
Abstract
Childbearing trans and nonbinary people are confronted with the heteronormative and cisgender frameworks that underpin “maternity” services. We explored the educational needs of 108 perinatal staff in the United Kingdom as related to the needs of trans and nonbinary service users. Participants were most confident in formulating care plans and least confident about the provision of colleagues’ perinatal care in this context. While the majority of participants were positive toward the trans and nonbinary communities, they considered that those communities remain marginalized in perinatal services. Transphobic, anti-trans, and nonbinary attitudes were highlighted by our respondents. Our findings suggest that caregivers witnessed transphobia among colleagues and were apprehensive themselves about providing care to childbearing trans and nonbinary people. They reported a cisheteronormative model of care that lacked awareness of trans and nonbinary issues. The educational needs identified included information about the practicalities of childbearing as a trans or nonbinary person, how to use inclusive language effectively, and creating policies and processes for supporting childbearing trans and nonbinary people. These caregivers’ preferences included hearing from trans and nonbinary people and sharing best practices among themselves, with open discussions about how to be inclusive.
Trans men and nonbinary people are a growing population within “maternity” services. They need services for a range of family planning outcomes, including pregnancy and birth (Riggs et al. 2020). Unlike the term cisgender, used to describe a person who experiences a normative relationship between their gender and assigned sex, trans is used by some as an umbrella term referring to individuals and groups who do not experience a normative relationship between their gender and assigned sex (Ellis, McNeil, and Bailey 2014; Puckett et al. 2018). We use the trans umbrella in such a way in this paper. Trans people may use a variety of alternate terms to describe their gender identity. There is a great diversity of identities under the trans umbrella, with some individuals living between or outside of commonly known genders (e.g., nonbinary).
Midwifery services have historically focused on women with related etymology, such as maternity (maternal: from French maternel/maternelle, from Latin maternus, from mater “mother”) and midwifery (Middle English: “with woman”) (Darwin and Greenfield 2019). Midwifery’s raison d’etre has, therefore, traditionally been understood as assisting childbearing women. The midwifery profession itself is one of the last almost mono-gendered professions in which the gendered term midwife is now considered to be limited in its ability to include people of all genders and none (Pendleton 2022). Midwives along with nurses may also be given highly gendered titles such as “Matron” or “Sister” in this context. “Maternity” care has been theorized from feminist perspectives, as “woman-centered” care, focusing on women’s choice and autonomy in relation to how and where they give birth (Stewart 2004). Midwifery’s traditional focus on “mothers,” “women’s health,” and the related gendered language used in such services may be seen as presenting a challenge for some gender-diverse clients, calling into question the place of trans men and nonbinary people within such services (Pendleton 2022). Meanwhile, attempts by health professional bodies to incorporate more inclusive language (as this paper does by using such terms as perinatal care as an alternative to maternal/maternity care) have been framed by some as “erasing women” (e.g., Guzman 2021). However, the needs of women, trans men, and nonbinary people need not be considered as at odds. Treating people as individuals, avoiding assumptions, and recognizing diversity are key principles in the ethical codes of all health professionals.
Reproductive justice is an intersectional feminist framework acknowledging that people may experience restricted access to, or feel excluded from, reproductive services due to intersecting factors such as race/ethnicity. A reproductive justice framework acknowledges interconnected systemic barriers to care such as sexism, racism, and heterosexism (Morison 2021). The term originally focused on social justice in relation to reproductive issues such as abortion and contraception. However, its focus on diversity has subsequently expanded to include the reproductive rights of other marginalized groups, including trans and nonbinary people’s access to fertility and perinatal health care (Riggs and Bartholomaeus 2020). This approach can incorporate the impact of cisgenderism, an ideology that presumes people who are cisgender are the norm and delegitimizes trans and nonbinary people’s own understanding of their gender (Ansara and Hegarty 2013). This may manifest itself in cultural assumptions about gender, sexuality, and pregnancy, such as the cisgenderist and heterosexist assumptions that only cisgender women become or wish to become pregnant and that all pregnancies take place in the context of a heterosexual relationship. This nexus of expectations and assumptions is sometimes referred to as cisheteronormativity (Luxion 2020). Such assumptions can mean that trans men and nonbinary people do not experience the same support throughout their pregnancy as their cisgender counterparts (Charter et al. 2018; Riggs, Power, and von Doussa 2016). Such cisgenderism is grounded in a worldview of a gender binary, sustaining attitudes and beliefs perpetuating the stigmatization and exclusion of trans and nonbinary individuals (Eliason and Chinn 2018). Thus, individuals who do not identify as women may be challenged in a variety of ways throughout their childbearing journeys.
Some childbearing trans and nonbinary individuals experience a worsening of gender dysphoria, poor care, and increased vulnerability along with a profound sense of physical, social, and emotional isolation (Greenfield and Darwin 2020). Moreover, there are reportedly low levels of health care provider awareness and knowledge in adequately addressing their unique needs (García-Acosta et al. 2020; MacLean 2021). This presents opportunities to improve experiences and outcomes through the education of professionals.
We observed and reflected upon the challenges faced by the trans and nonbinary communities in perinatal services (Pezaro 2019). The research team also engaged in patient and public involvement activities via a series of online polls. These indicated a need to explore the attitudes, knowledge, confidence, and experiences of professionals to allow concerns and training needs to surface. Equality Network, a leading national charity working for lesbian, gay, bisexual, transgender, and intersex (LGBTI) equality and human rights in Scotland, joined the research team in this project. This academic partnership along with patient and public involvement activities enabled the team to avoid duplicating existing research in the field (Crowther et al. 2021). Our goal was also aligned to improving education in this area (Besse, Lampe, and Mann 2020; Kattari et al. 2020). Ultimately, the aim of this research was to explore the trans- and nonbinary-related experiences and educational needs of professional perinatal staff. Specifically, our objectives were to investigate the knowledge, attitudes, and confidence of these health professionals and explore their experiences, challenges, educational needs, and preferences in this context.
This research was conducted in the United Kingdom where perinatal care is primarily delivered by midwives as autonomous practitioners. Contrariwise, in most of the industrialized world, obstetricians lead care and midwives follow care plans and decisions made by doctors. In the United Kingdom, most health care is delivered within a National Health Service, free to all citizens, rather than by private hospitals funded by insurance. Both factors are important to consider distinctly because they may have an impact on power and hierarchy, and therefore upon how and when trans and nonbinary people feel able to engage with perinatal services.
Methods
This research was underpinned by the interpretive framework of constructivism (Ültanir 2012), where new knowledge is constructed based on people’s previous experience and daily “real-world” observations in the process of tackling problems. Pragmatic theory supports our intended structure for mixed-methods research (Halcomb and Hickman 2015), whereby both qualitative and quantitative approaches were used to enable a detailed exploration of the complex phenomena posed.
In our patient and public involvement activities, 52 percent (37/71) of those who responded to our polls indicated that this research should consist of a survey with a large sample and a narrow focus. Significantly, 82 percent (56/68) who engaged also indicated that this research should be conducted predominantly online rather than face-to-face (before COVID-19 lockdowns). Consequently, a self-administered Internet survey was launched to collect data between February and August 2020.
Participants
During our patient and public involvement activities, 44 percent of those who engaged in our online polls (32/73) indicated that participants should include perinatal staff, more than any other participant group. Thus, participants were eligible if they currently provided care during the perinatal period in the United Kingdom and were above the age of 18 years.
Procedure
Participant recruitment began after ethical approval was granted by the Ethics Department at Coventry University, UK. A recruitment flyer was shared online by the research team, the “Make Birth Better” network, and Equality Network through professional networks and social media channels. This flyer was accompanied by a hyperlink to access the survey hosted on Qualtrics software. Participants who accessed the survey were first invited to read participant information and give their consent to participate. They were then invited to complete the entire survey, which ended by signposting participants to relevant sources of support.
Measures
Quantitative data were collected in two parts. The first part measured knowledge and attitudes using the 29-item TRansgender Attitudes and kNowledge Scale (TRANS) (Kanamori 2016). In this scale, after reverse coding negatively worded items, a higher score indicated a more positive attitude toward, and increased knowledge of, issues related to trans and nonbinary people. Responses on this scale are rated on a 7-point Likert-type scale, ranging from 1 = strongly disagree to 7 = strongly agree. The highest possible total score per participant was 203. Reliability of this instrument is high with an overall alpha value of .977. The second part consisted of four questions designed to measure confidence in providing care. These broadly aligned with similar questions posed in relation to nurses’ confidence in providing care to the trans and nonbinary communities elsewhere (Du Mont et al. 2020). A 4-point Likert-type scale was used to capture responses ranging from 1 = not at all to 4 = very. A higher score indicated a higher level of confidence. The maximum total score for each participant was 16. The only demographic information collected related to professional role to ensure anonymity and encourage participation.
Qualitative data were collected via four open text questions exploring participants’ experiences, challenges, educational needs, and educational preferences in relation to providing professional care to childbearing trans and nonbinary people.
Data Analysis
Demographic and quantitative data were analyzed descriptively. The internal consistency of both the TRANS and confidence scales was measured using Cronbach’s alpha (Connelly 2011). Because this research is applied to solve a practical problem, the five steps of framework analysis were employed to make sense of the qualitative data collected (Goldsmith 2021). This analysis was led by the lead author, who first read and reread the data in pursuit of familiarization. Subsequently, the framework of analysis was identified in partnership with the wider team, under which statements were indexed before being charted and mapped into subthemes comprising statements of similar meaning. Our thematic framework drew upon a priori issues, where data were grouped under the following: experiences of providing care for childbearing trans and nonbinary people, challenges in providing care to childbearing trans and nonbinary people, educational needs, and preferred knowledge exchange activities. Final subthemes grouped under each of these were reviewed, refined, and interpreted in partnership with the wider research team iteratively via a series of reflexive discussions. To tease out latent themes, a lens rooted in a reproductive justice approach was also applied to the data. While the analysis of qualitative data was focused on identifying semantic meanings, latent meanings are also highlighted throughout.
Strengths and Limitations
A key strength of this study is that it has enabled 108 professionals to voice their experiences, challenges, and educational needs and preferences about providing care to the childbearing trans and nonbinary communities. In taking a mixed-methods approach, this study has also been able to garner quantitative insights into the knowledge, attitudes, and confidence of professionals in a U.K. context. Nevertheless, the possibility of selection bias remains due to the nature of this study design in an area of research that may attract strong opinions. The overall alpha value for survey items relating to participants’ confidence is not necessarily “high” (Taber 2018), thus limiting their reliability somewhat. Yet as a research team, we have provided a detailed account of the study context and rich descriptions in the presentation of results to enhance the transferability of findings (Shenton 2004). However, because respondents represent only a small number of midwives working in the United Kingdom, it is difficult to ascertain whether the attitudes and educational needs described here are truly representative of all U.K. midwives. Future research could usefully seek a wider diversity of participants to better reflect the global context of perinatal service delivery. This may require the pursuit of additional avenues of recruitment. Equally, as the gender of those childbearing has been a key feature in this research, future research could also usefully collect demographic data on the gender and race of perinatal staff, as their characteristics are likely to be significant as well.
Results
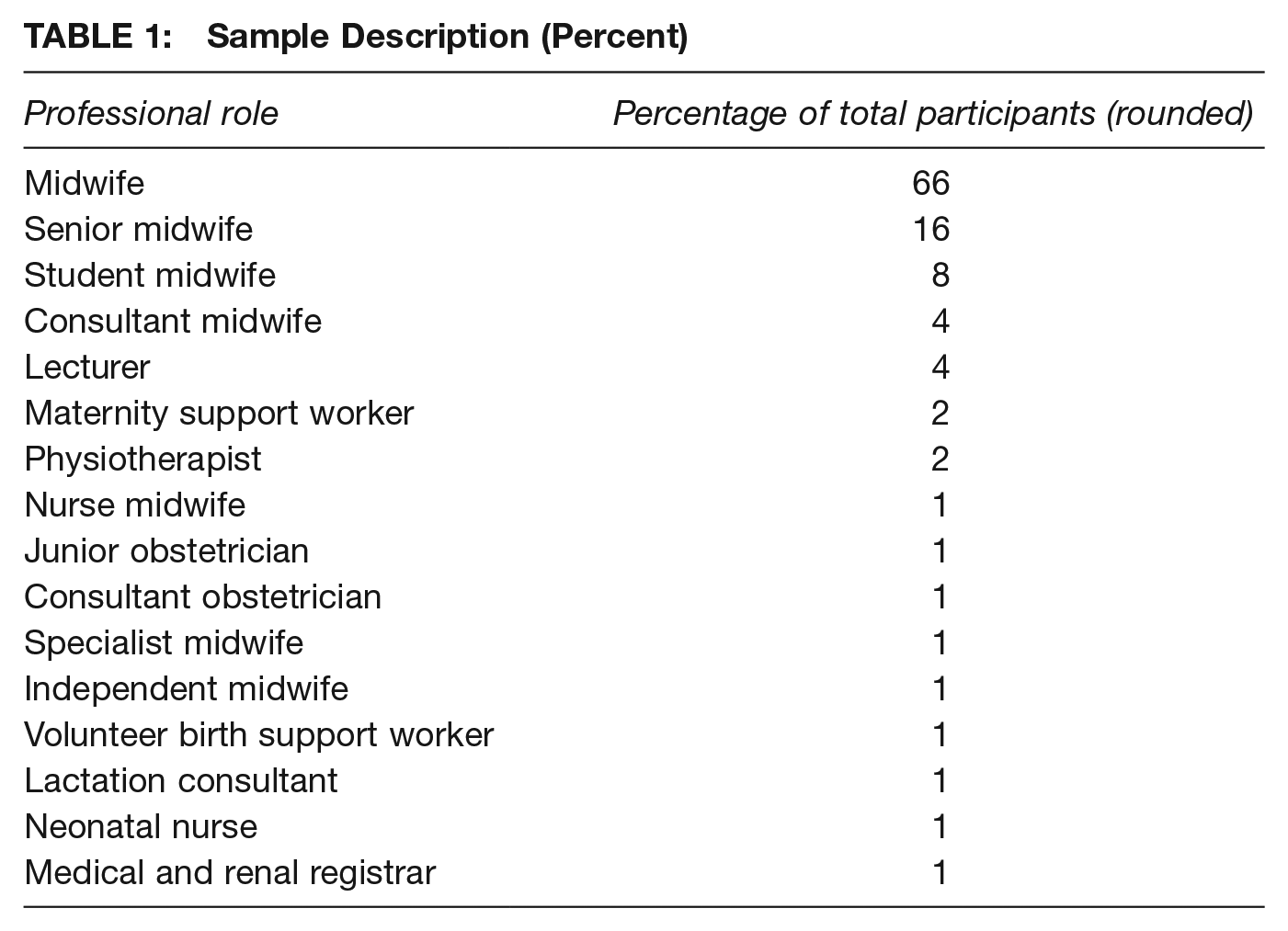
A total of 108 participants completed the survey, most of whom (66 percent) identified as midwives. Only 20 percent of the participants (n = 22) had knowingly provided perinatal care to trans and nonbinary people, whereas 80 percent of participants (n = 86) indicated they had not. The diversity of participant roles is presented in Table 1. Those childbearing in the United Kingdom do not necessarily need to engage with any other health care professional beyond a midwife, so having a sample which is primarily made up of midwives is appropriate in this context.
Sample Description (Percent)
The mean scores in relation to confidence about providing care are presented in Table 2. The highest mean score related to confidence in forming care plans in partnership with a childbearing trans or nonbinary person, whereas the lowest mean score related to confidence in feeling that colleagues would provide effective care to a childbearing trans or nonbinary person. All items related to confidence are presented separately because the overall score relates to a combination of individual question scores rather than a validated score. The alpha value for the confidence questions together represented an acceptable level of reliability, and the level of reliability for the TRANS was excellent (Cortina 1993) (Table 2). The overall mean score of the TRANS represents participants’ relatively positive attitude toward, and increased knowledge of, issues related to trans and nonbinary people. The narrow confidence interval presented in Table 2 also indicates that a high precision mean score has been generated using the TRANS (Schünemann et al. 2019).
Confidence and TRANS Scale Scores (Reported to 2 Decimal Places)
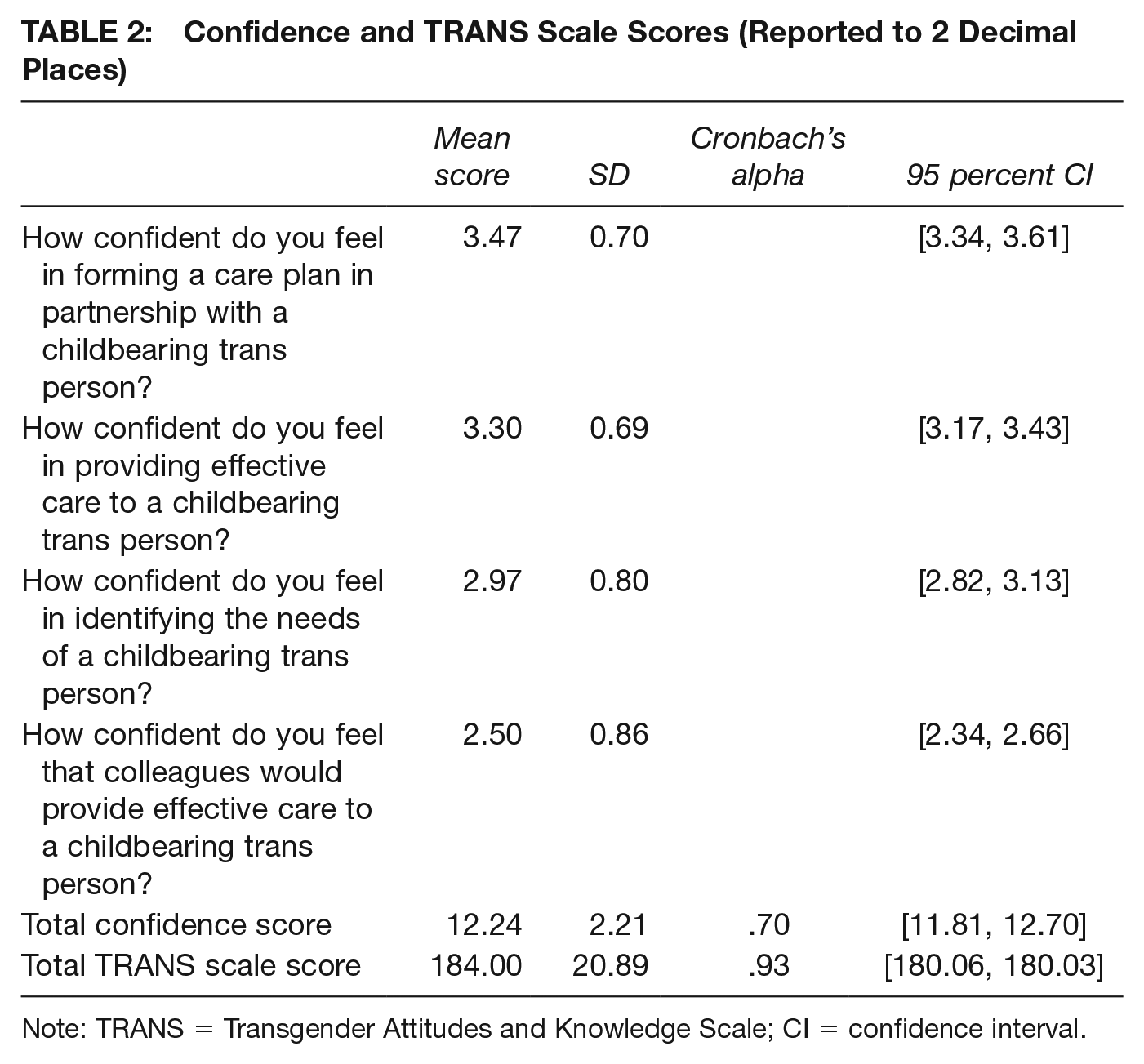
Note: TRANS = Transgender Attitudes and Knowledge Scale; CI = confidence interval.
In the qualitative analysis, 4 main themes and 12 subthemes were developed. Under the main theme of reported experiences of providing care for childbearing trans and nonbinary people, the subthemes focused on (1) recognizing individuality, (2) witnessing transphobia among colleagues, and (3) apprehension about providing care to childbearing trans and nonbinary people. Another main theme identified related to the challenges of providing care for childbearing trans and nonbinary people. Subthemes of these challenges included (1) a cisheteronormative model of care, (2) lack of awareness of trans and nonbinary issues, and (3) anti-trans and nonbinary attitudes. An important main theme was the need for education. The subthemes within educational needs focused on (1) understanding the practicalities of childbearing as a trans or nonbinary person, (2) inclusive language, and (3) how to develop policies and processes for supporting childbearing trans and nonbinary people. Finally, the last main theme that we analyzed related to respondents’ preferred method for knowledge exchange. The subthemes for gaining knowledge included (1) hearing from trans and nonbinary people, (2) sharing best practices with other professionals, and (3) open discussions about how to be inclusive.
Experiences of Providing Care for Childbearing Trans and Nonbinary People
The three subthemes identified in this main theme related to (1) recognizing individuality, (2) witnessing transphobia among colleagues, and (3) apprehension about providing care for childbearing trans and nonbinary people.
Recognizing Individuality
Participants highlighted the individual nature of cases. For instance, one participant offered contrasting examples of birthing people who identified as men, one of whom wished to be addressed by staff accordingly, while the other preferred to be referred to as “she/her”: [One] transgender person identified as male, had all his maternity documents updated accordingly and was addressed by staff in the way he preferred. . .[another] person identified as male but preferred to keep using pronouns she/her during pregnancy and her given name from birth. (Student midwife)
Participants recognized that some experiences occurred at unique time points. For instance, several respondents referred to providing care to those who were “part way through transition” (midwife) or had chosen to give birth before certain medical procedures. One case was described where a participant cared for someone “who had decided to transition to Male, ‘top but not bottom surgery’” (midwife). Such recognitions of individual circumstances are encouraging because the provision of individualized care is considered pivotal in improving childbearing experiences in this context (Lai-Boyd 2020).
Witnessing Transphobia Among Colleagues
Transphobia can diminish the trust in health care professionals required for a positive childbearing experience and add an extra layer of fear for the communities affected (Malmquist et al. 2019). Nevertheless, a number of respondents witnessed colleagues being “very prejudiced” (maternity support worker). In another case, “the midwives all made fun of his sexual orientation and gender identity. . . they also mocked him in front of him and used she/her pronouns in front of him” (student midwife). Others reported witnessing expressions of transphobia in nonclinical environments: “I haven’t provided care for anyone trans, but did witness some transphobia at [a midwifery] conference in 2018 that shocked me” (midwife).
Apprehension About Providing Care to Childbearing Trans and Nonbinary People
Some midwives expressed apprehension about providing care in this context. For instance, one participant described how they were initially very nervous that they might “slip up” and use the wrong terminology or pronouns, yet this became easier when they “saw him as an individual” (senior midwife). Another participant reflected embarrassment in assuming that a client was a male visitor: “[I] replied that he should use the visitor’s toilet, before realizing that he was a patient” (midwife). Confidence—and thus midwifery practice—may be strengthened through reflective activities on such scenarios in future.
Challenges
When participants were asked to reflect on the challenges in providing care for childbearing trans and nonbinary people, the three subthemes identified focused on a cisheteronormative model of care, lack of awareness of trans and nonbinary issues, and the anti-trans and nonbinary attitudes of their colleagues. However, one participant expressed how they did not “think there were any” [challenges], and that this issue is “dramatized” (midwife).
A Cisheteronormative Model of Care
Respondents reflected that perinatal (or “maternity care”) is structured “around a heteronormative model of care” (midwife). Essentially, the “language of ‘Mum’ and ‘Dad’, ‘husband’, ‘woman’” (midwife) is ingrained in everyday practices: Heteronormative language from staff and in notes/computer systems, legal issues with being recognised as a birthing person with non-female gender on registration and medical documents. (Lecturer)
Although several respondents specifically used the term heteronormative, what they were describing could perhaps more accurately be termed cisheteronormativity (Luxion 2020). The word heteronormativity may be used partly because participants are less familiar with the term cisgenderism or because they inadvertently conflate gender identity with sexual orientation (Ansara and Hegarty 2013). For instance, one participant highlighted that they were “aware of some lesbian couples but not transgender” (consultant midwife). Nevertheless, their awareness of heteronormativity within the services made many aware of the gendered language used in verbal and written discourse: “Gendered language is everywhere—written and conversational. Heteronormativity prevails within maternity departments” (midwife).
One senior midwife described covering with a sticky label a quotation about mothers that appeared on all handheld notes because it was not felt to be appropriate when they were working with a trans person who identified as a father. Others described how they were aware that the language used in information leaflets, online systems, and other written information may cause offense by misgendering the childbearing person or lead them to feel unsupported: “Traditionally we refer to our clients as ‘women.’ Maternity IT systems are built to only process female records. No space to document gender or pronouns” (midwife). Several respondents supported making perinatal services more inclusive of trans men and nonbinary people. One stated they had requested that language be changed in information leaflets to be more inclusive, while another reported using inclusive language such as “pregnant person” and “they/them” pronouns until they knew the person’s preferred pronouns.
Some had concerns about mixed gender accommodation, commenting that some women may find sharing a ward with trans men “disconcerting” (senior midwife). Others expressed concerns about disempowerment: “I am actually more concerned about the way that some transgender people and their supporters are trying to disempower cis women and make them invisible by using terms like ‘pregnant people,’ so I think this is very complex” (midwife). Evident within these responses was a tension between traditionally feminist constructions of “maternity services” being “woman centered” and intersectional feminist concerns for making health services more inclusive of gender-diverse childbearing people. However, respondents did not always see these as being contradictory; for example, another respondent stated “Trans rights do not undermine women’s rights . . . one can be a feminist and also provide understanding, accepting care to transgender people” (student midwife)
Ultimately, whereas some participants expressed concerns, others recognized that the removal of barriers for trans men and nonbinary people who access perinatal services does not require the construction of barriers for women.
Lack of Awareness of Trans and Nonbinary Issues
The childbearing trans and nonbinary communities require access to contextual and individualized advice and support (McCann et al. 2021). Nevertheless, many participants highlighted a lack of awareness of trans and nonbinary issues in this context: I have discussed care in pregnancy with colleagues, many of whom don’t understand simple factors such as “trans men” being those whose gender identity is male, but may have been assigned female at birth and be physiologically capable of pregnancy. (Volunteer birth support worker)
Several commented that a lack of training and resources in this area had led to a lack of awareness and understanding: [There is a] lack of inclusive resources, lack of training, lack of guidance and policies, lack of awareness about national reports from UK government and those from UK NGO relating to the LGBTQ+ population, lack of understanding about the views of healthcare professionals toward this particular group of service users. (Consultant midwife)
Respondents described how this lack of awareness can result in professionals causing harm. One respondent even described assumptions that a child born to trans or nonbinary parents requires engagement with safeguarding services: Some Trusts [healthcare organizations], mine included, wrongly safeguard children born to transgender parents and lack an ability to care for transgender and nonconforming families in a professional manner. (Midwife)
Anti-Trans and Nonbinary Attitudes
Much like when participants were asked to recount their experiences, when asked about challenges in the provision of care for the childbearing trans and nonbinary communities, our participants commonly cited the anti-trans and nonbinary attitudes of their professional colleagues. Such attitudes were frequently described as being based on conservative religious beliefs or gender-critical views. Other assumptions were often based on negative and stigmatizing stereotypes: A lot of experienced staff assume that any transgender person is going to be “difficult” or “combative” or . . . that transgender people are “deviant” or “attention-seeking” or “crazy”. (Volunteer birth support worker)
Other participants described colleagues’ biases or assumptions that the provision of individualized care negated the need for training in how to be inclusive of gender diversity: Assumptions and presuppositions, rigid thinking, and unknowing internal transphobia along with unwillingness to unlearn it. Attitudes like “we give everyone individualized care so why should I learn about trans people.” (Midwife)
In addition, some respondents reported that the attitudes of perinatal service users and their families acted as a barrier to inclusion, for instance, “complaints from other families about sharing a room with a man” (consultant midwife). Such complaints point to a need for increased societal acceptance of the trans and nonbinary communities along with gender diversity.
Educational Needs
When participants were asked about their educational needs, we identified several subthemes, including the practicalities of childbearing as a trans or nonbinary person, inclusive language, and policies and processes necessary for supporting childbearing trans and nonbinary people. Only one participant described feeling “well educated on this subject” (midwife). Another stated that they “don’t need to know” as they “treat everyone as individuals” (midwife). Such discourse adds to understandings about how “mundane cisgenderism” operates (Knott-Fayle, Peel, and Witcomb 2021) and can fail to acknowledge the need for awareness of diversity and the unique needs of this particular childbearing group.
Practicalities of Childbearing as a Trans or Nonbinary Person
Within this subtheme, participants reflected on their need to understand the practicalities involved with childbearing as a trans or nonbinary person, including impacts upon cross-sex hormone treatment, transitioning, and surgeries. Several respondents wanted to understand gender identity more broadly. Some struggled to understand why a trans man would want to experience what they saw as a “female act”: Why [a trans person] might engage in a very female act by carrying a pregnancy if it was a female who was identifying as a male. (Lecturer) How their trans status is managed while pregnant—I can’t figure out “living as a man” while pregnant/breastfeeding. (Physiotherapist)
This further highlights a cisgenderist understanding of childbearing, where it is presumed that only cisgender women will be or want to be pregnant, or that a desire to be pregnant must undermine a trans man’s sense of himself as a man.
Others expressed an interest in understanding the influences upon a trans or nonbinary person’s gender identity. This highlights potential cynicism and also identifies dominant cisheteronormative cultures that still define gender as immutable and render trans and nonbinary people unable to authenticate their own identities without question (wrongly) from the cis community (Nordmarken and Kelly 2014). Such responses also provide useful insight for addressing health care staff’s educational needs going forward.
Inclusive Language
Participants highlighted they would welcome training on how to use more inclusive language: “I would like to be able to access some workshops that could be shared with staff about the language we use” (consultant midwife). Several referred to wanting more information about what the “correct” terminology is and how to refer to parts of the childbearing trans or nonbinary person’s anatomy without causing offense: “How to approach discussion about interventions such as vaginal examinations” (senior midwife). Another noted difficulties with “terminology, referring to female sex organs by other non-gender specific names for example” (senior midwife).
One participant commented that they would appreciate training in how to approach “conversations about feeding, body image, mode of birth, and intimate examinations” (midwife). Nevertheless, another participant reflected that they “will find it hard to remember that we aren’t allowed to say they’re the mother” (student midwife). This latter comment reveals a need to understand that the use of affirming and inclusive language is not about what is “allowed,” but about ensuring that the needs of trans and nonbinary parents are met.
Policies and Processes for Supporting Childbearing Trans and Nonbinary People
Respondents expressed a desire for policies and guidelines to ensure perinatal services remain supportive of trans and nonbinary communities: What the NHS and other services’ policies are in relation to all aspects of transgender people’s care during pregnancy . . . Where and how to streamline access to other specialists who may be involved in their care. (Volunteer birth support worker)
One participant commented on the importance of having “a pathway in place so everyone provides the same standard” (midwife). Respondents also identified barriers in the legalities and processes relating to birth registration where the person who gave birth to the child identifies as a man: “registration of birth and the ability for records to be made in which the father has birthed the child” (midwife).
Some were uncertain what was legal in cases where parents question who will be documented as the “mother.” Even a midwife who was in a relationship with a trans woman was unsure how their partner would be registered on the birth certificate as a biological parent: For example, my girlfriend is trans and if we were to have a baby it would be inappropriate to have her listed as “father” on the birth certificate, but I don’t know a way around that as she will have provided sperm! (Midwife)
Preferred Knowledge Exchange Activities
When participants were asked what they may find useful in relation to educational knowledge exchange on the provision of care for childbearing trans and nonbinary people, subthemes related to hearing from trans and nonbinary people, sharing best practices, and open discussions about how to be inclusive.
Hearing From Trans and Nonbinary People
Many respondents expressed a desire to hear directly from trans and nonbinary people and engage them in “co-creating” better services: I would like to hear about transgender individuals’ personal experiences regarding maternity care and how they would have wanted it to be different/improve. (Student midwife) To hear from birthing people themselves and for them to be involved in co-creating a more effective service. (Lecturer)
Sharing Best Practice
Respondents expressed a desire for the sharing of good practice within the perinatal care community. For instance, one midwife suggested that they would like to see greater exchanges of “case studies, guidance, and policies” (midwife). One respondent called for more “research to support actions and discussions” (midwife), in recognition of evidence-based recommendations and practices. In line with earlier findings about a general lack of awareness, several respondents called for more staff training that could disseminate best practice along with “basic visual explanations about what relevant words mean” (midwife).
Open Discussions About How to Be Inclusive
Respondents recognized that there was a need for the matter of inclusive care to be openly discussed and addressed, although there was not always consensus regarding what that should look like in practice. Some expressed a desire to see a strong position from service providers in support of inclusion and against discrimination: The thing I would find most useful is a clear and decisive statement from all stakeholders that care that isn’t inclusive is totally unacceptable. There is no place in a professional role for cutting people slack because they are prejudiced, and they just cannot help it. A decisive stance is essential for making progress. (Midwife)
Others expressed concern about the removal of gendered language (e.g., “woman”) within services used by an overwhelming majority of cisgender women. For example, one respondent said they would “rail against ‘birthing parent’ being used as standard” (consultant midwife). Another stated, “[I] would not like to see the term ‘woman’ stopped from being used in maternity services and replaced with person . . . as both a woman and midwife” (senior midwife).
Whereas many respondents supported the idea of being inclusive of childbearing trans and nonbinary people, a minority expressed reservations based on the notion that inclusion might come at the expense of affirming cisgender women’s own identity: “Female voices are being excluded while decisions are being made that materially affect all female people” (medical and renal registrar).
Positing that inclusive language erases (cisgender) women arguably fails to acknowledge the pervasive marginalization of gender-diverse people and (by comparison) the privileges conferred by being a cisgender perinatal service user. This further contributes to understandings of how “mundane cisgenderism” may operate in perinatal services and beyond (Knott-Fayle, Peel, and Witcomb 2021). Overall, there was consensus in the need to be inclusive in this context, which may serve as a useful platform for respectful future discussions.
Discussion
In this article, we make contributions in relation to the educational needs and preferences of 108 U.K. health care professionals who provided care during the perinatal period. Our findings provide nuanced understandings of professional knowledge, attitudes, and experiences, along with professional confidence and challenges in providing care in this context. We used patient and public involvement activities to effectively engage a larger number of voices in shaping the design and direction of this research. In line with the majority of contemporary Britons (Tryl et al. 2022), participants were highly trans and nonbinary positive. Nevertheless, our findings highlight the ways in which childbearing trans and nonbinary communities are marginalized in perinatal services along with the transphobic, anti-trans, and nonbinary attitudes that remain apparent.
This study occurs within a geopolitical Western context in which some conservatives are attempting to police the category “female” (Sharrow 2021), as an oppressive force fuelling anti-trans rhetoric (Hsu 2022). We argue that a focus on the sexed body is bound up in the medicalization of both women’s bodies, childbirth and trans identities whereby trans people who seek perinatal care can be cast under suspicion as not being truly what they claim to be (Gill-Peterson 2014; Thomas 2021). The fecund body has similarly “been socially gendered as unquestioningly feminine because of its association with female-bodied people” (Ryan 2013, 119). As feminist struggle has produced “woman-centered” approaches to childbirth, our findings of cisheteronormative models of care show that such “successes” have oppressive outcomes for trans and nonbinary people. As the idea of reproductive labor has historically been inextricably linked to gendered divisions and their central role in perpetuating women’s subordination (Duffy 2007), such entrenched approaches to childbearing serve to both reflect and reinforce the patriarchal systems in which (cis) “women” have arguably been the forced and sole reproducers of the human species (Rich 1980; Wittig 1980).
Our findings are congruent with the minority stress model, in which individuals of minority groups are exposed to stressors that dominant groups are not (Meyer 1995). We find discussion of microaggressions by our caregiver participants that are similar to those associated with minority stress exposure. These microaggressions described by the midwives occur whilst childbearing trans and nonbinary people are receiving perinatal care. Such microaggressions are also seen elsewhere in health care and include the endorsement of binary gender norms, exoticization, mocking, questioning, awkwardness, avoidance, assumptions of sexual pathology, and the denial of individual needs including the use of incorrect pronouns or misgendering (Nadal, Skolnik, and Wong 2012; Nordmarken and Kelly 2014). If midwives misgender as some of them discuss, this could trigger microaggressions and victimization by exposing private information, exacerbate stress, and invalidate the experiences of those childbearing who identify differently, or as neither a “man” nor a “woman” (Nordmarken and Kelly 2014). In this sense, trans and nonbinary perinatal service users are effectively punished, dehumanized, and humiliated by the very people who have the power to provide or deny them health care. The anti-trans and nonbinary attitudes of providers and the transphobia witnessed here by participants and their colleagues further highlight the minority stress the trans and nonbinary communities are exposed to. Such stress has the potential to adversely affect their health (Hendricks and Testa 2012). Our findings build upon the concept of stigma visibility (Miller and Grollman 2015), as the childbearing trans men referred to by participants were viewed as holding a discredited and stigmatized status. In this context, secondary stigma visibility may also be apparent should a pregnancy lead to one’s trans status being more visible rather than concealable in this context.
Gender nonconformity (i.e., not conforming to the gender behaviors, attitudes, values, and actions that society expects of men and women) is used to signify that one’s gender expression breaks the societal and cultural expectations of “doing gender” (West and Zimmerman 1987) in a normative way. Such nonconformity also serves as a further form of stigma visibility, as trans people who are more frequently “read” as trans or gender nonconforming can experience increased discrimination and poorer health outcomes (Miller and Grollman 2015). Our findings add to the understandings and extend important debates around the “doing,” “undoing,” and arguably “re-doing” of gender (Butler 2004; Deutsch 2007; Risman, Lorber, and Sherwood 2012; West and Zimmerman 2009). For example, some of our participants were left perplexed as to why a trans man might engage in what they viewed as the “very female act” of childbearing. This is significant because trans and nonbinary people who live full time in their experienced gender and those who have received surgical treatment report the most transphobic discrimination (Miller and Grollman 2015). Therefore, future research could usefully explore how childbearing in the trans and nonbinary communities is perceived in relation to gender (non)conformity and the ways in which it may or may not be protective.
Discrimination can extend all the way to eugenics. Dunne’s (2017) analysis determined that 20 countries across Europe continued to enforce a sterilization requirement as a precondition for legal gender recognition, despite the weak intellectual and evidential basis for it. Such sterilization has been an expected step in the gender-affirming process where masculine gender identity and pregnancy were regarded as incompatible, as in Sweden (Falck et al. 2021). Although sterilization has never been a legal requirement for U.K. trans people, and the clinical evidence for recommendation is similarly weak, hysterectomy and salpingo-oophorectomy have still been strongly encouraged while pregnancy in these populations remained unthinkable to the medical establishment (Toze 2018). Elsewhere, trans people have been rejected by fertility clinics (Charter et al. 2018), further illustrating their exclusion from assisted reproduction. Our findings contribute to this by suggesting a kind of “passive eugenics” (Bowman 1996) where some participants demonstrated aversion to trans men and nonbinary people childbearing. Although our findings have focused predominantly on trans men and nonbinary birthing people, some participants suggested that several health care providers perceive being trans or nonbinary as being incompatible with parenthood more generally. Evidence for this is that one participant suggested that a child born to trans or nonbinary parents automatically requires engagement with safeguarding services.
As Radi (2020) observes, in a cultural framework where the articulation between medicine and justice is committed to both sexual difference and the gender binary, trans and nonbinary people and reproduction are essentially presented as mutually exclusive. Thus, the trans and nonbinary communities are effectively forced to choose between embracing their core human rights to gender identity and their sexual and reproductive health. Our findings show that data systems were rendered ineffective to identify a birthing parent as a “father.” Such reproductive injustices may be overcome via the theoretical assertions of the intersectionality approach within a reproductive justice framework by not relying solely upon “women’s” identity in defining rights and shaping political movements (Crenshaw 1989; Morison 2021). This approach would not only provide an intellectual shift to counter the impact of heteropatriarchal systems our findings describe in perinatal services but also enable the needs of everyone involved to be attended to and ensure that a more realistic approach is adopted to understand the complex phenomena we are dealing with.
The narrow gender norms, gender binary, and cisnormative assumptions in perinatal services we have documented in our findings are concerning because they can be associated with medical risks (Falck et al. 2021) and misdiagnosis (Stroumsa et al. 2019). In wider health care, cisgender system barriers may also be imposed by medical records systems and generalized rules that cancel or improperly flag results based on gender/sex binaries (Goldstein, Corneil, and Greene 2017). Consequently, trans and nonbinary people can miss relevant screening and, likewise, serious diagnoses (O’Hanlan, Gordon, and Sullivan 2018). Future medical record systems will need to recognize that trans and nonbinary people exist, to be individualized, and to remain consistent with preventive health screening standards relevant to the organs in situ. Perinatal services may usefully consider that their systems now also need to be able to reflect the diversity and reality of service user experiences, such as being able to record pregnancy on all medical records.
Historically, the trans and nonbinary communities have experienced cisgenderist and systemic exclusion from health care policies, which has led to distrust, lack of information, or misinformation. This has contributed to recent COVID-19 vaccine hesitancy and a lack of robust data to guide interventions and policy changes (Garg et al. 2021). Nevertheless, participants here expressed a need to be guided by policy and evidence-based approaches. Dolan et al. (2020) have similarly recommended that professionals should have access to relevant evidence-based guidelines and referral pathways. Such trainings may usefully be informed by further research and cocreated in partnership with those from trans and nonbinary communities, working to build trust in these areas.
Our findings explore the perspectives of perinatal staff and highlight how trans men and nonbinary people who decide to reproduce do so within services designed to exclude them. The discrimination apportioned to birthing trans and nonbinary people referred to in our findings is also consistent with assertions by West and Zimmerman (2009) that penalizing accountability structures remain for those who defy the “essential natures” of a woman or a man. Overall, our findings suggest that childbearing trans and nonbinary people are clashing with “woman centred,” heteronormative, cisgender, and heteropatriarchal perinatal services. Yet the particular suggestion that some childbearing women may find sharing a ward with trans men “disconcerting” presents trans men as the problem, rather than the systems in which they are marginalized and left without accommodation. Given our findings, we suggest it is trans and nonbinary people who may require additional protections in this context, given that they experience disproportionate rates of violence, victimization, and distal stress relating to depression and suicidality when compared with their cisgender peers (Pellicane and Ciesla 2022). Moving forward, it will be important to respect and integrate a range of identities in perinatal services and avoid segregation where trans and nonbinary people simply may not fit.
Conclusion
Cisnormative, heteronormative, cisgender, and heteropatriarchal services, administrative procedures, structural forces, and interpersonal treatment combine in the perinatal space. In this study, we provide evidence that such institutionalized “support” is designed to reinforce a gendered experience of pregnancy and childbirth that marginalizes childbearing trans and nonbinary people who do not conform to cisgender ideals. This study also offers important insights as to how providers’ stances inform mundane cisgenderism, passive eugenics, stigma visibility, the minority stress model, and the “doing” and “undoing” of gender.
Health care providers may usefully reflect on whether their service provision could be more identity affirming for the trans and nonbinary communities they serve. Professional trans and nonbinary competent education is needed, and reproductive health services and systems must be more inclusive of trans bodies and identities. Thus, future professionals, systems, and services must be prepared for a new and more inclusive (rather than exclusive) reality.
Footnotes
Author’s Note:
We acknowledge and thank those who participated in this research and also the Scottish Trans Alliance and Equality Network for acting as our learned partners in this work. Thank you also to the Make Birth Better network and the anonymous peer reviewers of Gender & Society, whose feedback enabled the enrichment of this article.
Sally Pezaro is a registered midwife, an adjunct associate professor at the university of Notre Dame in Australia, an assistant professor within the Centre for Healthcare Research at Coventry University in the United Kingdom, a fellow of the Royal College of Midwives, and an editorial board member of Evidence Based Midwifery, MIDIRS, and the International Journal of Childbirth. She is also a panelist on the Nursing and Midwifery Council’s fitness to practice Investigating Committee and a senior fellow of the Higher Education Academy. In 2021, she won a “Midwives Award” from the Iolanthe Midwifery Trust and a “Partnership Working” award from the Royal College of Midwives. In 2019, she was honored with a first prize award from the Royal Society of Medicine in “Leading and inspiring excellence in maternity care” and was also the first runner-up for the British Journal of Midwifery’s “Midwife of the Year” 2019.
Rebecca Crowther is the Policy Coordinator for Equality Network, a leading national charity working for lesbian, gay, bisexual, transgender, and intersex equality and human rights in Scotland. She leads on policy work in health, mental health, hate crime, ending conversion practices, kinship, and I/VSC equality. She is also a social researcher specializing in wellbeing, group dynamics, and space.
Gemma Pearce is an associate professor across the Centre for Healthcare Research and the School of Psychological, Social and Behavioural Sciences at Coventry University, UK. She is a chartered psychologist with the British Psychological Society and senior fellow of the Higher Education Academy. Her research specializes in women’s health, health care services, and cocreation methods, with a cocreation framework embedded across research and practice internationally, including National Health Service (NHS) England. She was part of the previous research project on hypermobile Ehlers–Danlos syndrome and pregnancy, where through public involvement, the need to develop research in this field of perinatal care for trans and nonbinary people arose. She received an award in 2018 by Emerald Publishing for impactful research making a difference to patients, public, and health care professionals.
Adam Jowett is associate head of the School of Psychological, Social and Behavioural Sciences at Coventry University. His research interests include LGBT+ (lesbian, gay, bisexual, transgender, and other) health and anti-LGBT+ prejudice and stigma. He is Chair of the British Psychological Society’s Sexualities Section, which promotes psychological work relevant to LGBT+ issues.
Laura Godfrey-Isaacs is an artist, midwife, creative producer, and birth activist. She aspires to bring her knowledge and experience in the arts together with midwifery to bring fresh interdisciplinary perspectives to inform birth education, practice, policy, and research. She regularly presents at conferences, writes, and blogs about birth and creates interdisciplinary projects and campaigns, such as Maternal Journal, which supports mental health and wellbeing through creative journaling, and Birth Café, an inclusive space to talk about the significance of birth for all. She is ambassador for Proceate Projects, Co-Chair of the Women’s Equality Party’s Health Committee, Board Advisor of the International Forum for Wellbeing in Pregnancy, and was member of the Thought Leadership Group at the NMC reviewing midwifery education standards.
Isaac Samuels is an established community campaigner and coproduction advisor. They has worked for 25 years within the health, social care, and housing sectors supporting those at risk of disadvantage due to social, political, and environmental barriers such as poverty, health, and/or disability, to live their best lives. They does this by supporting people to share their lived experience to shape policy and their desired life outcomes irrespective of the systematic barriers they may face. They has lived experience of their own inequalities associated with their own health and social care support needs. They is passionate about supporting others to overcome these particular barriers. Issac’s lived experience of the effects of life-changing health conditions has shaped their knowledge and approach.
Vic Valentine is the Manager of Scottish Trans, the trans-specific project of the Scottish LGBTI (lesbian, gay, bisexual, transgender, and intersex) equality and human rights charity Equality Network. Scottish Trans works to improve the equality, inclusion, and human rights of trans people across Scotland.