
Abstract
Background:
This paper describes barriers to engagement in the context of group activities attended by nursing home residents with dementia.
Objective:
The goal is to clarify the presence and types of barriers to group activities for persons with dementia.
Methods:
Therapeutic recreation staff (TRs) who conducted the group activities, and trained research observers (ROs) independently identified barriers occurring during group activity sessions through ratings and open-ended comments, which were analyzed via a mixed-method approach.
Results:
Barriers were related to specific participant, environmental, and group session characteristics. Most frequently noted barriers were participant-related, pertaining to apathy and challenging behavior. Noise was the most frequent environmental barrier. Overall, ROs reported more barriers than TRs, yet TRs reported the barrier of inappropriate topic more frequently than ROs.
Conclusions:
The study suggests that the number and specific types of barriers are associated with negative engagement outcomes. Insight into these barriers is the first step toward addressing them and minimizing their effects.
Introduction
Group activities can be effective in engaging individuals with dementia 1 and eliciting positive mood, 2 particularly when compared to unstructured time.3,4 However, the factors that facilitate or hinder engagement and mood in group activities are just beginning to be defined.
Research on engagement of persons with dementia (PwD) in group activities has largely been based on a framework similar to that used with individual activities. Both frameworks5,6 proffer that a participant’s engagement can be affected by characteristics of the person (e.g., demographics, cognitive and functional level), of the stimulus (e.g., activity content), and of the environment (e.g., ambient noise, time of day, group size, or group composition).
Noise and time of day have been identified as environmental factors affecting engagement and/or mood in nursing home residents with dementia. Specifically, high background noise was associated with significantly less engagement, and mood was more positive during afternoon compared to morning sessions. 7 The types of stimulus can also affect response to stimuli: exercise, music, and art resulted in higher levels of active participation compared to cognitive and functional household activities. 1 Well-being was higher for reminiscence therapy than for general group activities, such as crafts and games. 2 In one study, specific activities, including drama, wine/cheese social, gardening, and dancing produced engagement 98-99% of the time. 8 The same principle follows in group activities, i.e. different activities also affect different outcome variables. 3 For example, games and choral groups resulted in significantly more engagement, active participation, positive attitude, and positive mood, and in significantly less sleepiness than holiday discussion. 3 Exercise groups resulted in significantly more active participation, brain games in more positive mood, and baking in more positive mood and active participation thus affecting different outcomes. 3
With respect to personal characteristics, level of cognitive and functional impairment, speech impairment, number of medications, and liking group activities in general were highly correlated with engagement in group activities. These personal characteristics explained 46%–62% of the variance in the outcome measures. 9 Cognitive level, however, was the most consistent predictor of engagement, 9 and may have a greater impact on engagement than differences in group topic. 3
Barriers to activity implementation and effectiveness were commonly identified as insufficient time by staff and understaffing,10-12 and lack of skill and training among nursing staff.13,14 Effectiveness was enhanced by active engagement of staff and family and the ongoing provision of individualized interventions and support.15-17
In examining personalized interventions for behavioral symptoms, Cohen-Mansfield, Thein, Marx and Dakheel-Ali
18
provided a categorization of barriers: external barriers, which included those related to staff (e.g., general staff refusal/interruptions), family-related barriers (e.g., lack of availability or cooperation), environmental barriers (e.g., noise), and system process barriers (e.g., unavailability of materials for intervention); resident-related barriers including unwillingness to participate, and resident attribute barriers (e.g. cognitive level); and barriers related to resident unavailability (e.g., resident sleeping or eating).
Drawing on this categorization, we aim to investigate and categorize different types of barriers to group activities for PwD and to explore the specific impact of the barriers on the participants’ behavior and well-being. To further clarify this relationship, we assess how these barriers affect engagement and mood outcomes. We argue that a categorization of barriers and the clarification of their relationship to participants’ behavior and well-being can help plan for, address, and prevent barriers to group activities.
Methods
Design
This is an exploratory mixed methods study (i.e., combining both quantitative and qualitative data collection and analysis) to ascertain barriers to group activities as described by therapeutic recreation staff (TRs) and research observers (ROs), and to examine the relationship between the number and types of barriers and outcome variables. Two types of informants are used in order to critically examine and validate findings. While the presence of ROs might have an impact on TR behavior, the benefit of eliciting independent reports is seen as outweighing this potential limitation, particularly since TRs were aware that the role of the ROs was primarily to evaluate resident behavior.
Participants
This study was reviewed and approved by the Research Ethics Board of Baycrest Health Sciences. The sample included 69 older PwD recruited from 6 nursing home units. Informed written consent was obtained from participants’ substitute decision makers. Assent of participants was also required, so that the participants’ decisions not to participate were respected. The criterion for inclusion was a diagnosis of dementia (derived from the medical chart). Exclusion criteria were: 1) a diagnosis of bipolar disorder; 2) a lifelong diagnosis of schizophrenia; 3) Cognitive Performance Scale (CPS) Score 1 or below — scores of 0 or 1 indicate no, or borderline cognitive impairment, respectively 19 ; 4) no dexterity movement in either hand; 5) inability to be comfortably seated in a chair or wheelchair, or to be moved to the location of the group activity; and 6) absence of past or present competence in English. By design, we did not exclude participants on level of cognitive function, with the goal of studying the feasibility and outcomes of group activities for persons at all stages of dementia.
Assessment
Background information
Background information was gathered from the electronic health record system, Meditech, and also the Minimum Data Set (MDS) Version 2. This included age, gender, marital status, total number of medications, and total number of medical diagnoses. Cognitive functioning was assessed via the CPS, 19 with the scale of 0 = intact to 6 = severely impaired. Activities of daily living (ADL) performance was assessed via the ADL long form, 20 using a scale of 0 = independent to 28 = complete dependence.
Barriers
At the end of each group session, TRs and ROs independently indicated the presence (yes/no) of 5 barriers: lack of space, apathy of participants, challenging behavior of participants causing disruption, noise from outside, and inappropriateness of activity topic. Challenging behaviors are those which seem inappropriate to the occasion. Such behavior is often an expression of unmet needs that are difficult for caregivers to identify or address. 21 Additionally, raters were asked to elaborate on specific barriers (e.g., why the activity topic was inappropriate) and to provide written comments on any other barriers they identified. These comments were analyzed to clarify the cause of specific barriers and to identify additional barriers.
Engagement
Engagement outcomes were collected using the Group Observation Measurement of Engagement, GOME.
5
The construct of engagement was measured by 3 variables:
Procedure
Participants were invited to 2 sessions of each of 10 group activities. These activities, common in nursing homes and long-term care settings were: reading aloud with discussion, choral singing, baking, creative storytelling, brain games/fitness, active physical games (e.g., bowling or ring toss), exercise, reminiscence poetry, holiday newsletter, and holiday discussion. TRs conducted the group activities for PwD on their unit using pre-prepared materials. 22 One group activity was conducted per session, and each group activity was conducted twice, in random order, so that each unit completed a total of 20 group activities. Sessions lasted approximately 30 minutes. The study lasted approximately 3 to 4 months on each unit and 7 months overall.
Prior to the start of each session, TRs approached each study participant on their unit to describe the activity and to ask if the participant would like to attend. Those who agreed or did not, or otherwise indicated refusal were then escorted to the activity location either by TRs, ROs, or private aides. Participants who could not be asked for assent were informed about the activity and taken to it. Residents who indicated—verbally or nonverbally—that they did not wish to participate were not required to do so.
The assessments were completed by TRs, who were the regular TRs for the units, and by ROs, who were research staff or research volunteers with a degree in the social sciences and were trained for the assessment. At the end of each session, TRs who led the activity and a RO independently completed an assessment of the group, which included — in addition to information about barriers and engagement — attendance, time of day, location of the group, and other group characteristics.
Data Analysis
Barrier frequencies were determined separately for ROs and TRs and presented as means, as percent of sessions, and as percent of all barriers. Differences between raters were calculated using chi-square (for nominal level variables) and t-tests (for ordinal and interval level variables). In order to validate the information concerning barriers, we used Pearson correlations to examine relationships between number of different types of barriers and group and session characteristics (i.e., background noise level, group size, and group mean CPS and ADL). To understand the potential impact of barriers, Pearson correlations were calculated to examine the relationship between number of different types of barriers and outcome variables of engagement with the group activities.
Categories for different types of barriers resulted from a thematic analysis 23 of ROs and TRs’ responses. Following this method, the ROs and TRs’ open-ended comments were coded and recoded independently by research staff in multiple sessions. After discussing the codes and reaching agreement, we organized the codes into the themes presented below.
Given the likelihood that pre-identified barriers would be checked more often than those identified through analysis of open-ended responses, we differentiated between the 2 types of data.
Results
Participants
Of the 69 participants, 43 were female (62.3%), and age averaged 86.58 years (SD = 7.93, range 63–100). Most were widowed (42.0%) or married (42.0%). Participants had an average of 5.52 medical diagnoses (SD = 2.32, range 2–12). CPS averaged 4.19 (SD = 1.35, range 2–6); ADL performance averaged 20.52 (SD = 6.34, range 3–28).
Frequency of Reported Barriers
The correlation between number of barriers by the 2 types of raters was significant (r = 0.36, p < .0001). Overall, ROs reported more barriers than did TRs. ROs reported at least one barrier in over 3-quarters (76.7%) of the sessions; TRs reported barriers in just over half of the sessions (53.3%; Χ 2 (1) = 14.36, p = .0002). Similarly, average number of barriers per session for ROs (mean = 1.61, SD. = 1.29, range = 0–5) was significantly higher than that for TRs (mean = 0.98, SD = .16, range = 0–5; t(119) = 5.01, p < .0001).
Barrier Categories
Barriers could be divided into 3 categories: 1) Related to participants, 2) Related to the environment, 3) Related to group or activity characteristics. Barriers related to participants included apathy, challenging behavior, presence of non-verbal participants, and language difficulties. Environmental barriers included noise from the outside, lack of space, schedule conflict, and uncomfortable environment due to smells, heat, etc. Barriers attributed to characteristics of the group activity included inappropriate topic, size of group, either too small or too large, “difficult” group (see description below), issues with materials/resources, deviation from protocol, and sad memories raised by discussion. Table 1 presents frequencies for the different types of barriers identified by ROs and TRs, along with percentages, both per session and per total barriers.
Both TRs and ROs reported participant-related barriers most frequently — they formed 43.0% of all barriers reported by ROs and half (50.4%) of all barriers reported by TRs. Environment-related barriers constituted 37.3% of barriers for ROs and 23.9% for TRs; Barriers pertaining to group and activity issues were 19.7% for ROs and 25.6% for TRs. The mean number of barriers per session differed significantly between raters for participant-related (0.69 vs. 0.49, t(119) = 2.40, p = .0181) and environment-related (0.60 vs. 0.23, t(119) = 6.33, p < .0001) barriers, the number being lower for TRs in both cases. The number of environmental barriers also formed a significantly lower proportion of all barriers for TRs (23.9%) than for ROs (37.3%; Χ 2 (1) = 5.96, p = .0146). No significant differences occurred between raters for group/activity barriers.
Individual Barriers
Apathy, challenging behavior, and noise were the barriers identified most frequently by both raters, followed by lack of space and inappropriate topic (Table 1).
Barrier Frequencies as Noted by ROs and TRs.
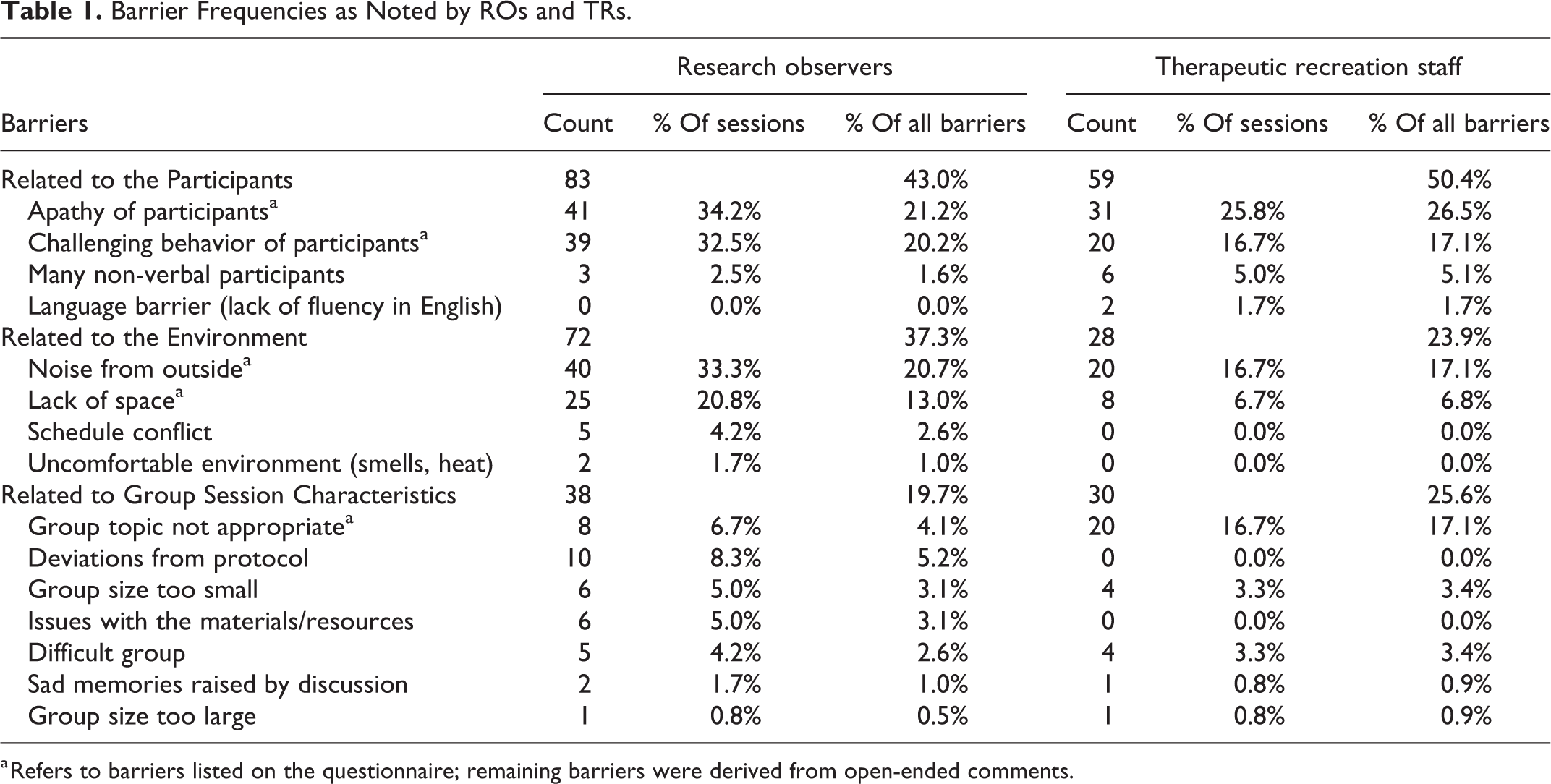
a Refers to barriers listed on the questionnaire; remaining barriers were derived from open-ended comments.
Participant-related barriers
The remaining participant-related barriers, derived from rater comments, involved verbal abilities of participants. Presence of
Environment-related barriers
Barriers related to group session characteristics
Comments of both ROs and TRs described
Both raters also noted
Only ROs reported
Relationship of Barriers With Engagement and Mood Outcomes
Number of barriers
The total number of barriers was significantly associated with the outcomes of decreased engagement and less positive mood in both RO and TR ratings (Table 2). The same trend was found for participant-based barriers and for group barriers, though the number of correlations that were significant varied between TRs and ROs for specific outcomes. The number of environmental barriers was not significantly related to outcome variables for either rater (Table 2).
Barrier Associations for Total Number of Barriers as Well as Number of Barriers in the Participant, Environment and Group Categories.
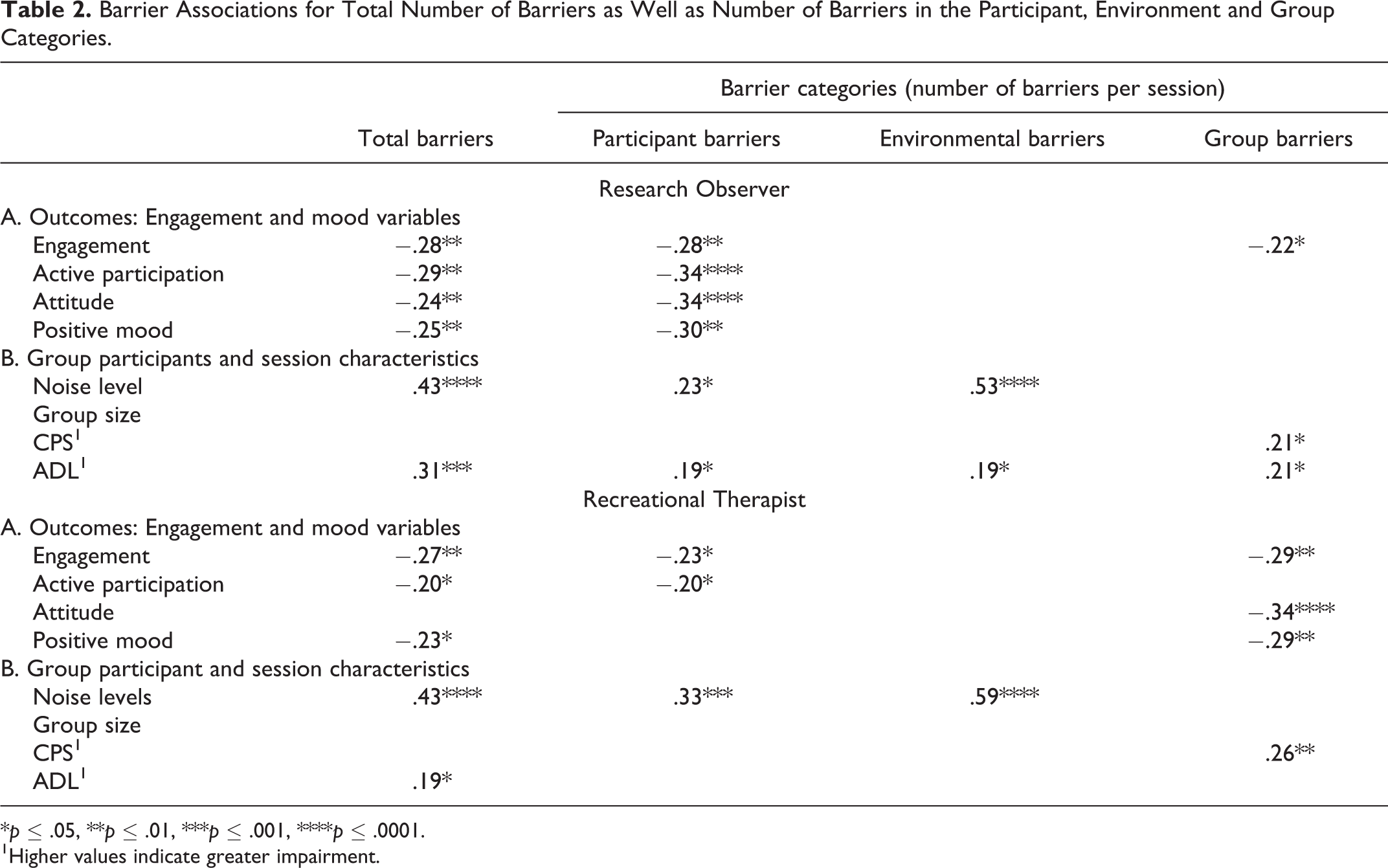
*p ≤ .05, **p ≤ .01, ***p ≤ .001, ****p ≤ .0001.
1Higher values indicate greater impairment.
Individual barriers
The designation of apathy as a barrier was significantly associated with outcome variables for both raters (ROs: active participation r = −.30, p < .001; attitude r = −.23, p < .05; positive mood r = −.22, p < .05; TRs: engagement r = −.20, p < .05; active participation r = −.20, p < .05).
Although behavior barriers occurred at a rate close to that of apathy, at least for ROs, such barriers had less of an effect on activity outcomes. RO ratings of behavior barriers were the only ones significantly correlated with a reduction in an outcome variable, that of engagement (r = −.18, p < .05).
Inappropriate topic as a barrier, noted by TRs, was significantly negatively associated with levels of engagement, attitude, and positive mood (r = −.24, p < .01; r = −.30, p < .001; r = −.25, p < .01, respectively). Inappropriate topic as rated by ROs was not associated with the outcome variables.
Noise and space barriers were not significantly associated with any outcome measure.
Relationship of Barriers With Group Activity and Participant Characteristics
Total number of barriers, participant barriers, and environmental barriers increased significantly with level of background noise for both raters (Table 2). Not surprisingly, for both raters, background noise level was higher when a noise barrier was indicated, but behavior barriers were also associated with background noise.
Group size was not significantly associated with any barriers in TR data. However, for RO data, as group size increased, space barriers were more frequently noted (r = .37, p < .001).
Functional impairment correlated with both total barriers and almost all types of barrier categories for ROs, with some similar correlations also manifested in TR data and some in relationship with cognitive impairment (Table 2). TR designation of inappropriate topic as a barrier was significantly correlated to participants’ cognitive impairment (CPS) (r = .24, p < .05). The barrier of apathy was related to ADL impairment (TR: r = .23, p < .05) as was the barrier of behavior (RO: r = .26, p < .01).
Discussion
As with individual activities, barriers are prevalent in group activity sessions for PwD. At least one barrier was reported in half (TRs) to 3-quarters (ROs) of the group sessions, pointing to the importance of monitoring barriers as an important tool for improving group activities for PwD. We classified barriers as those related to participants, to the environment, and to group and activity characteristics, finding participant-related barriers to be the most frequent, with apathy being the most frequently reported individual barrier by both raters. Barriers, both collectively and individually, were related to engagement and mood in participants.
The results show that the 2 types of informants, TRs and ROs, while differing in their perceptions and biases, provided results that converged in terms of the main research questions: what are the barriers to group activities? And, what is the impact of such barriers?
From the comments, it appears that barriers may have had little direct effect on the conduct of the groups and, in most cases, groups continued as planned. There is only one mention of negative reaction on part of TRs (to challenging behavior), and only one mention of a group being cut short or terminated (due to apathy), even though a number of groups were characterized as difficult. Yet, the data show that barriers may affect, or be reflected in group outcomes, as mean engagement and mood levels for the groups significantly decreased with increases in the number of barriers. Nevertheless, although barriers may decrease activity engagement outcomes, they do not eliminate them altogether. We have shown in other work that engagement and mood levels during group activities are higher than engagement observed during a control no-group-activity condition. 3
Apathy, challenging behavior, and inappropriate topic were the individual barriers that were most often significantly correlated with engagement in group activities. Apathy is the principal barrier in this regard, as significant effects were seen in the data from both raters, both of whom reported it more frequently than other barriers. Countering apathy and its effect on older adults is one of the leading reasons for presenting group activities. Engagement in activities can reduce symptoms of apathy,24,25 and without such participation, an increase in apathy 26 or further cognitive deterioration 25 may occur. Yet, residents who displayed apathetic behaviors, such as being asleep, or residents who were nonverbal, were, at times, left out of the group activity, neither given activity materials, nor approached by the TRs. Such residents were described as difficult to engage, and sessions with apathetic participants were often considered difficult groups. It may be that TRs are insufficiently exposed to such persons in a group activity environment, as staff-led activities tend to be geared to higher functioning individuals who are alert and oriented and therefore deemed most likely to benefit. 27 Nevertheless, just being in a group situation, even without active participation, can be of benefit by satisfying needs for belonging and social connectedness.28,29 TRs may benefit from additional training on how to encourage engagement with strategies aimed at helping PwD feel valued and part of the group. When planning and leading group activities, TRs should anticipate a certain degree of apathy, recognizing it as one of the manifestations of cognitive decline, rather than as a barrier, and regarding it as a condition that can be somewhat alleviated by group activity.
Although ROs noted barriers due to challenging behavior at a rate equal to that of apathy, TRs were less likely to report a behavior barrier under conditions where an observer felt one was present. Generally, TRs seem better able to deal with challenging behavior than with apathy. When challenging behaviors did occur, they were mostly overcome by TRs, and TRs may not have felt it necessary to report a barrier in these cases. This may be due to their experience with such challenges, their acceptance of behavior issues as part of the norm in this population, or their sense of efficacy in handling such behaviors. In only a very few instances did participants need to be removed for challenging behavior. 30 The effect of behavior barriers on engagement was limited and seen only in RO data.
Inappropriate topic is the one barrier that TRs reported with greater frequency than observers, and it is the barrier with the greatest impact on engagement according to TR data. According to their narrative explanations, TRs were most likely to designate a topic as inappropriate when it was perceived as beyond the capabilities of the participants, or when there was apathetic behavior. Such barriers appear to be a function of the cognitive abilities of group participants, as mean cognitive levels of the group were significantly lower for topics considered inappropriate. Cognitive impairment itself explains some of the effects on engagement, as cognitive function is the most potent factor affecting the engagement response to group activities. 3 And, indeed, 2 of the 3 significant associations with inappropriate topic were no longer significant when controlling for cognitive function. The presence of these barriers requires TRs to be flexible and prepared to select activities and/or modify materials to match the needs and abilities of participants. This tailoring is especially crucial when persons with advanced dementia attend group activities.31,32 PwD prefer activities that do not reveal their weaknesses, but rather allow them to participate equally with others in the group. 28
Some of the common nursing home activities presented here were considered inappropriate more frequently than others, and some were better than others in fostering engagement in participants. 3 For example, TRs labeled storytelling inappropriate 40% of the time, and storytelling resulted in significantly lower levels of engagement, active participation, and positive attitude compared to a reference activity of holiday discussion. In contrast, choral singing was not considered inappropriate by TRs in any session, and choral singing was associated with significantly higher levels of engagement. 3 This type of information provides useful guidance in the selection and presentation of group activities. However, existing data should be considered preliminary. More work is needed on characterizing the appropriateness and potential for success of various activities across different stages of dementia, and on how to structure groups in order to include persons at all functional levels.
The 2 environmental barriers of noise and lack of space were noticed primarily by ROs, but neither barrier correlated with engagement outcomes. Although high background noise has been associated with lower engagement during group activities, 7 noise as a barrier did not have similar effects. Comments suggest that, in addition to background noise, designation of noise as a barrier may include noise from the group itself.
Lack of space was related to group size in RO data, and was more likely to be noted as a barrier when groups were larger and the space was insufficient for the number attending the group. Space could be a problem in the sitting areas on the units where furniture did not leave sufficient room for wheelchairs. However, as with group size, 7 space barriers had no effect on engagement.
By design we opted not to exclude potential participants based on level of cognitive function as we aimed to examine the feasibility of group activities for persons at all stages of dementia. This, in conjunction with personal invitations by TRs, escort to the activity location, and a relationship between cognitive level and refusal to attend, 30 appears to have contributed to relatively high attendance at the sessions of persons with more advanced dementia. In fact, 52% of the sample could be classified as having at least moderately severe cognitive impairment (i.e., CPS scores of 4, 5, or 6), with 29% being very severely impaired. Thus, the sample is unique in its large percentage of persons with advanced dementia. Since such persons are least likely to attend staff-led activities,31-33 they may not be representative of residents who choose to attend group activities on their own. Yet, as seen in our sample, it is possible to get them to attend group activities under supportive conditions. Such highly-impaired persons do benefit from involvement in activities, albeit at a lower level than those less severely impaired.3,24 The mere participation in an activity may be more important than the type of activity.3,34 Keeping these individuals involved is especially important 32 to help maintain existing abilities and to prevent or slow further decline.
Despite predominant agreement on ratings of outcomes, the 2 types of raters provided some differing perspectives on barriers, both in number and type of barriers reported and in criteria underlying reports. One of the reasons for the differences might be that the primary task of ROs was specifically to observe and note what occurred during the sessions. This mission would have encouraged a greater frequency of reports. Features that can readily be seen, such as functional impairment, appeared to influence RO reports. ROs, unfamiliar with the environment, also reported more barriers for noise and space, features to which TRs were likely to be habituated as normal conditions of work. Given their experience in conducting activities, TRs may not have noticed certain barriers or might have overcome those that occurred, not reporting them unless they substantially impacted the sessions. Demand characteristics also could have limited TRs barrier reports, as reports of more barriers might be considered negative reflections on their work.
Conclusion
This paper provides information on the barriers associated with group activities common in nursing homes from the perspective of outside ROs and TRs. More research is needed to determine factors that facilitate or inhibit activity participation and outcomes among nursing home residents, particularly those in the later stages of dementia. Relevant studies have often been limited to those with mild to moderate dementia. The current work on barriers provides initial information on impediments to the success of group activities for persons with more severe dementia, and points the way to what may need to be improved, architecturally, programmatically, or in terms of staff training. Awareness of what the barriers are, and understanding the factors which contribute to them are the first steps in trying to address and minimize their effects in long-term care settings.
Footnotes
Acknowledgments
Sadly, co-author Barbara Jensen has passed away. She was a scholar of great wisdom, resourcefulness and generosity. I will miss our collegial relations and our long-time friendship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Rotman Family, the Morris Justein Visiting Scholars Program, and the Minerva Foundation, Grant 3158329500.