
Abstract
Objective:
We investigated whether physical exercise interventions improve cognitive functioning in nondementia populations.
Methods:
We conducted a systematic review of meta-analyses including only randomized controlled trials (RCTs). Two reviewers completed a systematic search of PubMed, Embase, PsychInfo, and Cochrane Controlled Register of Trials. Study characteristics, effect size data, and heterogeneity estimates were extracted and presented in tabular form. Methodological quality was assessed by 2 reviewers using the AMSTAR-2 checklist. The validity of results was considered based on AMSTAR-2 scores and study characteristics.
Results:
We included 11 meta-analyses: 6 focused on disease-free older adults and 5 on mild cognitive impairment (MCI) excluding dementia. These meta-analyses summarized 97 unique RCTs. Methodological quality ranged from critically low to high. For overall cognitive functioning, which was the outcome of 6 meta-analyses, 1 showed improvement due to exercise interventions in disease-free older adults (g = 0.29, P < .01), while 2 reported nonsignificant effects. In patients with MCI, 3 meta-analyses reported significant benefits of exercise interventions on overall cognitive functioning (g = 0.25-0.57, P < .01). For cognitive domains such as attention and memory, there was limited evidence of beneficial effects of exercise demonstrated in either disease-free or MCI samples.
Conclusions:
Exercise may improve overall cognitive functioning in disease-free older adults, but there is too little high-quality evidence to conclude whether this is achieved through improvement in any of the specific cognitive domains assessed. There is clearer evidence that exercise may improve cognitive functioning in MCI, but again there is limited evidence across most cognitive domains.
Keywords
Introduction
The identification of interventions targeting lifestyle factors that promote healthy aging is of particular relevance in the context of an aging population and increasing pressure on health- and social care resources. In this context, age-related cognitive decline is a significant public health concern due to the impact on life functioning and the risk of development of neurodegenerative disorders. 1 Dementia is an age-related neurodegenerative disorder which consists of acquired cognitive decline in at least one cognitive domain, resulting in disturbance to essential cognitive processes such as thinking, memory, and perception. Population-level data suggest that Alzheimer disease (which accounts for 60%-70% of dementia cases) may be prevented by targeting lifestyle factors including physical inactivity. 2,3 Interventions aiming to increase exercise levels may therefore help protect against age-related cognitive decline, cognitive impairment, and neurodegenerative disorders including dementia.
Although there is a considerable body of prospective observational research on the association between physical exercise and age-related cognitive decline including dementia, 4 the observational nature of this research limits valid conclusions on causality due to the possible impact of confounding variables. Randomized controlled trials (RCTs) represent the best available methodology by which to test the hypothesis that age-related cognitive decline may be prevented by physical exercise. Due to the large samples and the long follow-up duration required for trials on true prevention of dementia, only a small number of trials assessing exercise interventions for the prevention of dementia have been published. One systematic review and meta-analysis which included 3 randomized studies assessing exercise interventions in the prevention of dementia diagnosis concluded that exercise did not significantly reduce the risk of dementia. 5 Since only 3 trials were available for this comparison, there is a high chance of false-negative findings. 6 Consequently, evidence on whether physical exercise prevents the onset of dementia is currently limited. Numerous trials are available on intermediate, related cognitive function outcomes, and therefore, a number of meta-analytic reviews have assessed the impact of exercise interventions on age-related cognitive decline. These outcomes are routinely assessed in clinical practice via neuropsychological testing to facilitate dementia diagnosis 7 ; therefore, investigating the impact of exercise intervention on these measures of cognitive functioning may provide an important insight into the prevention or lessening of age-related cognitive decline.
This article systematically reviews randomized preventative outcome studies testing the impact of physical exercise on overall (also known as global) cognitive functioning and specific cognitive domains (eg, executive function, memory recall, verbal fluency, or attention). We investigated whether there is evidence for a protective effect of physical exercise interventions on cognitive decline in nondemented populations, primarily disease-free older adults or adults with mild cognitive impairment (MCI). Due to the existence of a range of relatively up-to-date meta-analyses on this topic, 8 -10 we chose to conduct a systematic review of meta-analyses rather than replicate existing systematic searches for individual RCTs. “Providing a review of reviews allows the opportunity to assess the existing evidence on a macro level alongside commenting on the methodological stringency of the included reviews. This approach therefore allows the provision of clear recommendations for improvement of meta-analytic research in this field.”
Methods
A systematic literature search and systematic review of meta-analyses was performed adhering to the PRISMA 11 guidelines detailing the preferred reporting of systematic reviews and meta-analyses.
Protocol
A protocol was registered at PROSPERO specifying the intended aims and methodology of the broader project from which this particular review of meta-analyses developed as a subsection (PROSPERO registration number CRD42018094215).
Search Strategy and Study Selection
A systematic literature search was completed in December 2019 including the following databases: PubMed, Embase, PsychInfo, and Cochrane Controlled Register of Trials. Our initial aim was to search for meta-analyses focused on the prevention of dementia, while our secondary aim was to search for meta-analyses which targeted secondary or precursory outcomes, primarily cognitive impairment. An example of the search strings for PubMed is included in the Supplementary Materials. When possible we entered the relevant MeSH terms to better facilitate accurate category searching. We also performed simple searches of Google Scholar and examined the reference lists of published articles. All study selection was facilitated by the Covidence web application, which requires that 2 researchers (authors D.T.T. and M.X.H.) independently review each citation. Abstracts were first screened based on our exclusion and inclusion criteria. When abstracts suggested that studies met these criteria, full-text PDFs were extracted and examined in detail. Conflicts in study selection were discussed and resolved at both the abstract and PDF screening stages. Figure 1 provides the PRISMA diagram as an overview of study selection.
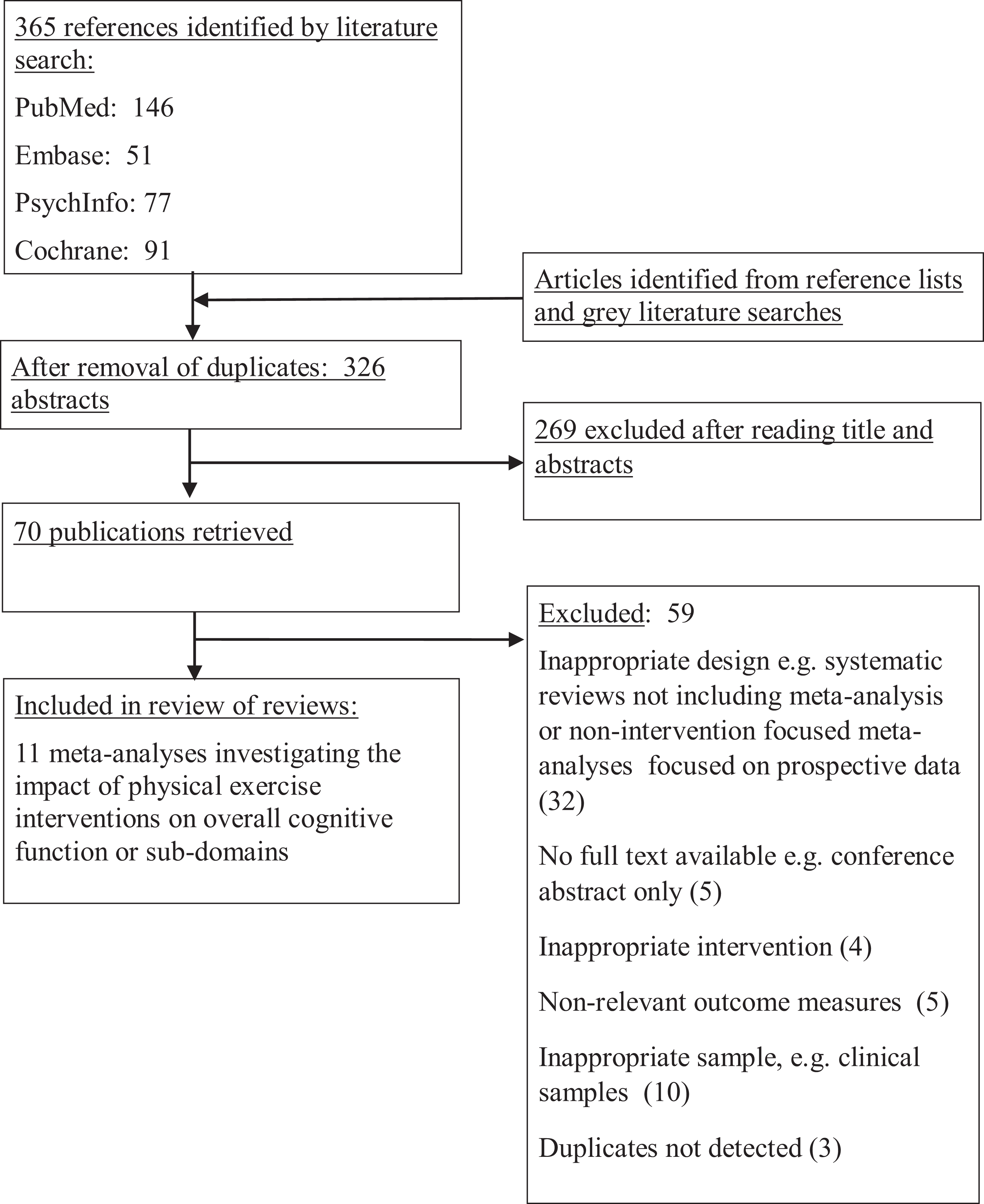
Flowchart of inclusion of studies.
Inclusion and Exclusion Criteria
We included (1) meta-analytic reviews which (2) reported pooled effect sizes from comparisons including only RCTs of (3) physical exercise interventions for (4) adults not diagnosed with dementia or (5) other morbidities (eg, obesity, cancer, and stroke). Meta-analytic reviews that reported pooled effect sizes from a combination of RCTs and noncontrolled trials were excluded, as were non-meta-analytic systematic reviews or reviews including observational research. Physical exercise interventions that integrated other elements into the intervention (eg, dietary advice or medication) were also excluded. Inclusion of participants with MCI formed a subsection of our review relevant to our research objectives. We excluded meta-analyses focused on children and/or adolescents since cognition at this early stage is not considered an indicator of dementia-relevant cognitive decline. For the disease-free older adults section, we included only meta-analyses studying older adults aged 55+. We included only meta-analyses published in English, Spanish, German, Dutch, or Greek based on language availability within the research team.
Assessment of Methodological Quality
To assess the methodological stringency of the included meta-analyses, we administered the AMSTAR checklist for each review. The AMSTAR-2 12 checklist is a measurement tool designed to assess the quality of the execution and reporting of systematic reviews. It consists of 16 items relevant to design methodology, such as satisfactory completion of a systematic search, adherence to population, intervention, comparison and outcome (PICO) design principles, assessment and consideration of the impact of risk of bias on meta-analytic findings, and duplication of study selection and data extraction. Two authors (D.T.T. and M.X.H.) independently rated the criteria and resolved any conflicts via discussion. Scores for each review were entered on the AMSTAR website, which applies a formula to categorize the relevant review as critically low, low, moderate, or high quality.
Data Extraction
Data on relevant study characteristics were extracted, namely, author, year of publication, target population, total number of RCTs included, form of exercise intervention, control condition, and which cognitive domains were assessed. We also extracted information on the effect size data from relevant meta-analytic comparisons alongside and preferred Hedge’s g when possible while also extracting Cohen’s d or mean difference effect sizes when g was absent. All meta-analyses utilized continuous outcome measures rather than dichotomous data; therefore, risk ratio or odds ratio effect sizes were not present. All data were extracted by one author (D.T.T.) and presented in tabular form. When possible we extracted information on the number of RCTs included in each comparison and the total N of each comparison. Data on the degree of heterogeneity present in meta-analytic comparisons were also obtained when available via the I 2 statistic. The included meta-analyses did not include sensitivity analyses for low risk of bias, which is a method that can be applied to provide a potentially more reliable effect size estimation by excluding trials with high risk of bias in subcomparisons. 13 We were therefore unable to provide effect size estimates from comparisons in which risk of bias had been minimized.
Overlap Between Meta-Analysis
In order to estimate the extent of crossover between meta-analytic research, we calculated the percentage of studies in each meta-analysis which were not included in any other of the included meta-analyses. This information was provided alongside study characteristics.
Power Calculation
For each meta-analytic comparison included, we calculated the available power based on the recommendations by Cuijpers et al. 14 Since the available effect sizes were of small to medium range, we estimated whether each meta-analysis had sufficient power to detect an effect size of Cohen’s d = 0.3 when assuming 0.80 power. We included this information as a column within the results tables.
Results
Figure 1 presents the study flow diagram detailing the inclusion of meta-analyses in this review. After the automated removal of duplicate records, 365 abstracts were screened for inclusion, resulting in 70 full-text PDFs being assessed. Of these, 11 meta-analyses assessing the impact of physical exercise on cognitive function and/or its subdomains were included in this study.
The resultant sample of meta-analyses included 97 unique RCTs in total. The percentage of unique RCT in each review is provided in Table 1. Six meta-analyses included healthy or nonclinical older adults as participants, while 5 included adults with MCI. AMSTAR-2 ratings ranged between critically low (2 meta-analyses), low (2 meta-analyses), and moderate (7 meta-analyses). One meta-analysis satisfied AMSTAR-2 criteria sufficiently to be rated as high quality. AMSTAR-2 ratings for each meta-analysis are provided in the Supplementary Materials.
Selected Characteristics of Included Meta-Analyses.
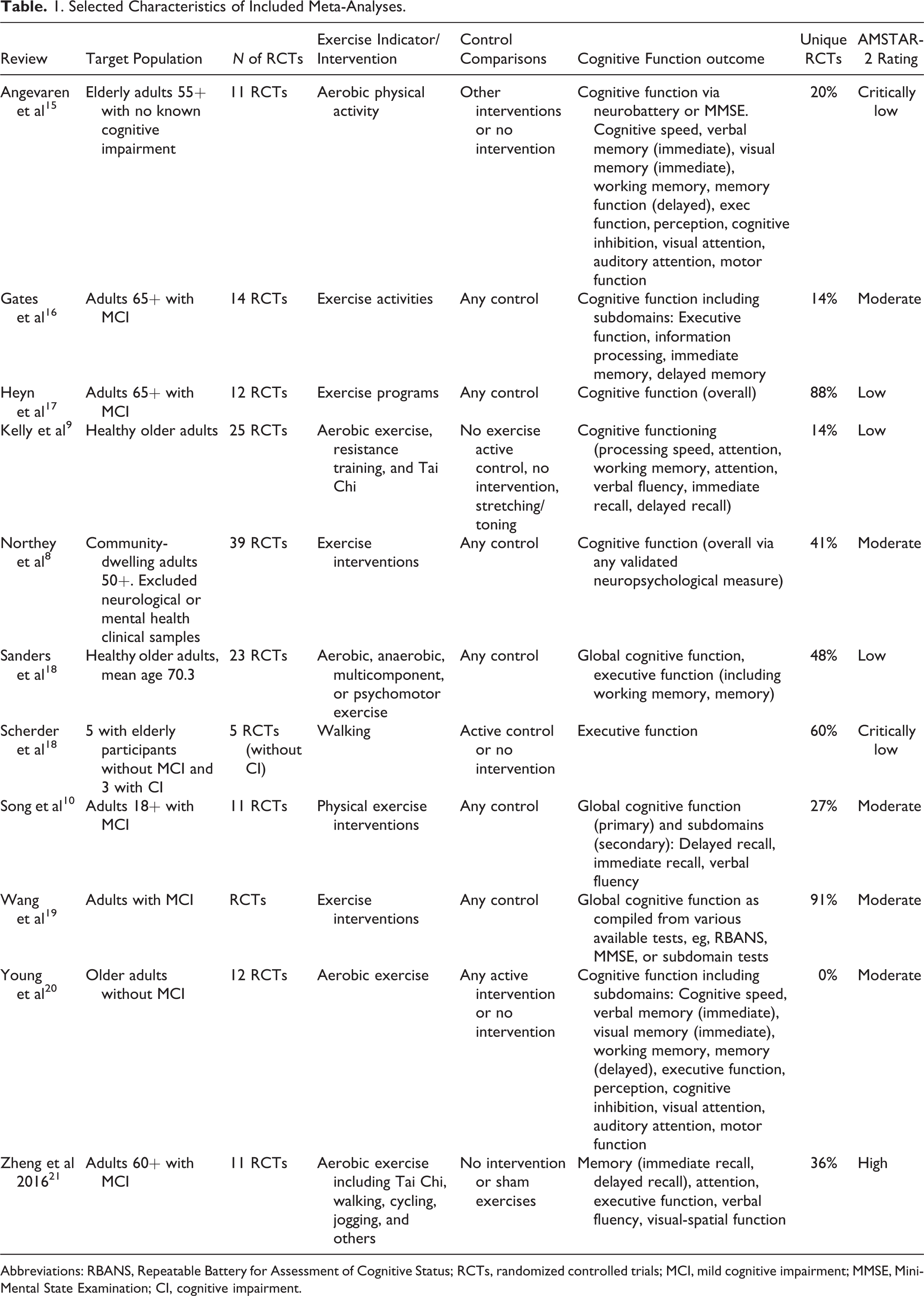
Abbreviations: RBANS, Repeatable Battery for Assessment of Cognitive Status; RCTs, randomized controlled trials; MCI, mild cognitive impairment; MMSE, Mini-Mental State Examination; CI, cognitive impairment.
Six meta-analyses assessed overall cognitive function as an outcome measure. A variety of cognitive domains were also assessed in meta-analytic comparisons including visual attention, auditory attention, simple attention, verbal memory, visual memory, working memory, executive function, and motor function. Further details on the outcome measures included in meta-analytic comparisons are included in Tables 1, 2, and 3.
Results of Meta-Analyses of Physical Activity Interventions for Healthy or Nonclinical Older Adults on Cognitive Function.
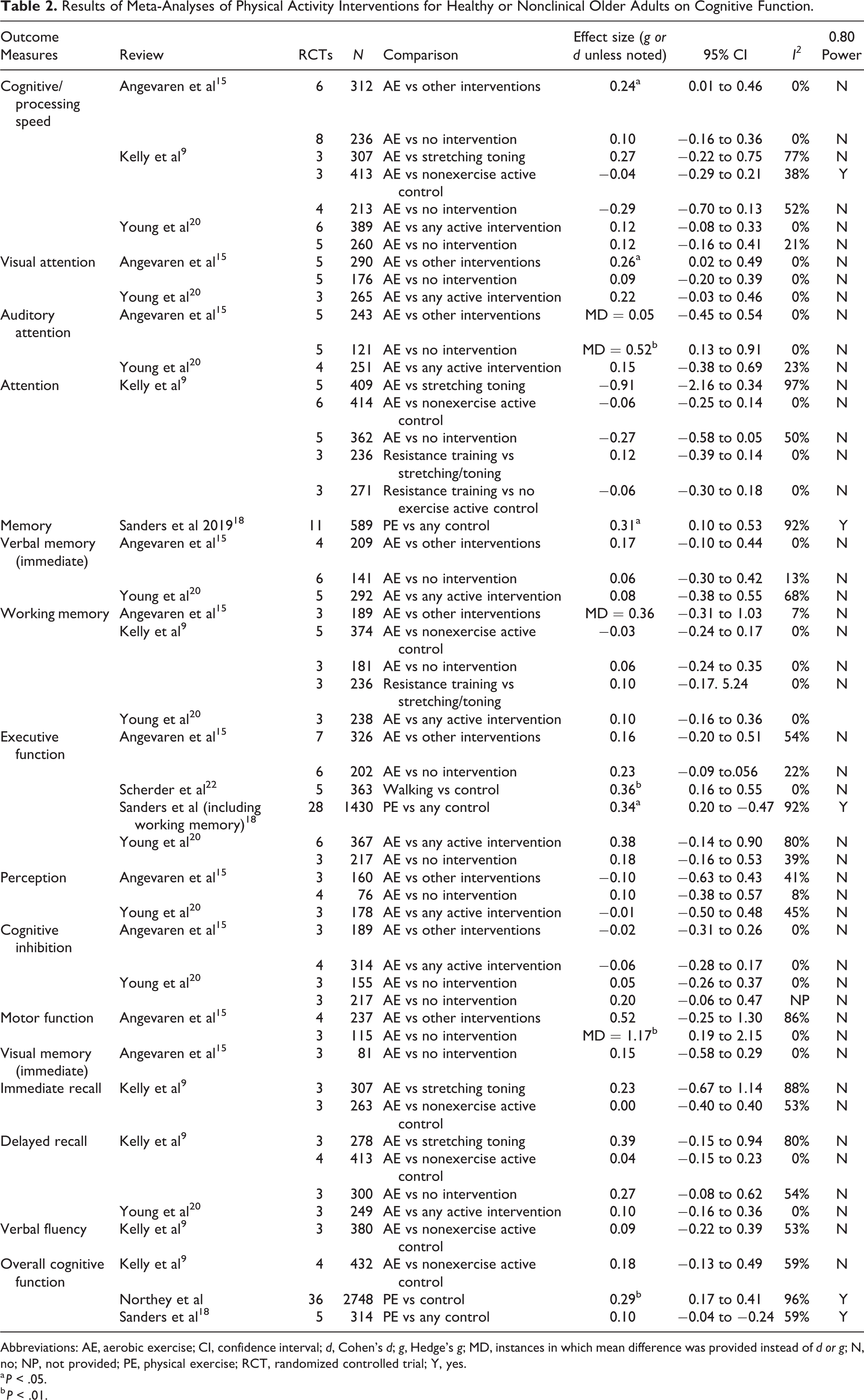
Abbreviations: AE, aerobic exercise; CI, confidence interval; d, Cohen’s d; g, Hedge’s g; MD, instances in which mean difference was provided instead of d or g; N, no; NP, not provided; PE, physical exercise; RCT, randomized controlled trial; Y, yes.
a P < .05.
b P < .01.
Results of Meta-Analyses of Physical Activity Interventions in Other Populations.a
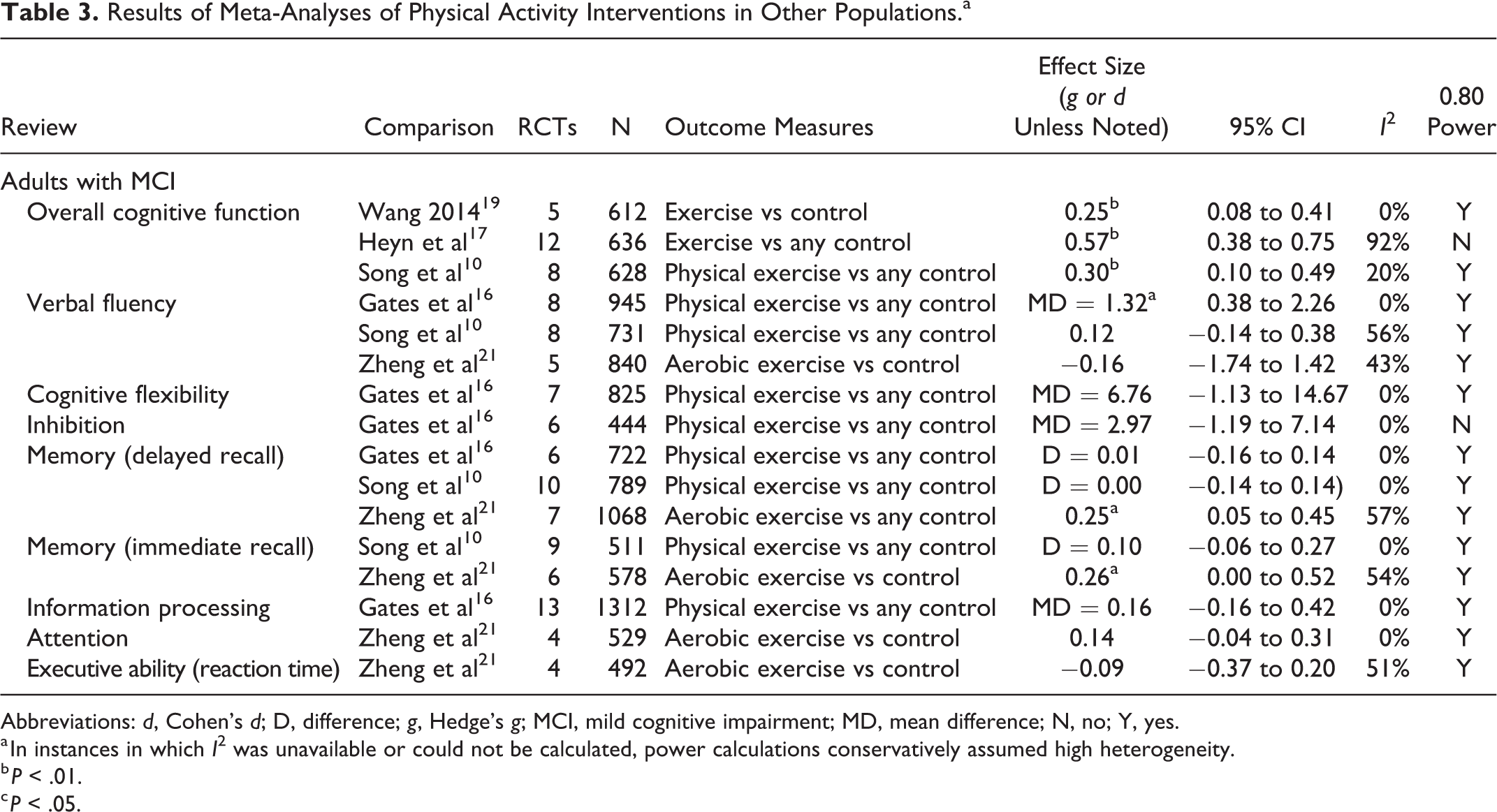
Abbreviations: d, Cohen’s d; D, difference; g, Hedge’s g; MCI, mild cognitive impairment; MD, mean difference; N, no; Y, yes.
a In instances in which I 2 was unavailable or could not be calculated, power calculations conservatively assumed high heterogeneity.
b P < .01.
c P < .05.
The majority of meta-analyses assessed physical or aerobic exercise/activity as the intervention, while 1 meta-analysis utilized walking only. 22 One meta-analysis also included resistance training as a subcategory, 9 while another included subcategories of exercise as “moderator” variables. 8 Control conditions ranged from nonexercise controls, active interventions, no intervention, or any control. One meta-analysis provided a subcategory of resistance training versus stretching/toning.
Overall Cognitive Functioning
Table 2 presents all results of meta-analytic comparisons of physical exercise interventions in disease-free older adults. Kelly et al 9 reported a nonsignificant effect (g = 0.18, P = .26) from 4 RCTs including 432 participants when comparing aerobic exercise versus any nonexercise control. Sanders et al 18 also reported a nonsignificant effect (g = 0.18, P > .05) when examining 6 RCTs including 314 participants comparing physical exercise to any control. Northey et al 8 included 36 RCTs (total N not specified) and reported a significant beneficial effect (g = 0.29, P < .01) when comparing physical exercise to any control. Significant heterogeneity was reported for this comparison, and although the I2 statistic estimating the percentage of variance explained by heterogeneity was not provided, we calculated heterogeneity as 96%. Twelve RCTs (85%) included in the meta-analyses of Kelly et al 9 and 3 (60%) of those in the meta-analysis of Sanders et al were included in the considerably larger meta-analysis of Northey et al. 8
Table 3 contains results for comparisons of physical exercise interventions in MCI samples. Overall cognitive functioning was also analyzed in 3 MCI meta-analyses. Wang et al 19 included 5 meta-analyses with 612 participants and reported a significant effect favoring exercise versus control (g = 0.25, P < .01), with no study heterogeneity present. Heyn et al 17 included 12 RCTs which included 636 participants and reported a significant effect favoring exercise versus any control (g = 0.57, P < .01). Heterogeneity was reported as nonsignificant. Finally, Song et al 10 included 8 RCTs with 628 participants and reported a significant effect favoring physical exercise versus any control (g = 0.30, P < .01) with low heterogeneity (20%).
Specific Cognitive Domains
Results of meta-analytic comparisons of exercise interventions for specific cognitive domains are presented in Tables 2 and 3. Significant comparisons and results of note are summarized subsequently.
Angevaren et al 15 included 6 RCTs in a comparison which included 312 participants in total and reported a significant effect favoring aerobic exercise versus other interventions for cognitive processing speed (g = 0.24, P < .05) with no heterogeneity. This effect was not replicated by Young et al 20 when comparing to active interventions (g = 0.12, P = .23). Inconsistency in results between Young et al 20 and Angevaren et al 15 is of note since the meta-analysis by Young et al 20 was commissioned as an update of Angevaren et al 15 for the Cochrane Collaboration; differential outcome may be explained by differential inclusion. The Angevaren et al’s 15 comparison of aerobic exercise versus no intervention was however nonsignificant, and there were no further significant comparisons in other meta-analyses. 9,20
Sanders et al 18 reported a significant effect of physical exercise interventions versus any control for memory (g = 0.31, P < .05) in disease-free adults. Scherder et al 22 reported a beneficial effect of walking versus control on executive function in disease-free adults (g = 0.36, P < .01) in a meta-analysis including 5 RCTs (N = 363) without significant heterogeneity. Sanders et al 18 also reported a significant effect for executive function (g = 0.34, P < .05), although their categorization also subsumed working memory within executive function. Both memory effects reported by Sanders et al 18 had high (92%) heterogeneity.
Angevaren et al 15 reported a beneficial nonstandardized mean difference effect on motor function (1.17, P < .01) for aerobic exercise compared to no intervention in disease-free older adults. No heterogeneity was observed, although only 3 RCTs (N = 115) were included. The effect for aerobic activity versus other interventions was nonsignificant (g = 0.52, P = .19).
In participants with MCI, Zheng et al 21 reported significant effects of aerobic exercises versus control for memory, each for delayed recall (g = 0.25, P < .05) and immediate recall (g = 0.26, P < .05). This meta-analysis was rated as high quality on the AMSTAR-2 criteria.
No meta-analyses found beneficial effects of physical exercise interventions on perception, verbal fluency, or cognitive inhibition, although comparisons were often hampered by low power.
Discussion
We found a mixed and in some instances conflicting pattern of results between meta-analyses examining the impact of physical exercise interventions on cognitive functioning and its subdomains. There was also considerable heterogeneity in the RCTs included between meta-analyses. Although exercise was suggested as beneficial to overall cognitive function in healthy or nonclinical older adults, this effect suffered from very high heterogeneity, which limits valid conclusion. Due to the reporting style in the review reporting this effect, 8 it was not possible to determine the specific RCTs included in this comparison, although on investigation, this comparison appeared to combine measures of various cognitive domains to produce one overall effect size for cognitive function rather than utilizing only outcome measures intended to comprehensively assess global cognitive function. We note a smaller nonsignificant effect size for global cognitive function reported by Northey et al 8 in the moderator analysis, which suggests that this comparison included outcome measures designed specifically to assess global cognitive function. This may therefore limit the reliability of this effect size. Other meta-analyses pooling measures of global cognitive function in healthy or nonclinical older adults did not report significant effects, albeit with smaller RCT samples.
In the specific cognitive domains, beneficial effects demonstrated by some meta-analyses were inconsistent in others. The methodological quality of meta-analyses also hampered conclusions in a number of instances, while in many subdomains, limited study availability meant low powered comparisons and the likelihood of unreliable estimates increasing the risk of both type 1 and type 2 errors.
Disease-Free Older Adults
Available evidence suggests that exercise has a beneficial effect on overall cognitive functioning in disease-free older adults; the best powered and best quality meta-analysis in this category by Northey et al 8 reported an effect size of g = 0.3 in favor of exercise versus controls, while the other meta-analyses in this category 9,18 were underpowered and assessed as low quality on the AMSTAR criteria. These null findings may therefore be unreliable. However, we also note the very high degree (96%) of heterogeneity in the meta-analysis of Northey et al, 8 which may be the result of the aforementioned combination of disparate cognitive outcomes to formulate a nonstandardized global cognition outcome. High heterogeneity limits clear conclusions by suggesting that the research included in this meta-analysis may be too divergent in terms of populations, outcome measures, and interventions for meaningful comparison. The pooled effect provided included RCTs applying aerobic exercise (17), resistance training (12), multicomponent training (9), Tai Chi (4), and yoga (2), which may explain high heterogeneity. This meta-analysis therefore risks comparing “apples and oranges” rather than a homogenous set of related interventions. Furthermore, limited reporting meant that estimates of heterogeneity, publication bias, or power were not possible on the moderator analyses that Northey et al 8 provided in an attempt to investigate subgroups in interventions, outcomes, and populations.
There were also significant beneficial effects reported for exercise for this population on cognitive processing speed, visual attention, motor function, and auditory attention in the meta-analysis of Angevaren et al. 15 These findings were not replicated in the update of Young et al 20 despite a high degree of crossover; 80% of RCTs included in the meta-analysis of Angevaren et al 15 were also included by Young et al, 20 while only 3 new unique RCTs were added. This inconsistency, alongside low power in a high proportion of the subdomains meaning a high chance of type II errors, adds to an unclear picture regarding the impact of physical exercise. Similarly, the meta-analysis by Scherder et al 22 reported a beneficial effect on executive function for walking versus controls, although the critically low AMSTAR rating for this meta-analysis limits reliable conclusion. The rest of the cognitive domains, namely, verbal memory, working memory, immediate and delayed recall, perception, cognitive inhibition, visual memory, and verbal fluency, did not demonstrate significant improvement following exercise interventions, although again limited study availability and therefore low power across comparisons limits firm conclusions. We therefore conclude that for disease-free older adults, there is preliminary evidence that exercise may improve overall cognitive functioning, but there is too little high-quality evidence to conclude whether this is achieved through improvement in any of the specific cognitive domains assessed. The broad nature of inclusion of outcomes and interventions for the Northey et al’s 8 pooled effect on cognitive function limits firm conclusion on the validity of the effect on global cognition. As discussed, such broad inclusion may have resulted in increased heterogeneity, which may indicate limited validity of the comparisons. The moderator analyses, while useful in indicating possible differential effects of exercise subtypes such as aerobic exercise or yoga, did not provide conventionally reported statistics for meta-analysis; therefore, it was difficult to conclude on the validity of these comparisons.
Adults With MCI
We observed a similar pattern of results for adults with MCI. All 3 meta-analyses assessing the impact of exercise on overall cognitive functioning in this population reported significant beneficial effects of the intervention, with effect sizes ranging from g = 0.25 to g = 0.57 without significant heterogeneity in any comparison. Two of these meta-analyses were assessed by the AMSTAR criteria as moderate, 10,19 while one was assessed as low quality, 17 which is somewhat understandable due to publication before full development of the PRISMA guidelines. 11 In summation, these results provide evidence that exercise interventions are broadly beneficial to cognitive function in MCI, although only 3 domains (verbal fluency, immediate recall, and delayed recall) showed evidence of significant improvement as a result of exercise. Study availability and therefore power was relatively higher in these comparisons than in the aforementioned comparisons of older adults, but there remained a lack of significantly beneficial effects observed in the cognitive domains.
Limitations
Like any review, the conclusions possible in this review of meta-analyses were dependent firstly on the available outcome data in terms of the RCTs included in the original meta-analyses both from a power and a methodology perspective. We also depended on the methodological stringency and reporting quality of the meta-analyses we included in our review, which when assessed by the AMSTAR-2 23 criteria were (excepting one review by Zheng et al 21 ) moderate at best and on occasions critically low. It is evident that meta-analyses in this area should strive to improve methodology and reporting to facilitate researchers drawing firmer conclusions regarding efficacy and the impact of potential bias. For example, in a number of the included meta-analyses, the total number of participants or heterogeneity statistics per comparison was not clearly reported. 8 Such problems were typically reflected in low or critically low AMSTAR-2 ratings; although in some instances, meta-analyses scoring moderate on the AMSTAR-2 showed evidence of such reporting problems. 8 Reporting problems may hinder the extent to which findings can be considered valid and reliable. We also note that our macro-approach of reporting from and assessing the methodological quality of published meta-analysis does not allow detailed comment on the methodological stringency of the RCTs included in each meta-analysis. We do however note that many comparisons were underpowered, suggesting that the RCT evidence base has room for further development in many areas, especially in disease-free populations when compared to the better powered MCI comparisons. Furthermore, 36% of the included meta-analyses did not assess risk of bias among the included RCTs, while 45% did not consider the impact of risk of bias on result. The methodological quality of much of the primary research is therefore unknown.
A further weakness of our design is that we were unable to compute our own effect sizes based on meta-analytic data from other studies, although we hope that our design provides as best possible a clear overview of the available efficacy data on exercise interventions targeting cognitive functioning. Strengths include a stringent systematic search procedure involving 2 authors and the assessment of methodological quality of included meta-analyses via AMSTAR, which allowed more detailed critique of the validity of conclusions.
Future Research
For the broader field, it is evident that more high-quality outcome research is required to allow clearer conclusions across the various cognitive domains by allowing sufficient pooling of RCTs to provide more reliable effect estimates. Further development of such research is required to draw firmer conclusions on the relationship between the provision of exercise interventions, their specific effects within the cognitive domains, and the currently observed effect on overall cognitive function; this effect was relatively consistent across both disease-free older adults and MCI populations.
For future meta-analytic research, the tendency toward broad inclusion of diverse physical exercise interventions, and on occasion broadly combined measures of cognition, may also require closer attention. To improve the validity of findings, it is important that interventions are conceptually similar rather than heterogeneous, and therefore, future research must consider this in design. There is however merit in the broad pooling of diverse exercise interventions followed by more specific sensitivity analyses which attempt to provide effect sizes on subtypes such as aerobic training, yoga, and resistance training as attempted by Northey et al. 8 We note however the importance that such comparisons clearly report heterogeneity statistics and participants included for each comparison alongside clear demarcation of RCTs included in each comparison since each of these important inclusions were limited in the review by Northey et al. 8 Where possible, pooling of original RCT data in individual participant meta-analyses may also allow investigation of the impact of individual participant characteristics (eg, demographic or clinical variables) on cognitive outcome.
Based on our assessment of the included reviews using the AMSTAR-2 criteria, there are specific areas of improvement required in meta-analytic design. Six of 11 included meta-analyses did not provide adequate explanation for or discussion of heterogeneity, while 9 did not address potential publication bias. A significant minority also failed to adequately investigate the impact of risk of bias in individual studies and/or the impact of risk of bias on interpreting outcomes. These methods are essential for the appropriate critical interpretation of meta-analytic results; therefore, inclusion of these specific features would help improve the quality of meta-analytic evidence in this field. Future meta-analyses should also ensure that risk of bias is assessed comprehensively among the included trials and that the potential impact upon the validity of results is considered, preferably in a statistical rather than narrative manner.
Conclusions
This review of meta-analyses attempted to collate and summarize efficacy data in the somewhat disparate field of outcome research investigating the impact of physical exercise interventions targeting cognitive function and its subdomains. We included only meta-analyses focused exclusively on RCTs in order to present the best available contemporary evidence. Although the evidence summarized in this review of meta-analyses does not provide direct evidence that physical exercise interventions are preventative of dementia, the evidence provided does suggest that cognitive functioning may be improved by exercise interventions and therefore may hold promise for future development in this domain.
Supplemental Material
Supplemental Material, JoGPN_supp_matts - Physical Exercise Interventions Targeting Cognitive Functioning and the Cognitive Domains in Nondementia Samples: A Systematic Review of Meta-Analyses
Supplemental Material, JoGPN_supp_matts for Physical Exercise Interventions Targeting Cognitive Functioning and the Cognitive Domains in Nondementia Samples: A Systematic Review of Meta-Analyses by David T. Turner, Mandy X. Hu, Ellen Generaal, Daniel Bos, M. Kamran Ikram, Alis Heshmatollah, Lana Fani, M. Arfan Ikram, Brenda W. J. H. Penninx and Pim Cuijpers in Journal of Geriatric Psychiatry and Neurology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Hersenstichting (English translation: Netherlands Brain Foundation). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.