence of OH events was 1% in the treatment group (6/406) compared to 6% in the placebo group (7/108).
31
The authors also investigated adverse events according to age; a greater proportion of participants over 75 years old experienced OH in both groups. This was 10% (2/20) and 3% (2/69) in the placebo and rotigotine group, respectively. Nicholas et al.’s study was the only study that favoured the dopamine agonist compared to placebo (Figure 3), which is probably due to small participant numbers. The authors did not include participant characteristics, such as past medical history or a medication list. Forest plot with all MAO-B inhibitors studies. Forest plot with all dopamine agonist studies.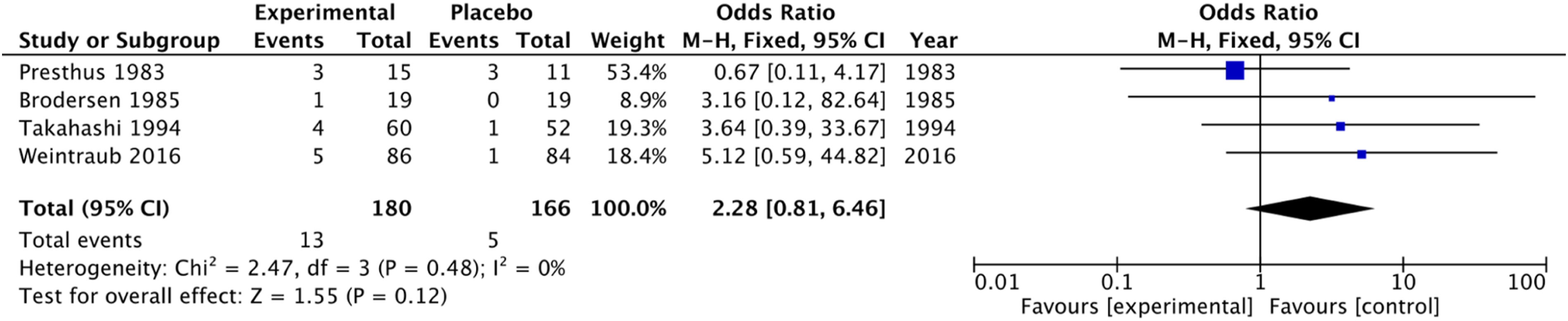
Ropinirole
One study investigated 2–24 mg oral ropinirole in a 24 week parallel RCT with 393 participants, mean age 66 years and disease duration was 8.6 years. 36 OH was determined by measuring BP during 12 study visits. The incidence of OH events was 5% in the treatment group (11/202) compared to 2% in the placebo group (3/191), but there was no significance testing.
Other Antiparkinsonian Medications
COMT Inhibitors
Two RCTs investigated OH in the treatment of PD by oral COMT inhibitors, in participant numbers ranging from 13–750 and study duration ranging between 1 and 26 weeks. Mean age was 70 years, and disease duration was 4.6 years. Limousin et al. investigated 200 mg and 400 mg tolcapone vs placebo
20
in a crossover trial of 7 days with 13 participants and assessed lying and standing BP. Olanow et al. compared 200 mg entacapone with placebo in a parallel trial of 26 weeks with 750 participants recording vital signs.
21
The number of participants affected by OH was not reported in the study by Limousin et al., only the mean decrease in BP for the tolcapone group. The mean decrease in lying BP was 35/17 mmHg and in standing BP 38/22mmHg, but the authors report this decrease was similar in tolcapone and placebo groups.
20
Olanow et al. found the proportion of participants with OH was similar in both the entacapone and placebo groups, 47/373 (13%) and 51/377 (14%), respectively.
21
These studies suggest COMT inhibitors were not associated with an increase in OH compared to placebo, but the strength of evidence is low. Forest plot with pramipexole studies. Forest plot with apomorphine studies. Subgroup analysis forest plot of studies in the top 2 categories of OH reporting.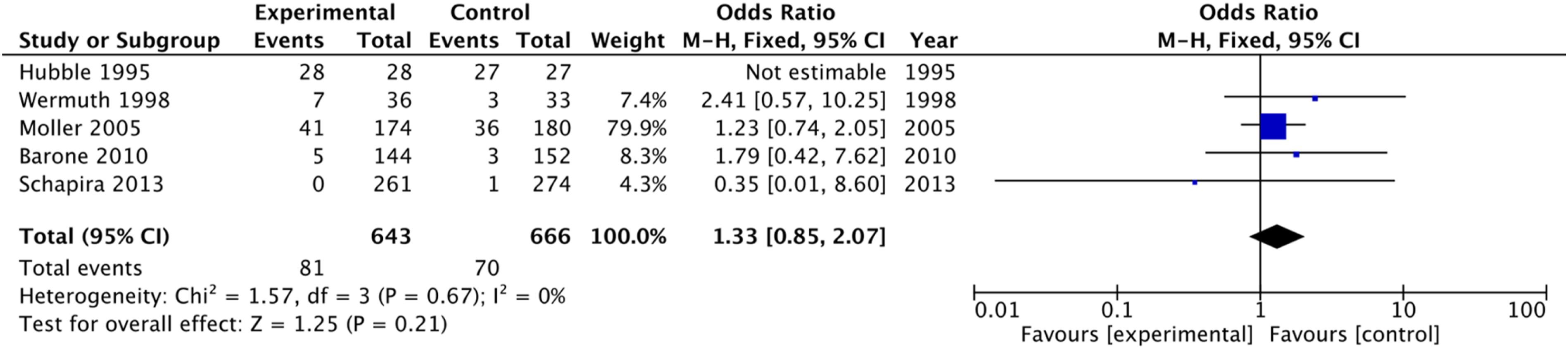
Amantadine
One study investigated 274 mg oral amantadine in a 13 week parallel RCT with 77 participants, mean age 65 years and disease duration 10.4 years. 37 OH was determined by measuring vital signs and performing a physical examination during 9 visits. There were also safety follow up visits but is unclear if BP was measured during these. The incidence of OH events was 10% in the treatment group (4/37) compared to 0% in the placebo group (0/38). However, the sample size is small and the study likely underpowered.
Adenosine Receptor Antagonist
One study investigated 5–40 mg istradefylline in a 12 week parallel RCT with 83 participants, mean age was 62 years and disease duration was not reported. 39 The incidence of OH events was 6% in the treatment group (3/54) compared to 10% in the placebo group (3/29). The strength of evidence is low, as the authors state OH was detected by ‘adverse events at each visit’, and it is unclear how BP was measured.
Levodopa
One study investigated 84 mg inhaled levodopa in a 39 day crossover RCT with 36 participants, mean age 63 years and disease duration 7.9 years. 38 Postural BP examination was performed using a threshold of ≥ 20 mmHg systolic /≥ 10 mmHg diastolic drop, on 2 observation days separated by an interval of 1 to 7 days. It was measured 30 mins before the dose was given and every 30 minutes for 3 hours afterwards. The incidence of OH events was similar, 17% in the treatment group (6/36) compared to 19% in the placebo group (7/36).
Subgroup Analysis
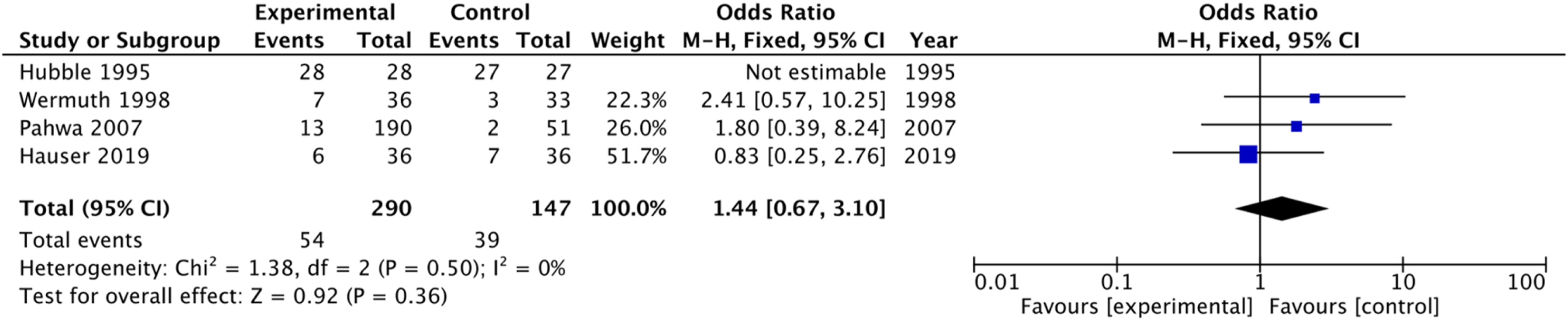
Two studies amongst all included studies reported a ‘measured and validated’ method for assessing OH and 2 recorded ‘lying and standing BP’ or ‘semisupine and standing BP’.27,29,34,38 These 4 studies were therefore in the top 2 categories of OH reporting and included in a subgroup analysis. Limousin et al., also measured the lying and standing BP, but this was not reported for individual participants, and therefore, the data could not be included in the analysis. 20 This meta-analysis found no difference in risk of OH between the trial medications compared with placebo (OR 1.44 [95% CI .67–3.10]) (Figure 6).
Discussion
Our narrative synthesis did not provide conclusive evidence that OH incidence was greater in antiparkinsonian medication compared to placebo, and meta-analysis did not demonstrate a significant difference between MAO-B inhibitors or dopamine agonists in OH incidence compared to placebo. Similarly, the meta-analyses of studies of apomorphine, pramipexole and studies that were in the top 2 categories of OH reporting (‘measured and validated’, ‘lying and standing measured’ or ‘semisupine and standing measured’) did not demonstrate significant differences than the placebo group. These findings are in contrast to what is observed in clinical practice and previous observational studies.6,7 We believe this discrepancy is likely due to issues of poor reporting in comparison to populations studies.
Despite OH being a recognised complication of PD and its treatment, RCTs rarely used the classical definition of OH to report OH. In most RCTs reporting OH, this was recorded as an adverse event or as a measurement of vital signs. However, as OH is not included in the common terminology criteria for adverse events (CTCAE) system, the standard reporting method for adverse events in most clinical trials, 41 many trials likely, would have reported ‘dizziness’ or ‘hypotension’. Few trials specifically assess lying and standing OH, and therefore, only symptomatic OH was likely to be reported as an adverse event. This is likely to be an underestimation of the true incidence of OH in PD, particularly as the majority of OH in PD is asymptomatic. 1 Many studies were small with low incidence rates that precluded significance testing. As OH was not the primary outcome and assessed specifically in many studies, many studies are rated as having ‘some concern’ or ‘high’ risk of bias, and the GRADE assessment was either low or very low quality.
The studies included in this systematic review may also be overrepresenting younger populations and those in the earlier stages of the disease. The average age was 57–70 years old, whereas the greatest prevalence of PD is seen in people aged 70–84. 42 This population is typical for that seen in RCTs in PD, which are often younger, as traditionally older people were underrepresented and excluded from trials despite higher rates of chronic diseases. 43 Similarly, most of the trials were conducted in earlier disease stages, where OH is less common than in advanced stages. As both PD and ageing are associated with other risk factors for OH, including PD progression, increased susceptibility to OH at baseline, antiparkinsonian medication, non-PD medications and comorbidities, 4 the likely rate of OH with these medications in PD is higher. However, no study explored this complexity. Many did not describe past medical or concurrent medication history, which is important in this population.
Furthermore, the relatively low event rates and relatively short trial duration of some studies (Table 1) may have contributed to the lack of a significant finding. However, a previous meta-analysis of the efficacy and safety of non-ergot dopamine agonists in PD also found no difference in the incidence of OH between dopamine agonists and placebo (RR .84 [95% CI .20–3.55]). However, this study only included data from 3 trials, and was limited by the same data limitations as this study, for example, short observation periods in some studies. 44 A further study exploring the safety of ropinirole vs other dopamine agonists and levodopa explored OH in 665 participants and found cabergoline to be the only dopamine agonist to be associated with a higher risk of OH when prescribed with levodopa compared to placebo. 12 Our systematic review used a broader search strategy, but theirs only searched for dopamine agonists and did not focus specifically on OH as an adverse outcome, which explains why they found fewer number of studies.
A Cochrane review of RCTs evaluating the safety of adjuvant treatment to levodopa in PD reported that dopamine agonists increased the odds of hypotension (OR 1.46 [95% 1.15, −1.84]) when compared to placebo, but COMT inhibitors and MAO-B inhibitors did not. This meta-analysis included 20 studies that recorded ‘hypotension’ or ‘orthostatic hypotension’ and the authors did not differentiate between the 2 terms. 45 As mentioned above, studies are more likely to report ‘hypotension’ or ‘dizziness’ to indicate OH, as both are common terminology criteria for adverse events (CTCAE), instead of ‘orthostatic hypotension’. 41 However, there are differences compared to our review. In the Cochrane review, all adverse effects were explored, while we examined OH specifically. They also only focused on patients who were receiving levodopa in addition to other PD medication, while our review covered all drugs used in the treatment of motor symptoms in PD. Finally, their search was conducted in 2008, and we have identified 7 new studies published since then, which are included in our review.
Some other systematic reviews and meta-analyses on PD drug safety and efficacy exploring ‘hypotension’ and ‘dizziness’ have found associations with the use of some PD medications and OH. For example, a meta-analysis of 17 studies found an increased risk of hypotension when ropinirole was compared with placebo, but this was not the case for pramipexole (6.46, 95% CI 1.47–28.28 for ropinirole and 1.65, 95% CI .88–3.08 for pramipexole). 46 However another Cochrane review exploring dopamine agonist therapy in early PD did not find an association between dopamine agonists and hypotension when compared to placebo (OR 1.73 [95% .9–3.35]), including pooled results from 3 studies. The authors found dopamine agonists did increase the odds of developing dizziness, and these results were from 7 pooled studies (OR 1.9 [95% 1.32–2.74]). 47 This illustrates how differences in assessment of adverse side effects can lead to different conclusions.
Unlike the other studies investigating dopamine agonists, Nicholas et al. found rotigotine was protective against OH, where 6% of the placebo and 1% of the treatment group experienced OH, respectively. 31 The participant numbers in each group ranged from 94–108 and were therefore small, which may have contributed to the result. Rotigotine stimulates dopamine D1–D3 receptors and transdermal application avoids the ‘first pass’ effect but also facilitates long acting profiles and hence systemic exposure over 24 hours. Also, plasma profiles have shown stable concentrations after multiple dosages, when applying multiple days of patches, which may possibly attenuate risk of side effects. 48 Rotigotine is administered in transdermal patch formulation. Interestingly, a recent study reported the lack of clarity in the effect of route of administration on the OH mechanism, and therefore, further investigations are required whether rotigotine’s effects could be attributed to transdermal delivery. 49
Furthermore, a recent drug vs drug vs placebo RCT compared ropinirole, rotigotine and placebo and found the incidence of OH to be 7/167 (4.2%), 5/168 (3%) and 4/85 (4.7%), respectively, where OH was reported less frequently in the rotigotine group compared to placebo. 50 These results were not significant as P values were > .5, and therefore support our overall findings.
Strengths and Limitations
Strengths of this review include a comprehensive literature search aided by an information scientist and according to published guidelines. 14 There was also substantial agreement between reviewers, and a broad multidisciplinary team was involved in the interpretation of results, including primary care physicians, a neurologist and pharmacist. However, our systematic review only explored placebo vs drug studies, not drug vs drug RCTs, which tend to be more recent and would have provided additional data. As discussed above, we searched for studies specifically mentioning OH, rather than terms that might suggest presence of OH, which is likely to have led to an underestimation of the rate of OH, highlighting the need to specifically assess OH in clinical trials of medications reported to be associated with this adverse effect. Furthermore, the RCTs rarely included patients with more advanced disease and multiple other medications that may contribute to OH.
Future Research and Implications
As generally acknowledged, RCTs should strive to include a study population that truly represents the PD population, including older participants (>75 years old), those with multimorbidity and longer disease duration. Reporting of adverse event studies need to adhere to standard reporting frameworks and additional reporting of adverse events that are particularly relevant to the PD population, such as OH, should also be included in reporting adverse events in future PD trials.
Conclusion
In this systematic review and meta-analysis of RCTs reporting OH in antiparkinsonian medications, these drugs were not significantly associated with an increased risk of OH compared to placebo. However, the limitations in reporting OH and the populations included are likely to have resulted in an underestimation of this potential adverse effect.
Footnotes
Author Contributions
All authors contributed substantially to the conception, design of the work, analysis, and interpretation of data for the work; drafted the work or revised it critically for important intellectual content. All approved the final version to be published; and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Danielle Nimmons is an In-Practice Fellow supported by the Department of Health and Social Care and the National Institute for Health Research.
Search Strategy.
Risk of Bias.
GRADE Criteria.
Quality assessment
No of patients
Effect
Quality of evidence for OH
Recommendation
No of studies
Design
Risk of bias
Inconsistency
Indirectness
Imprecision
Other considerations
Drug
Placebo
95% CI
Odds ratio
MAOBI
4
RCT
Most information is from studies at high ROB
No
Yes - unclear how and when OH was measured in most studies
Wide CI
Downgraded due to high risk of bias and small studies
180
166
(.81, 6.46)
2.28
Very low
No increased odds of OH compared to placebo. It is unclear how and when OH was measured, most studies had a high risk of bias because of this. OH therefore needs better reporting
Dopamine agonists
13
RCT
Most information is from studies at high ROB
No
Yes - unclear how and when OH was measured in most studies
No
Downgraded due to high risk of bias
1621
1150
(.97, 1.98)
1.39
Low
No increased odds of OH compared to placebo. It is unclear how and when OH was measured, most studies had a high risk of bias because of this. OH therefore needs better reporting