
Abstract
Background:
According to self-determination theory, when an individual’s psychological needs for autonomy, competence, and relatedness are satisfied, human flourishing can occur. The simultaneous satisfaction of the three needs has not yet been examined in the context of lactation and offers a potential explanation for variations in breastfeeding outcomes and well-being among lactating individuals.
Research Aim:
To develop and preliminarily validate an instrument measuring lactation-related psychological need satisfaction.
Method:
Initial items for the Lactation Psychological Needs Scale were developed based on a literature review, and refined based on content validity testing. An online cross-sectional survey was administered in two phases to lactating individuals in the United States (n = 634) to assess validity and reliability.
Results:
Exploratory (n = 388) and confirmatory factor analyses (n = 246) in separate samples yielded a three-factor solution with excellent goodness-of-fit (chi-square Bollen-Stine adjusted p = 0.05, root mean square error of approximate: ≤ 0.06, comparative fit index > 0.95, and Tucker-Lewis Index > 0.95). The new instrument includes 12 items on three subscales: autonomy, competence, and relatedness. Internal consistency reliability was acceptable for the full scale (0.856) and subscales (0.790–0.861). The full instrument scores and subscale scores were positively correlated with maternal satisfaction with lactation, and negatively correlated with Edinburgh Postnatal Depression Scale scores.
Conclusion:
The results of this study provide preliminary psychometric support for the novel instrument. Self-determination theory provides an opportunity for a new paradigm in understanding behavior and well-being among lactating individuals. Further validation of the instrument is required.
Keywords
Background
Globally, breastfeeding is recognized for its positive influence on the health of both infants and mothers (North et al., 2022). In the United States, breastfeeding initiation rates have improved over the last several decades (Lubold, 2019). However, rates of exclusivity and duration continue to fall short of Healthy People 2030 targets, with 24.9% (target 42.4%) of infants exclusively breastfeeding at 6 months and 35.9% (target 54.1%) breastfeeding at all at 12 months (Centers for Disease Control and Prevention [CDC], 2022; Office of Disease Prevention and Health Promotion, n.d.). Additionally, parents may not be meeting their own goals. A recent study showed that fewer than half (47%) of low-income women in the United States enrolled in the Special Supplemental Nutrition Program for Women, Infants, and Children who intended to exclusively breastfeed were doing so at 1 month postpartum (Beauregard et al., 2022). The persistent gap between recommended breastfeeding practices and actual rates underscores the need to better understand breastfeeding individuals’ perspectives.
Breastfeeding outcomes are not determined solely by the dyad’s physiological abilities but reflect a complex interplay of psychological, emotional, social, and structural factors (Pérez-Escamilla et al., 2023). Historically, lactation research has examined the psychosocial aspects of breastfeeding, with Self-Efficacy Theory and the Theory of Planned Behavior as the most used frameworks in research to improve breastfeeding outcomes (Amoo et al., 2022). Self-Efficacy Theory emphasizes an individual’s belief in their capability to perform a specific behavior and the influences on the likelihood of success (Bandura, 1997). The Theory of Planned Behavior posits that attitudes, social norms, and perceived behavioral control directly predict intentions, which proximally predict behavior (Ajzen, 1991). While both theories have demonstrated some utility in improving lactation outcomes, they may not be as helpful in promoting sustained breastfeeding. In a recent meta-analysis and systematic review, Chipojola et al. (2020) demonstrated that while interventions based on Breastfeeding Self-Efficacy theory improved breastfeeding self-efficacy at 1–2 months postpartum, they did not improve exclusive breastfeeding rates at 6 months. Similarly, a systematic review yielded inconsistent relationships between breastfeeding duration and the Theory of Planned Behavior constructs. While maternal intentions were consistently positively associated with duration, the evidence for attitudes, subjective norms, and perceived behavioral controls was mixed (Lau et al., 2018).
An alternative approach to understanding decisions about breastfeeding is through the lens of Self-Determination Theory (SDT), a broad psychological theory that explores the nature and motivation behind human behavior (Ryan & Deci, 2018). One aspect of SDT posits that innate psychological needs for autonomy, competence, and relatedness drive individuals.
In SDT, well-being is conceptualized from a eudaimonic perspective, encompassing more than subjective happiness (Ryan & Deci, 2018). Eudaimonia, or “flourishing,” involves pursuing worthwhile endeavors and realizing one’s capabilities. When individuals experience psychological need satisfaction, they are more likely to be motivated and engaged in behaviors that align with their authentic selves. In essence, satisfying basic psychological needs becomes a pathway to eudaimonic well-being, influencing motivation and behavior engagement (Figure 1). While conventional metrics like breastfeeding exclusivity or duration provide vital benchmarks, solely focusing on these outcomes may overlook the broader context of the individual’s experience. Emphasizing eudaimonic well-being underscores the importance of improving traditional breastfeeding outcomes and enhancing the overall quality of the breastfeeding and postpartum experience for the individual. This perspective acknowledges that fostering the flourishing of the individual may, in turn, lead to improved breastfeeding outcomes.
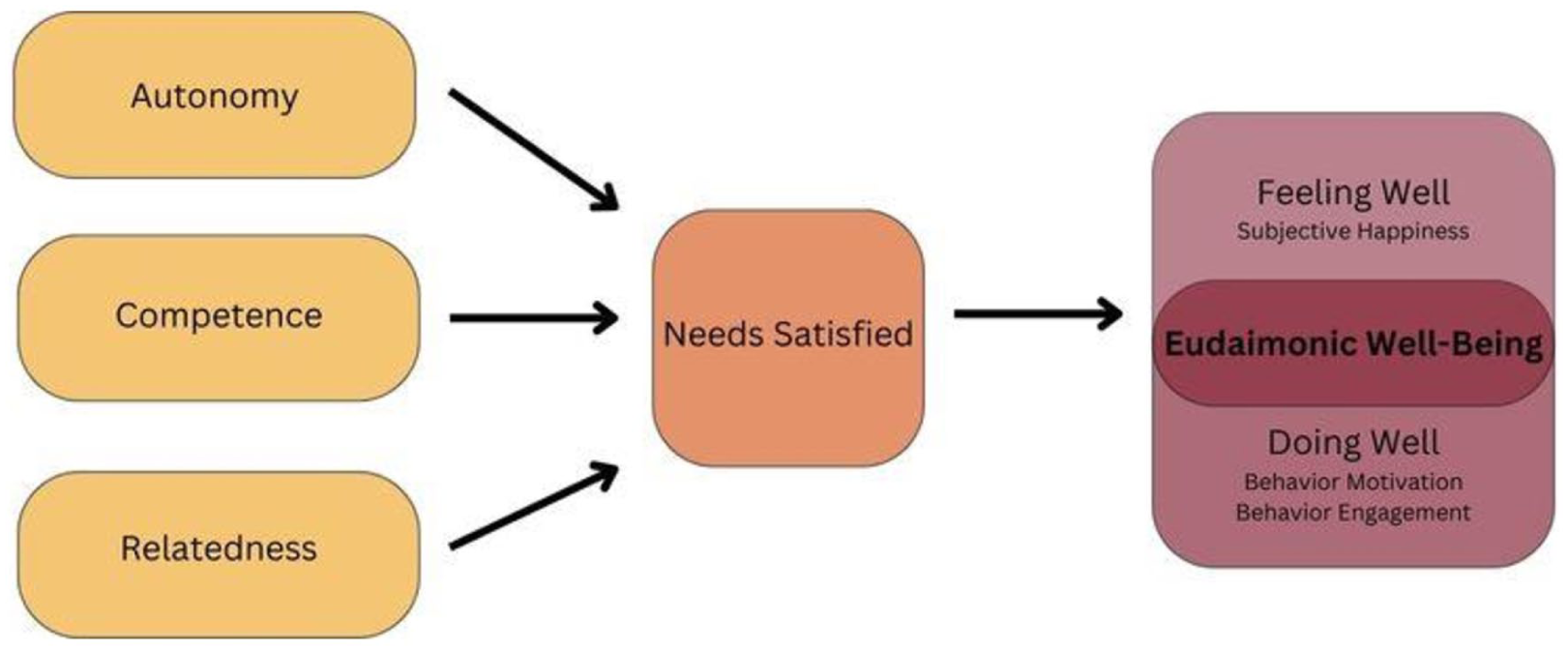
A model depicting basic psychological need satisfaction.
Key Messages
According to Self-Determination Theory, fulfilling the psychological needs for autonomy, competence, and relatedness helps people thrive; this premise has not previously been tested in the context of lactation.
This study developed a new instrument—the Lactation Psychological Needs Scale—which measures autonomy, competence, and relatedness among lactating individuals.
The Lactation Psychological Needs Scale had good preliminary validity and reliability.
This research contributes a new theoretically based instrument to the field of lactation and offers a new perspective on how to approach improving breastfeeding outcomes while holistically considering the individual’s well-being.
The three basic psychological needs are not entirely novel in lactation research. Competence is closely related to self-efficacy, a widely studied construct in breastfeeding (Chipojola et al., 2020). Similarly, maternal–infant attachment is closely related to relatedness and has been explored in lactation research (Linde et al., 2020). Autonomy has been researched in the context of breastfeeding, with SDT as the guiding framework in several instances. In particular, several studies have examined the degree of autonomy or control underlying breastfeeding motivation (Kadzikowska-Wrzosek, 2016; Kestler-Peleg et al., 2015; Lau et al., 2017, 2022; Martin et al., 2022; Mizrak Sahin et al., 2019).
However, the simultaneous consideration of autonomy, competence, and relatedness among lactating individuals is unprecedented in the literature. According to SDT co-founders Ryan and Deci (2018), a hierarchy does not exist within the basic psychological needs. Human flourishing cannot occur when the satisfaction of any or all of the basic psychological needs is thwarted. The notion that complete well-being cannot happen if only some of the needs are met (i.e., competence without autonomy) might explain why the existing lactation paradigms do not yield optimal results.
The present study explored SDT as a paradigm for understanding breastfeeding outcomes and general well-being in the postpartum period. To test the premises of basic psychological need satisfaction in this population, a valid and reliable measurement of the pertinent concepts is required. Few SDT-derived instruments related to breastfeeding exist (Kadzikowska-Wrzosek, 2016; Kestler-Peleg et al., 2015; Lau et al., 2017, 2022; Martin et al., 2022; Mizrak Sahin et al., 2019), but none examine the three needs in concert. Thus, the aim of this study was to develop and preliminarily validate an instrument measuring lactation-related psychological need satisfaction.
This study includes gender-diverse families, as not all individuals providing human milk to infants identify as women or use the term "breastfeeding." Our recruitment materials explicitly conveyed that any individuals who feed their infant at the breast or chest were welcome to participate, encouraging participants to substitute terms like "chestfeeding" or the most fitting designation for their infant feeding method where “breastfeeding” language was used. In this article, gendered language, including “women” and “mothers,” is presented when citing previous research. We use "breastfeeding" throughout for brevity.
Methods
Research Design
An online cross-sectional design was used to assess the validity of the Lactation Psychological Needs Scale (LPNS). This design was chosen because it allowed for efficient data collection from a geographically diverse sample of lactating individuals. As a novel instrument, the validation of the LPNS required evaluation of the content validity, exploration and confirmation of the factorial structure, internal consistency reliability, and criterion-related validity. Human Subjects Research approval was obtained from the Texas Woman’s University Institutional Review Board.
Setting and Relevant Context
This study was situated in the United States, and its findings must be interpreted in the sociocultural and economic landscape of breastfeeding within this country. Despite improvements in breastfeeding initiation rates in recent decades, substantial inequities persist, particularly affecting women of color and those with lower socioeconomic status (Chiang et al., 2021). The United States health care system is largely privatized and insurance-based, resulting in fragmented access to maternal and infant care. While some families receive breastfeeding support through programs like Special Supplemental Nutrition Program for Women, Infants, and Children (WIC), Baby-Friendly hospital initiatives, and community organizations like La Leche League, these resources may be unevenly distributed. Many families rely on out-of-pocket or community-based support, which may not be consistently accessible. In the United States, over half of women do not have access to paid leave after the birth of a child, and many (28.8%) do not qualify for appropriate breastfeeding breaks upon returning to work. Of the 193 United Nations member countries included in Sprague and colleagues’ (2024) study, the United States was one of seven to not provide paid maternity leave, and one of four to not provide paid breastfeeding breaks. Additionally, the country’s decision not to adopt the 1981 World Health Organization Code for Marketing of Breast-Milk Substitutes has allowed pervasive marketing practices that disproportionately target vulnerable populations, further exacerbating challenges in maintaining breastfeeding (Hastings et al., 2020).
Sample
Participants were eligible if they (1) lived in the United States, (2) could read and write in English, and (3) were breastfeeding or chestfeeding a child under a year old through latching. Exclusion criteria included breastfeeding or chestfeeding more than one child and exclusively pumping or expressing milk. Participants who expressed milk in addition to latching their infant were included, as were those who exclusively latched. This study focused on participants in the United States to maintain a more comparable cultural context, as international differences in parental leave policies, healthcare system, and breastfeeding norms could introduce additional variability. The instrument was designed specifically for individuals who engaged in direct latching. Screening was performed through eligibility questions at the start of the survey.
Participants were recruited in two phases. The first phase focused on exploratory factor analysis to refine the initial instrument and identify its underlying structure, and the second aimed to confirm the factor structure through confirmatory factor analysis. In both phases, participants were recruited through social media posts shared by the first author and La Leche League USA, a community breastfeeding organization. Social media posts included a brief study description and a survey link. Recruitment materials were also distributed via email. Snowball sampling was used as a secondary method, an approach that has previously been combined with social media as a recruitment strategy (Leighton et al., 2021). Individuals encountering the recruitment materials were encouraged to share with others that might be eligible to participate in the study. Participants in the second phase of the study were given the opportunity to enter to win a $100 gift card by entering their email address after completing the survey. After data collection was complete, 20 participants were selected using a random number generator and were emailed a $100 gift card.
A total of 481 surveys were submitted in the first phase, and 330 in the second phase. After removing responses that were less than half complete or flagged as potential duplicates, 388 responses from the first phase and 246 from the second phase remained for the exploratory and confirmatory analyses, respectively. Tabachnick and Fidell (2013) deem 300 cases as a generally appropriate sample size for exploratory factor analysis; this recommendation was met. Confirmatory factor analysis is also generally considered a large sample procedure. However, newer techniques have shown that samples smaller than 300 are often appropriate. For example, a Monte Carlo data simulation was used to establish sample size requirements based on the number of factors, indicators per factor, and the magnitude of factor loadings (Wolf et al., 2013). For a three-factor model with three indicators with factor loadings around 0.65, a minimum of 220 cases was deemed acceptable. With higher factor loadings and more items per factor, this requirement diminishes. Given the final 12-item instrument’s composition, a total of 246 cases is considered adequate. The amalgamated dataset (N = 634) from both phases was employed for the subsequent construct validity analyses.
Measurement
Demographic variables
Participants responded to items assessing their eligibility to participate in the survey, their sociodemographic characteristics, pregnancy history, and infant feeding practices. These items were developed by the first and second authors to capture relevant background information for descriptive purposes and to compare characteristics between exclusively and non-exclusively breastfeeding participants. Including demographic and clinical variables allowed for better understanding of potential confounders and helped control for bias in group comparisons. The full survey can be found in the online Supplemental File 1.
Developing the LPNS
The Lactation Psychological Needs Scale (LPNS) was developed and validated using the methodological steps outlined by Polit and Beck (2021). Table 1 depicts the study phases.
Summary of Study Phases.
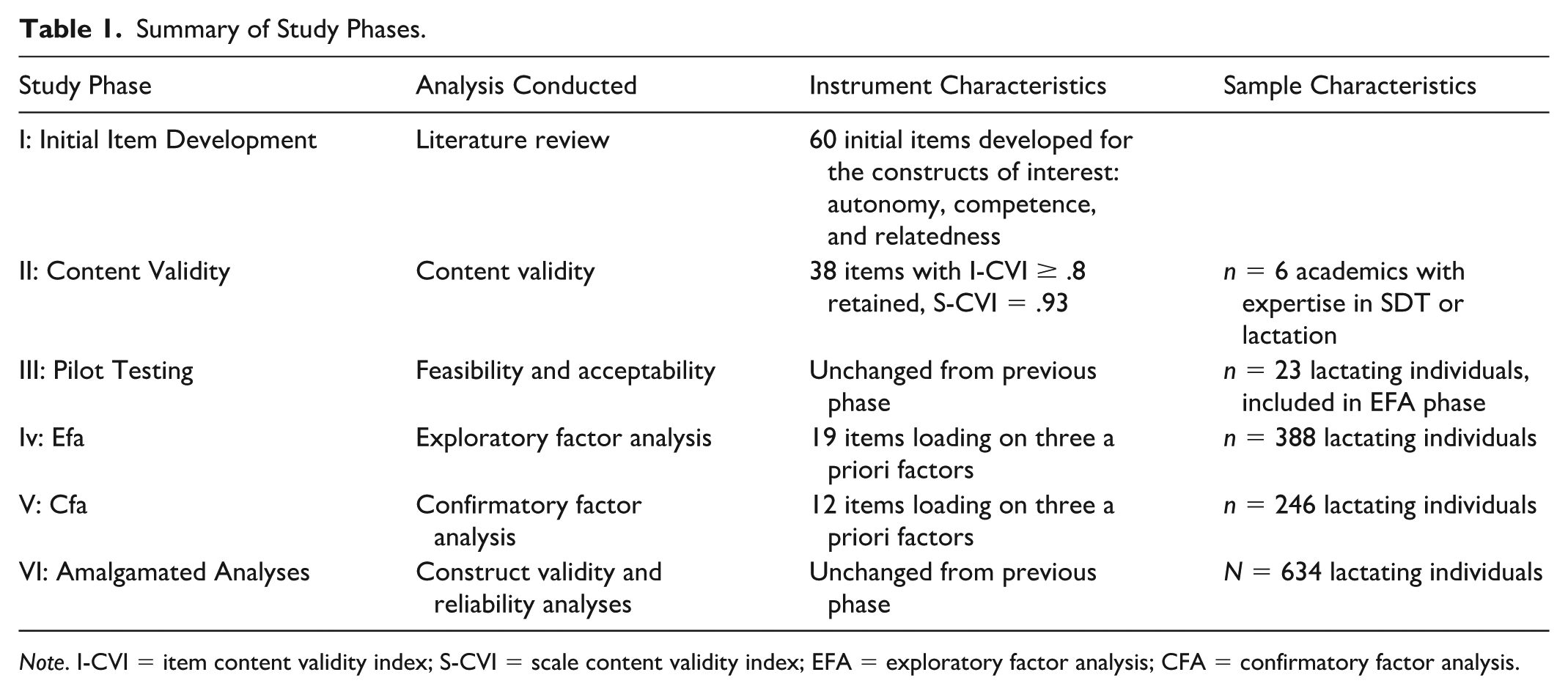
Note. I-CVI = item content validity index; S-CVI = scale content validity index; EFA = exploratory factor analysis; CFA = confirmatory factor analysis.
An initial pool of items to assess psychological need satisfaction was created by the first and second authors based on an extensive literature review. This review included gaining a comprehensive understanding of SDT literature and existing instruments relating to psychological need satisfaction in general and in other health and behavior contexts. Existing instruments from SDT that measure psychological need satisfaction in general or concerning specific contexts were examined. New items were generated, and some were adapted from previously developed measures (Dennis & Faux, 1999; Kestler-Peleg et al., 2015; Martin et al., 2022). The initial item pool consisted of 60 items using a 5-point Likert scale. The number of scale steps was selected because five options represent a moderate level of response granularity and permit a neutral response. The Flesch-Kincaid of the initial items and instructions was 6.4, indicating that a 6th-grade reading level was required.
The initial item pool was distributed to a panel of six external experts for content validation. These panelists, who were not involved as authors in this study, were selected for their expertise in SDT or lactation. All experts had an academic background. For each item, feedback was sought on the clarity and relevance. Experts were also invited to give feedback on whether additional items were necessary to encompass a concept fully. A content validity index was calculated for each item (I-CVI), and items with an I-CVI less than 0.8 were eliminated (Lynn, 1986). A full-scale content validity index (S-CVI) for the 37 retained items was 0.93, exceeding the standard for excellent content validity (Polit & Beck, 2021). An additional item was added after content validity testing based on the recommendation from one expert, but was removed in the exploratory factor analysis due to low factor loading, and is not included in the final version of the instrument.
The parsed item list was then field tested amongst the population for whom it was created: lactating individuals. Twenty-three participants meeting the criteria to participate in the study were asked to provide feedback on the clarity and appropriateness of the items and instructions. Participants identified no issues or suggested changes, and the instrument was not further revised after this stage. Therefore, survey responses from these 23 participants were included in the first phase of data collection described below. The use of expert content validation helped reduce potential measurement bias in item clarity and relevance.
Maternal satisfaction with lactation
Maternal satisfaction with lactation was measured using a single item asking participants, “How would you rate your overall breastfeeding experience?” on a 10-point Likert scale from “absolutely awful” to “absolutely wonderful” (Oggero & Wardell, 2022).
Edinburgh Postnatal Depression Scale
Depressive symptoms were assessed using the 10-item Edinburgh Postnatal Depression Scale (EPDS), an instrument that has been widely used and validated in the postpartum population (Park & Kim, 2023).
Breastfeeding exclusivity
Exclusive breastfeeding was measured by asking participants, “Has the infant you are currently breastfeeding ever had infant formula?” Those indicating yes were categorized as non-exclusively breastfeeding, while those who indicated no were exclusively breastfeeding. The World Health Organization (WHO, 2021) definition of exclusive breastfeeding is defined as solely breastfeeding with the exclusion of all other food and drinks, even water. However, this survey did not assess complementary food and fluid intake, given the inclusion of parents of infants older than 6 months.
Data Collection
The instrument was validated based on data collected during two separate periods. In the first phase, a sample of participants completed an online survey administered by PsychData between January and May 2023. In the second, participants completed an online survey administered by Qualtrics between August and November 2023. The survey software change between phases was due to amendments in institutional access. Before beginning the survey, participants were presented with information about the study outlining the purpose, procedures, risks, and benefits of participation. Consent was obtained electronically, with participants indicating their agreement by proceeding with the survey.
Email addresses were obtained for gift card incentive distribution. To enhance confidentiality, they were not linked to the survey data and participants were given the choice to create a new email address or to not participate in the drawing for the gift card. No other identifying data were collected from participants. Study data were downloaded by the principal investigator directly from PsychData and Qualtrics and stored on a password-protected computer that was accessed only by the principal investigator.
Data Analysis
Data were coded and analyzed using SPSS (Version 27) or SPSS (AMOS) for confirmatory factor analysis. The data were screened pre-analysis to assess accuracy, completeness, and fittingness between the analysis procedure and the data. Participant responses were removed from the data set if participants did not complete at least half of the questions. Response variability for each multi-item measure included in the survey was calculated, and cases with zero variability were removed. Additionally, cases with missing responses for any items on the LPNS were removed from the data set. Cases with missing data on other variables were not removed from the data set, and values for missing data were not estimated. Instead, cases with missing data were not included in any analysis for which they did not have a complete response. For example, if a participant did not provide an answer for all 10 items on the EPDS, a total EPDS score was not calculated, and their response was not included in any of the analyses that used EPDS scores.
Descriptive statistics were used to describe the demographics and clinical characteristics of the sample and examine homogeneity between exclusively and non-exclusively breastfeeding participants. A Chi-square test of independence was used for nominal and ordinal variables (gender, race, ethnicity, education level, previous lactation experiences), and independent t tests for continuous variables (participant age, infant age).
Exploratory factor analysis using principal axis factoring was conducted to identify the factor structure of the initial 38 items (Costello & Osborne, 2005). Factor extraction and retention were determined through various strategies, including examination of the scree plot, parallel analysis, and theoretical congruence. Oblique (Promax) rotation was used to determine item quality and reduction. Items with low factor loadings, poor internal consistency reliability, or conceptual incongruence were eliminated individually. In the separate sample, model fit was analyzed using the chi-square statistic, root mean square error of approximation (RMSEA), a comparative fit index (CFI), and a Tucker-Lewis Index (TLI). Modification indices, including standardized regression weights and standardized residual covariances, assisted in re-specification to improve model fit (Byrne, 2016). Internal consistency reliability was examined by calculating Cronbach’s alpha for the final full scale and each subscale. The cutoff for acceptable internal consistency reliability of a new scale was set at ≥ 0.70 (Nunnally, 1978). To examine construct validity, bivariate correlations between LPNS subscale scores, EPDS scores, and maternal satisfaction with lactation were carried out using Pearson’s r. Independent t tests were used to compare mean LPNS scores between the exclusively and non-exclusively breastfeeding cohorts.
Results
Characteristics of the Sample
The demographics and clinical characteristics of the sample are presented in Table 2. These characteristics are displayed for the total sample and further stratified by exclusively breastfeeding and non-exclusively breastfeeding participants, as well as by participants in the exploratory and confirmatory factor analysis phases. Among the total sample, 12 (1.9%) participants identified as non-female. Within this subgroup, the mean LPNS total score was 50.2 (SD = 2.19), with subscale scores of 16.33 (SD = 2.06) for competence, 17.67 (SD = 2.64) for relatedness, and 16.2 (SD = 3.01) for autonomy. The mean EPDS score for non-female participants was 6.33 (SD = 3.26), and the mean maternal satisfaction with lactation was 7.63 (SD = 1.41).
Sample and Subsample Demographics (N = 634).
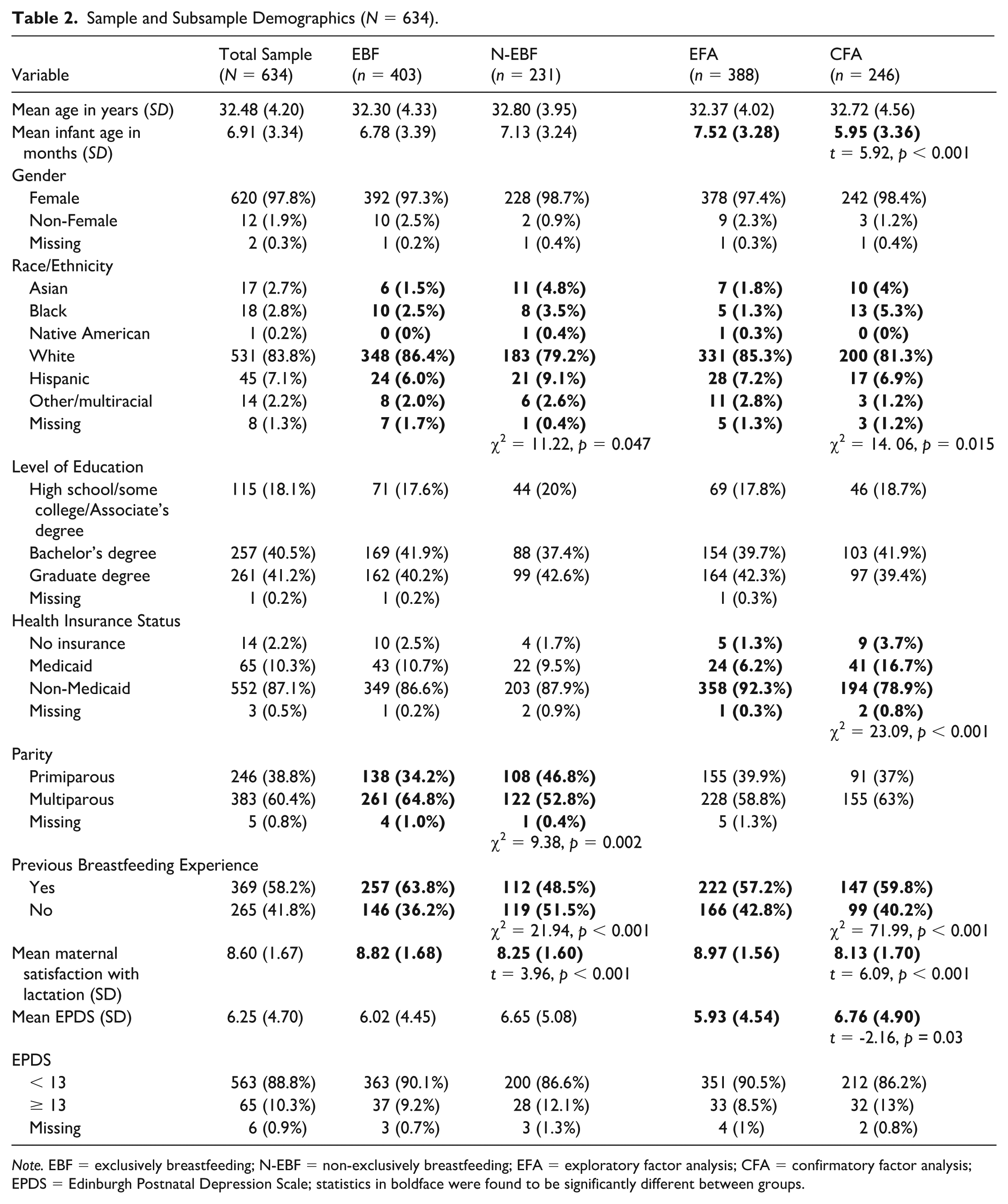
Note. EBF = exclusively breastfeeding; N-EBF = non-exclusively breastfeeding; EFA = exploratory factor analysis; CFA = confirmatory factor analysis; EPDS = Edinburgh Postnatal Depression Scale; statistics in boldface were found to be significantly different between groups.
Psychometric Evaluation of the LPNS
Exploratory factor analysis
Exploratory factor analysis utilized the sample from the first data collection phase to discern the underlying factor structure and reduce the number of items by evaluating factor loadings. The 38 content-validated items underwent principal axis factoring with Promax rotation. The Kaiser-Meyer-Olkin measure of sampling adequacy (0.903) and Bartlett’s test of sphericity (p = 0.000) supported the suitability of the sample for factor analysis. Examination of the scree plot, eigenvalues exceeding one, and parallel analysis converged on a three-factor solution congruent with the instrument’s theoretical underpinnings. This solution, elaborated in Table 3, explained 46.8% of the total variance. Items were removed based on low factor loadings, internal consistency reliability, and theoretical/conceptual congruence, resulting in a 19-item instrument.
Factor Loadings of LPNS Items After Principal Axis Factoring.

Note. LPNS = Lactation Psychological Needs Scale; Items in boldface are retained in the final 12-item instrument
Reverse-coded items. Extraction method: principal axis factoring. Rotation method: Promax with Kaiser normalization.
The three identified factors contained items reflecting competence, relatedness, and autonomy. This alignment with the a priori structure of the final instrument suggests preliminary support for its construct validity.
Confirmatory factor analysis
Confirmatory factor analysis using Maximum Likelihood Estimation was performed on the sample collected from the second data collection phase to evaluate the data’s fittingness with the exploratory model. Fit indices included in this study are the chi-square statistic, RMSEA, CFI, and TLI. Norms and observed values for each of these indices are presented in Table 4. In this sample, the assumption of multivariate normality was violated, even after removing outlier cases. After the best-fitting model was identified, a Bollen-Stine bootstrap adjustment was used to correct for potential overestimation of the chi-square’s significance due to the multivariate nonnormality.
Goodness-of-Fit Results and Model Re-Specification Decisions.
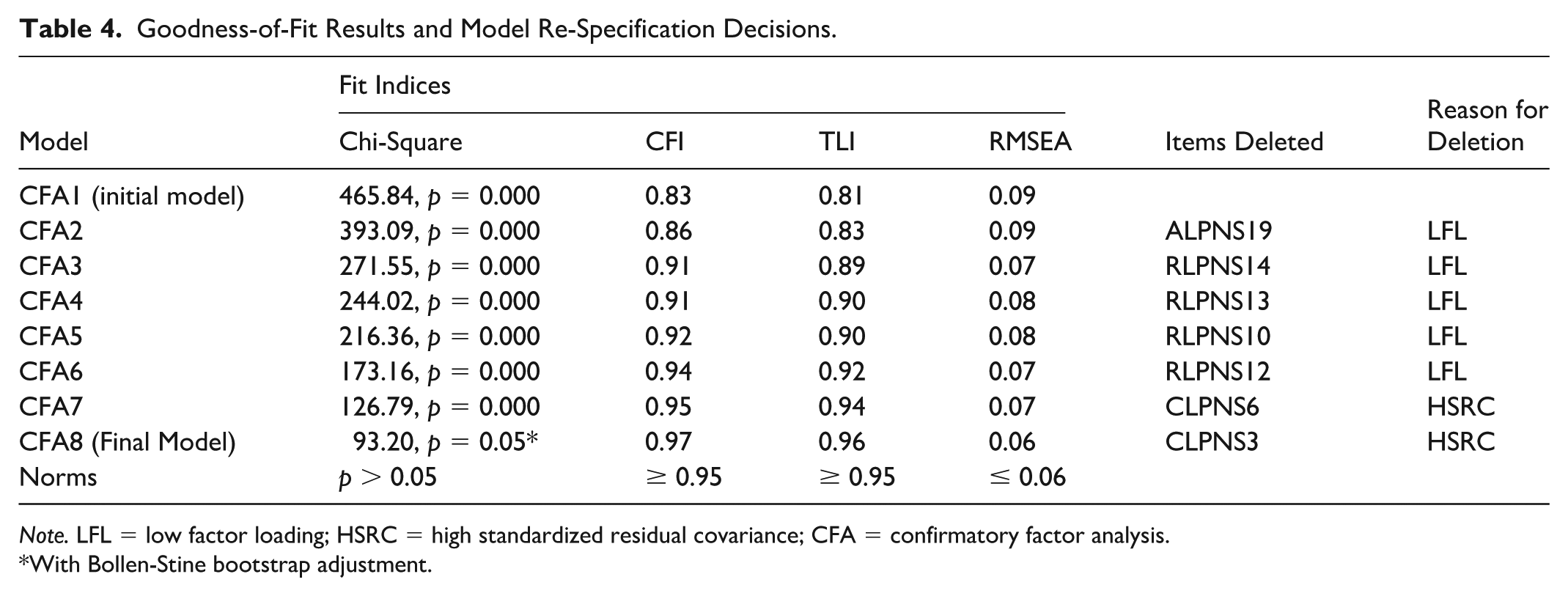
Note. LFL = low factor loading; HSRC = high standardized residual covariance; CFA = confirmatory factor analysis.
With Bollen-Stine bootstrap adjustment.
The initial model did not yield acceptable results for a well-fitting model. Post-hoc modifications were undertaken to improve the model’s fittingness and to create a more parsimonious model. Model re-specification was carried out considering factor loadings, covariance modification index, standardized residual covariances, and theoretical congruence. Problematic items were removed in a stepwise fashion. The resulting final model (Figure 2) demonstrated excellent model fit (Table 4). All standardized regression weights were > 0.6 and significant. As hypothesized, the competence items loaded well on Factor 1, the relatedness items on Factor 2, and the autonomy items on Factor 3. The confirmatory factor analysis confirms that the LPNS has 12 items with three dimensions. Possible scores on the final instrument range from 12–60, with higher scores indicating greater psychological need satisfaction. For each subscale, scores ranged from 4–20, with higher scores indicating greater satisfaction of the specific psychological need for that subscale.
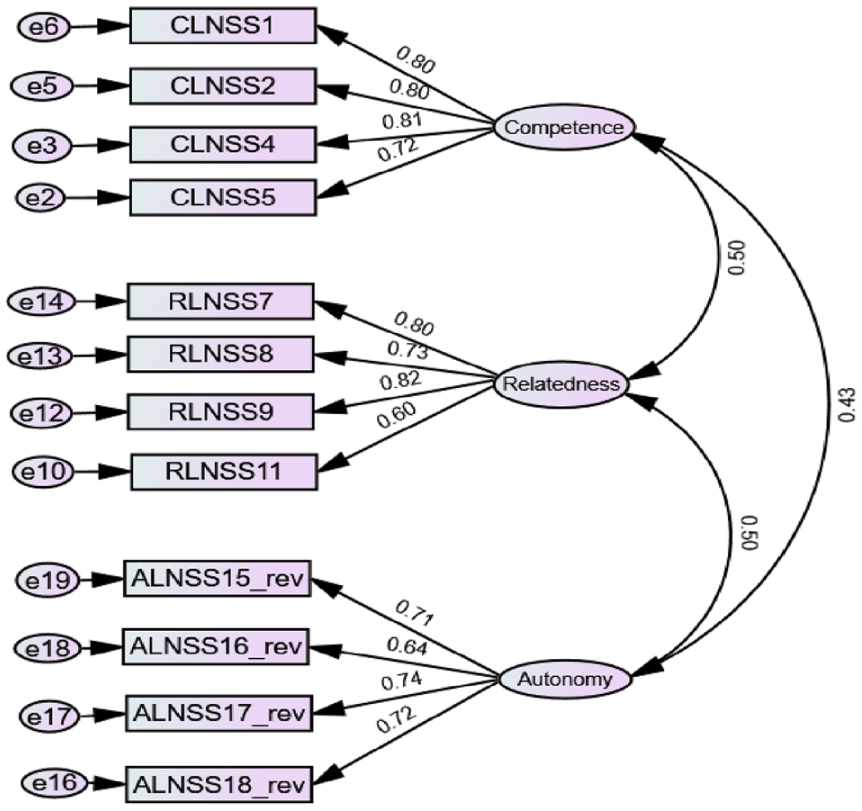
Confirmatory factor analysis results of final 12-item LPNS.
Construct validity and internal consistency reliability
Internal consistency reliability was calculated using Cronbach’s alpha. The total LPNS internal consistency reliability was 0.8. Additionally, each subscale demonstrated adequate reliability (Table 5). Bivariate correlations (Table 5) were used to establish the construct validity, indicating that the instrument measures the construct it is designed to measure. Each of the subscales was positively correlated with one another. Each subscale was negatively correlated with EPDS scores and positively correlated with maternal satisfaction with lactation. Independent t tests revealed significant differences in mean LPNS total and subscales scores between exclusively and non-exclusively breastfeeding participants in the expected direction (Table 6).
Variable Means, Correlations, and Reliability.
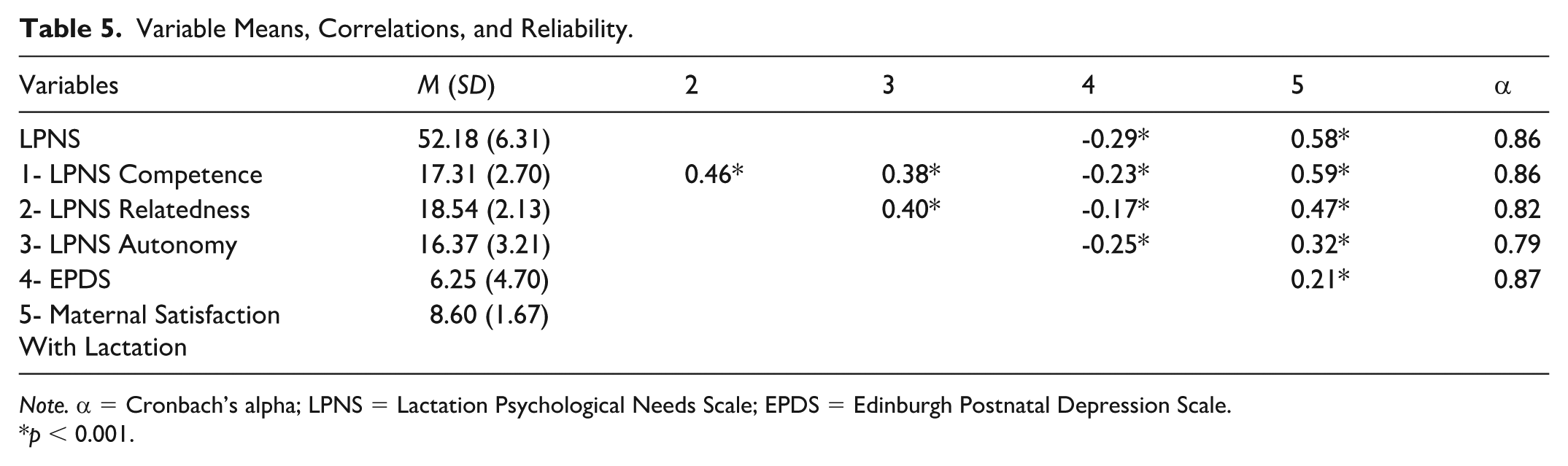
Note. α = Cronbach’s alpha; LPNS = Lactation Psychological Needs Scale; EPDS = Edinburgh Postnatal Depression Scale.
p < 0.001.
Comparison of Variable Means by Breastfeeding Exclusivity.
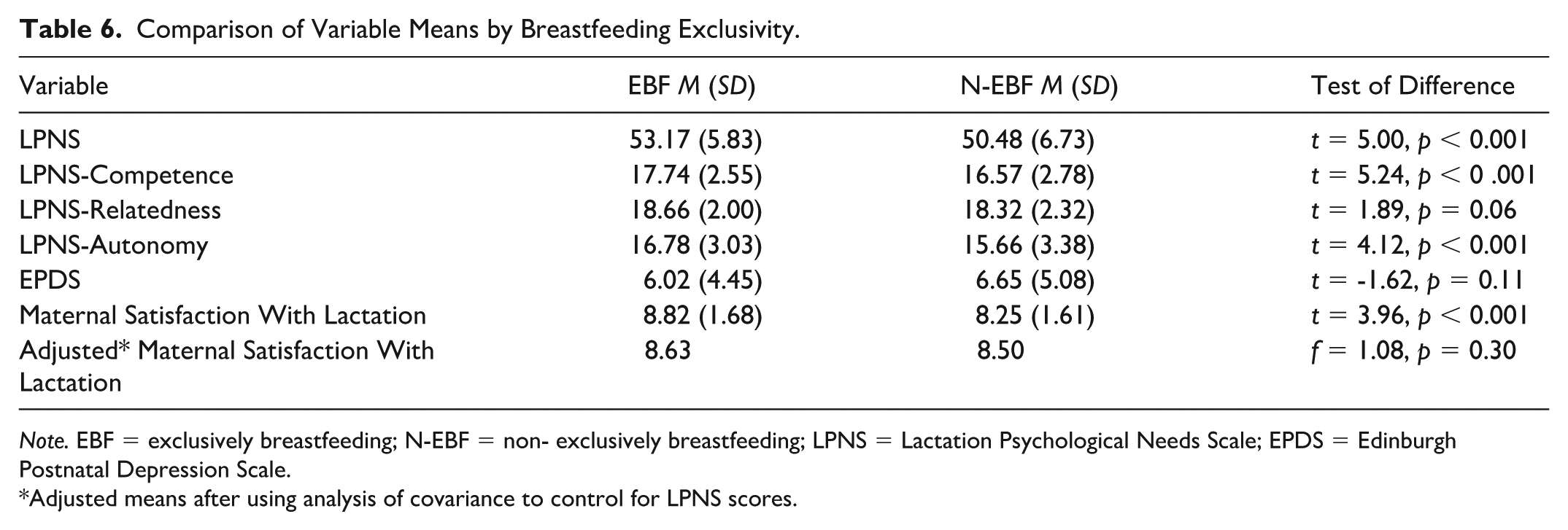
Note. EBF = exclusively breastfeeding; N-EBF = non- exclusively breastfeeding; LPNS = Lactation Psychological Needs Scale; EPDS = Edinburgh Postnatal Depression Scale.
Adjusted means after using analysis of covariance to control for LPNS scores.
Discussion
A novel instrument measuring psychological need satisfaction among lactating individuals appears preliminarily valid and reliable. Exploratory and confirmatory factor analyses revealed a three-factor structure that aligns with the basic psychological needs identified in SDT: autonomy, competence, and relatedness. The intercorrelations between these subscales support the psychological needs’ distinct yet interconnected contributions.
This study contributes to the expanding knowledge on applying SDT to health behaviors, and extends the application to lactation. As hypothesized, exclusively breastfeeding participants demonstrated higher LPNS scores, and greater satisfaction with lactation than participants who combined breastfeeding and formula feeding, supporting the scale’s construct validity. Autonomy nurtures intrinsic motivation, competence turns intention into effective action, and relatedness provides the social support that sustains effort. When all three needs are satisfied—reflected in higher LPNS scores—exclusive breastfeeding is more likely to persist. Accordingly, SDT offers a compelling lens for understanding and ultimately improving breastfeeding practices.
Psychological need satisfaction may play a meaningful role in shaping postpartum emotional experiences. While the observed associations between need satisfaction and depressive symptoms were directionally consistent with our hypotheses based on Self-Determination Theory, their small-to-moderate magnitude indicates that psychological need satisfaction explains only a modest proportion of the variance in depressive symptoms in this sample. Nevertheless, this pattern highlights the importance of addressing psychological needs in lactation support interventions while acknowledging that additional factors contribute to postpartum mood.
The inclusion of participants who did not identify as female is also noteworthy. While this subgroup represented a small proportion of responses, their participation is significant because of historical underrepresentation in research. Descriptive analysis of their responses provides some initial insight into their experiences; however, given the small sample size, inferential analysis was not possible, and findings should be interpreted with caution. Future research with diverse samples is needed to better understand the psychological need satisfaction and lactation experiences of gender-diverse individuals.
This study is highly relevant to contemporary sociocultural dynamics of lactation in the United States. In 2022, the American Academy of Pediatrics issued a policy statement strengthening the language of their breastfeeding recommendation (Meek & Noble, 2022). Previously, they recommended infants be breastfed for “1 year and beyond,” which was amended to “2 years and beyond.” This recommendation was rooted in acknowledging the health benefits but also responded to concerns of parents who felt unsupported in breastfeeding after the first year (Tchaconas et al., 2018). Paradoxically, some may view the recommendation as unnecessary societal pressure, or feel that 2 years is unrealistic with the challenges of contemporary parents (Campoamor, 2022). In the landscape of breastfeeding in the United States, our study takes a crucial step toward prioritizing the needs of parents. By exploring the emotional dimensions of the maternal experience and the autonomy felt in infant feeding choices, we contribute valuable insights to the broader dialogue on supporting parental well-being in the face of evolving cultural norms and systemic shortcomings.
Future research should strengthen and expand the utility of the LPNS. Prospective studies are needed to establish predictive validity by determining whether early LPNS scores forecast breastfeeding exclusivity and continuation at later postpartum timepoints. The LPNS’s temporal stability can be evaluated through test-retest reliability. Additional, future research is needed to test the LPNS in diverse populations and varied cultural contexts.
Limitations
Several limitations should be considered when interpreting the findings. The recruitment strategy, which predominantly involved participants recruited through La Leche League USA, limits the study’s generalizability. Participants recruited through an organization that advocates for breastfeeding are likely more inclined to feel positively toward breastfeeding. Consequently, the responses and conclusions of this study may not reflect the viewpoints of those with negative or neutral perspectives on breastfeeding. The sample’s lack of demographic diversity represents another limitation to the external validity of the LPNS. Participants in this study were primarily White, highly educated, and had a non-Medicaid health insurance plan, similar to a previous study that recruited through La Leche League (Keim et al., 2022).
During our confirmatory factor analysis, we opted for a nuanced approach involving model refinement. This process was guided by statistical indices and theoretical considerations, allowing us to fine-tune the instrument's underlying structure. However, it is essential to acknowledge that this study's validation process remains incomplete, as part of the customary psychometric validation process involves a confirmatory procedure (Tabachnick & Fidell, 2013). While our exploration has enriched our understanding of the instrument's structure, a dedicated confirmatory analysis in an independent sample is warranted to solidify its structure and enhance its overall validity.
While this study yielded a concise and practical tool with 12 final items, it is crucial to acknowledge limitations inherent in the pursuit of parsimony. The recommendation to start with a substantial number of intentionally overlapping items to retain the best-performing ones has undoubtedly enhanced the instrument’s efficiency and feasibility. However, the brevity may come at the expense of some conceptual richness that a more extensive instrument could have preserved.
Conclusion
This study developed and preliminarily validated an instrument rooted in SDT’s basic psychological need satisfaction. Our findings contribute to the literature by addressing a gap in existing paradigms and exploring the simultaneous measurement of autonomy, competence, and relatedness in the context of lactation. Ultimately, the theoretical insights gained from LPNS can be translated into actionable strategies to develop interventions to positively influence the breastfeeding outcomes and psychological well-being of lactating individuals.
Supplemental Material
sj-docx-1-jhl-10.1177_08903344261430141 – Supplemental material for Development and Validation of the Lactation Psychological Needs Scale
Supplemental material, sj-docx-1-jhl-10.1177_08903344261430141 for Development and Validation of the Lactation Psychological Needs Scale by Kelsie R. Barta, Misty M. Richmond, Becky Spencer and Sandra K. Cesario in Journal of Human Lactation
Footnotes
Acknowledgements
We would like to thank the research participants for their contributions to this work, Drs. Marcus Fagan and Thomas Guffey for their assistance with statistical analyses, and La Leche League USA for their assistance in distributing study recruitment materials.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Sigma Theta Tau Beta Beta Houston Chapter, Jesse H. & Mary Gibbs Jones Research Grant.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: At the time this study was conducted, Kelsie Barta was a doctoral student in the Nursing PhD program at Texas Woman’s University. Misty Richmond was the chair of her dissertation committee, and Becky Spencer and Sandy Cesario were members of her dissertation committee.
Supplemental Material
Supplementary Material may be found in the "Supplemental material" tab in the online version of this article.