
Abstract
Objectives:
This study examined the effect of breastfeeding education using the motivational interviewing technique on breastfeeding motivation, self-efficacy, and mother–infant bonding in mothers who gave birth vaginally.
Methods:
This randomized, controlled trial included 80 primiparous mothers. The experimental group received breastfeeding education with the motivational interviewing technique at four time points. Data were collected using Maternal Descriptive Information Form (MDIF), the Primiparous Breastfeeding Motivation Scale (PBMS), the Breastfeeding Self-Efficacy Scale (BSES), the Mother–Infant Bonding Scale (MIBS), and the Motivational Interviewing Importance and Confidence-Efficacy Rating Scale. Data were collected at three time points: immediately before training (pretest), 15 days following completion of the training (post-test), and 4 weeks thereafter (follow-up). Data were evaluated using Student’s t test, Mann–Whitney U test, analysis of variance, Friedman variance test, and intention-to-treat analysis.
Results:
In the post-test and follow-up evaluations, the experimental group had significantly higher mean scores than the control group in the “Value ascribed to breastfeeding” (p < 0.001 and p = 0.004, respectively) and “Midwife support” (p < 0.001 and p = 0.003, respectively) subdimensions of the PBMS as well as in “Motivational interviewing importance” (p < 0.005) and “Confidence-efficacy rating scale” (p < 0.001). During the follow-up period, the experimental group also showed significantly higher scores in the “Self-efficacy” subdimension (p < 0.001) and total mean scores of the BSES (p = 0.033) and MIBS (p = 0.002) than the control group. However, the “Expectation of success” subdimension score of the PBMS was not significant (p > 0.05).
Conclusion:
Breastfeeding education using the motivational interviewing technique enhances breastfeeding motivation (including values ascribed to breastfeeding, self-efficacy, and midwife support), breastfeeding self-efficacy, mother–infant bonding, and the importance and confidence-efficacy levels in breastfeeding.
Introduction
The World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) recommend that infants be exclusively breastfed for the first 6 months of life, followed by continued breastfeeding for up to 2 years or longer with appropriate complementary foods (WHO, 2023). According to the Global Breastfeeding Scorecard, 46% of infants are breastfed within the first hour after birth, and 48% are exclusively breastfed during the first 6 months of life (WHO, 2024). Data from the Turkey Population and Health Survey 2018 revealed that the exclusive breastfeeding rate for infants under 6 months of age is 41%, with a median exclusive breastfeeding duration of 1.8 months. Additionally, 71% of infants were breastfed within the first hour after birth (Hacettepe University Institute of Population Studies, 2023). The timing of initial breastfeeding, the exclusive breastfeeding rate during the first 6 months, and the overall breastfeeding continuity fall short of the recommended targets (Hacettepe University Institute of Population Studies, 2023).
During the breastfeeding process, mothers may encounter various challenges, including a lack of knowledge about breastfeeding, low motivation and self-efficacy, and psychosocial factors (Whittaker et al., 2025). Primiparous mothers may experience high stress and anxiety due to postpartum uncertainties and difficulties related to breastfeeding and infant care, resulting in a negative impact on maternal psychosocial well-being and contributing to problems in initiating and maintaining breastfeeding (Palancı Ay & Aktaş, 2024a). Furthermore, breastfeeding difficulties can adversely affect maternal functioning and parental self-efficacy, potentially leading to disruptions in mother–infant bonding (Davis & Sclafani, 2022). Healthcare professionals, particularly nurses and midwives responsible for postnatal care, play a crucial role in preventing and addressing these breastfeeding-related challenges (Chipojola et al., 2020; Shipton et al., 2023).
Among the modifiable factors influencing breastfeeding success, maternal motivation is particularly significant (Zhao et al., 2024). Breastfeeding motivation encompasses internal and external factors that shape a mother’s willingness and determination to breastfeed her infant (Carrasco-López et al., 2025). Breastfeeding motivation directly affects a mother’s initiation, continuation, and determination to sustain breastfeeding (Mizrak Sahin et al., 2019; Stockdale et al., 2011). Mothers with high motivation levels are more likely to persist with breastfeeding despite challenges. Therefore, enhancing maternal motivation is a critical factor in promoting breastfeeding continuity and success (Cangöl & Şahin, 2017). Breastfeeding motivation is influenced by various individual and environmental factors (Kestler-Peleg et al., 2015; Martin et al., 2022). Among these, one of the most significant factors affecting a mother’s approach to breastfeeding, as well as breastfeeding duration and continuity, is her perception of breastfeeding self-efficacy (Aluş Tokat & Okumuş, 2013). Breastfeeding self-efficacy refers to a mother’s perceived ability and efficacy to breastfeed her infant (Dennis, 2003). Mothers with low breastfeeding self-efficacy may be more likely to discontinue breastfeeding prematurely (Aluş Tokat & Okumuş, 2013; Mizrak Sahin et al., 2019). Breastfeeding self-efficacy and maternal motivation significantly influence mother–infant bonding. Therefore, providing timely support for breastfeeding immediately after birth is essential for strengthening this bond (Kheirandish et al., 2026).
Breastfeeding education programs to enhance maternal self-efficacy and motivation play a crucial role in empowering mothers, fostering confidence, and addressing individual needs throughout the breastfeeding process (Franco-Antonio et al., 2021). Nurses assume critical roles as educators and consultants in promoting positive attitudes and behaviors related to breastfeeding as well as in supporting breastfeeding initiation and continuation (de Sousa et al., 2025). One effective approach nurses can use in breastfeeding education is the motivational interviewing (MI) technique.
MI is a patient-centered, directive counseling method to resolve ambivalence, strengthen motivation, and facilitate behavioral change (Miller & Moyers, 2006). MI activates an individual’s intrinsic motivation for change and promotes active participation (Miller & Rollnick, 2013). MI plays a supportive role in helping mothers adapt to the breastfeeding process by addressing their knowledge gaps, concerns, and lack of confidence; enhancing intrinsic motivation; and facilitating behavioral change when necessary, ultimately promoting breastfeeding continuation (Bekmezci & Meram, 2025; Palancı Ay & Aktaş, 2024b). Some mothers experience both physical and emotional challenges during breastfeeding, with primiparous mothers often facing greater difficulty in effectively coping with these challenges (Whittaker et al., 2025). MI is a valuable technique for enhancing mothers’ ability to manage these difficulties (de Sousa et al., 2025).
Despite the potential benefits of MI in breastfeeding education, a limited number of studies in the literature explore its application in this context (Bekmezci & Meram, 2025; Cangöl & Şahin, 2017; Franco-Antonio et al., 2021; Naroee et al., 2020; Zunza et al., 2023). Some of these studies have been conducted during pregnancy, whereas others have focused on the postpartum period. However, postpartum mothers—especially primiparous mothers—require greater support from healthcare professionals regarding breastfeeding and infant care (Cangöl & Şahin, 2017; Ertem &Aktaş, 2025; Naroee et al., 2020; Zunza et al., 2023).
This study aimed to investigate the effect of breastfeeding education, delivered using the MI technique, on breastfeeding motivation, self-efficacy, and mother–infant bonding among primiparous mothers who gave birth vaginally. Existing evidence has revealed a paucity of randomized, controlled trials examining breastfeeding education based on MI techniques (Bekmezci & Meram, 2025; Cangöl & Şahin, 2017; Kheirandish et al., 2026; Naroee et al., 2020; Zunza et al., 2023). This study is distinguished by three key features. First, it focuses exclusively on primiparous mothers who gave birth vaginally. Second, the MI-based breastfeeding education provided had an average total duration of 3 hours, with sessions strategically scheduled according to postpartum care follow-up frequency. Third, the effectiveness of the education was assessed using a post-test and follow-up test incorporating five key variables (i.e., breastfeeding motivation, breastfeeding self-efficacy, mother–infant bonding, the importance ascribed to breastfeeding, and confidence efficacy in breastfeeding). Given these distinct methodologic features, the study is expected to fill a critical gap in the literature and provide a foundation for future research on MI-based breastfeeding education interventions. In this study, breastfeeding education based on the MI technique, delivered by a nurse, can enhance the quality of postpartum care while promoting maternal and newborn health. The WHO emphasizes that breastfeeding support should be provided by experienced and trained nurses and midwives and continue throughout the postpartum period, involving direct, face-to-face communication (Öcalan et al., 2024; WHO, 2024). This study directly aligns with and contributes to these WHO recommendations.
The hypotheses of this study are as follows:
Key Messages
• Evidence on the use of motivational interviewing in breastfeeding education is limited.
• This randomized, controlled trial showed that the technique significantly improved breastfeeding motivation, self-efficacy, and mother–infant attachment compared with standard care.
• The findings highlight motivational interviewing as an effective approach to strengthening breastfeeding-related psychosocial outcomes in primiparous mothers.
Methods
Study Design
This randomized, controlled trial investigated the effects of IM-based breastfeeding education for mothers following vaginal birth on breastfeeding motivation, self-efficacy, and mother–infant bonding. The study is registered at https://clinicaltrials.gov/ under the No. NCT06313034.
Setting and Participants
The study was conducted in the maternity unit of a hospital in northeastern Turkey between May 2023 and March 2024. Obstetricians and midwives provide care in the maternity unit, where all rooms are single occupancy. Women admitted for childbirth remain in the same room throughout birth and the immediate postpartum period. Breastfeeding support is initiated by midwives immediately after birth. The maternity unit recorded 256 vaginal births in the preceding year. The study sample comprised mothers who delivered vaginally at this hospital, met the inclusion criteria, and provided informed consent. Sample size was determined through a priori power analysis using G*Power 3.1.9.2 software (Heinrich Heine University Düsseldorf, Düsseldorf, Germany). Based on the study by Franco-Antonio et al. (2021), the minimum total sample size was set at 80 (40 per group) using a one-way independent-sample t test with a 95% confidence interval, 80% power, and an effect size of d = 0.565 (Franco-Antonio et al., 2021). To account for potential data loss, 86 mothers (43 per group) were included in the study. Following the pretest, three participants in the experimental group were withdrawn: one due to nonattendance at the second breastfeeding education session and voluntary withdrawal and two because their infants were admitted to the neonatal intensive care unit. In the control group, three participants were excluded because of neonatal intensive care unit admission (n = 1) or loss to follow-up after the education period (n = 2). The study was completed with 40 mothers in the experimental group and 40 in the control group.
The inclusion criteria for mothers were being ≥ 20 years of age, primiparous, at least a primary school graduate, fluent in Turkish, having no conditions impairing communication, and having no major medical breast problems that could interfere with breastfeeding (e.g., deeply inverted nipples or undiagnosed breast mass). The inclusion criteria for infants were term birth (≥37 weeks of gestation), birth weight ≥2,500 g, and no congenital anomalies affecting breastfeeding (e.g., cleft palate or cleft lip).
The exclusion criteria for mothers were having a medical condition that prevents breastfeeding (e.g., HIV-positive status or active tuberculosis), a diagnosed psychiatric disorder, or giving birth to two or more live newborns in the current birth. For infants, the exclusion criterion was being identified as risky in newborn screening programs (e.g., diagnosed with phenylketonuria).
Randomization
Randomization was performed by an independent statistician using a simple randomization approach. Participant allocation to the experimental and control groups was generated via a computer-based system (www.randomizer.org), consistent with recommendations for randomized, controlled trials to ensure allocation concealment and minimize selection bias (EQUATOR Network, 2010; Schulz et al., 2010). A randomization list was prepared, and eligible mothers were assigned to study groups accordingly. To maintain allocation concealment, the sequence was placed in sequentially numbered, sealed, opaque envelopes. After eligibility confirmation and completion of baseline assessments, the envelopes were opened by an independent individual on participants’ admission to the maternity unit. During the recruitment period, 108 mothers were assessed for eligibility. Of these, 86 met the inclusion criteria and were randomly allocated to the experimental group (n = 43) or the control group (n = 43; Figure 1).

CONSORT flow diagram.
Blinding of participants was not feasible due to the nature of the intervention. The experimental and control groups were established concurrently within the same clinical setting. To minimize contamination, MI-based breastfeeding education was delivered individually in the mother’s room during the final 4 hours before hospital discharge (20–24 hours postpartum). The control group received routine postpartum care provided by the national health system (e.g., instruction on breastfeeding positions, nipple assessment, monitoring of vaginal bleeding, and fundal examination). The study was conducted in accordance with CONSORT reporting guidelines (see Figure 1).
Data-Collection Tools
Data for this study were collected using the following instruments: the Maternal Descriptive Information Form (MDIF), the Primiparous Breastfeeding Motivation Scale (PBMS), the Breastfeeding Self-Efficacy Scale (BSES), the Mother–Infant Bonding Scale (MIBS), and the Motivational Interviewing Importance and Trust-Efficacy Rating Scale.
Maternal Descriptive Information Form
The MDIF was developed by the researcher based on the current literature and gathers information about sociodemographic characteristics (e.g., maternal age and education level), obstetric history (e.g., number of pregnancies and mode of birth), newborn characteristics (e.g., birth weight and Apgar score), and breastfeeding-related details (e.g., time of first breastfeeding after birth, duration of breastfeeding, and individual assisting with first breastfeeding) (Aluş Tokat & Okumuş, 2013; Çerçer & Nazik, 2023; Chipojola et al., 2020; Mizrak Sahin et al., 2019; Naroee et al., 2020).
Primipara Breastfeeding Motivation Scale
The PBMS was developed by Stockdale et al. (2011). The Turkish validity and reliability study of the scale was conducted by Akçay and Bal (Akçay & Demirgöz Bal, 2020; Stockdale et al., 2011). The scale consists of 29 items measured on a 7-point Likert scale and includes four subdimensions: “Value ascribed to breastfeeding,” “Self-efficacy,” “Midwife support,” ad “Expectation of success.” The scale does not yield a total score; instead, higher scores in each subdimension indicate greater breastfeeding motivation in that respective area. In the Turkish adaptation, Cronbach’s alpha values for the subdimensions ranged from 0.68 to 0.88 (Akçay & Demirgöz Bal, 2020). In this study, Cronbach’s alpha values were calculated separately for the pretest, post-test, and follow-up assessments, ranging from 0.60 to 0.91.
Breastfeeding Self-Efficacy Scale
The BSES was developed by Dennis (1999) as a 33-item instrument. In 2003, Dennis revised the scale, reducing it to 14 items to create the Breastfeeding Self-Efficacy Scale–Short Form (BSES-SF) (Dennis, 2003). The Turkish validity and reliability study of the scale was conducted by Aluş Tokat et al. (2010). The scale consists of 14 items rated on a 5-point Likert scale. A high score on the scale indicates greater breastfeeding self-efficacy. In the Turkish adaptation, Cronbach’s alpha was reported as 0.86. In this study, Cronbach’s alpha values were assessed separately for the pretest, post-test, and follow-up tests, ranging between 0.80 and 0.86.
Mother–Infant Bonding Scale
Developed by Taylor et al. (2005), the MIBS scale was adapted into Turkish by Aydemir Karakulak and Alparslan (2016). It consists of eight items rated on a 4-point Likert scale (0–3). Items 1, 4, and 6 assess positive emotional expressions toward bonding, scored from 0 to 3, whereas items 2, 3, 5, 7, and 8 measure negative emotional expressions, scored in reverse from 3 to 0. The total score ranges from 0 to 24, with higher scores indicating greater bonding difficulties between mother and infant. The Turkish adaptation reported Cronbach’s alpha values of 0.69 within 1 day postpartum and 0.68 at 8–12 weeks postpartum (Aydemir Karakulak & Alparslan, 2016). In this study, Cronbach’s alpha value of the scale was evaluated separately in the pretest, post-test, and follow-up tests, ranging between 0.51 and 0.57.
Motivational Interviewing Importance and Confidence-Efficacy Rating Ruler
The Motivational Interviewing Importance and Confidence-Efficacy Rating Ruler is one of the fundamental parameters of MI. This scale assesses the average scores of two dimensions: “Importance” and “Confidence/efficacy” (Cangöl & Şahin, 2017; Ögel, 2009). The importance scale ranges from 0 to 10 points, where 0 indicates “Not at all important” and 10 indicates “Very important.” Similarly, the confidence-efficacy ruler is evaluated on a 0–10 scale, with 0 representing “I do not trust at all/I am not efficient” and 10 representing “I trust a lot/I am very efficient” (Ögel & Şimşek, 2021).
Study Initiative: Breastfeeding Education Using MI Technique
Mothers in the experimental group received breastfeeding education delivered by the researcher using the MI technique in four individual, face-to-face sessions. Each MI session lasted ~30–40 minutes. The sessions were planned following the Turkish Ministry of Health Postpartum Care Management Guidelines (2018), which recommend specific postpartum follow-up intervals (Republic of Turkey Ministry of Health, General Directorate of Public Health, 2018b). The first session took place in the hospital’s birth unit (between postpartum 20 and 24 hours) before discharge. The remaining three sessions were scheduled based on recommended follow-up periods and were conducted in the breastfeeding room of the Family Health Center on days 2–5, 13–17, and 30–42 postpartum. The breastfeeding room was equipped with a chair for the mother, a changing table, a privacy curtain or partition, and a sink.
Breastfeeding education through MI was developed based on the Turkish Ministry of Health Breastfeeding Counseling Practitioner’s Book (Republic of Turkey Ministry of Health, General Directorate of Public Health, 2018a). The core education topics included the importance and characteristics of breast milk, breast milk characteristics, benefits of breastfeeding for the mother and baby, breastfeeding techniques, breastfeeding positions, duration and frequency of breastfeeding, signs of effective breastfeeding, indicators of adequate milk intake, hand and pump expression of breast milk, storage and feeding of expressed milk, newborn stomach capacity and hunger cues, breastfeeding and bonding, nipple pain, and solutions for cracked nipples.
The basic principles of MI (i.e., demonstrating empathy, identifying contradictions, resolving resistance, and supporting self-efficacy) were integrated into every breastfeeding education session using MI techniques (such as open-ended questioning, supportive communication, reflective listening, and summarization). To enhance the hands-on learning experience, breast and baby models were used during the education process. The breastfeeding education program with the MI technique is shown in Table 1. Three academic experts with experience in MI for breastfeeding evaluated the four-session curriculum. For this training program in our study. Each session title was rated on a 4-point Likert scale (1 = not appropriate, 2 = somewhat appropriate/needs revision, 3 = appropriate with minor revision, 4 = completely appropriate). Ratings of 3 or higher were considered acceptable. The Davis Content Validity Index (I-CVI) was calculated based on the proportion of acceptable items (L. L. Davis, 1992). The overall content validity of the training program was 0.89, indicating a high level of content validity.
Breastfeeding Education Plan Given with Motivational Interviewing Technique.

Mothers in the control group received routine breastfeeding education before hospital discharge following the Turkish Ministry of Health protocol and postnatal care services according to the standard follow-up schedule (four visits in total on postpartum days 2–5, 13–17, and 30–42) (Republic of Turkey Ministry of Health, General Directorate of Public Health, 2018b). Routine breastfeeding education comprised standard information on the benefits of breastfeeding and breast milk for maternal and infant health, breastfeeding positions, nipple assessment, and common breastfeeding problems. This education was delivered face-to-face by a midwife in the birth unit and lasted ~15–20 minutes. During follow-up visits, the health status of the mother and newborn was evaluated, the breastfeeding process and potential breastfeeding problems were reviewed, and routine counseling was provided. No structured MI-based training was administered to mothers in the control group.
Data Collection
Data collection was conducted face-to-face by researchers between May 2023 and March 2024. Pretest data were collected before the mothers in the experimental group received breastfeeding education using MI technique, using the MDIF, PBMS, BSES, MIBS, and Importance and Confidence-Efficacy Rating Ruler. Post-test data were obtained 15 days after the four-session MI-based breastfeeding education (postpartum days 45–57) using PBMS, BSES, MIBS, and the Importance and Confidence-Efficacy Rating Ruler. Follow-up test data were collected 4 weeks after the post-test (postpartum days 75–87) using the same assessment tools. The data from mothers in the control group were collected at the same intervals as those in the experimental group for the pretest, post-test, and follow-up assessments. The average duration of data collection at each follow-up session was ~20–25 minutes.
Data Evaluation
The data were analyzed using IBM SPSS version 27.0 for Windows (IBM Corp, Armonk, NY). Descriptive statistics, including percentages, means, medians, and standard deviations, were employed for data evaluation. The normality of the data distribution was assessed using the Shapiro–Wilk test (Gravetter et al., 2021). Relationships between descriptive characteristics and categorical variables were examined using Yates’ correction, Fisher‘s exact test, and the χ2 test. Differences in measurements between participants in the experimental and control groups across time points were analyzed using robust analysis of variance, the Bonferroni correction, and the Friedman test with repeated measures. For comparisons between paired groups, Student’s t test and the Mann–Whitney U test were applied. The effect size for significant differences in independent-sample t test results was determined using Cohen’s d, whereas η² was employed to calculate the effect size for significant differences identified in the analysis of variance. The contribution of fixed effects was quantified using marginal R². Analyses were conducted according to the intention-to-treat principle, including all randomized participants in their originally assigned groups. To account for missing repeated outcome measurements across three time points, we used linear mixed-effects models with maximum likelihood estimation/multiple imputation, with fixed effects for group, time, and group × time and a random intercept for participants. Missing repeated measures were handled using maximum-likelihood estimation within mixed models, which employs all available data without listwise deletion. All data were evaluated at a 95% confidence interval, with a significance level set at p < 0.05.
Ethical Considerations
Ethical approval was obtained from the Gümüşhane University Scientific Research and Publication Ethics Committee (March 23, 2022; No. E-95674917-108.99-86712). Institutional permission was received from the Gümüşhane Provincial Health Directorate for the relevant hospitals and family health centers (April 29, 2022; No. E-51020271-044). Written informed consent was obtained from all participants before enrollment. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Researcher Competence
The researcher (ÖPA) completed a 3-day training program in MI techniques delivered by expert academics in the field. In addition, the researcher holds certification in breastfeeding counseling (46 hours) and childbirth preparation educator training (115 hours).
Results
Participant Flow
Pretest analyses included data from 43 participants in each group, whereas post-test and follow-up analyses were conducted with 40 participants per group. The study was reported in accordance with CONSORT guidelines for randomized, controlled trials (EQUATOR Network, 2010; see Figure 1).
As shown in Table 2, no statistically significant differences were observed between the experimental and control groups regarding sociodemographic, obstetric, or breastfeeding characteristics (Table 2).
Comparison of Sociodemographic, Obstetric, and Breastfeeding Characteristics of Mothers in the Experimental and Control Groups (n = 80).
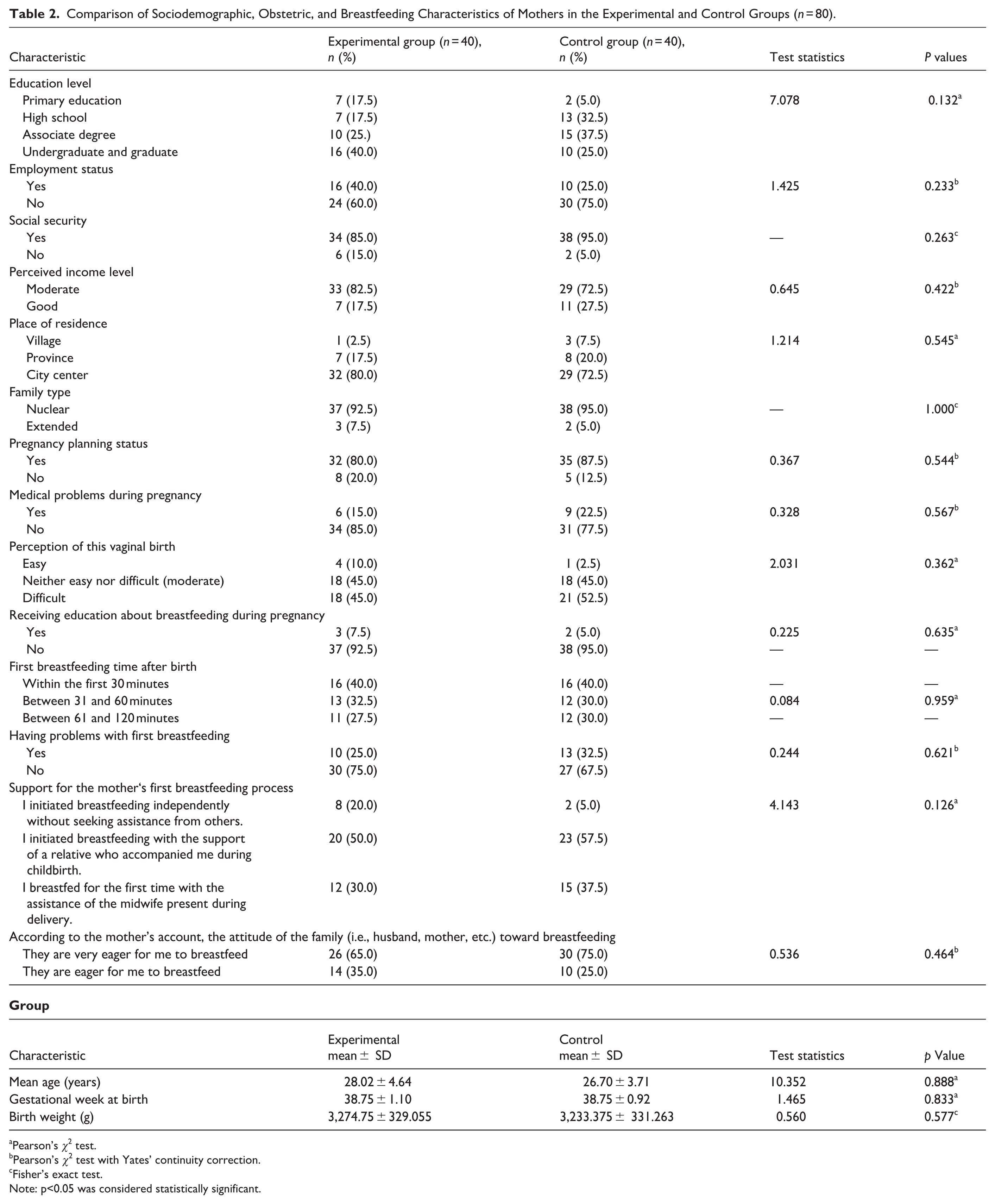
Pearson’s χ2 test.
Pearson’s χ2 test with Yates’ continuity correction.
Fisher’s exact test.
Note: p<0.05 was considered statistically significant.
Regarding the PBMS subdimensions, no statistically significant difference was observed between the pretest mean scores of the experimental and control groups (p > 0.05). In the post-test measurements, the experimental group showed significantly higher scores in the values ascribed to breastfeeding subdimension (p < 0.001) and midwife support subdimension (p < 0.001) than the control group. However, no statistically significant difference was noted between the groups in the self-efficacy and expectation of success subdimension scores (p > 0.05). In the follow-up test measurements, the experimental group continued to exhibit significantly higher mean scores than the control group in the subdimensions of value ascribed to breastfeeding (p = 0.004), self-efficacy (p < 0.001), and midwife support (p = 0.003). The difference in expectation of success subdimension scores between the groups remained statistically insignificant (p > 0.05; Table 3).
Comparison of the Mean Scores of the Subdimensions of the Primipara Breastfeeding Motivation Scale (n = 80).

Note. Fa = linear mixed model. Contribution of fixed effects was quantified using marginal R². p<0.05 was considered statistically significant.
Student’s t test.
Two-way analysis of variance in repeated measures.
Mann–Whitney U test.
Friedman test.
Pre-education (pretest).
Post-education (post-test).
Follow-up test.
The within-group analysis of the experimental group over time revealed statistically significant differences in the subdimensions of value ascribed to breastfeeding (p < 0.001), self-efficacy (p < 0.001), and midwife support (p < 0.001). However, no significant difference was observed in the expectation of success subdimension (p > 0.05; see Table 3).
Similarly, the within-group analysis of the control group over time indicated statistically significant differences in the value ascribed to the breastfeeding (p < 0.001) and self-efficacy (p = 0.004) subdimensions. In contrast, no significant differences were found in the midwife support and expectation of success subdimensions (p > 0.05; see Table 3).
The analysis of the joint effect of group and time demonstrated significant differences in the value ascribed to the breastfeeding (p = 0.025), self-efficacy (p = 0.002), and midwife support (p < 0.001) subdimension scores. However, no statistically significant difference was found in the expectation of success subdimension (p > 0.05; see Table 3).
There was no statistically significant difference between the BSES pretest and post-test mean scores of the experimental and control groups (p > 0.05). However, in the follow-up test measurement, the experimental group had significantly higher scores than the control group (p = 0.033; Table 4).
Comparison of the Mean Scores of the Breastfeeding Self-Efficacy Scale (n = 80).
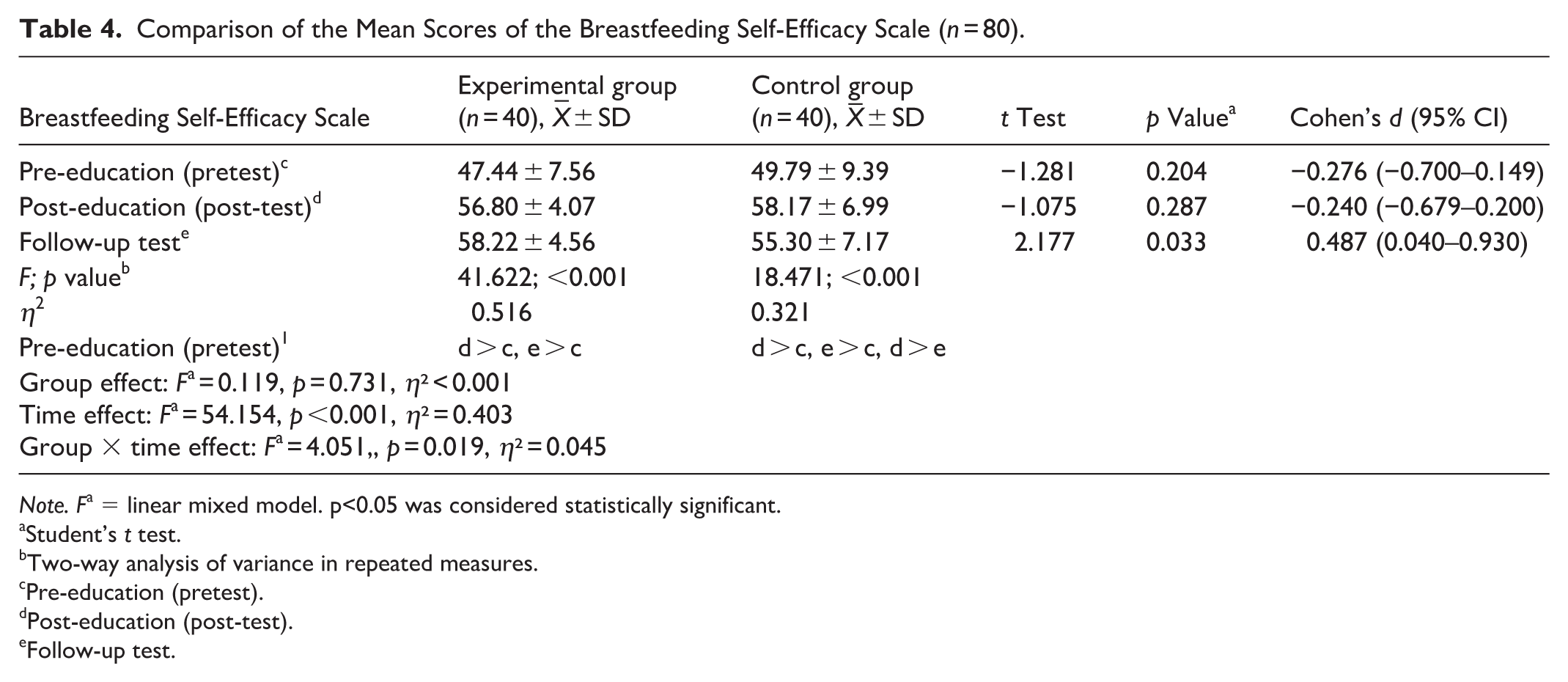
Note. Fa = linear mixed model. p<0.05 was considered statistically significant.
Student’s t test.
Two-way analysis of variance in repeated measures.
Pre-education (pretest).
Post-education (post-test).
Follow-up test.
A statistically significant difference was observed in the BSES scores within both the experimental (p < 0.001) and control (p < 0.001) groups over time (see Table 3). Furthermore, the joint effect of group and time on the BSES score was significant (p = 0.041; see Table 4).
There was no statistically significant difference between the pretest and post-test mean scores of the MIBS in the experimental and control groups (p > 0.05). However, in the intergroup comparison of the follow-up test, the median score of the experimental group was significantly lower than that of the control group (p = 0.002), indicating a higher mother–infant bonding in the experimental group during follow-up (Table 5).
Comparison of Mother–Infant Bonding Scale Mean Scores (n = 80).
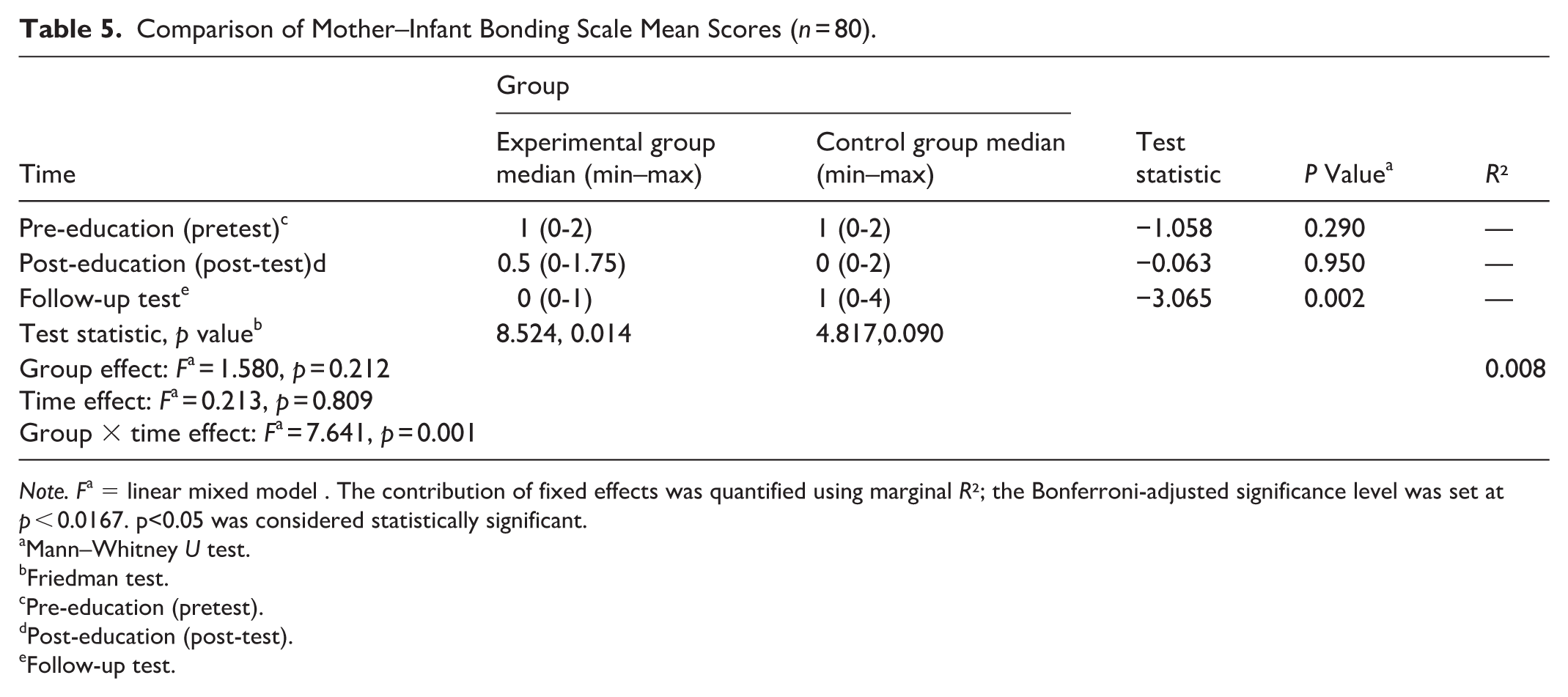
Note. Fa = linear mixed model . The contribution of fixed effects was quantified using marginal R²; the Bonferroni-adjusted significance level was set at p < 0.0167. p<0.05 was considered statistically significant.
Mann–Whitney U test.
Friedman test.
Pre-education (pretest).
Post-education (post-test).
Follow-up test.
Within-group analysis revealed a statistically significant difference in MIBS scores over time in the experimental group (p < 0.014), whereas no significant change was observed in the control group (p > 0.05; see Table 5). Additionally, the interaction effect of group and time on MIBS scores was statistically significant (p = 0.001; see Table 5).
No statistically significant difference was observed between the experimental and control groups in mean pretest scores on the Motivational Interviewing Importance and Confidence-Efficacy Rating Ruler (p > 0.05). However, the experimental group demonstrated higher scores than the control group at both the post-test (p = 0.030 and p < 0.001, respectively) and the follow-up assessment (p = 0.020 and p < 0.001, respectively; Table 6).
Comparison of the Mean Scores of the Motivational Interviewing Importance and Confidence-Efficacy Rating Ruler (n = 80).

Student’s t test.
Note: p<0.05 was considered statistically significant.
Discussion
This study evaluated the effect of breastfeeding education incorporating MI technique on breastfeeding motivation, self-efficacy, and mother–infant bonding among mothers who had a vaginal birth. Findings indicate that the value ascribed to breastfeeding, a subdimension of breastfeeding motivation, was significantly higher in the experimental group than in the control group. Bekmezci and Meram (2025) reported that mothers receiving postpartum breastfeeding education based on MI demonstrated higher scores in the value ascribed to breastfeeding than the control group. Although their study focused on mothers who had undergone cesarean section, it was consistent with our study. Several studies have reported that breastfeeding education based on solution-focused counseling, the theory of planned behavior, and group-based training approaches enhances the perceived value of breastfeeding and supports breast milk production (Dağlı & Aktaş Reyhan, 2024; Laily et al., 2021; Okhovat et al., 2024).
In this study, the self-efficacy subdimension of breastfeeding motivation did not show a statistically significant difference between the groups in the post-test measurements; however, a significant difference was observed in favor of the experimental group in the follow-up test. Additionally, although the self-efficacy subdimension scores in the experimental group increased progressively in the post-test and follow-up test periods, a decline was observed in the control group between these periods, suggesting that breastfeeding education incorporating the MI technique has a sustained positive effect on self-efficacy. Previous studies have similarly indicated that breastfeeding education based on MI enhances maternal self-efficacy (Bekmezci & Meram, 2025; Franco-Antonio et al., 2020). MI is grounded in the principle of reinforcing an individual’s capabilities (Salehi et al., 2019). In line with this principle, various breastfeeding education techniques structured according to MI philosophy have been shown to improve breastfeeding self-efficacy among mothers (Chan et al., 2016; Salehi et al., 2019).
In this study, the midwife support subdimension of breastfeeding motivation was higher in the experimental group than in the control group. Consistent with this finding, previous studies have reported that mothers who received breastfeeding support from nurses and midwives using MI technique in the postpartum period experienced increased breastfeeding self-efficacy, motivation, and duration (Addicks & McNeil, 2019; Bekmezci & Meram, 2025; Cangöl & Şahin, 2017; Naroee et al., 2020). Comprehensive nursing and midwifery care that facilitates mother–infant interaction, encourages breastfeeding, and motivates mothers in the early postpartum period has been associated with improved breastfeeding outcomes and a more positive birth experience. A qualitative study revealed that some mothers described their first breastfeeding experience as a particularly meaningful and memorable moment. They expressed gratitude toward midwives who provided assistance, encouragement, and emotional support during this process (Aktaş & Küçük Alemdar, 2025).
In this study, the expectation of success subdimension of breastfeeding motivation did not show a statistically significant difference between the experimental and control groups. In contrast, Nikula et al. (2024) reported that breastfeeding counseling delivered through a mobile application significantly supported mothers’ breastfeeding success in the 6-month postpartum period (Nikula et al., 2024). The discrepancy between these findings may be attributed to differences in the educational methods used and variations in the sociodemographic characteristics and postnatal support perceptions of the study participants.
Breastfeeding self-efficacy plays a critical role in initiating breastfeeding and sustaining breastfeeding behavior (de Sousa et al., 2025). In the post-test measurements, no statistically significant difference was observed between the experimental and control groups in terms of breastfeeding self-efficacy. However, in the follow-up test, a significant difference emerged in favor of the experimental group. This finding supports another result of our study, which indicates that breastfeeding education provided through the MI technique positively influences breastfeeding confidence and efficacy scores. The consistency between these findings suggests a potential positive relationship between a mother‘s confidence and efficacy in breastfeeding and her overall breastfeeding self-efficacy. Franco-Antonio et al. (2021) conducted motivational interviews with mothers who had vaginal deliveries immediately postpartum and at the first, third, and sixth months postpartum and reported an increase in breastfeeding self-efficacy over time. Similarly, in a study conducted in Spain in 2022, the experimental group exhibited significantly higher breastfeeding self-efficacy scores at 3 months postpartum following motivational interviews that supported breastfeeding in the context of postpartum depression (Franco-Antonio et al., 2022). Furthermore, a study in Brazil by Dodou et al. (2021) implemented four postnatal MI sessions via telephone, demonstrating that mothers in the experimental group had higher breastfeeding self-efficacy scores at 60, 120, and 180 days postpartum (Dodou et al., 2021), consistent with our findings.
In this study, the comparison of mother–infant bonding levels between groups showed no statistically significant difference in the post-test evaluation. However, in the follow-up test, the bonding level was significantly higher in the experimental group than in the control group. A review of the literature revealed no previous studies specifically examining the effect of breastfeeding education delivered through MI technique on mother–infant bonding. Therefore, this finding was evaluated in the context of studies investigating the impact of breastfeeding education using different techniques on mother–infant bonding. Similar to our findings, Sarı Öztürk and Demir (2023) reported that a mandala-based breastfeeding program did not have a statistically significant effect on mother–infant bonding immediately post-intervention. However, in a follow-up test conducted 8 weeks later, mother–infant bonding levels were higher in the experimental group (Sarı Öztürk & Demir, 2023). Likewise, Kheirandish et al. (2026) demonstrated that a four-session MI intervention administered to mothers with a history of birth trauma significantly improved mother–infant bonding (Kheirandish et al., 2026). Previous studies have highlighted that while immediate breastfeeding initiation did not necessarily correlate with child bonding, prolonged breastfeeding is significantly associated with secure bonding (Britton et al., 2006; Linde et al., 2020). The post-test comparison of mother–infant bonding levels between groups did not show a statistically significant difference, but the follow-up test did in favor of the experimental group in our study, which supports this established association. One possible explanation is that skin-to-skin contact during breastfeeding, frequent maternal touch, and increased emotional engagement may foster a stronger mother–infant bond (Linde et al., 2020; Roth et al., 2021). In this context, the breastfeeding education provided through MI technique may have contributed to mother–infant bonding by promoting breastfeeding duration and continuity.
Studies using MI technique have commonly employed the Importance and Confidence-Efficacy Ruler (Addicks & McNeil, 2019; Ögel & Şimşek, 2021). In our study, we examined the impact of breastfeeding education incorporating MI on the importance that mothers place on breastfeeding as well as their confidence and efficacy in breastfeeding. The results showed that the experimental group demonstrated significantly higher levels of importance attached to breastfeeding, confidence in breastfeeding, and overall efficacy than the control group, consistent with previous research (Addicks & McNeil, 2019; Bekmezci & Meram, 2025; Cangöl & Şahin, 2017).
Strengths and Limitations
This study has several strengths. Breastfeeding education based on MI technique was delivered face-to-face, all sessions were conducted by the same researcher, and the intervention was implemented in accordance with the postpartum follow-up schedule specified in the Ministry of Health’s postpartum care management guidelines. In addition, the inclusion of primiparous mothers with no prior breastfeeding experience, comparable sociodemographic characteristics, and vaginal birth only enhanced group homogeneity and enabled a clearer evaluation of the intervention’s effectiveness.
The study also has several limitations. First, the sample consisted of primiparous mothers recruited from a single center. Second, the long-term effects of the education on breastfeeding behavior (e.g., at 3 and 6 months postpartum) were not assessed. Third, participant blinding was not feasible because informed consent had to be obtained before the delivery of breastfeeding education. Fourth, the inclusion of only Turkish-speaking mothers and the culturally homogeneous sample may limit the generalizability of the findings to populations with different cultural backgrounds.
Conclusion
Breastfeeding education delivered through MI enhanced mothers’ breastfeeding motivation, including the value attributed to breastfeeding, self-efficacy, and perceived partner support, as well as mother–infant bonding and mothers’ understanding of the importance of breastfeeding and self-efficacy in breastfeeding. At follow-up, the improvements in the value attributed to breastfeeding, self-efficacy, and partner support were maintained, and these improvements were accompanied by higher breastfeeding self-efficacy and stronger mother–infant bonding. However, no significant effect was observed for the expectation of success subdimension of breastfeeding motivation at either the post-education or follow-up assessments.
Based on these findings, integrating the MI technique into breastfeeding education provided by healthcare professionals, particularly nurses and midwives, is recommended. Future research should explore its effectiveness in both primiparous and multiparous mothers, enhance the frequency and number of sessions, and extend the study to larger populations using a mixed-methods research approach. Additionally, future longitudinal studies are recommended to evaluate the long-term effects of breastfeeding education based on MI on mothers’ breastfeeding attitudes and behaviors (e.g., at 3 and 6 months postpartum).
Footnotes
Acknowledgements
We thank all the mothers who participated in the study. This study was presented as an oral presentation at the 2nd International Gülhane Breast Milk and Breastfeeding Congress, Ankara, Türkiye, October 2024. This study received the Best Doctoral Thesis Award in the Field of Health at the award ceremony held annually by Karadeniz Technical University and determined by the commission on May 21, 2025.
Ethical Considerations
Ethical approval was obtained from the Gümüşhane University Scientific Research and Publication Ethics Committee (No. E-95674917-108.99-86712). Institutional approval was obtained from Gümüşhane Provincial Health Directorate (No. E-51020271-044).
Consent to Participate
Written informed consent was obtained from all mothers prior to the study.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Presidency of Turkish Health Institutes (TÜSEB) of the Ministry of Health of the Republic of Türkiye (Call No. 2023-A4-02; No. 32307).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Clinical Trial Registration
This study was a randomized, controlled experimental study. The study is registered at https://clinicaltrials.gov/ under No.NCT0631303.