
Abstract
Background:
Pain in Parkinson’s is problematic but under treated in clinical practice. Healthcare professionals must understand the impact of pain in Parkinson’s and patient preferences for management.
Objective:
To understand the impact of pain in Parkinson’s and to understand current management and preferences for pain management.
Methods:
We conducted a national survey with 115 people with Parkinson’s (PwP) and 10 carers. Both closed and open questions were used. The questions focused on how pain affected the individual, healthcare professional involvement in supporting pain management, current pain management strategies and views on future pain management interventions. We used descriptive statistics to summarize closed responses and thematic analysis to summarize open question responses.
Results:
70% of participants reported pain impacted their daily life. Pain had a multifactorial impact on participants, affecting movement, mood and quality of life. Improved pain management was viewed to have the potential to address each of these challenges. Pain affected a number of different sites, with low back pain and multiple sites being most frequently reported. Exercise was the most frequently noted strategy (38%) recommended by healthcare professionals for pain management. PwP would value involvement from healthcare professionals for future pain management, but also would like to self-manage the condition. Medication was not suggested as a first line strategy.
Conclusions:
Despite reporting engagement in some strategies to manage pain, pain still has a wide-ranging impact on the daily life of PwP. Results from this survey highlight the need to better support PwP to manage the impact of pain.
Pain can affect up to 85% of people with Parkinson’s (PwP)1,2 yet is poorly recognized and managed within clinical practice, 3 which can have significant consequences on quality of life. 4 Pain is biopsychosocial and has a multifactorial impact on individuals lives, yet this has been found to not be acknowledged by healthcare professionals. 5 Despite the problem of pain, there are limited options for pain management in Parkinson’s. 6 Between 50% 7 and 63% 8 of those reporting pain have not received any pharmacological or non-pharmacological treatment for their pain, which has been attributed to an inadequate awareness of clinicians. 9 There is a need to increase education concerning pain in Parkinson’s for healthcare professionals and to develop options for both pharmacological and non-pharmacological management of pain. 10 Currently, it is unknown if pharmacological therapy will relieve pain in Parkinson's due to the distinct mechanisms involved with pain processing interacting with Parkinson’s pathophysiology. 11 A small number of cross sectional studies have provided some detail on how PwP manage their pain. Physiotherapy and pain medication are the most frequently cited approaches.7,8,12 However, this must be considered in the wider context of a number of individuals not receiving any treatment. There is limited literature to date exploring the impact of pain, current management strategies and the preferences of PwP for future interventions. Understanding of these factors will help to inform the development of pain management for PwP.
Currently there is only a small amount of research that focuses specifically on PwP views on pain. This work aimed to enable PwP and their carers to share their experiences of pain and pain management in their own words and, importantly, to share their thoughts on what pain management interventions should look like. This survey forms part of a wider piece of patient and public involvement to inform the direction of a future research study about pain management in Parkinson’s.
Materials and Methods
Ethics
The survey was approved by Northumbria University Research Ethics committee.
Informed consent was obtained at the start of the survey. We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this work is consistent with those guidelines.
Developing the Survey
In order to ensure the survey was clear and that questions focused on aspects important to PwP, we considered it vital to work with PwP to develop the survey questions. JN, AA and NR drafted questions based on existing literature and the research team’s plans for a future study. The draft survey was then sent to 5 people affected by Parkinson’s (3 male & 2 female; time since diagnosis: ranging between 2-15 years) who provided feedback on the clarity of questions and recommended changes. As a result of this feedback, a number of amendments were made including reducing the length of the survey, refining the focus and providing more detail for certain questions.
Recruitment and Procedures
The survey was administered in March 2020 by Parkinson’s UK on SmartSurvey, an online survey software and questionnaire tool. Participants were recruited via Parkinson’s UK Research Support Network—an online network that brings together people driven to help find a cure and better treatments for Parkinson’s. The Research Support Network has around 6,000 members (as of February 2020), the vast majority of whom are PwP and partners, family members and carers of those with the condition living in the UK. An email was sent to the network inviting people to complete the survey, and the survey was also included in the Network’s monthly e-newsletter.
The survey gathered feedback from both PwP and partners, family members and carers. The target population was those who had experience of pain. The question set was the same for the 2 groups, aside from minor variations in wording to make questions applicable. The first question required the individual to indicate if they were a person with Parkinson’s or a partner, family member or carer so the appropriate question set could be shown (supplementary material). The survey consisted of 2 parts. Part 1 included 8 questions focused on how pain affected the individual (or their partner/family member/person they cared for), their experience of healthcare professional involvement in supporting pain management, current pain management strategies and views on future pain management interventions. Three questions collecting demographic information were also included. Part 2 consisted of a further 9 questions focused on feedback for the specific design of a study. Results from part 2 are not reported here. The survey did not collect any identifying information. Participants were able to skip any questions they did not wish to answer. The survey included a mixture of closed and open-ended questions. Open ended questions were deemed important to allow participants to develop responses due to the limited research in this area, and also provided an opportunity for participants to highlight any additional points they deemed relevant.
Data Analysis
We used descriptive statistics to characterize the sample. Categorical data were analyzed via SPSS (version 21) to generate frequencies. Open ended questions were summarized using thematic coding analysis. 12 These were informed by the aims of the research, while allowing new themes to emerge. One author (JN) read through the responses, coded these and then categorized into themes. A second author (KB) independently categorized the coded responses and a final presentation of themes was agreed through a peer debriefing meeting between the 2 authors and discussed with the wider team.
Results
We received responses from 115 PwP and 10 carers. Almost all the questions (except 3) were focused on the experience of the person with Parkinson’s, with partners, family members and carers responding on the person’s behalf. Therefore, the reporting of “participants” refers to the information captured from both groups of respondents (N = 125), unless specified otherwise. All participants answered the closed questions (see Table 1), and the number of responses to the open questions is indicated within the Tables 2-5. Participants could choose more than 1 answer to the closed and open questions.
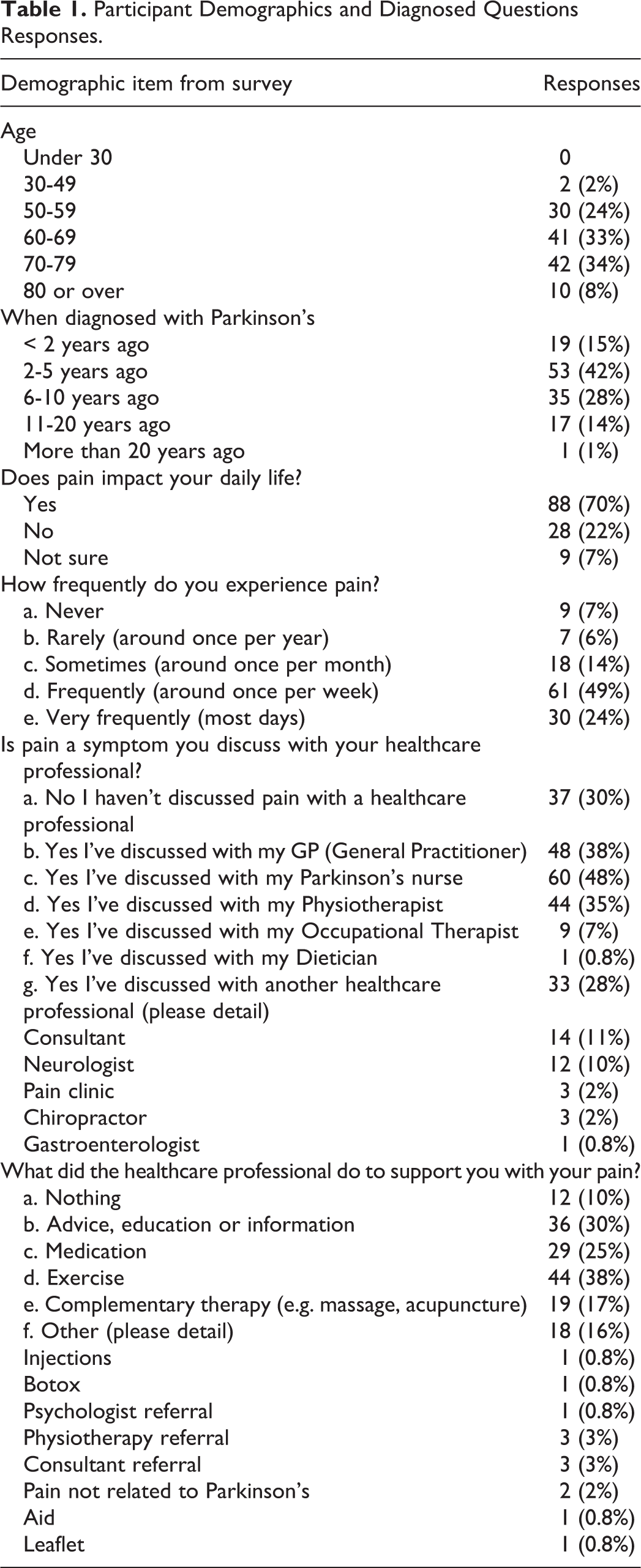
Participant Demographics and Diagnosed Questions Responses.
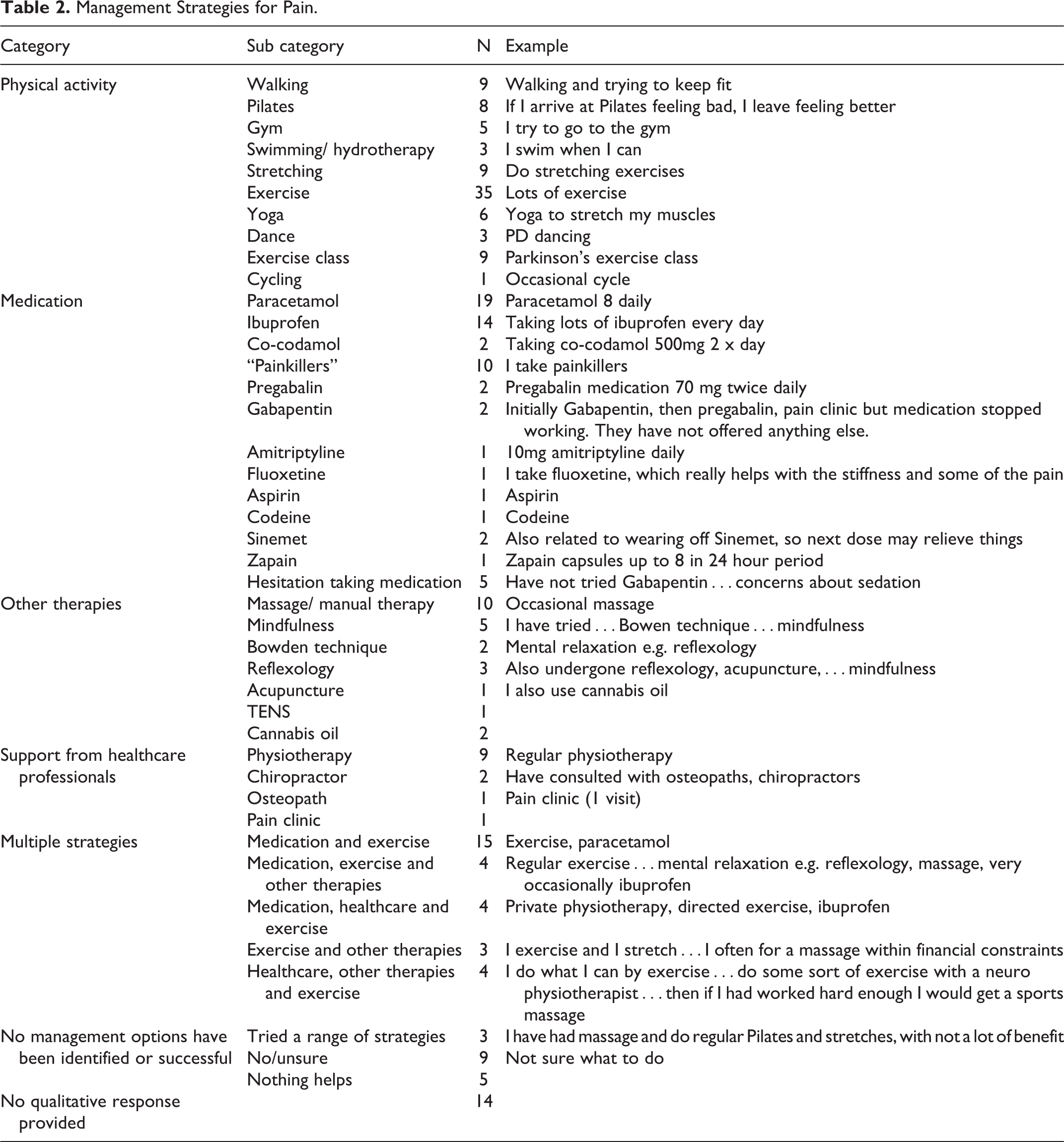
Management Strategies for Pain.
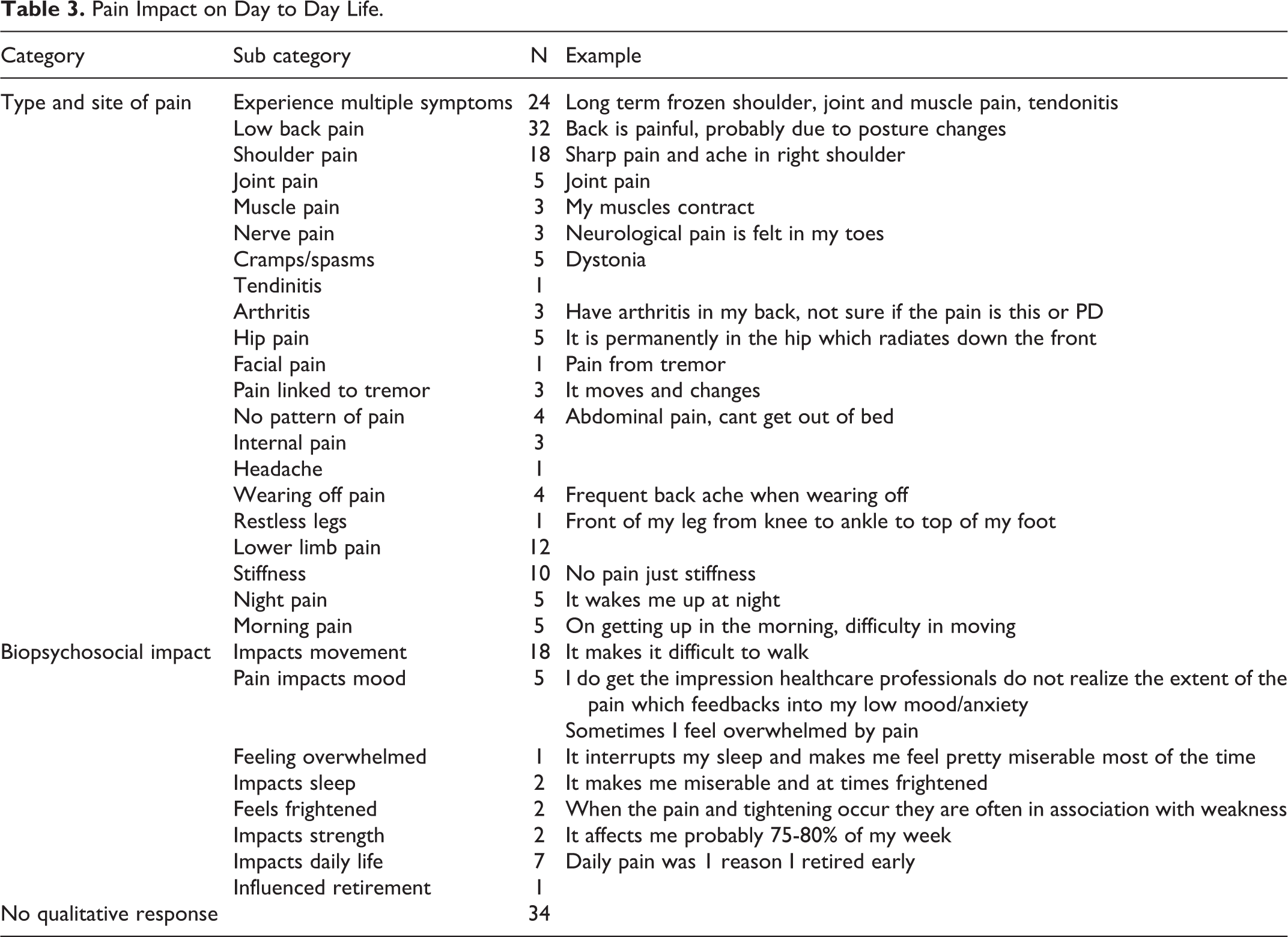
Pain Impact on Day to Day Life.
Expectations From a Pain Management Intervention.a
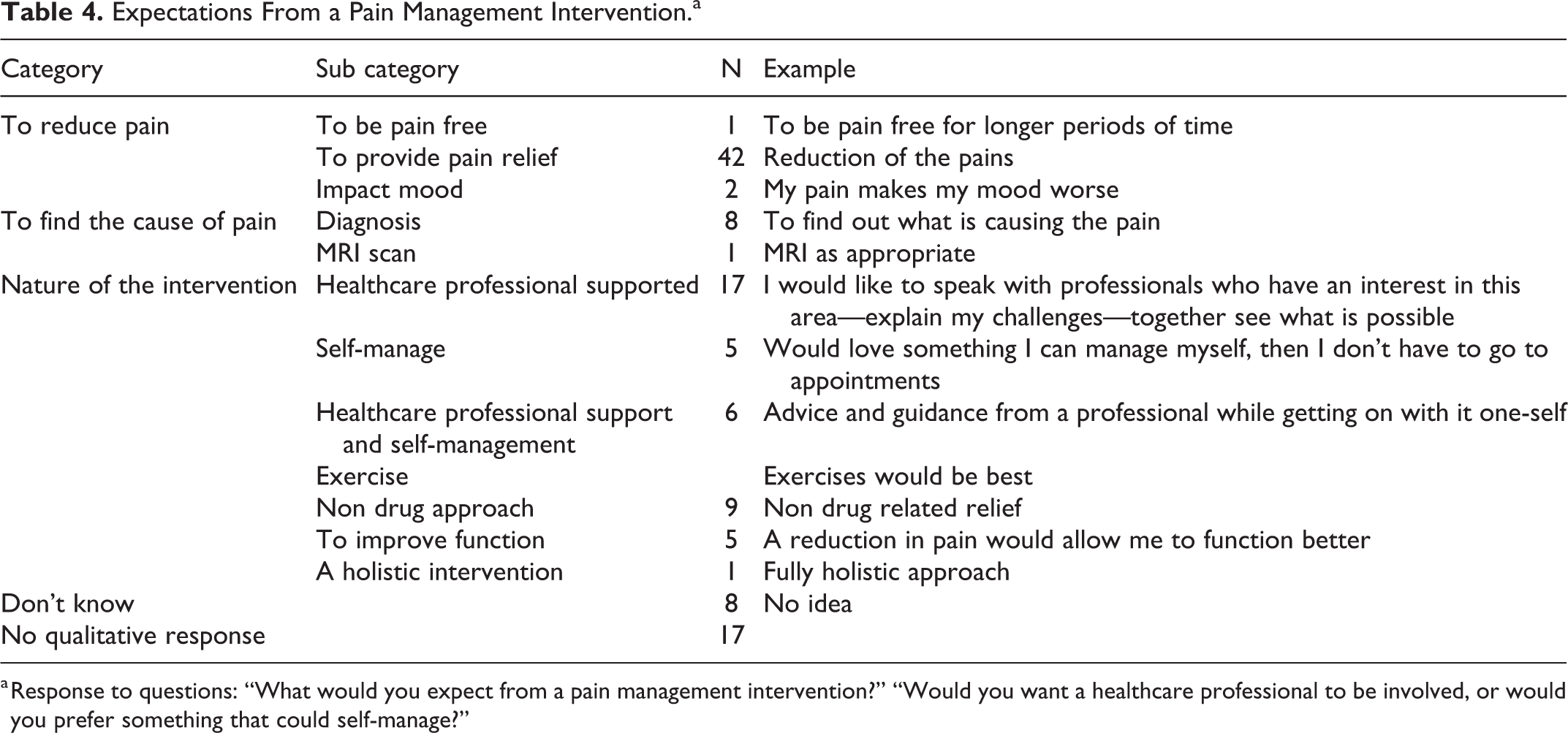
a Response to questions: “What would you expect from a pain management intervention?” “Would you want a healthcare professional to be involved, or would you prefer something that could self-manage?”
Expected Impact of a Better Pain Management Strategy?a
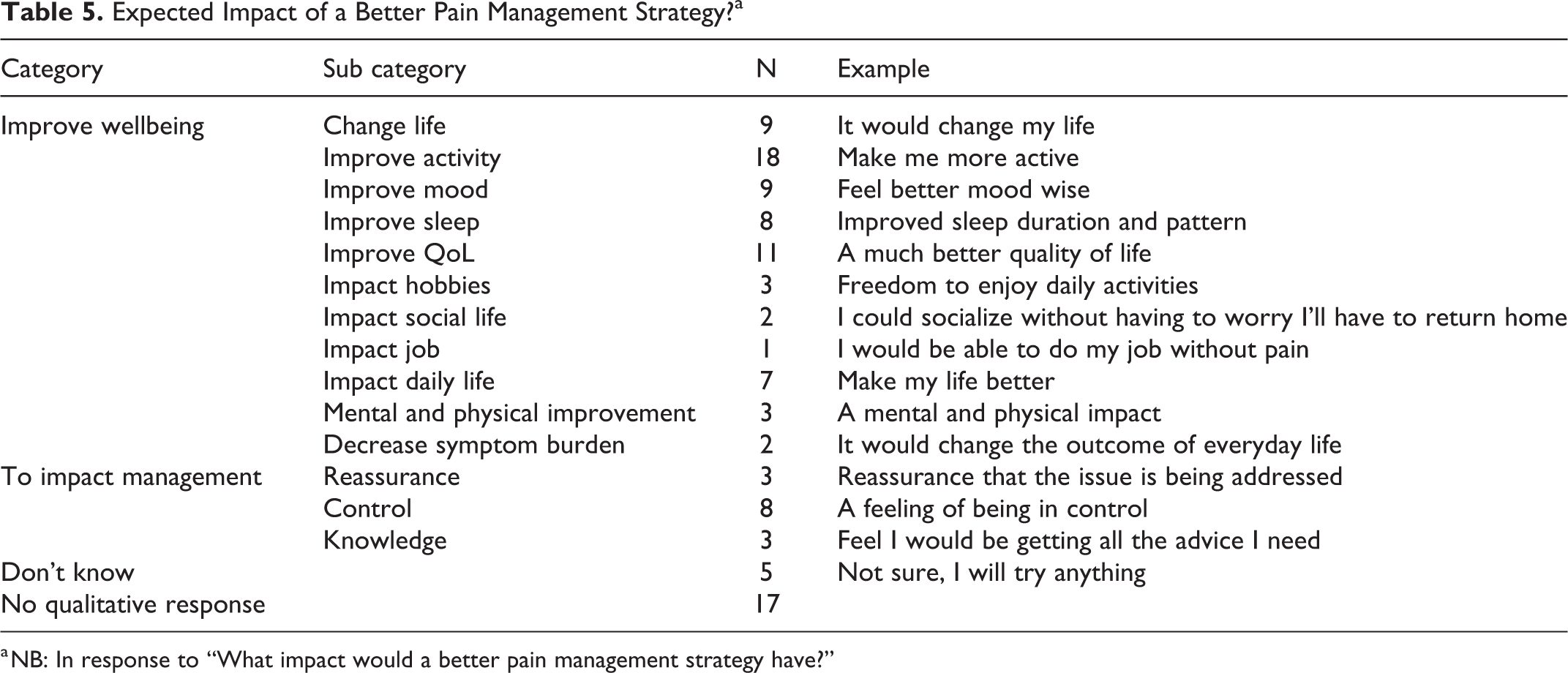
a NB: In response to “What impact would a better pain management strategy have?”
Closed Questions
Please see Table 1 for details of participant characteristics. 75% of participants were aged 60 or over. 42% had been diagnosed between 2 and 5 years. A large majority of participants indicated pain impacted their daily life (70%), with 49% experiencing pain multiple times per week and 24% experiencing pain multiple times per day. The healthcare professional (HCP) with whom the highest number of participants had discussed their pain was their Parkinson’s nurse (48%) followed by a general practitioner (38%) and a physiotherapist (35%). 10% of PwP discussed pain with their neurologist. Exercise was the most frequently noted mechanism by which healthcare professionals supported individuals with their pain (38%).
Open Questions
The open-ended questions provide detailed information regarding the current impact of pain, it’s management and future management suggestions.
The impact and current management of pain in Parkinson’s
When asked about what pain management strategies PwP used, physical activity, paracetamol and ibuprofen were the most frequently reported. Some individuals described multiple strategies, with some participants identifying a wide range of strategies that had been tried to manage their pain. Other participants acknowledged that no management options had been successful to date or not being sure how to manage their pain. While medication was cited, some participants expressed reluctance at taking this. Parkinson’s medication was not linked with pain. Five individuals noted painful muscle spasms and cramps. Some participants had tried other therapies such as massage and mindfulness. Table 2 provides a description of each of the pain management strategies and examples identified by participants. When asked if pain impacted their daily life, responses focused around describing the location of their pain and the timing of this, alongside capturing the biopsychosocial impact that this can have. Pain was reported in a number of locations, with low back pain being the most frequently reported, alongside having pain in multiple locations. Wearing off pain was noted by few participants. Pain made movement difficult for some participants, alongside having a negative impact on mood and wider daily life. Detail surrounding these open-ended responses is provided in Table 3.
Pain management needs for people with Parkinson’s
Participants identified the need for pain management interventions to provide pain relief. Involving healthcare professionals with pain management was deemed important, with some individuals viewing it necessary to be able to self-manage their pain or to have a combination of support and self-management. When asked an open question about future pain management medication was not mentioned as a suggestion for pain management, however some participants highlighted a non-drug approach to be the preference. Table 4 provides further detail pertaining to the nature of pain management interventions suggested by participants. Participants indicated improved pain management would provide an overall positive impact on general wellbeing, in particular improving activity and quality of life. An impact on mood, sleep and daily life were often referred to alongside improved pain management as having the potential to “change the life” of some individuals. A sense of being in control of pain was deemed important by some. Table 5 elaborates on these findings, with specific examples provided.
Discussion
This survey has identified the anticipated impact improved pain management strategies would have on PwP living with pain, alongside preferences on how such strategies should be delivered. Studies to date present findings on strategies that have been tried for PwP but have involved little dialogue with people about their preferences. This survey provides a direct account of what PwP would like from future pain management interventions and the potential impact they felt that this would have.
Pain was highlighted as having a biopsychosocial impact, with movement, mood and daily life each being cited as being impacted by pain. Despair and despondency associated with living with pain in Parkinson’s has been reported in a qualitative study (n = 4). 5 This study reported individuals experiencing high levels of pain which had psychological and social impacts. Some participants tried management strategies such as exercise, while others felt this to not be possible. Having a sense of control over pain was key. A disconnect between healthcare professionals and PwP was highlighted, with individuals needs surrounding pain not addressed. 5 While small samples can be expected in this type of study, transferability of these findings is limited as a stand-alone study. The current survey adds to these findings, highlighting on a larger scale the wide-ranging impact of pain, and variation among the use of strategies. A key development with the current survey is individuals reporting how improved pain management would impact their daily life. A feeling of overall improved wellbeing including improved activity, mood and quality of life were each highlighted if pain were to be better managed. Pain can influence all aspects of someone’s life 13 and be a particularly bothersome symptom. 14 Individuals in this survey noted the dominating effect of pain, and the overarching positive impact that a reduction in pain could have on daily life.
Exercise is encouraged for PwP as a key aspect of the management of the condition.3,15 The current survey identified that exercise is a frequently advised strategy by healthcare professionals to support the management of pain. At early stages of Parkinson’s it has been found that activity levels are reduced compared to age matched controls. 16 Pain can be a barrier to exercise 15 and increased physical activity has been found to be associated with worse pain scores in Parkinson’s. 17 Within the literature related to chronic musculoskeletal pain, avoidance of activity due to fear and reduced self-efficacy regarding managing symptoms can occur. 18 Keeping active may not seem plausible to patients with low perceived control over their pain 19 and has been identified as an issue with PwP and pain. 13 While exercise is also advocated for the management of pain in the general population20,21 this is often in conjunction with other strategies including education and support.22,23 Given that PwP in this survey highlighted exercise as a key strategy for reducing pain, future work to investigate pain management strategies specific to Parkinson’s is necessary.
Medication was also identified as a method currently used to manage pain. The most frequently cited medication was paracetamol (15% of individuals) followed by ibuprofen (11% of individuals), which follows a similar pattern to cross sectional studies, which have collected medication use data.2,12 This type of medication use has been criticized as not targeting the central mechanisms of pain in Parkinson’s. 2 Alongside this, these are not large numbers of the participants reporting medication use, and often individuals do not receive any support with pain management, including medication.7,8 Some participants in the current survey identified a hesitance at taking medication or suggesting a non-drug approach for future management. It is important to note that in an open question about expectations for a pain management intervention, medication was not suggested as a potential strategy by participants.
Healthcare professional support was valued by participants for pain management, appreciating the knowledge and advice healthcare professionals could provide being most frequently cited. A recent systematic review of pain management for PwP 6 advocates the need for further research in this area. The review demonstrated promise for pharmacological therapy focusing on Safinamide, and from 1 study, efficacy for multidisciplinary team (MDT) management. “Miscellaneous therapies” were highlighted including hydrotherapy, massage and resistance exercise, yet the quality of these studies was poor. Pain is multifactorial, 24 and individual approaches like those approaches did not reflect the biopsychosocial impact of pain. The review was comprehensive in its search, including allied health, behavioral therapy and client centered therapy, yet identified little in these areas. While MDT management had shown promise for pain 25 this was not the primary outcome or focus of this study and there was limited detail of the MDT management. A previous cross sectional survey found the greatest efficacy for pain management was reported in conjunction with treatment in a rehabilitation clinic or physiotherapy. 12 To date, there is limited literature focusing on interventions for pain management in Parkinson’s. 6 Pain management in the context of wider care, with support from healthcare professionals warrants investigation given PwP identifying the wide ranging impact of pain on their daily lives and a preference for support in pain management.
The participants in this study identified a number of different HCPs with whom they have discussed their pain with. In previous studies an orthopaedic doctor or general practitioner were the most frequently cited, with a small number citing neurologists. 12 In agreement, the current survey found a small number of neurologists and consultants cited. However, the Parkinson’s nurse and physiotherapist were frequently referred to as those who individuals had consulted. This finding is crucial as it indicates that there is a need for a multidisciplinary approach to pain management in Parkinson’s, in support of previous work. 25 HCPs working with individuals with chronic musculoskeletal pain have reported challenges in supporting people with pain and require support themselves. 26 Alongside this, literature exploring clinician attitudes and beliefs to chronic musculoskeletal pain has found HCP attitudes and beliefs to be associated with those of their patient. A biomedical orientation has a negative association with patient education, adherence to treatment guideline and activity recommendations. 27 These results of the current survey show that PwP feel HCPs have a key role to play in pain management. It is therefore important for future work to understand attitudes and beliefs among HCPs regarding pain in Parkinson’s, particularly given the limited focus on pain management in current Parkinson’s practice.7,8
70% of participants reported pain influenced their daily life, which aligns with other cross sectional studies focusing on pain and Parkinson’s, which report between 52% 28 and 85% 2 of people reporting pain. The current survey found 49% to experience pain daily and 24% multiple times per day. These findings are higher than previously reported of up to 21% “often” experiencing aches and pains and 6% “always” experiencing these. 29 Low back pain is frequently cited as problematic in Parkinson’s30,31 and was noted most frequently in this survey, followed by individuals experiencing pain at multiple sites. A diagnosis of the cause of pain was important to some individuals. However, given the central processes involved in pain, and PwP potentially being more predisposed to pain32,33 a definitive diagnosis may be difficult to achieve. A diagnosis can provide legitimacy to pain, and one potential way to achieve this is to consider education regarding pain physiology. 18 This captures the biopsychosocial nature of pain, supporting participants to understand the multifactorial influences on a pain experience. The participants focused predominantly on the location of pain within this survey. Given that there are often different pain mechanisms involved with pain and Parkinson’s 34 communicating these to PwP may help with understanding.
A limitation of this study is the lack of measures of disease severity including Hoen and Yahr staging, MDS UPDRS and measures of non-motor symptoms such as sleep and mood. This was a non-random sample, using self-report data, which is also acknowledged as a limitation of the study. Those responding are more likely to have had a problem with pain in view of the nature of the study. Alongside this, as individuals recruited would have expressed an interest to be contacted regarding research, the population may not be entirely representative of the Parkinson’s population as a whole. The relationship between pain, OFF periods and anti Parkinson medication was not specifically explored, however pain has been found to be no different between the ON and OFF state in the largest pain and Parkinson’s study to date. 2 We did not use a validated scale to capture information regarding pain in Parkinson’s, for example the Kings Parkinson’s pain scale. 35 However, the survey was able to address the aim of this exploratory study, to identify current pain management strategies and suggestions for the future. There were responses from 10 carers within this survey and it should be acknowledged they may have differing views to the PwP themselves, though there were not sufficient data to investigate this here. Respondents were all from the United Kingdom, which has implications for the availability of services.
The key strength of this study is that it has explored preferences and needs regarding pain management by directly asking PwP for their views. Feedback from a small group of PwP on the draft survey questions helped ensure that the survey focused on aspects important to PwP, and the use of open-ended questions allowed PwP to make suggestions about what pain intervention strategies should look like. Key HCPs who could be involved in pain management have also been identified, which will help when providing tailored support and guidance to healthcare professionals themselves. This study highlights the need to develop evidence surrounding how to manage pain in Parkinson’s, alongside the potential impact improved management would have on PwP quality of life, movement and wellbeing.
Supplemental Material
Supplemental Material, sj-pdf-1-jgp-10.1177_08919887211023592 - A Survey of People With Parkinson’s and Their Carers: The Management of Pain in Parkinson’s
Supplemental Material, sj-pdf-1-jgp-10.1177_08919887211023592 for A Survey of People With Parkinson’s and Their Carers: The Management of Pain in Parkinson’s by Jenni Naisby, Anneesa Amjad, Natasha Ratcliffe, Alison J. Yarnall, Lynn Rochester, Richard Walker and Katherine Baker in Journal of Geriatric Psychiatry and Neurology
Footnotes
Authors’ Note
Author Roles: Research project: A. Conception, B. Organization, C. Execution; Statistical/Qualitative Analysis: A. Design, B. Execution, C. Review and Critique; Manuscript Preparation: A. Writing of the first draft, B. Review and Critique;
JN: 1A, 1B, 1C, 2A, 2B, 2C, 3A, 3B
AA: 1A, 1B, 1C, 2A, 2B, 2C, 3B
NR: 1A, 1B, 1C, 2C, 3B
AJY: 1A, 2C, 3B
LR: 1A, 3B
RW: 1A, 3B
KB: 1A, 1B, 2B, 2C, 3B
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. JN was awarded a research involvement award from Parkinson’s UK who supported this work. Financial Disclosures for the previous 12 months: Richard Walker receives research funding from NIHR, MRC and The Dunhill Medical Trust. Lynn Rochester receives research funding from NIHR, MRC, EU, Stroke Association, GE Healthcare, Parkinson’s UK, Dunhill Medical Trust, Cure Parkinson’s Trust, New Zealand Health Research Council. Alison Yarnall has received funding from Parkinson’s UK, Dunhill Medical trust, EU IMI, NIHR, Michael J Fox Foundation and Weston Brain Institute for project grants. She has received honoraria / funding for educational events from Britannia, UCB, Abbvie, GSK, Teva-Lundbeck and Genus.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.