
Abstract
Background:
Breastfeeding and the feeding of human milk is widely accepted as the standard for infant nutrition, but early discontinuation or mixed feeding with human milk substitutes is common in the United States. Breastfeeding difficulties from complex health needs including chronic illness of the mother or infant, and infant prematurity can play a role in early discontinuation. Improving breastfeeding support can improve breastfeeding duration. Physicians with expertise in management of chronic health conditions, infant prematurity, and breastfeeding medicine distinct from the lactation consultant's scope of practice are uniquely equipped to address the needs of medically complex dyads. Integrating a breastfeeding medicine clinic within the general pediatric clinic potentially allows for more timely breastfeeding medicine support in a familiar setting where newborns usually receive care within the first few days of their life. Physicians with expertise in breastfeeding medicine have been providing this care, but it is not widely available, and there are few reports documenting this model, or the impact of this model, including the care of adult patients within a pediatric practice.
Innovation:
Our aim was to design and implement a physician-run breastfeeding medicine clinic caring for both adult and pediatric patients, embedded within a pediatric practice specializing in high-risk dyads, and to begin the work of documenting use and successes of this type of care.
Conclusion:
The establishment of this breastfeeding medicine clinic increased access to breastfeeding medicine care and provides a first step towards describing clinical models and their impact in the growing field of breastfeeding medicine.
Keywords
Background
Breastfeeding and the feeding of human milk is widely accepted as the standard for infant nutrition (Meek et al., 2022). The American Academy of Pediatrics recommends exclusive breastfeeding for the first 6 months of life with continuation to 2 years and beyond (Meek et al., 2022). Early discontinuation, or mixed feeding with human milk substitutes along with breastmilk, is common, and results from a variety of reasons that include breastfeeding difficulties and illness (Odom et al., 2013). Breastfeeding duration in the United States falls short of recommended guidelines (Centers for Disease Control and Prevention [CDC], 2023), and breastfeeding initiation rate in 2019 was 82.9% (CDC, 2023). Continuation rates drop each month, and U.S. data from 2019 shows that 55.8% of infants receive breastmilk at 6 months and only 24.9% exclusively (CDC, 2023). Women with chronic diseases have been shown to have lower rates of breastfeeding to 6 months as compared to women without chronic diseases (Scime et al., 2022). Many women do not reach their breastfeeding goals and stop breastfeeding earlier than intended (Odom et al., 2013).
Breastfeeding support, including following hospital discharge after birth, has been shown to ameliorate early breastfeeding discontinuation (Gianni et al., 2019; Patnode et al., 2025). Only half of women with breastfeeding issues felt supported by a health care professional after discharge (Gianni et al., 2019). Lactation education is not standardized for physicians during training, and not all are prepared to provide evidence-based lactation counseling and management (Meek et al., 2020). Parents may have delays or difficulty in accessing care from trained lactation providers. These delays, during this critical period of lactation, increase the chance of suboptimal breastfeeding. Integrating a lactation clinic within the pediatric clinic potentially allows for more timely breastfeeding support—such as for establishing milk supply or latching assistance—in a familiar setting where newborns receive care within the first few days of life. These could be staffed by lactation professionals such as International Board Certified Lactation Consultants (IBCLCs) and/or physicians with training in lactation management. For such U.S.-based practices, no referral is needed for the infant, and families already know their insurance is accepted within the clinic, which reduces the need for families to find a separate IBCLC or lactation clinic in network with their insurance.
There is a further need to support the more medically complicated dyads: mothers and infants with chronic disease, infants with prematurity, and those that have persistent breastfeeding issues despite initial lactation management, such as continued pain or low milk supply (Hwang et al., 2013). Physicians with expertise in both management of chronic health conditions and breastfeeding medicine distinct from the IBCLC scope of practice are uniquely equipped to address the needs of these medically complex dyads, and can address both infant and parent medical and psychosocial concerns as part of the medical visit. Breastfeeding medicine physicians should have experience and training to be proficient in standard core competencies to provide medical care and lactational management for these dyads (Rosen-Carole et al., 2022). They can evaluate through examinations, laboratory testing, and imaging, and make diagnoses and treatment plans that include prescriptions, not all of which non-physician lactation providers are licensed to do. This may include medical treatment of maternal breast dermatitis or mastitis, obtaining milk cultures, medication management, infant jaundice, growth faltering, or food intolerances in the context of supporting and trouble-shooting breastfeeding. Breastfeeding medicine physicians, including those with clinical expertise without separate certification, physician-IBCLCs, Fellows of the Academy of Breastfeeding Medicine, and now, since 2023, physicians board-certified through the North American Board of Breastfeeding and Lactation Medicine (NABBLM), have been providing expert breastfeeding care in inpatient settings, specialty practices, or within the scope of general clinical practice, often as part of well-baby care in the outpatient clinic. However, access to these services is not widespread, and there are few published reports documenting the latter model or the impact or sustainability of this model, including the integration of providing care for adult patients within a pediatric practice. Especially as the NABBLM field grows, documenting sustainable breastfeeding medicine clinical models is imperative (Demirci et al., 2025). There is little research into impact on breastfeeding duration with practices that include physician breastfeeding medicine visits addressing the maternal and infant medical complexities that arise or are existing during lactation, in the United States, especially as distinct from well-baby care, and more work is needed to evaluate clinic sustainability and outcomes (Balogun et al., 2016; Bunik et al., 2014; Shaikh & Smillie, 2008).
The authors decided to address this issue by documenting the creation of a physician breastfeeding medicine clinic embedded within an established pediatric medical practice. The project took place at an academic center in a large city in the Western United States. The clinic is an academic general pediatric practice that serves as a teaching site to medical students and pediatric residents and provides acute and preventive care to patients of diverse backgrounds with a variety of insurance payors. A premature infant clinic run initially by one physician with expertise in breastfeeding medicine and supporting breastfeeding in premature infants, and an IBCLC, which later transitioned to physician care only, was previously established within this practice, with one half day session per week; however, there was previously no comprehensive breastfeeding medicine clinic. The team’s objective was to demonstrate patient use for this type of comprehensive breastfeeding medicine service as well as the ability of a general pediatrics practice to incorporate care of the adult lactating person. Our aim was to design and implement a physician-run breastfeeding medicine clinic within the pediatric clinic specializing in dyads at high risk of lactation problems, including those with premature infants and mothers or infants with complex or chronic health conditions impacting lactation.
The authors acknowledge and recognize that not all people who lactate identify as female or mothers, and not all people who lactate use the term breastfeeding. There are no standard terms that are inclusive to all genders in all languages and which are always appropriate. The terms mother and breastfeeding are used in this paper, but the authors’ intention is to be inclusive of all breastfeeding and human milk feeding individuals (Bartick et al., 2021).
Key Messages
• Physicians with expertise in breastfeeding medicine can provide lactation care as part of their medical practice, but it is not widely available, and there are few published reports documenting the model of integrating physician-run lactation care, or the care for adult patients within a pediatric practice, or the impact of this model.
• We describe the design and implementation of a physician-run breastfeeding clinic specializing in high-risk dyads that includes the care of both adult and pediatric patients and is embedded within a general pediatrics practice.
• This work is a first step in evaluating the impact of this model and promoting more widespread physician-delivered lactation care to dyads with complex needs.
Clinical Innovation
Many of the mothers seen in this clinic have high risk pregnancies and deliver preterm and/or have comorbid conditions that result in suboptimal breastfeeding, and there is a high demand for breastfeeding medicine services among this population. Three pediatrician breastfeeding medicine experts, who are either board-certified in breastfeeding medicine through NABBLM or a Fellow of the Academy of Breastfeeding Medicine (FABM), worked with clinic leadership to design and open a clinic for physician-run breastfeeding care within a pediatric practice focusing on dyads at high risk of lactation problems.
Clinic Model
Given the population, the decision was made to design the clinic with physician level care, without separate lactation counselor support, to enable the treating physician to address lactation needs while also addressing complex medical needs. It is common for pediatricians to offer breastfeeding medicine care that is directed toward issues with the lactating parent, even when the infant is the only registered patient. This limits the time that may be spent with a dyad and reimbursement. The model for our clinic is to register both the infant and the mother as patients. This extends the time allowable for each dyad, and allows for diagnosis and treatment of pediatric problems such as slow weight gain, jaundice, and hypotonia impacting breastfeeding, along with maternal problems such as screening and coordination of care of postpartum depression, hypo- or hypergalactia, and mastitis. This allows for the billing and reimbursement of both pediatric and maternal services, improving clinic sustainability. It allows for prescribing and laboratory analysis of both the infant and the mother. The team conducted an informal gathering of information such as staffing model, visit length, registration of parent and/or baby, and coding practice, from breastfeeding medicine physicians in outpatient academic settings across the United States, through an email request to approximately five groups, to identify common practices. Based on that information and current practice within the premature infant clinic, it was decided that new visits would be scheduled for 60 minutes per dyad and return visits for 30 minutes per dyad. A scheduling protocol for office staff was designed, and training provided. Office staff schedule and check-in patients per standard protocol, and medical assistants room patients obtaining length, head circumference, and dry diaper and naked weights on the infants, to allow for test weights to be obtained and growth to be assessed. Mothers have blood pressure taken and complete a postpartum depression screening tool. Pertinent mother and infant physical examinations are conducted, such as breast exam for the mother, to assess for physical findings such as wounds, erythema, and shape, and infant head, neck, jaw, and oral examinations are made to assess for physical findings such as tone, torticollis, tongue movement, and suck ability. Breastfeeding and pumping assessments, support, and follow-up plans are provided. Open breastfeeding medicine slots can be filled with pediatric acute care visits the same day; this flexibility is not available in a breastfeeding medicine only practice.
Physical Space
The clinic uses existing patient care rooms within the practice. New reclining chairs were purchased. Breastfeeding support pillows and footstools were available to patients. The clinic was stocked with breastfeeding care supplies such as nipple shields and dressings for nipple care. A variety of flange types and sizes along with breast and infant models are used as demonstration tools for learners in the clinic or patients as needed.
Electronic Health Record and Billing
The electronic health record (EHR) in this practice uses a pediatric-specific instance. The clinical team worked with the EHR team to develop breastfeeding medicine note templates and integrate them within the EHR, which include sections on current breastfeeding problems, maternal and infant health history, maternal breastfeeding history, medications, current feeding and pumping plan (Table 1).
Breastfeeding Medicine Note Template Sample Information.
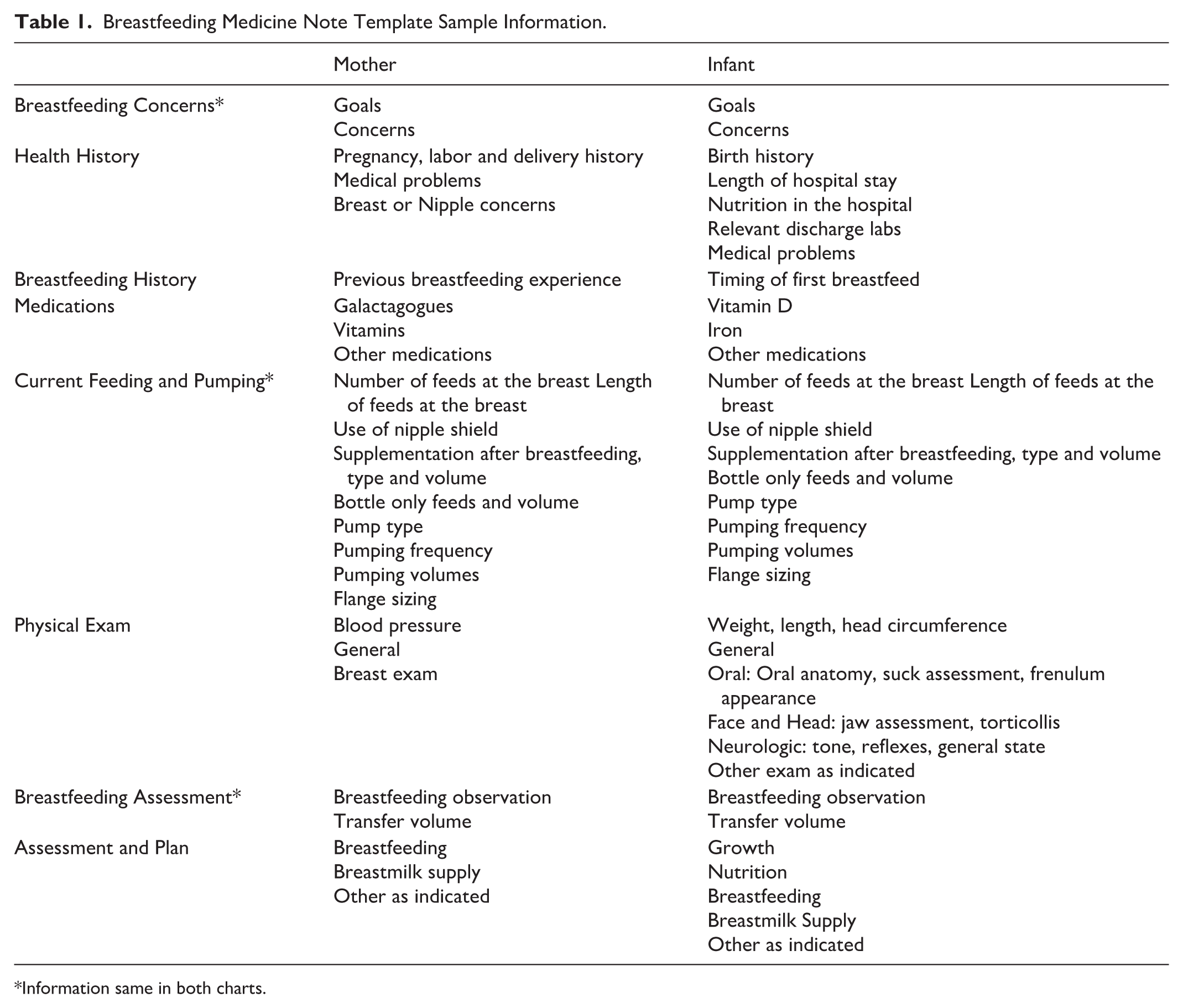
Information same in both charts.
Mothers fill in a questionnaire electronically on a tablet before the visit, and information from this auto-populates into the note templates. Drop-down options with common information and responses are available to reduce typing time. The clinical team worked with the EHR team to develop billing and order sets and embed them within the EHR to standardize billing (Table 2).
Billing and Order Set Sample Selections.
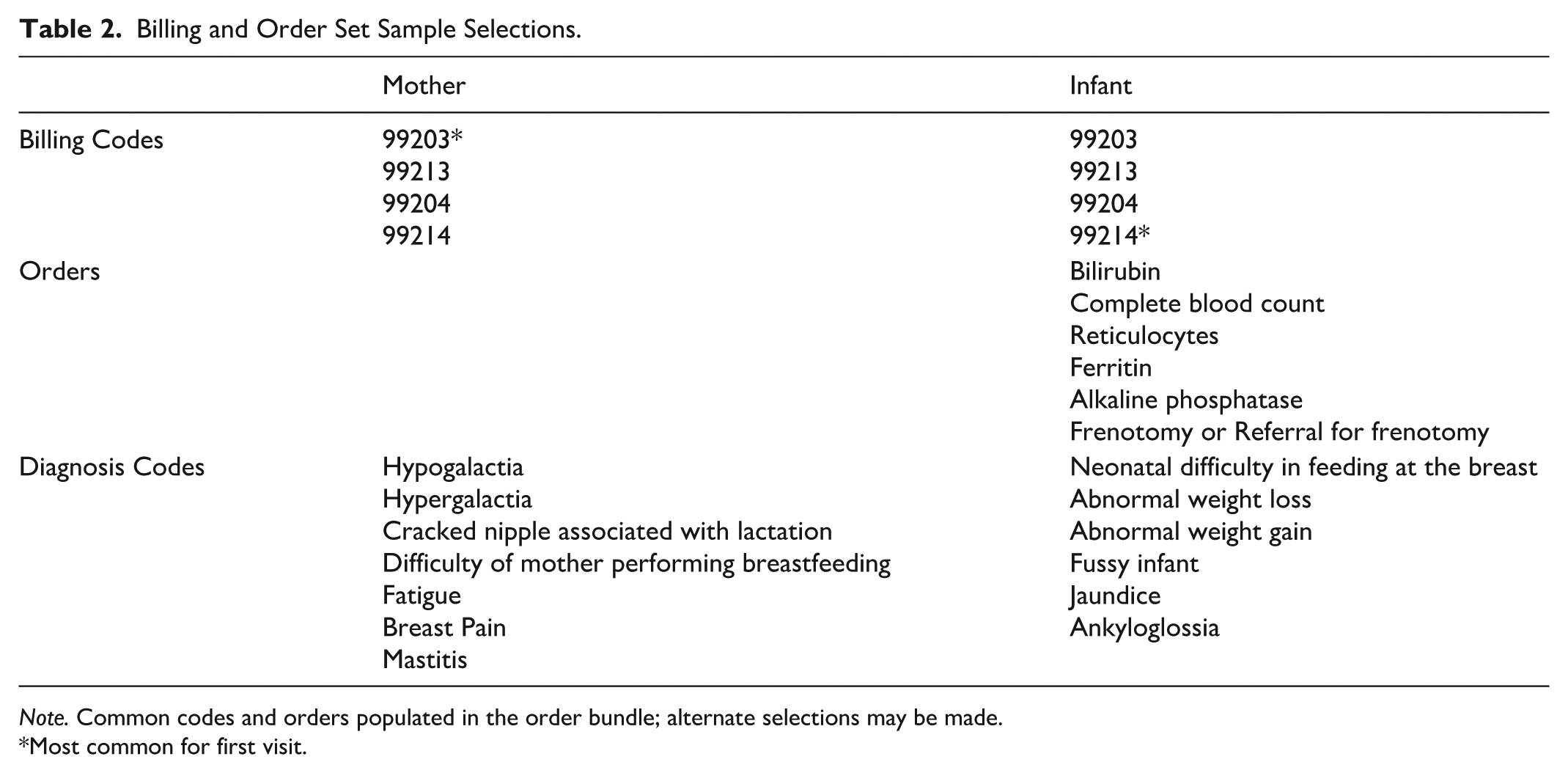
Note. Common codes and orders populated in the order bundle; alternate selections may be made.
Most common for first visit.
Billing is generally time-based and split between the dyad evenly or weighted based on the complexity of the two patients. The EHR work allows for standardization of information collection across breastfeeding medicine physicians within the practice and saves time by streamlining documentation and orders.
Eligibility
Eligible patients include those with identified lactation problems or those at risk for suboptimal breastfeeding including preterm infants, lactating mothers or infants with complex medical conditions, older lactating mothers, and previous suboptimal breastfeeding. Pre-delivery consultations are available.
Referrals
The services were advertised through our institution and a large local breastfeeding organization. Patients self-refer or are referred by the baby’s provider or maternal provider, upon newborn or neonatal intensive care discharge. A challenge identified in this process was insurance approval for the adult patient. Some insurance payors require a referral to our clinic from the mother’s primary care provider or obstetrician, which needs to be authorized before services are rendered. As a primary care practice, this office had not previously needed a process for verifying insurance authorization of referrals. The team worked with leadership on developing a referral system and process for obtaining authorization for mothers’ visits from insurance. Mothers are informed whether a referral is needed based on their insurance type at the time they call to schedule an appointment, and are directed to request a referral be sent by their primary physician. Verifying referral status, which can be challenging when the referrals originate in an EHR system outside our pediatric EHR, adds to the workload for the front office team. Inaccurate referral information can lead to reduced reimbursement. The referral process remains an ongoing area for process improvement. Our biggest source of referrals is our hospital system’s NICU and obstetric groups.
Clinic Launch
The clinic opened in January 2023. The half-day clinic opened with appointment slots for four breastfeeding dyads per week per provider, on separate days of the week, in addition to the pre-existing premature infant breastfeeding medicine half-day clinic. Thus, breastfeeding medicine access in this practice more than doubled. The clinic sees many infants with history of NICU stays, prematurity, faltering weight or medical conditions requiring treatment including reflux and food intolerances, and mothers with chronic health conditions or medical needs, such as history of breast cancer or recurrent mastitis, leading to breastfeeding challenges. One challenge noted with the clinic launch was an increased no-show appointment rate as compared to the general practice. This was reduced by instituting a procedure for the front office staff to personally call families the day before the appointment, not relying on automated appointment reminders as is done in the general clinic. On average, three to four dyads are seen during each clinic session, and clinic sessions have been consistently booked by both new and returning dyads. The first visit often occurs within the first 7–14 days after birth or NICU discharge, and many dyads are seen for multiple visits. On occasion, either the mother or infant may be seen without the other if the issue exclusively relates to one, such as the case of breast dermatitis in an exclusively-pumping mother. This breastfeeding clinic within the larger academic general pediatric clinic was incorporated into the pediatric residency program breastfeeding medicine elective, and the elective is hosting three to four residents per year for dedicated breastfeeding medicine teaching. The breastfeeding medicine physicians communicate with the mother’s provider when appropriate, such as for breast surgical needs.
Perspectives and Lessons Learned
Breastfeeding support is traditionally delivered through many avenues, each requiring varying levels of training in maternal and infant health, with varying scope of practice, including community health workers, non-medical lactation consultants or IBCLCs, and nurse or physician lactation consultants or IBCLCs. Physician-level breastfeeding medicine care of medically complex dyads provides for breastfeeding medicine management within the context of a robust medical foundation. Establishing a breastfeeding medicine clinic within the pediatric practice allows for more time to devote to specific breastfeeding problems, including social and maternal mental health problems as well as medical concerns and lactation and latch issues. It allows physicians to better address and bill for both maternal issues and infant issues. Physicians have been providing breastfeeding medicine care within their practices for years, and there are also physician-run clinics that provide only breastfeeding care and not general pediatric or maternal care. Yet, U.S. physician-run breastfeeding medicine care, especially through breastfeeding medicine visits in clinics distinct and separate from routine well-baby or postpartum care, is not widely accessible, and outcomes of these clinics are not well studied. We created a new physician-staffed breastfeeding medicine clinic and embedded it within our busy academic general pediatric practice to address this need for increased access to breastfeeding medicine care. This work reflects practices within our state, and may not reflect financial or clinical environments in other countries or states. Even with a physician-staffed clinic specializing in medically complex dyads, there is a need for other breastfeeding professionals such as IBCLCs to provide lactation care, and each has expertise in distinct areas. Addressing breastfeeding problems often takes time, and working in conjunction with other lactation providers may be optimal. The development of the NABBLM highlights the need to have physicians teaching medical students and residents standardized breastfeeding medicine practices for these complex dyads. As a resident physician teaching site, this breastfeeding medicine clinic serves that role. Recognizing the impact of physician-led breastfeeding care in teaching future physicians to provide this care is a step toward the more widespread implementation of breastfeeding medicine departments within academic institutions, which is a goal for this institution (Eglash, 2020).
Next Steps
The next phase of this work includes continued clinic growth with a goal of reaching more diverse populations, especially those with difficulty accessing care. Establishing best practices for referral coordination and authorization to improve reimbursement for pediatricians providing care to adult patients will be important for clinic sustainability. Program evaluation through survey data is being performed. Collaborative research with other physician-led breastfeeding practices and a standardization of data collection would improve evaluation of these practices (Shaikh & Smillie, 2008). It will be important to evaluate the impact of this and other physician-run breastfeeding medicine clinics on long term outcomes, including duration of breastfeeding, especially for those highest-risk groups.
Conclusion
Breastfeeding medicine physicians are a vital part of the lactation workforce and specialize in medically complex breastfeeding cases. The field is growing, but access is not yet widespread, and there is little published on clinic models or the impact of these models. The expanded breastfeeding medicine service in this practice increased access to early lactation care of dyads at high risk for lactation problems. Integration of a physician-staffed breastfeeding medicine clinic into the general pediatric practice that includes care of both the adult and infant patients is feasible and well-used. Improving outpatient breastfeeding medicine care for high-risk dyads may help increase breastfeeding duration. The establishment of this breastfeeding medicine clinic increased access to breastfeeding medicine care for high-risk dyads, was well used, enhanced breastfeeding support in the pediatric office, and provided a first step towards describing clinical models and their impact in the growing field of breastfeeding medicine.
Footnotes
Authors’ Note
A portion of the findings presented in this manuscript appeared on a poster at the International Meeting of the Academy of Breastfeeding Medicine in November 2024
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was partially funded by the Academy of Clinician Scholars at UC San Diego Health Sciences
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.