
Abstract
Objective:
The aim of this work was to investigate marker profiles for proposed anxiety subtypes in Parkinson disease (PD).
Methods:
We used the persistent anxiety, episodic anxiety, and avoidance behavior subscales of the Parkinson Anxiety Scale as dependent variables in multivariable linear regression analyses using a cross-sectional data set of 311 patients with PD. Independent variables consisted of a range of demographic, psychiatric, and disease-specific markers.
Results:
In the most parsimonious model of persistent anxiety, higher Hamilton Depression Rating Scale scores, a history of anxiety, fewer years of education, lower Mini-Mental State Examination scores, lower Lawton Instrumental Activities of Daily Living scores, female sex, and complications of therapy (higher Unified Parkinson Disease Rating Scale part IV scores) were all associated with more severe persistent anxiety. Markers associated with more severe episodic anxiety included PD-specific disturbances of activities of daily living, complications of therapy, higher Hamilton Depression Rating Scale scores, female sex, and a history of anxiety. Finally, higher Hamilton Depression Rating Scale scores, a history of anxiety, complications of therapy, and longer disease duration were associated with avoidance behavior. After excluding clinically depressed patients with PD, disease severity and longer disease duration were significantly associated with episodic anxiety, but not with persistent anxiety.
Conclusion:
Persistent anxiety is mainly influenced by nonspecific markers, while episodic anxiety seems to be more PD-specific compared to persistent anxiety and may be more situational or contextual. These results provide support for possible distinct underlying constructs for anxiety subtypes in PD.
Introduction
Parkinson disease (PD) is a neurodegenerative disorder primarily characterized by motor symptoms; however, nonmotor symptoms such as anxiety and depression are common. 1 Depression has an estimated point prevalence of 17% in PD, and a recent meta-analysis showed a weighted point prevalence of 31% for anxiety disorders. 2,3 Anxiety contributes to cognitive impairment, increased severity of motor symptoms such as freezing episodes, and has a negative impact on quality of life and self-perceived health status. 4 -8
In the general population, anxiety disorders are typically classified according to the Diagnostic and Statistical Manual of Mental Disorders (DSM). This manual differentiates various anxiety disorders, such as generalized anxiety disorder, which is characterized by a chronic, persistent state of anxiety, as well as anxiety that is episodic such as panic disorder or social phobia, with the latter typically accompanied by avoidance behavior. 9 Although many studies investigating anxiety disorders in PD have relied upon DSM classification, it is increasingly recognized that DSM criteria do not adequately describe the types of anxiety reported in the context of PD. 2,10,11 First, this finding is supported by the fact that approximately one-third of patients with PD diagnosed with anxiety experience a variety of symptoms from multiple anxiety disorders. Second, up to 13% of patients with PD have anxiety disturbances that do not meet the criteria for any specific anxiety disorder and are classified as anxiety not otherwise specified. Third, there is a high co-occurrence of depression and anxiety in PD, which is not accounted for in the DSM classification. 2
In PD, alternative classifications have been proposed, for example, Starkstein et al identified a 4-group classification system based on a latent class analysis of a sample of 342 patients with PD. 11 They defined 4 groups: (1) “no anxiety or depression,” (2) “episodic anxiety without depression,” (3) “persistent anxiety with depression,” and (4) “both persistent and episodic anxiety with depression.” These 4 categories have been consolidated into descriptive groupings: “episodic anxiety” and “persistent anxiety.” 11 Episodic anxiety includes mainly symptoms of panic disorder, agoraphobia, and social phobia, with a notable lack of depressive symptoms. Persistent anxiety encompasses the essential symptoms of generalized anxiety and is considered independent of the symptoms for panic disorder, social phobia, and agoraphobia but showing a high correlation with symptoms of depression. 11 This division of PD anxiety into “episodic” and “persistent” subtypes is further supported by a canonical correlation of items of the Hamilton Anxiety Rating Scale and Beck Anxiety Inventory in a large PD cohort. One factor interpreted as “generalized anxiety” primarily included symptoms associated with generalized anxiety disorder (GAD), while a second factor primarily included symptoms most associated with panic attacks and panic disorder. 12 Identifying dissociable anxiety subtypes in PD could point to different underlying neurobiology, that is, pathologic mechanisms, which may provide further guidance in classifying anxiety in PD and unraveling phenotype–genotype correlations. 13
In this study, we investigated marker profiles for anxiety subtypes using the Parkinson Anxiety Scale (PAS). 14 It is the only validated anxiety rating scale that consists of 3 subscales assessing persistent anxiety, episodic anxiety, and avoidance behavior. Using the PAS, we aimed to identify evidence for possible subtypes of anxiety in a large cohort of patients with PD.
Materials and Methods
Data from a cross-sectional multicenter study were used that was undertaken to develop and validate the PAS. Enrollment occurred between March 2012 and April 2013 and results of the primary study objective have been previously described. 14,15
Population
The multicenter PAS validation study includes data from 362 participants with idiopathic PD, diagnosed according to the Queen Square Brain Bank criteria. 16 Participants were recruited from 6 tertiary referral centers, including movement disorder clinics as well as neurology and psychiatric outpatient clinics of the participating centers. Participants with neurodegenerative disorders other than PD and those with severe cognitive impairment, defined by a Mini-Mental State Examination (MMSE) score below 23, were excluded. 17 All types of medication, including neurological and psychotropic agents, were allowed. Participants who previously underwent deep brain surgery could show different anxiety markers compared to nonoperated participants 18 and were therefore excluded from the current analysis. The total number of participants included in this analysis was 311.
Standard Protocol Approvals, Registrations, and Patient Consents
The local medical ethics committee at each participating institution approved the study. Participants gave written informed consent before inclusion in the study and received a small financial compensation for their participation.
Assessment
All participants underwent a comprehensive neurological and neuropsychiatric assessment. Both demographic and PD-specific variables were recorded (Table 1). Levodopa equivalent daily dose (LEDD), 19 marital status, education level, a history of anxiety or depression, and family history of anxiety or depression were assessed by a semi-structured interview during a baseline interview. In accordance with Movement Disorder Society Task Force recommendations, participants who experienced motor fluctuations were examined only during on states and were rated using an “inclusive” approach. 20 Disease stage was assessed using Hoehn and Yahr score. 21 The Unified Parkinson Disease Rating Scale (UPDRS) was used to assess motor function (part III), disease-related decline in activities of daily living (ADL, part II), and complications of therapy (part IV). 22 The UPDRS part IV allows for patient-reported assessment of the presence and severity of on/off fluctuations, dystonia, dyskinesias, and autonomic dysfunction as they occurred during the past week. Cognitive function and non-PD-specific, instrumental activities in daily living (IADL) were assessed with the MMSE 17 and the Lawton Instrumental ADL scale, respectively. 23 The presence of DSM-defined depressive and anxiety disorders was determined using the Mini International Neuropsychiatric Inventory section for depression (A and B) and anxiety (D, E, F, and H). 24 The severity of depressive symptoms was quantified with the 17-item Hamilton Depression Rating Scale (HAMD). 25
Demographic and Disease-Related Characteristics Included in the Analyses.a
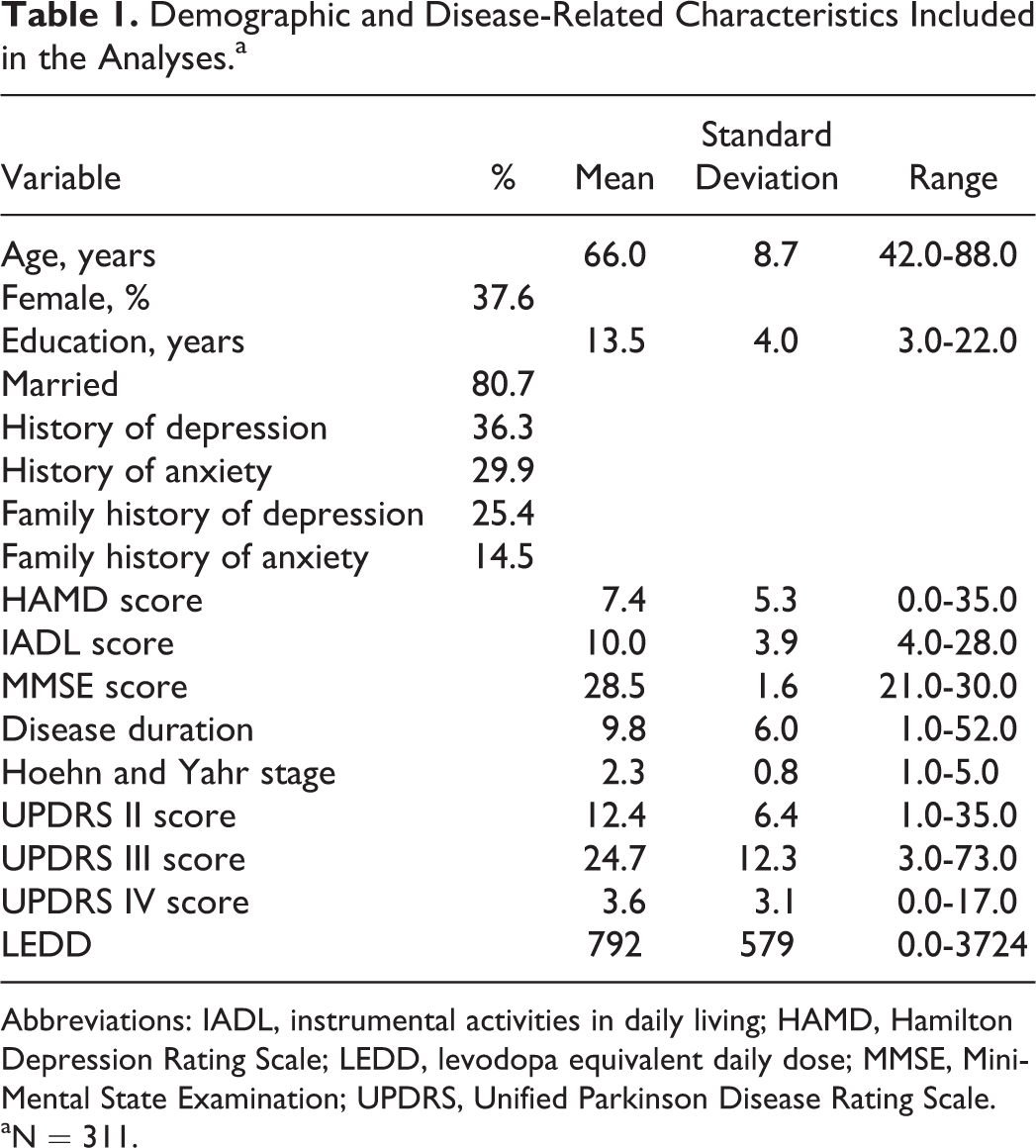
Abbreviations: IADL, instrumental activities in daily living; HAMD, Hamilton Depression Rating Scale; LEDD, levodopa equivalent daily dose; MMSE, Mini-Mental State Examination; UPDRS, Unified Parkinson Disease Rating Scale.
aN = 311.
Parkinson Anxiety Scale
The PAS consists of 3 subscales assessing persistent anxiety, episodic anxiety, and avoidance behavior with 5, 4, and 3 items for each subscale, respectively, and a total of 12 items. Avoidance behavior is considered a specific feature of anxiety, since it is listed in the DSM criteria of social phobia, specific phobia, and agoraphobia. 9 Each item is scored on a 5-point Likert scale, with a score of “0” indicating “not” or “never” and “4” indicating “severe or almost always.” The maximum score of the scale is 48 points. The PAS has previously been assessed and validated for acceptance, distribution, reliability, and stability with a good concurrent and known group validity. 14 It has a satisfactory factorial structure and it measures different dimensions of anxiety with acceptable to good Cronbach α values for all subscales. 14
Statistical Analysis
All analyses were performed using SPSS version 21.0 software (SPSS Inc, Chicago, Illinois, 2007). Demographic and PD-specific variables are presented descriptively. We used the observer-rated PAS as the primary outcome measure. A Spearman ρ correlation analysis was conducted to rule out multicollinearity between the explanatory variables. For each anxiety subtype, a separate multiple linear regression was used to test the hypothesis that different predictor variables would have a selective association with that specific anxiety subtype. Although there may have been some controversy in the past, recent opinion seems to justify using parametric tests with Likert scales measures. 26,27 First, a saturated multivariable model was fit with persistent anxiety as the dependent variable and all demographic variables and clinical variables listed in Table 1 as the independent variables. The included independent variables were chosen based on their known contribution to anxiety in PD from previous literature and their availability in the data set. 8,10,28 We used the UPDRS IV total score instead of single UPDRS IV items because no satisfactory explorative factorial analysis of the UPDRS IV scale has been reported to date. Next, backward stepwise regression (probability of F entry .05; removal .10) was used to test reduced models sequentially and to determine the best fitting and most parsimonious model. This procedure was repeated twice more with episodic anxiety and avoidance behavior as the dependent variable as well, to visually compare the significant associated markers in the final models. Statistical significance was set a priori at an unadjusted P = .05.
Results
Demographic and Disease-Related Characteristics
Table 1 shows demographic and disease-related variables for 311 participants. The study sample was comprised of 194 men and 117 women with an average age of 66.0 years (standard deviation [SD]: 8.7). The mean disease duration was 9.8 years (SD: 6.0), with a mean UPDRS III total score of 24.7 (SD: 12.3). Based on the MINI, 47 (15%) participants met the diagnostic criteria for a generalized anxiety disorder, 34 (11%) for agoraphobia without panic disorder, 11 (4%) for panic disorder, and 26 (8%) met the diagnostic criteria for social phobia. In addition, 7% suffered from major depressive disorder and 8% from dysthymia. Descriptive statistics for anxiety disorders, depressive disorders, and PAS total and subscale scores are shown in Supplemental Table 1.
Markers Associated With Anxiety Subtypes
An exploratory correlation analysis showed no multicollinearity between the independent variables included in the analysis (correlations all <.70). A backward regression analysis with persistent anxiety as the dependent variable showed a final model explaining 53% of total variance (adjusted R 2 = .533). More years of education, lower MMSE total score, higher HAMD total score, a history of anxiety, complications of therapy (UPDRS part IV score), non-PD-specific problems in ADL functioning (total IADL total score), and female sex were significant associated markers for more severe persistent anxiety. The final model with episodic anxiety as the dependent variable explained 33.5% (adjusted R 2 = .335) of the total variance and showed disease-specific problems in ADL functioning (UPDRS part II score), complications of therapy, higher HAMD total score, female sex, and a history of anxiety as significant markers for more severe episodic anxiety. The final model with avoidance behavior as the dependent variable showed complications of therapy, higher HAMD total score, a history of anxiety, and longer disease duration as significant associated markers and explained 26% of total variance (adjusted R 2 = .259). The UPDRS part III, motor function, was not included in any of the final models because it did not reach significance. The HAMD total score had the strongest association with persistent anxiety (β = .507), followed by avoidance behavior (β = .345) and episodic anxiety (β = .278). See Table 2 for complete coefficients, standard error, and P values and Figure 1 for a model summary.
Standardized Regression Coefficients for the Significant Markers in the Final Models for Each Anxiety Subtype.a
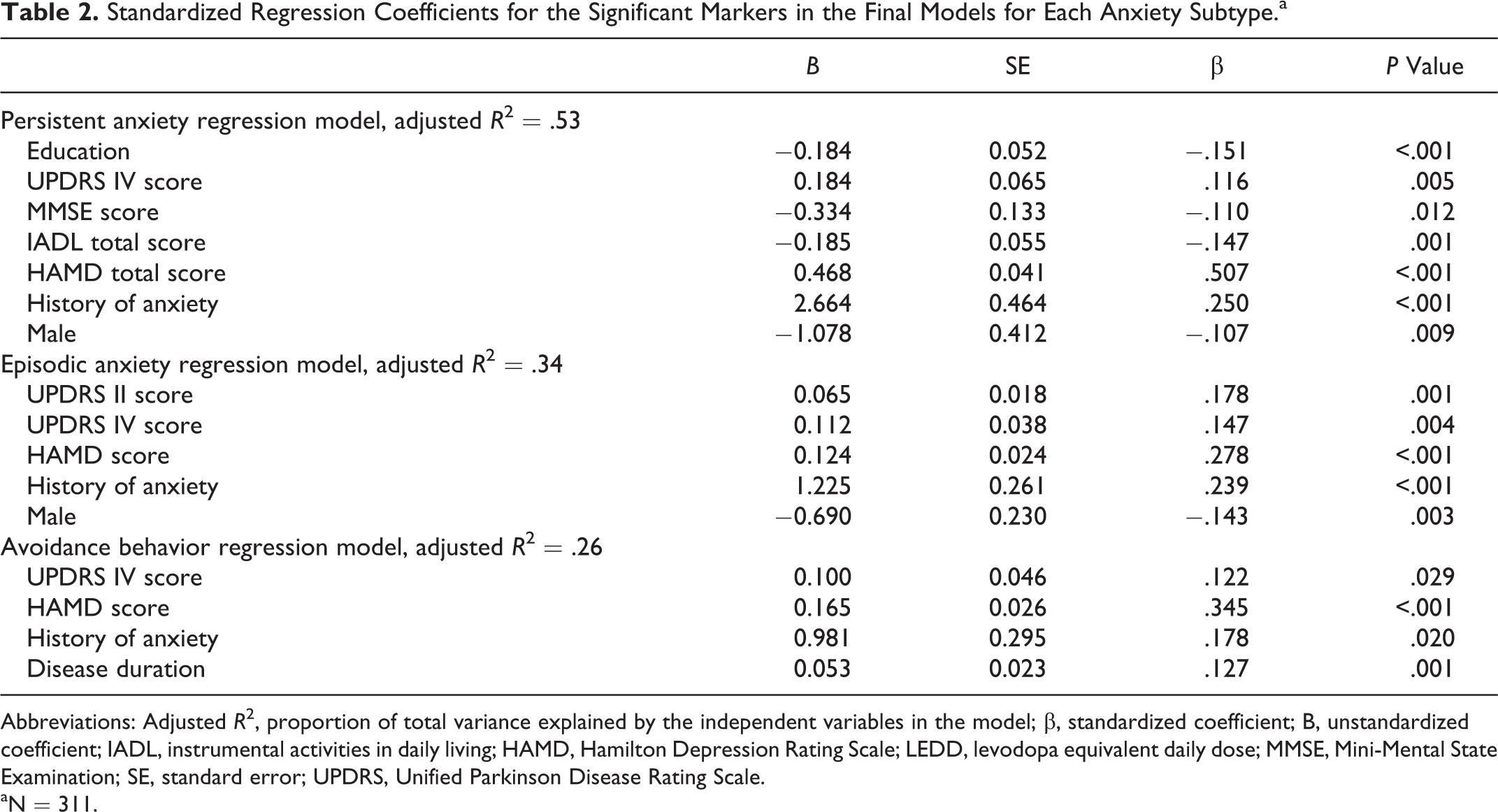
Abbreviations: Adjusted R 2, proportion of total variance explained by the independent variables in the model; β, standardized coefficient; B, unstandardized coefficient; IADL, instrumental activities in daily living; HAMD, Hamilton Depression Rating Scale; LEDD, levodopa equivalent daily dose; MMSE, Mini-Mental State Examination; SE, standard error; UPDRS, Unified Parkinson Disease Rating Scale.
aN = 311.
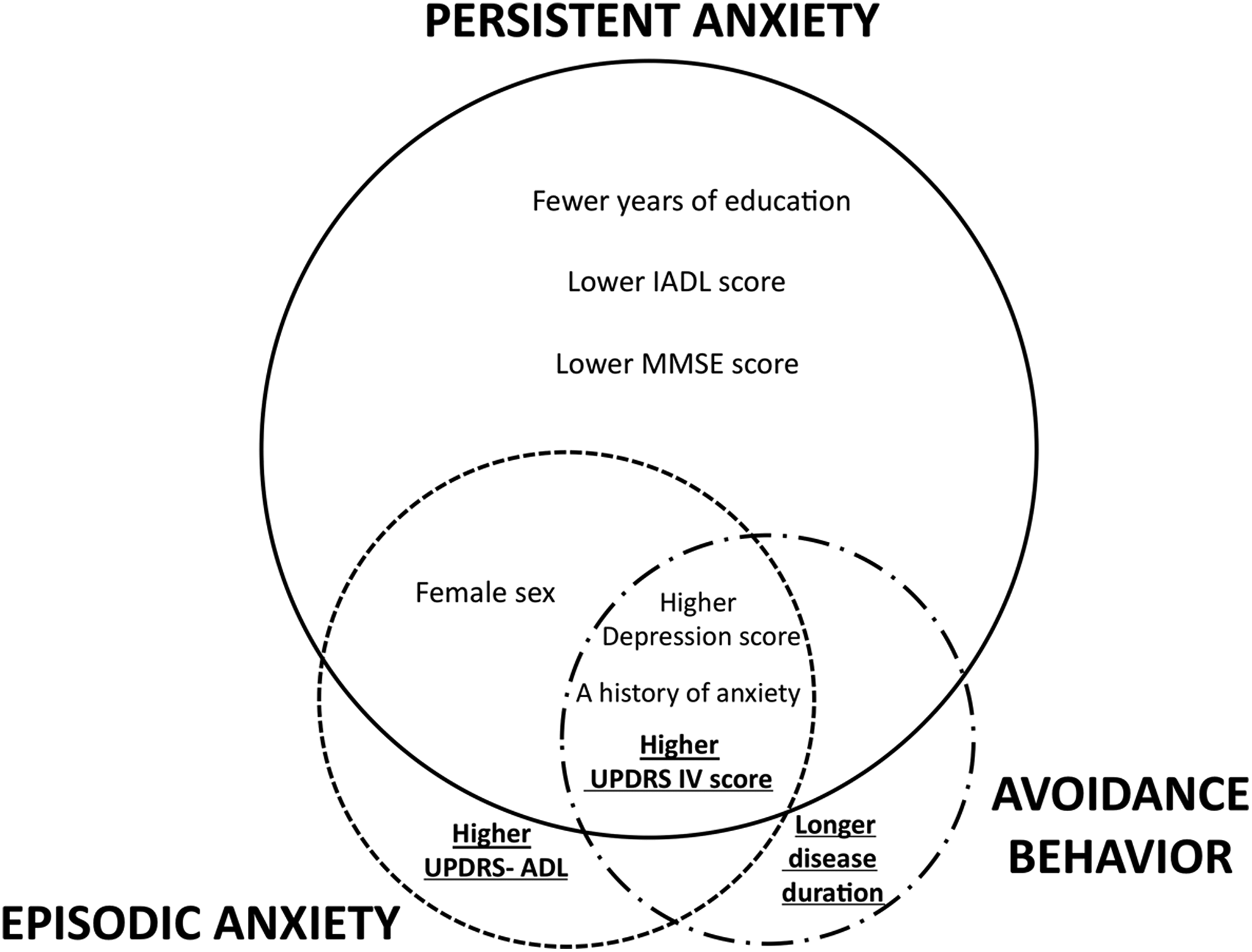
Venn diagram of the anxiety subtypes. The diameter of the circles correlates with the total variance explained by the regression models. Overlapping circles represent shared markers. Parkinson disease–specific markers appear in bold and underlined.
Markers of Anxiety Subtypes in Nondepressed Patients With PD
Given that the HAMD depression score was the strongest marker in all 3 models, we conducted an exploratory post hoc analysis to test whether markers would change if participants with clinically significant depressive symptoms were excluded. To this end, we excluded participants with an HAMD score ≥10, the cutoff score for screening depressed patients with PD. 29 We repeated the multiple regression analyses with each anxiety subtype as the dependent variable in the remaining 219 participants (70% of total sample). Coefficients, standard error, adjusted R 2 and P values for these adjusted models are shown in Supplemental Table 2. In the final model with persistent anxiety as dependent variable, total years of education and non-PD-specific problems in ADL functioning remained significant associated markers. Complications of therapy, higher HAMD total score, a history of anxiety, and a family history of depression were associated with more severe persistent anxiety. In the final model with episodic anxiety as a dependent variable, higher Hoehn and Yahr stage and longer disease duration became significant PD-specific markers, with higher HAMD total score and history of anxiety as significant non-PD-specific markers. The final model of avoidance behavior remained the same, with the exception that HAMD total score was no longer a significant marker. A history of anxiety was the marker with the strongest association in all 3 models.
Finally, several studies reported a possible association between anxiety levels and motor fluctuations. 8,30 We explored the association between UPDRS item 36 (wearing off fluctuations) and anxiety subtypes by replacing UPDRS IV total score with item UPDRS 36 in the multiple regression models (data not shown). However, no significant association was found in any of the 3 final models.
Discussion
Our results provide evidence for distinct underlying constructs of persistent and episodic anxiety subtypes in PD. We found markedly different profiles of significant markers for the different anxiety subtypes, and after excluding depressed patients with PD, PD-specific markers showed a stronger association with episodic anxiety when compared to persistent anxiety.
In our study, demographic and psychiatric markers that are not PD-specific, and in particular depression scores, were the main markers for all anxiety subtypes. This finding aligns with a previously proposed model of anxiety in PD, based on a different patient sample, in which depression appears to be the main marker for anxiety and nonspecific risk factors had a greater influence compared to PD-specific risk factors. 31 Our observation that the most important markers for a specific psychiatric disorder are not specific to PD is also similar to a model of depression in PD. 32 Depression is the most important marker for all anxiety subtypes and this is substantiated by high comorbidity, especially between persistent anxiety and depression in PD. 10,28 This relationship is similarly observed in the general population. 33 The association between persistent anxiety and depression is also reflected in the considerable overlap in DSM-5 criteria for GAD and major depressive disorder. 9 Therefore, an “anxious-depressive subtype” was proposed to exist in PD, which is supported by its association with different clinical and demographic profiles when compared to depression alone. 34,35 A history of anxiety is the second strongest marker for all anxiety subtypes, and this result is in line with previous studies that have found that history of anxiety strongly predicts anxiety disorders in PD. 8,10
Few PD-specific markers were included in the final models, which may be explained by several observations. First, the fact that disease-specific problems in ADL functioning were associated with episodic anxiety is consistent with our previous finding that PD-specific anxiety may be more contextual or situational and related to off periods or impairment in ADL activities. 31 For example, psychological factors related to fluctuations, such as fear of falling, may elevate anxiety levels. Second, the marker “complications of therapy” includes a wide range of symptoms and this variety is a possible explanation of the association with all anxiety subtypes. It likely reflects not only dopaminergic deficits but also other monoaminergic impairments such as noradrenergic deficits in orthostatic hypotension. 36 Third, disease duration is associated with avoidance behavior and could reflect embarrassment and social withdrawal that accompany worsening of symptoms 37 or general social isolation due to immobility, although one would expect other PD-specific markers to be associated as well. Fourth, although the presence of motor fluctuations is a principal marker of anxiety in most studies, 8,30 we were unable to find an association between “wearing off” fluctuations and any of the anxiety subtypes in a post hoc analysis. Although likely the result of attempting to use a single item as a marker, another explanation could be that participants in our study were evaluated during the “on” state. The PAS rates anxiety in the past 4 weeks, and therefore, it is vulnerable to recall bias and it is shown that depressed participants in the general population have a high discrepancy between retrospective ratings and actual experiences. 38 Participants with anxiety related to wearing-off might rate their anxiety level lower during the “on” state, even if the recall period is 4 weeks. As a result, more subtle associations, especially with episodic anxiety, will be lost. In future studies, we suggest rating anxiety levels both in an on and off state to detect associations between certain anxiety subtypes and motor fluctuations. In addition, rating anxiety levels in both states could also reveal an underlying association between freezing of gait (FOG), a common off phenomenon, and certain subtypes of anxiety. Some studies suggest that episodic anxiety, for example, panic attack, is more common in patients with FOG, 39,40 but it is unclear whether there is also an association with persistent anxiety or avoidance behavior. Fifth, LEDD was not associated with any of the anxiety subtypes in this study. However, whether antiparkinsonian medication is a risk factor for anxiety in PD at all is still debatable with some studies reporting an association, 10 but others not. 8,41,42 Lastly, we only found an association between disease severity (Hoehn and Yahr stage) and disease duration with episodic anxiety after excluding clinically depressed patients in a post hoc analysis. This underlines the finding that depression is the most important marker, but might reflect that episodic anxiety is more specific to PD than persistent anxiety.
The PAS measures different dimensions of anxiety, 14 but our results show some overlap between markers of anxiety subtypes. This is in line with what clinicians encounter in daily practice, since about one-third of patients with PD with an anxiety disorder have 2 or more comorbid anxiety disorders. 2 Having multiple anxiety disorders is associated with greater morbidity, and finding patient-tailored and even subtype-directed treatments might be crucial. 43 The overlap in significant markers suggests that there may be shared pathophysiologic elements, but other factors may also be important for determining anxiety subtypes in PD. Findings in the general population and in previous PD studies could provide some guidance. In the general population, dependent or avoidant personalities are associated with different anxiety disorders and even predict their persistence. 44,45 There is evidence of an association between personality traits and anxiety in PD as well, 46 with different coping strategies comprising significant predictors of heightened anxiety and depression. 47 In addition, genetic vulnerability and developmental risk factors seem to play an important role in the general population in the differentiation of GAD and panic disorder. 48,49 Some evidence exists suggesting that patients with PD with certain mutations, for example, of the serotonin transporter gene, are more prone to develop anxiety. 50,51 Finally, anxiety is more common in PD compared to other chronic illnesses, suggesting a cause that is in part unique to PD. 52,53 Some research suggests a shared pathophysiology between anxiety and PD 54 with not only dopaminergic involvement but also impairment of the serotoninergic and noradrenergic network. 55 Moreover, impairment in dopaminergic networks, including mesolimbic projections to the amygdala, might be expected to cause an anxiety subtype differentiable from anxiety arising from widespread involvement of noradrenergic or serotonergic deficits. 56 -58
Recent studies demonstrate that anxiety is poorly identified in PD, with nearly half of patients with a current DSM-IV anxiety diagnosis not being treated. 42 In addition, of the patient who received pharmacotherapy, 83% still experienced a current anxiety disorder, suggesting that anxiety in PD is difficult to treat. Unraveling the associations between demographic or PD-specific factors and anxiety subtypes, and not anxiety as one symptom, could assist in the development of tailored pharmacotherapy or psychotherapy approaches.
This study has several limitations. First, variables selected to be included in the analysis were based on availability, and other potential important markers, such as personality, were not available. This limitation is reflected by the R 2 values of the final episodic anxiety and avoidance behavior models, and as such, some caution is warranted while interpreting the results. Inclusion of additional variables would provide a more complete overview. Second, the study is based on a cross-sectional data set, meaning no causal interferences can be drawn. Therefore, confirmation of these findings with inclusion of more psychosocial, genetic, and imaging variables, is needed. Third, we used an anxiety rating scale to classify anxiety subtypes instead of anxiety disorders based on DSM criteria. However, some anxiety disorders such as social phobia exhibit both avoidance behavior and characteristics of persistent anxiety, which confounds the use of the proposed subtypes. In addition, the DSM classification of anxiety disorders does not adequately describe the types of anxiety reported in the context of PD and the PAS is a valid measure of different dimensions of anxiety in PD. 14 Last, we used the terms “PD-specific” and “nonspecific” rather than “PD-related” and “PD-unrelated” markers because it is difficult to separate markers that are related to PD and those that are not directly related to PD. For example, in patients with PD, cognitive decline may be due to PD, but is also a known risk factor for anxiety in the general population, and hence not unique for PD.
In summary, our results provide support for possible distinct underlying constructs for anxiety subtypes in PD. Persistent anxiety is closely related to depression and mainly influenced by non-PD-specific markers. Episodic anxiety seems to be more PD-specific compared to persistent anxiety and may be more situational or contextual. These findings could not only provide the opportunity to develop preventive measures or interventions that target specific situations, but adequate classification of anxiety in PD could also give some guidance in phenotype–genotype research. Deciphering phenotype–genotype associations is an important step, which ultimately may lead to subtype-directed treatment strategies and individualized patient care. Studies are warranted with inclusion of more nonspecific markers, such as personality. Future studies of anxiety in PD may further benefit from use of real-life momentary assessments to unravel relationships among motor symptoms, anxiety, and contextual factors since they have demonstrated utility for detecting associations between motor fluctuations and emotional fluctuations at an individual level. 59
Supplemental Material
Supplemental Material, Supplementary_tables - Clinical Markers of Anxiety Subtypes in Parkinson Disease
Supplemental Material, Supplementary_tables for Clinical Markers of Anxiety Subtypes in Parkinson Disease by Martinus P. G. Broen, A. F. G. Leentjens, J. T. Hinkle, A. J. H. Moonen, M. L. Kuijf, N. M. Fischer, K. Perepezko, A. Bakker, and G. M. Pontone in Journal of Geriatric Psychiatry and Neurology
Footnotes
Authors’ Note
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Pontone is supported by NIH K23 AG044441. A. F. G. Leentjens receives payment from Elsevier Inc as Editor-in-Chief of the Journal of Psychosomatic Research. He has received research grants from the Michael J Fox Foundation and the Stichting Internationaal Parkinson Fonds, as well as royalties from Reed-Elsevier, de Tijdstroom, and Van Gorcum publishers. J. T. Hinkle receives tuition and stipend support through the Medical Scientist Training Program at the Johns Hopkins School of Medicine (NIH/NIGMS 5 T32 GM007309). A. Bakker has received research grants from the National Institutes of Health and is an inventor on Johns Hopkins University intellectual property with patents pending and licensed to AgeneBio, Inc. G. M. Pontone has received research grants from the Michael J Fox Foundation and the National Institutes of Health.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.