
Abstract
Background:
Awareness of the diagnosis or related changes in functioning varies in people with dementia (PwD), with implications for the well-being of PwD and their carers. Measuring awareness in a clinical setting could facilitate tailored support and optimize involvement in personal health and care decisions. This scoping review aimed to identify validated methods of assessing awareness in dementia and appraise their clinical utility.
Method:
A systematic search was conducted of English-language publications that measured awareness in PwD, in 6 electronic databases. Search terms included dement*, Alzheimer*, Pick disease, and awareness, unawareness, anosognosia, insight, denial, metacognit*, or discrepanc*.
Results:
We screened 30,634 articles, finding 345 articles that met our inclusion criteria. We identified 76 measures, most commonly using a discrepancy questionnaire comparing evaluations of function by PwD and an informant. There were 30 awareness measures developed and validated for use in dementia populations but few designed for general clinical use.
Conclusions:
Although we found a range of clinical indications for measuring awareness, there were few studies investigating clinical applications and few tools designed for clinical purposes. Further investigation and development of a person-centered tool could facilitate health and care choices in mild-to-moderate dementia.
Introduction
Background
A diagnosis of dementia, or major neurocognitive disorder, requires evidence of functional impairment alongside cognitive decline. 1,2 People with dementia (PwD) vary in their awareness of the diagnosis 3 or of their decline in cognitive and functional abilities. 4 -7 The frequency of impaired awareness is difficult to affirm as it depends on how and in whom it is measured, 4,5 and estimates range from 20% to 81%. A study using a multidimensional assessment in people with mild-to-moderate dementia found 14% had greater awareness and 41% had limited awareness, with the remainder classed as moderately aware. 8 This has consequences for the well-being of PwD, with reduced awareness shown to predict risk of unsafe behavior, hospital admission, and institutionalization, 9,10 and has implications for care provision and planning. For family members or close friends who provide unpaid support (for convenience, we will refer to these as “carers”), lack of awareness of difficulties with functioning on the part of PwD is associated with increased stress 8,11,12 and poorer perceived relationship quality. 13 This in turn may indirectly reduce the quality of life for PwD 14 and could contribute to a breakdown of home-care arrangements. A small proportion of PwD retain high levels of awareness of their condition, and this can be associated with dysthymia and anxiety 15 and may infer a need for increased support around the time of diagnosis. 16 Furthermore, some PwD underestimate their abilities particularly in the area of socioemotional functioning. 17 This might reflect the more complicated appraisal needed by PwD or informants to rate socioemotional behavior, which may be more influenced by personal values or beliefs. Alternatively, it may represent an awareness of changes, and perhaps in the context of the stigma associated with dementia, result in an overly pessimistic view of abilities. This could lead to unnecessary avoidance of beneficial activities.
Measuring awareness effectively in a clinical setting could help to build a more accurate picture of an individual’s experience, resulting in personalized care and activity planning. Benefits could include improved communication, for example, by establishing whether the individual is aware of the diagnosis of dementia as a starting point, and enhanced involvement in decisions around personal health care or self-management. Higher awareness may mean that an individual is able to make use of adaptive strategies such as memory aids to continue living at home independently and managing own medication, and awareness measurement could be useful in assessing outcomes of rehabilitative interventions. Awareness has been shown to be an important independent factor influencing capacity to make decisions particularly in the mild-to-moderate stages of dementia, where people with lower awareness are less likely to be judged to have capacity, for example, in decisions around medication, 18 -20 or when addressing legal matters such as wills and advance directives. 21 Understanding an individual’s awareness profile could also be helpful for discussions around health and care needs on occasions when a person with dementia attends the clinic unaccompanied.
Nevertheless, awareness is a complex phenomenon, as demonstrated by the range of models developed to explore the related concepts. 22 -25 Different approaches have been taken to measure awareness, using different terminology to reflect the slightly different concepts. Terms include “anosognosia,” used initially to describe lack of awareness of a specific neurological deficit 26 but applied since then to loss of awareness in dementia 5,27 ; “insight,” originally from psychiatry regarding awareness of a condition or symptoms 28 ; “denial,” referring to largely psychodynamic factors that affect expression of awareness 29 ; and “metacognition,” describing self-awareness of cognitive ability. 24 Awareness can be considered to operate at different “levels,” ranging from simple sensory registration, to online monitoring of performance, evaluating specific situations, and the higher level of meta-representation of one’s situation and the impact on others. 25,30 It can also be implied indirectly through observations of behavior if not explicitly stated. 31,32
Awareness should be understood as having an “object,” for example, awareness of specific cognitive deficits such as memory problems or awareness of changes in behavior such as social functioning. Since the degree of loss of awareness can vary in any individual between objects, it is helpful to specify the object that is being considered either clinically or in research. 17,33 For clinical applications, the object studied would determine the usefulness of an assessment. While awareness of cognitive deficits such as memory impairment is commonly studied, awareness of difficulties with activities of daily living (ADLs) may be more directly relevant to determine where help is needed, although there is an overlap between cognitive difficulties and the ability to carry out everyday tasks. 34,35 Additionally, considering the individual objects of awareness helps to clarify the correlates and potential consequences. For example, impaired awareness of dangerous behavior has been associated with hospital admission and residential care placement 9 and physical health awareness has implications for managing other health problems. Impaired functional awareness has been associated with developing frailty 36 and measurement of awareness could contribute to frailty assessment.
Building on a model of the cognitive processes behind awareness, 37,38 a wider approach incorporates psychosocial factors, as well as the concepts of levels and objects of awareness, 22 and has helped to explain the heterogeneity of results from earlier studies where these issues were not specified, 17,39 Other studies have clarified the influence of cultural factors on expressed awareness 4 and the importance of social opportunities to demonstrate awareness. 30,40,41 A comprehensive biopsychosocial model assists understanding by describing awareness as a sequence of registering and reacting to change, where responses are influenced by the social environment, individual features of past history, personality and coping styles, as well as the degree of neurocognitive impairment. 6,22 From this model, the term “awareness” is defined here as “the ability to hold a reasonable or realistic perception or appraisal of, and/or respond accordingly to, a given aspect of one’s environment, situation, functioning, or performance.” 30 ,p20 This broad definition permits consideration of awareness, either retained or reduced, across different objects and levels, and either explicitly or implicitly demonstrated.
Methods of measuring awareness include ratings or judgments from clinician interviews, or use of questionnaires that compare the self-evaluation of ability by PwD with an informant evaluation, using the discrepancy between them as an index of awareness. A further method utilizes the discrepancy between self-ratings by PwD and their performance on an objective task. There are also activity-based qualitative and observational methods described in the research literature. 42 There are known limitations to each type of method, which may be nonspecific or restricted in terms of the object and level of awareness assessed, or at risk of bias from use of subjective ratings. 43 The majority of methods have been developed for research purposes, rather than as clinical tools for assessing awareness in everyday living, perhaps because in clinical practice, awareness tends to be appraised informally or nonspecifically.
Objectives
We wanted to explore the availability of methods that could be used to measure awareness in a clinical setting. Expectations for an ideal clinical tool might include the following features: it should assess objects of awareness that are relevant to everyday situations; it should be brief and simple enough to administer in clinic with basic staff training, to encourage widespread use; and it should be developed with, and validated for, PwD to ensure relevance and acceptability. To investigate and compare the available methods, we planned a review showing the approaches taken across different settings and with people at different stages of dementia and with different dementia diagnoses. Previous reviews date from 2005 or earlier, 42,43 or cover different patient populations 44 and to our knowledge there are no recent English-language systematic or scoping reviews of these methods, relating specifically to dementia. We, therefore, describe a scoping review, which aimed to provide a comprehensive overview of the available methods of measuring awareness in PwD. This enables identification of validated measures and further appraisal of the components for potential clinical use. We chose a scoping methodology as it combines rigor with flexibility and allows inclusion of quantitative and qualitative studies, as well as case studies, because we wanted to demonstrate current clinical and research practice for assessing awareness.
Methods
Study Design
This scoping review focused on the question: “What methods and measures are used to assess awareness in PwD, and what are the characteristics and utility of each method?” The review is based on the Arksey and O’Malley framework 45 with additional guidance from later publications. 46,47 This involves a systematic search of a broad range of literature leading to an overview or map of the relevant research with a descriptive analysis. 48 Our previously published protocol 49 used guidance from Preferred Reporting Items for Systematic Reviews and Meta-analysis-Protocol (PRISMA-P); 50,51 and this report follows the PRISMA extension for scoping review guidelines. 52
Search Strategy
A search was made on February 4, 2019, of the electronic bibliographic databases PubMed, Embase, PsycInfo, Cumulative Index to Nursing and Allied Health Literature complete, Web of Science Core collection, and Cochrane Library for relevant peer-reviewed, published literature. Search terms used were (dement* OR Alzheimer* OR “Pick’s disease”) AND (aware* OR unaware* OR anosognosia OR insight OR denial OR metacognit* OR discrepanc*), with unlimited date range and no language restriction (see protocol for electronic search strategy). Duplicate records were removed. Titles and abstracts were screened by 2 independent researchers for removal of inappropriate articles, with 98% agreement. Full texts of the remaining articles were examined according to eligibility criteria, as outlined below and detailed in our published protocol, 49 to produce a list of included articles. A second researcher screened a 10% sample of the full-text articles for selection, reaching 92% agreement. Differences were discussed and resolved by consultation with a third senior researcher. Members of the review team were not involved in decisions about the inclusion of those studies which they had authored.
Study Selection
Population
We included studies that measured awareness (or equivalent term) in people with a clinical diagnosis of dementia of any type and all degrees of severity. Settings were not restricted and included community, outpatient, inpatient, and residential settings. There were no limitations of age, gender, or ethnicity. Studies with mixed populations were included if 50% or more of the participants had a clinical diagnosis of dementia and these data were separately identifiable.
Concepts
We included studies that measured awareness in PwD using either standardized tools or new methods devised for a specific study, where awareness was measured as a global construct or in relation to specific objects or domains such as awareness of memory function, socioemotional functioning, or everyday functional ability.
Context
Selected studies were English-language publications, where full text was available. We included quantitative, mixed method and qualitative studies, and case studies to scope a broad range of awareness research.
Exclusion criteria
We excluded studies that primarily studied mild cognitive impairment or non-dementia diagnoses, along with non-original or non-peer-reviewed material or where data from dementia participants were not separately identifiable. Studies that did not measure the awareness construct were excluded. Exclusion decisions and characteristics of excluded studies were recorded according to PRISMA guidelines.
Data Extraction and Mapping Results
For each included study, standard information was recorded and charted according to key characteristics. A second reviewer checked data extraction for the first 20 articles, and discussions enabled refinement of the data extraction process. Data items included name of study or grant number, study design, geographical region of study derived from country (assumed from author affiliation if otherwise unclear), setting, sample size, type and severity of dementia based on mean Mini-Mental State Examination, 53 Clinical Dementia Rating 54 or verbal report where available, age and gender of participants, the type of informant, the specific measures, and the type of method used. The object of awareness was recorded where stated, or otherwise inferred from the methodology reported. Method of data analysis was included for qualitative studies. Details of specific measures included how the awareness rating was made, the scoring and number of items where relevant, and whether the measure was intended for clinical use. Validation data were reported if there was evidence of any evaluation of validity, reliability, or internal consistency.
Collating, Summarizing, and Reporting Results
The results have been tabulated to demonstrate the full scope of included articles, to identify the key named and validated measures, and to appraise the characteristics and clinical utility of these measures. The range of methods used and the objects studied have been mapped diagrammatically. We shared the findings with expert clinicians, consulting in particular regarding the clinical implications. Results will be reported regarding the included articles and the types of methods and objects assessed, followed by the specific measures identified.
Results
Search Findings
Exclusion decisions are documented in the PRISMA flow diagram (see Figure 1). Of the 30,634 records identified in the search, 345 articles were included in the review: 325 quantitative articles including 4 case studies, and 20 qualitative articles. There were 39 articles reporting longitudinal studies. The influence of awareness on the outcome of or responses to interventions was investigated in 7 quantitative and 4 qualitative studies. The majority of research was conducted in Europe or North America. Details of quantitative articles and case studies are recorded in Supplementary Table 1a and b, respectively. Qualitative studies are summarized in Supplementary Table 2. Articles excluded at full-text screening, with exclusion reasons, are listed in Supplementary Table 3.
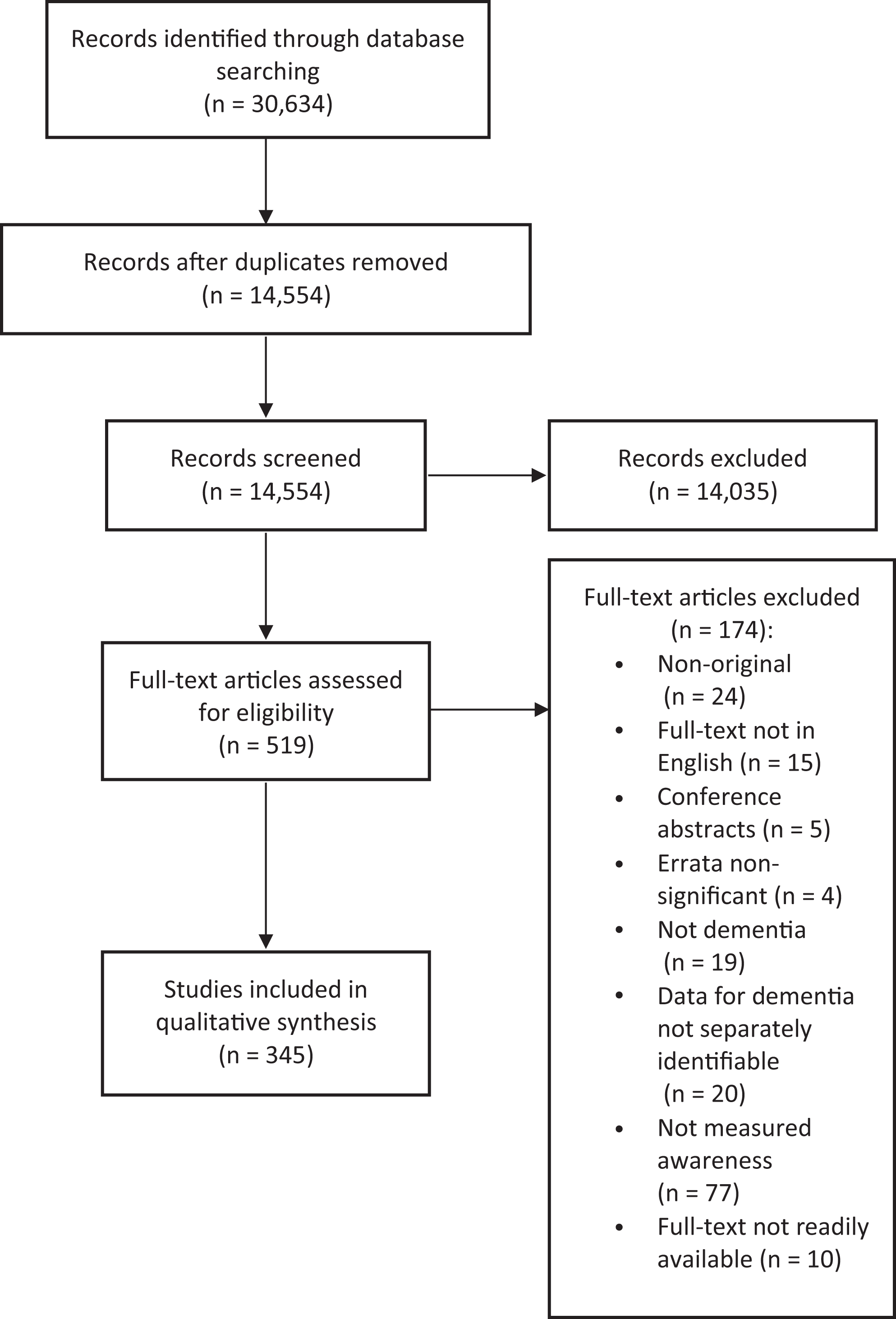
Preferred Reporting Items for Systematic Reviews and Meta-analysis-Protocol flow diagram.
Demographic Characteristics of Participants
Most of the participants were community dwelling and recruited from outpatient clinics or memory clinics. The majority of the articles studied people with mild-to-moderate dementia, and the most frequent diagnosis was Alzheimer disease (AD). For further details, see Table 1.
Demographic Characteristics of Participants in the Included Studies.
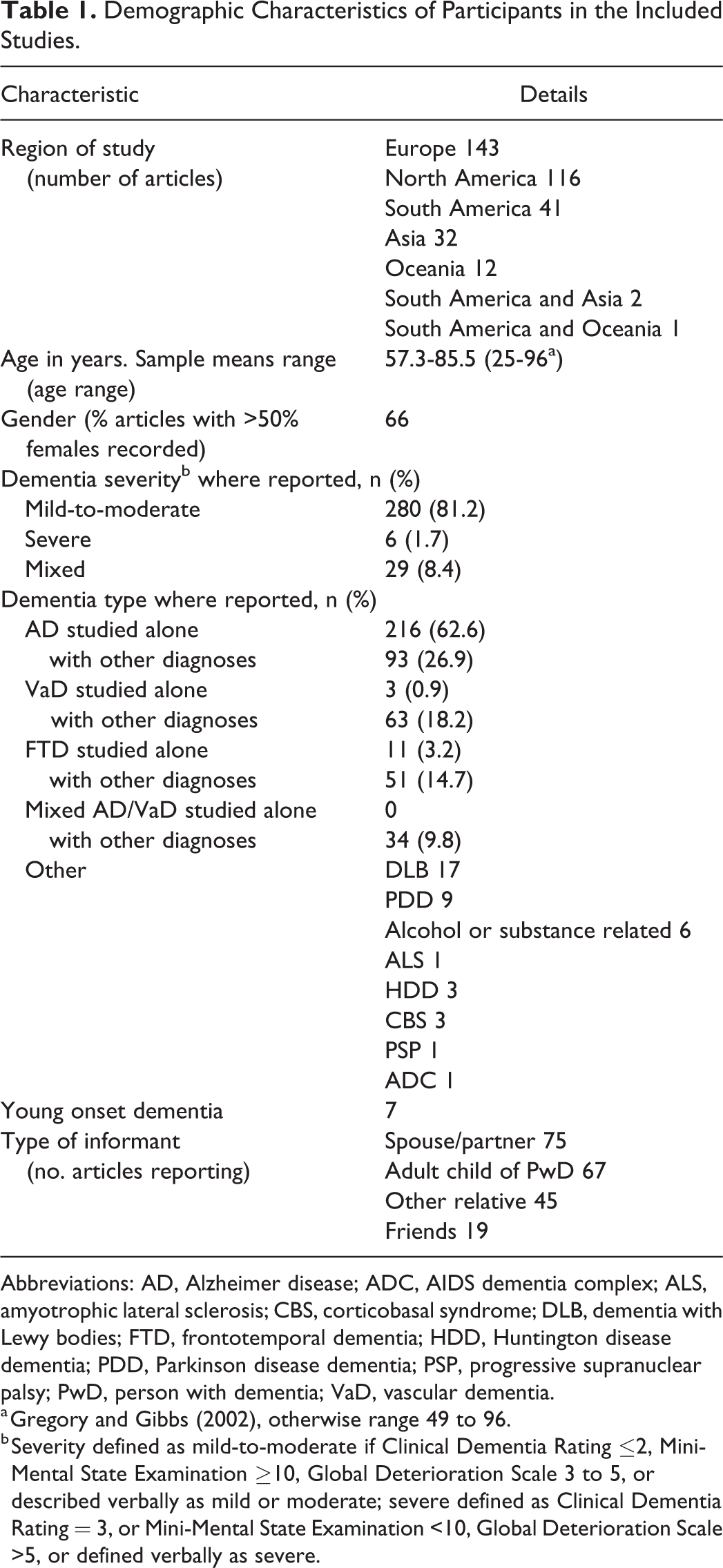
Abbreviations: AD, Alzheimer disease; ADC, AIDS dementia complex; ALS, amyotrophic lateral sclerosis; CBS, corticobasal syndrome; DLB, dementia with Lewy bodies; FTD, frontotemporal dementia; HDD, Huntington disease dementia; PDD, Parkinson disease dementia; PSP, progressive supranuclear palsy; PwD, person with dementia; VaD, vascular dementia.
a Gregory and Gibbs (2002), otherwise range 49 to 96.
b Severity defined as mild-to-moderate if Clinical Dementia Rating ≤2, Mini-Mental State Examination ≥10, Global Deterioration Scale 3 to 5, or described verbally as mild or moderate; severe defined as Clinical Dementia Rating = 3, or Mini-Mental State Examination <10, Global Deterioration Scale >5, or defined verbally as severe.
Methods Shown in Articles
Quantitative Articles (Including Case Studies)
We found 325 articles that investigated awareness quantitatively, 4 of which were case studies. Broadly categorized, the quantitative methods comprise questionnaires eliciting discrepancies between self- and informant ratings (used in 55% of articles), discrepancies between self-ratings and objective measurement of performance (24%), and ratings by a clinician or researcher based on an interview (37%). This latter category includes in-depth unstructured interviews as well as brief clinical ratings based on responses to a single question or a few questions. Informants were usually informal carers, typically a female relative. Other variations of these methods were used in 47 articles; see Figure 2 for details. Mixed methods were used in 8 of these studies and the qualitative methods employed are recorded in Figure 2.
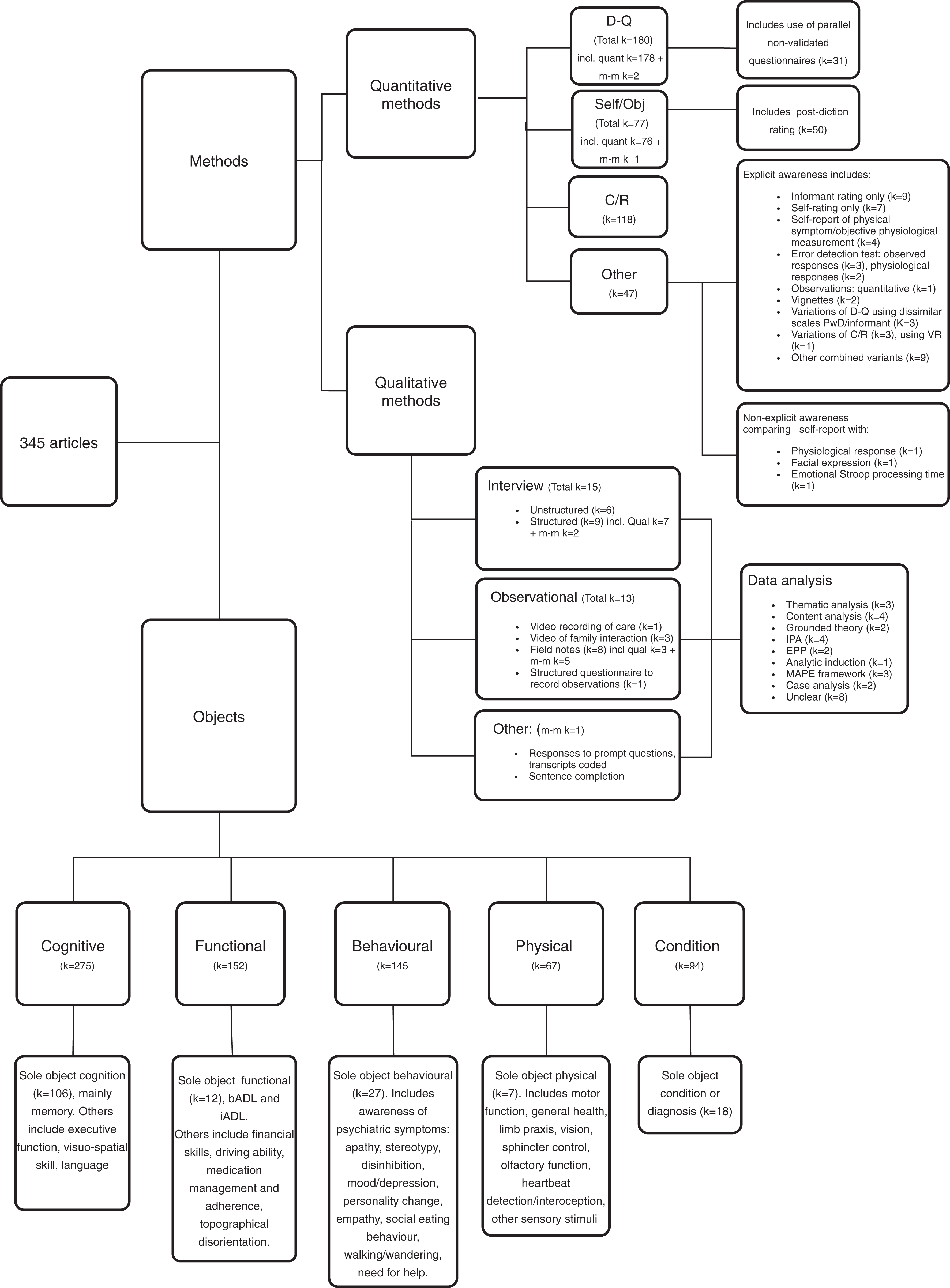
Map of methods and objects. bADL indicates basic activities of daily living; C/R, clinician rating; D-Q, discrepancy questionnaire; EPP, empirical phenomenological psychological; iADL, instrumental activities of daily living; IPA, interpretative phenomenological analysis; k, number of articles; MAPE, markers of assimilation of problematic experiences; m-m, mixed-methods article; PwD, person with dementia; self/obj, self-rating/objective performance; VR virtual reality.
The discrepancy questionnaires included non-validated methods where a questionnaire validated to assess ability of PwD was supplemented by a parallel version of the questionnaire for an informant, creating a discrepancy score as an indication of awareness (see Figure 2). The most frequently utilized measure for this purpose was the Physical Self-Maintenance Scale/Instrumental Activities of Daily Living scale 55 used in 9 articles to study awareness of ADL. Some studies used self-rating scales of cognitive function, for example, Everyday Memory Questionnaire 56 used in 6 articles, or Cognitive Difficulties Scale 57 in 6 articles, which alone are subjective measures of cognitive complaint; however in these articles, they were used to produce a discrepancy with informant ratings or with objective performance as an indicator of awareness. Additional nonstandardized approaches are seen in 59 articles measuring objective performance compared to self-ratings, including experimental metamemory methods. Eighty-five articles employed more than one measure, with some using up to 6 measures (3 articles); see Figure 2 for more details.
Qualitative Articles
We found 20 articles that investigated awareness qualitatively. The most common qualitative method of assessing awareness was by interview (65% of qualitative articles) with varying degrees of structure, mostly involving analysis of an audio transcript. Observational techniques were used in 8 (40%) articles. Group session transcripts were analyzed in 2 articles, and family carers were involved in 8 articles either with a separately recorded interview or video-recordings of family interactions. Three articles used more than 1 qualitative method to gather data and 3 used an additional quantitative method. A range of methods was used to analyze the data; see Figure 2 for further detail.
Objects of Awareness
The most commonly examined object was cognition (in 80% of articles), typically memory function. Functional ability was assessed in 44% of articles, that is, basic and/or instrumental ADL. Behavioral domains were assessed in 42% of articles with most looking at general awareness of social and emotional functioning; some were more specific to awareness of a psychiatric symptom. Other main objects were awareness of physical symptoms (19%) and awareness of the diagnosis of dementia (27%). Nearly half of the articles (170 of 345) focused on a single object of awareness; see Figure 2 for more details.
Identified Measures
There were 76 named or standardized measures (see Supplementary Table 4a-d for full names and abbreviations used, and references), of which 30 presented some form of validation data (see Supplementary Table 4a). Some measures were developed for PwD but lack reported validation data (see Supplementary Table 4b). Other well-established measures were developed in populations other than dementia, though 3 of these have subsequently been validated for dementia (see Supplementary Table 4c). We also found single-item measures used to assess awareness, taken from clinically developed assessment tools (see Supplementary Table 4d). Some of these “insight items” were taken from scales designed for a broader assessment of dementia (n = 6), from scales for assessing mental illness (n = 4), or from dementia diagnostic scales (n = 2). While they were treated as single items in an overall scale, some of these items required responses to more than one question or information from more than 1 source to form the score of the item. In total, 206 articles used at least 1 standardized measure, and 160 of these used a validated measure developed for dementia.
Validated Measures Designed to Measure Awareness in PwD
We further investigated the 30 measures that reported validation data (see Supplementary Table 5a-d). Of the validated measures, the most common method was the discrepancy questionnaire (see Supplementary Table 5a), with the most frequently employed being the Anosognosia Questionnaire-Dementia (AQ-D). Clinician interview ratings were the next most common type (see Supplementary Table 5b), with the Reed rating the most frequently used. Methods which combine self-evaluation with informant rating and objective task performance formed just 3 measures (see Supplementary Table 5c), of these the most frequently used was the Memory Awareness Rating Scale (MARS). Nine measures used other variations on these methods (see Supplementary Table 5d). Mixed objects of awareness were assessed by most of these measures, followed by memory only, while 2 tools looked at very specific functional objects (see section 3.7 below for more detail). There was no apparent pattern in choice of measure according to the type of dementia. No gold standard was evident. The validated tools used in the intervention studies were MARS, Clinical Insight Rating Scale (CIRS), Self-Consciousness Questionnaire (SC-Q), and Reed. The only validated tool used among the 4 case studies was the Assessment Scale of Psychosocial Impact of the Diagnosis of Dementia (ASPIDD).
Clinical Utility of Validated Measures
Regarding brevity, the questionnaires employed to produce a discrepancy rating varied considerably in number of items and estimated time to complete (see Supplementary Table 5a). The clinician rating measures generally had fewer items, typically with 3 or 4 opening questions, though the duration of interview required is unclear (see Supplementary Table 5b). The combined methods with both questionnaire items and objective tasks were characteristically longer (see Supplementary Table 5c). For scoring, one measure used a categorical rating, and 29 used a scale, of which 4 employed cutoff scores to dichotomize awareness. In terms of accessibility, questionnaire measures placed different requirements on participants; the majority asked PwD to rate abilities or problems on a Likert-style scale or by frequency of occurrence (n = 13), or to endorse items or symptoms with yes/no responses (n = 6). Some rate function compared to an average person or as a self-comparison over the past 3/5/10 years.
Six of the validated measures were designed to be used in clinical settings (see Table 2). These include 2 measures designed with a specific purpose: assessing awareness of financial skills (Measure of Awareness of Financial Skills [MAFS]) or assessing awareness of navigational ability (Questionnaire for Everyday Navigational Ability [QuENA]). Only 1 measure was specifically designed for use in severe dementia to support provision of person-centered care (AwareCare). One well-established multidomain research measure (AQ-D) has been abridged as a 9-item clinical tool (Abridged Anosognosia Questionnaire [AAQ]). Another was designed as a more detailed tool with predictive capability for risk assessment and care planning (Structured Interview for Insight and Judgment in Dementia [SIJID]). One measure can be used with dual purpose for dementia diagnosis and assessment of awareness (Symptoms of Early Dementia-11 Questionnaire [SED-11Q]).
Validated Tools With Potential Clinical Use.
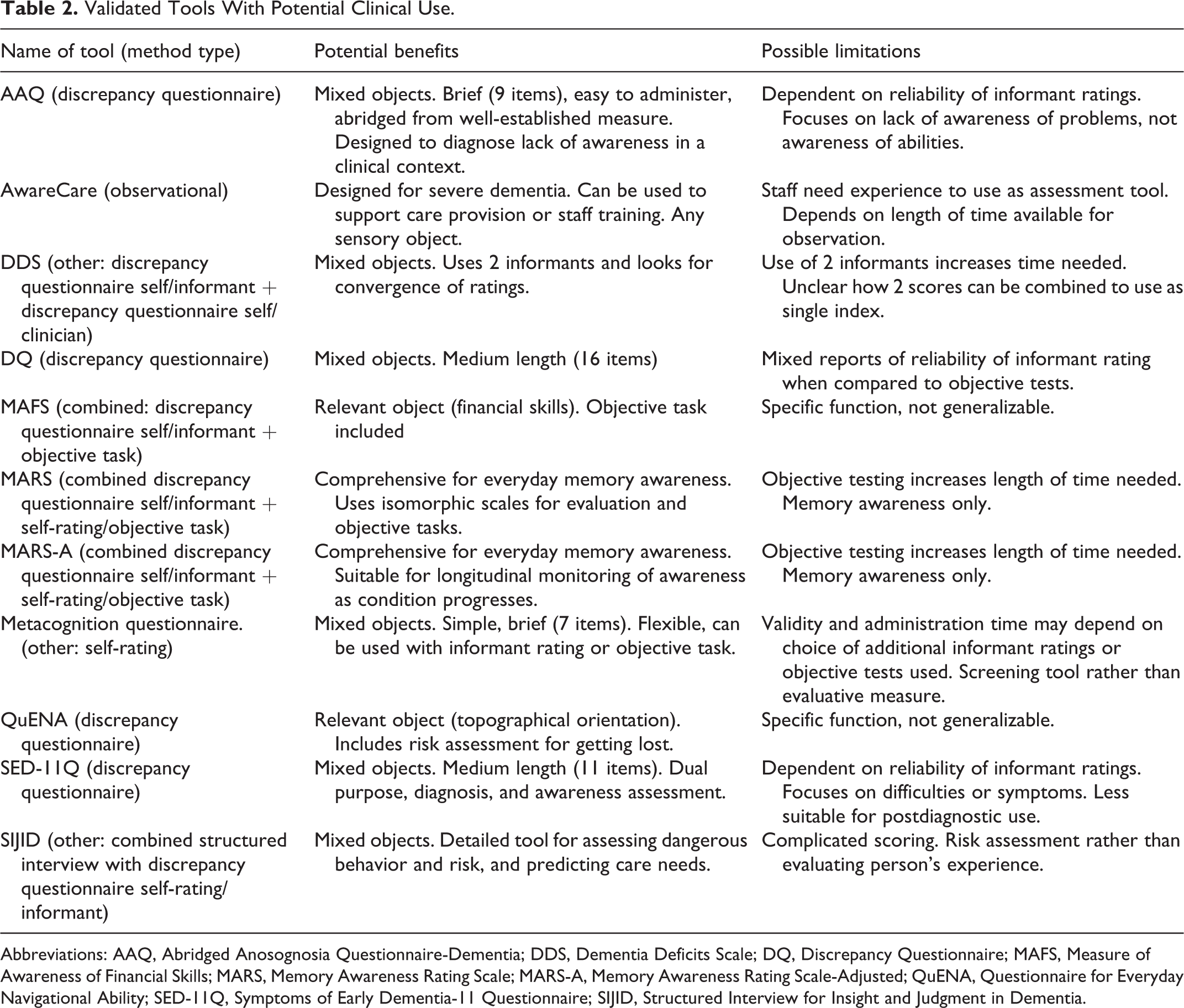
Abbreviations: AAQ, Abridged Anosognosia Questionnaire-Dementia; DDS, Dementia Deficits Scale; DQ, Discrepancy Questionnaire; MAFS, Measure of Awareness of Financial Skills; MARS, Memory Awareness Rating Scale; MARS-A, Memory Awareness Rating Scale-Adjusted; QuENA, Questionnaire for Everyday Navigational Ability; SED-11Q, Symptoms of Early Dementia-11 Questionnaire; SIJID, Structured Interview for Insight and Judgment in Dementia.
Finally, in 5 measures, clinical use is suggested, although it is not fundamental to the design. This includes 2 related tools (MARS and Memory Awareness Rating Scale-Adjusted [MARS-A]) that compare self- and informant ratings with an objective, ecologically valid measurement of memory function as well as computing a discrepancy between the self- and informant ratings. Another tool employs 2 informants to produce 2 discrepancy scores (Dementia Deficits Scale [DDS]). There is also a medium length discrepancy questionnaire that assesses mixed objects of awareness (Discrepancy Questionnaire DQ), and a brief questionnaire offering a simple, flexible scale that could be used alongside informant ratings and/or objective tests (Metacognition Questionnaire).
Discussion
Key Findings
To our knowledge, this is the first scoping review to use systematic methodology to investigate awareness measures in PwD and to appraise clinical utility. The review included both quantitative and qualitative methods and a range of dementia diagnoses and severity, with most of the research carried out in Western populations of people with mild-to-moderate AD. The results show that numerous methods of measuring awareness have been employed, which may reflect the different aspects of awareness that have been conceptualized and explored and/or the lack of an agreed gold standard. The most commonly used method employs the discrepancy between the person with dementia and an informant in evaluation of function, with clinician ratings the second most common method. Interestingly, we found that many methods were not validated and were frequently designed and used in a single study only. When established validated measures were employed, they were often modified (in 28 articles) and consequently were used in a non-validated way. There were 16 tools used in dementia but developed in other populations, of which 3 have subsequently been validated for dementia. There were 30 measures that were developed and validated for use in dementia populations; only 11 of these have been proposed for clinical use, but there is little evidence that these tools have been adopted into clinical practice. The qualitative methods identified in the review demonstrate how awareness can be elicited and described, which could perhaps lead to the development of interventions, but are not directly suitable for a clinical tool. We anticipated that including case studies would demonstrate how awareness had been measured in clinical practice; however, we found only 4 case reports that provided detail of how awareness was assessed.
Addressing the Review Objectives
Characteristics of the measures
The characteristics of the validated measures can initially be delineated by the type of method represented. For measures that use discrepancy methods, reliability depends on the accuracy of each rating type. Informant ratings are supported in health measures used elsewhere, for example, 58 and if the informant knows the person well, they can describe everyday situations and highlight abilities or problems. Not all PwD have a close family member or carer available to provide this information. While increased carer burden and/or carer stress has been associated with impaired awareness, 11,59 there are also documented concerns about accuracy of informant ratings, with more negative ratings made in the context of carer stress or a difficult relationship with the person with dementia. 6,60 -62 Apart from denoting areas where there is lack of awareness, perhaps indicating a need for closer supervision, measures of this type might also be useful in identifying areas of potential disagreement between the dyad, where sensitive negotiation is required.
Self-ratings by PwD can be influenced by personality, self-concept, and mood, 6,63 which can further reduce the reliability of the discrepancy methods. However, some studies have shown ratings by PwD to be more accurate than the informant evaluation when compared to actual performance. 64 Awareness is an essentially subjective experience, so enabling self-expression of experiences, as demonstrated in some of the qualitative studies, 65 -68 may be integral to portraying the phenomenon faithfully. Ideally, this would be in comparison to an objective marker, such as expressed awareness of diagnosis or condition in relation to a clinically determined diagnosis of dementia.
There is some evidence that objective performance methods are more accurate than informant discrepancy methods. 69 Performance tasks can sometimes be unrepresentative of everyday function, and reliability can be influenced by anxiety due to an unfamiliar task and surroundings. Some of the measures we reviewed employed everyday tasks to reduce this factor, for example, rating prior experience and current performance of remembering a message to deliver, recognizing people or finding one’s way around (MARS), or being able to remember medication instructions or name and address (Williamson Percentile Ranking Method). As the dementia progresses, tasks at home tend to be performed with more supervision from carers, so formal assessment under standardized conditions may become a more typical representation of everyday situations. 64 Using a combination of these methods, with self-rated, informant rated, and objective scores as in MARS, MARS-A, and MAFS, is likely to improve accuracy of the awareness assessment, 8 but may become unwieldy where brevity is required, such as in a clinical setting.
Clinician ratings can be prone to subjectivity bias, particularly the least structured measures that may depend on clinician experience, or be influenced by prior knowledge of the participant or the strength of the professional relationship. Some measures provide detail of inter-rater reliability (eg, Reed) but typically lack other validation data. However, it should be noted that recommendations for validation criteria have developed over the years, 70 as reflected in the increasingly comprehensive validation data generally provided for the more recently developed measures, for example, AAQ, SIJID, and Insight Questionnaire.
The scope of a measure is indicated by the intended aim, for example, a predictive tool such as SIJID, developed for risk assessment, could assist in care planning and resource management. A discriminative tool, such as the CERAD insight item, could be used to assist in determining diagnosis of dementia subtype or offering interventions. Single-item measures tend to treat lack of awareness as a symptom to be elicited but lack the amount of detail about individuals that would be needed for personalized care planning. Dual-purpose tools (eg, SED-11Q) could assist time management at the diagnostic appointment, but may be less suitable for a post-diagnostic assessment of awareness. Some tools are designed for an in-depth evaluation, which could allow a more tailored response to care discussions (eg, MARS, MARS-A), but again, the length of assessment could be a barrier to clinical use.
We would expect a clinical measure to assess awareness of relevant and specified objects. A range of objects were assessed in most of the validated measures, including 7 of the potential clinical tools, although 2 are limited to memory awareness (MARS, MARS-A). Tools with relevant but specific narrow aims (MAFS, QuENA) would benefit a specialized assessment, for example, by an occupational therapist, where these specific needs had been identified, but not a general assessment. Only one tool (AwareCare) was specifically designed to assess awareness in people with severe dementia. This is also the only tool that uses a purely observational method that is not reliant on verbal ability of PwD, and the only validated measure that assesses awareness at the sensory registration level.
In general, the articles in this review did not specify the level of awareness under consideration, 25 although those using discrepancy questionnaires could be described as operating at the evaluative level. Again, there are few measures with a stated aim to measure meta-representational awareness, although many measures, including clinician ratings, start with a question for the person with dementia concerning any problems with function or eliciting the reason for attendance, such as CIRS, ASPIDD, SC-Q, and Guideline for the Rating of Awareness of cognitive Deficits (GRAD), or how their condition affects others, such as University of California Los Angeles Structured Insight Interview (UCLA-SII), DDS, and DQ. The use of vignettes explored how PwD may recognize and interpret changes in others with dementia, without a direct challenge to personal identity. Studies using mixed methods 71 have shown how illness representations could be used to enhance communication by mirroring the language used by the person with dementia, regarding illness, to explore awareness of identity and cause of condition. It would be interesting to see if these approaches could be incorporated into a quantitative measure of awareness.
Awareness can be assessed at the level of performance (online) monitoring, and research has demonstrated the contribution of this aspect of awareness to overall functioning, using error detection methods, for example. 72 -74 Although these metamemory studies, as well as some naturalistic studies 64,69,75 investigate error responses and/or evaluation of performance after a test, only a few validated measures of awareness incorporate this approach, such as MARS, MAFS, and CMT. Online monitoring of performance is an ability that could be targeted in goal-orientated cognitive rehabilitation programs, 76 and testing awareness at this level would be a useful component of a clinical tool to direct interventions.
The review showed that the commonly used terms were anosognosia, insight (or lack of), and awareness, but also found the use of “self-consciousness” and “self-awareness” as additional, broader descriptions of the awareness phenomena, incorporating self-concept with awareness of mental, physical, social, and moral matters. 77 -80 Different awareness terms were often used interchangeably, suggesting that the terms themselves may have little value in distinguishing between phenomena examined, unless clearly defined. Research has demonstrated that awareness is a complex nonunitary phenomenon, 17,22,23,37 and applying the levels and objects framework, it is clear that the validated measures do not all assess the same aspect or aspects of awareness, which leads to difficulties in making direct comparisons. Different processes are considered, for example, in acknowledging difficulties either with general memory (Memory discrepancy rating, Reed) or with specific tasks such as managing money and writing cheques (DQ, AQ-D, AAQ, MAFS); these are distinct from assessing awareness of actual performance in these areas (MAFS, MARS), and something different from a global assessment of awareness of having a brain condition or memory problem (UCLA SII, GRAD).
Clinical utility
A comparison of the clinical utility of the validated measures is problematic as there is currently no clear evidence of which phenomena would be most useful to measure in a clinical setting. Studies that have used awareness measures to select or assess interventions, 81 -85 or assist in diagnosis, 86,87 or to explore awareness in the context of capacity to make treatment decisions 18 have used a range of different measures, but there are insufficient clinical studies to provide a direct comparison of methods. The area of capacity to make decisions offers wide-ranging applications in clinical care, for example, regarding decisions about medication, further medical investigations and procedures, 18 -20,88 as well as social issues such as appointing power of attorney or making choices about hospital admission or care placement. Identifying the most appropriate way to measure awareness to inform capacity assessments would be valuable. Further studies may be required to ascertain precisely which phenomena and hence what kind of tool would be useful for these clinical purposes.
For simplicity, we can speculate which features would be beneficial. For ease of use in a clinic, discrepancy questionnaire measures are likely to be the simplest and quickest to administer, with reasonable training requirements for staff. The AAQ is the shortest of these, with 9 items. The optimal length of an assessment would be determined by the specific setting and use of a tool, with different requirements, for example, in an emergency assessment of needs, or a planned assessment for choosing activities or interventions. Single-item measures vary in brevity. Some, with limited complexity, use the response to a single question or a few questions, such as the CAMDEX awareness item. Others use information from a combination of sources, for example, Inaccurate Insight item, and could be incorporated into an in-depth assessment, but would be too lengthy to be used in a brief tool. Most of the validated questionnaire measures use an uncomplicated scoring method using a scale, a feature which would be suitable for evaluation of needs and monitoring of outcomes in a clinical context.
Considering accessibility to PwD, some validated measures require comparison of current ability to ability 5 years ago or ability 10 years ago (Memory Questionnaire and AII, respectively). This cognitively complex task could be difficult in the context of impaired memory function, although does potentially interrogate the awareness of change over time. A comparison of ability with an average person of the same age has also been used (Williamson Percentile Ranking Method). This concept may also be difficult for PwD to grasp, as found in the original MARS scale that was later amended to drop the “averageness” score. 89 Use of diagrams to indicate self-rated ability (eg, bell curve in Williamson Percentile Ranking Method) could be challenging if visuospatial function is impaired and for dementia diagnoses with primarily visual deficits such as posterior cortical atrophy, but may be more suitable where there is language impairment such as in semantic dementia.
Person-centered care 90,91 embodies the views of PwD at the center of decision-making, considering their individuality and seeking their perspective where possible. This should lead to a flexible approach to care that respects personal preferences and individual circumstances and relationships and is recommended in national and international guidelines. 92,93 The terminology used in some of the tools reflects their origins in a disease or deficit-orientated model rather than a person-centered approach, which may restrict the depth of personal information shared by the person with dementia. An interrogative style that describes a scenario and encourages the participant to describe how they think they might manage in that situation could collect information that is perhaps more authentic and different from a questionnaire that asks direct questions about the presence or absence of problems or deficits. Balancing the negative items that rate difficulties with the positive items that rate abilities could encourage highly aware PwD to report personal strengths and adaptations as well as perceived weaknesses. Using shared language when describing dementia has been shown to be helpful, 3 that is, finding out and using the term that the person uses to describe their condition, for example “memory problems,” “being forgetful,” or a diagnostic label such as “Alzheimer's,” and this could be effective when measuring awareness clinically. Although a relatively new advancement, involving PwD and carers in the development of tools, is likely to help in this regard.
Implications
Although there is an array of tools for measuring awareness, there are relatively few designed for clinical use and few studies in a clinical context. Considering the broad range of clinical areas where an awareness assessment would be valuable, it is conceivable that the requirements would not be satisfied by a single tool. Therefore, choice of tool should be governed by the task requirements, but we would anticipate the tool would include the features of relevant objects, brevity, and development in consultation with PwD. Awareness is most pertinent to the care of PwD where it influences well-being and autonomy. These areas can be summarized as (1) where impaired awareness of difficulties has serious safety implications, (2) where awareness of difficulties or prognosis leads to anxiety and low mood, (3) where impaired awareness of abilities results in unnecessary restriction, and (4) where the mismatch in perception of ability between PwD and carers causes friction and stress. The available tools for clinical use tend to focus on the first issue, and recent developments include validated tools for risk assessment (SIJID) and for diagnosing lack of awareness (AAQ).
A finding of the review suggests that further investigation of clinical uses of measuring awareness would be informative. A new clinical tool for use in mild-to-moderate dementia, which uses a person-centered approach to elicit and measure awareness would be useful. The tool could build a profile of awareness across different domains, be used in individual care decisions, and identify areas of tension between PwD and carers, highlighting where extra support may be needed and identify areas for intervention. This might benefit from combining methods to improve reliability, with inclusion of a range of objects relevant to everyday life, while remaining short enough to be feasible for clinical use. The involvement of PwD and their carers in tool development would help ensure that a new tool is sensitive to the needs of PwD and the views of their advocates.
Models of care for PwD now focus on facilitating “living well” and maintaining independence where possible, recognizing individuality and encouraging self-involvement in decisions about care and activity where achievable. 94 A new clinical tool could help understand the lived experience of those living with dementia and to offer appropriate support in health care decisions, activity planning and care need provision as well as supporting carers, and signposting suitable interventions.
Strengths and Limitations
The scoping review framework allowed a broad scope, including studies employing different methodologies, and a range of types and severity of dementia. It also allowed flexibility in data extraction and analysis. The search was performed systematically, in line with a previously published protocol. The broad range of search terms resulted in a large number of articles included in the review. In keeping with scoping review guidance, quality criteria were not applied to the included articles; however, focusing on validated measures may have mitigated this to some extent. The psychometric properties of the validated measures were not fully evaluated, as this was outside the remit of this review; here we set a low threshold for describing studies as validated, to allow for a more inclusive and comprehensive appraisal of measures. A follow-on study could usefully employ systematic review methodology to review the selected validated measures in more detail.
Gaps in Research
The articles in this review are primarily from Western regions and ethnicity was not consistently reported, though it is possible that this may have been due to limiting articles to English-language only. It is unclear whether measures would be acceptable for use across cultural groups. Few methods categorized the level of awareness studied and inclusion of different levels could ensure a wider ranging assessment of awareness. There are few measures suitable for clinical use that adopt a person-centered model. Studies using or comparing tools in clinical settings are lacking. A brief clinical tool with a person-centered approach would be a useful addition.
Conclusions
Although there are many areas where measuring awareness could be advantageous, there were few studies that investigated clinical applications in dementia and there were few tools designed specifically for clinical purposes. For assessing awareness in severe dementia, the AwareCare measure offers a useful observational tool that can be used in care home settings. In earlier stages of dementia when the person is likely to be living at home, specific functional awareness testing could include the MAFS to assess awareness of financial management skills, and the QuENA could be used to assess the risk of getting lost. A wider assessment of memory awareness could include MARS, or the MARS-A, in moderate dementia, which would be useful to indicate the problems likely to be encountered due to impaired awareness around everyday memory function. For a brief assessment of general awareness, use could be made of the AAQ in a home or hospital setting, or the Metacognition Questionnaire, which has the advantage of the flexibility to use different objective tests.
The identified clinical tools available for mild-to-moderate dementia were designed to measure reduced awareness and risk. However, there are other areas of care where assessing awareness could be beneficial. These include identifying people who are at higher risk of mood disturbance due to awareness of their condition, or highlighting choices or activities that are restricted by underestimation of ability by either the PwD or the carer, as well as revealing tensions between carer and PwD where views on abilities differ. Currently, there is no brief tool that evaluates awareness from a person-centered perspective. This is needed to enhance communication and the effectiveness of the assessment. Further investigation and development of a brief person-centered tool could facilitate health and care choices in mild-to-moderate dementia, targeting the most appropriate and effective use of resources and optimizing outcomes for living well with dementia.
Supplemental Material
Supplementary_File - Measuring Awareness in People With Dementia: Results of a Systematic Scoping Review
Supplementary_File for Measuring Awareness in People With Dementia: Results of a Systematic Scoping Review by Catherine M. Alexander, Anthony Martyr, Sharon A. Savage, Robin G. Morris and Linda Clare in Journal of Geriatric Psychiatry and Neurology
Footnotes
Acknowledgments
The authors are thankful for the contribution of Nicholas Luscombe and Jason Weetch who assisted in the title screening and full-text screening of articles for the review. The authors are also grateful for the additional expert opinion on clinical implications of the findings, provided by Professor Ivana S. Marková and Professor Robert T. Woods.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an Alzheimer’s Society clinical training fellowship for CMA (grant number AS-CP-17-001).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.