
Abstract
Infant food allergies present significant challenges for breastfeeding families, who often receive conflicting information and inadequate support when implementing elimination diets. This article examines current research on protein transfer in human milk and proposes evidence-based approaches to managing suspected food allergies while preserving breastfeeding. Recent studies demonstrate that food proteins transfer into human milk with consistent timing patterns across multiple allergens, typically peaking within 2 hours of maternal ingestion and clearing within 6 to 8 hours. This understanding challenges conventional recommendations for extended elimination periods and supports more targeted dietary modifications. When appropriate trigger foods are completely removed from the maternal diet, infant symptoms typically begin improving within 72 to 96 hours, with most cases showing resolution within days to weeks, depending on symptom severity. Effective management requires a comprehensive assessment that evaluates infant factors, including gut microbiome development, medical history, feeding patterns, and oral function, alongside maternal nutritional status and mental health. Elimination diets should be viewed as short-term interventions requiring intensive monitoring to prevent nutritional deficiencies and psychological burden. Successful resolution of infant allergic symptoms can be enhanced by interprofessional collaboration between pediatricians, allergists, dietitians, International Board Certified Lactation Consultants (IBCLCs), or other lactation support providers, and mental health professionals. IBCLCs play a crucial role in supporting milk production and maternal wellbeing during elimination periods. The research-informed approach we present here prioritizes family-centered care, recognizing that each management strategy must be individualized based on unique circumstances, symptoms, and goals while providing families with evidence-based information and comprehensive support throughout their journey.
Keywords
Background
A new mom pops up on my screen for a telelactation appointment; she's bouncing a 2-month-old. She greets me with tired eyes, messy hair, and a forced smile. I introduce myself, an IBCLC and Registered Dietitian, I tell her it's nice to meet her and her sweet baby. When I ask how she is doing, I see her brain start to search for an answer; she gives an uncomfortable chuckle and then bursts into tears. I wish so badly that I could reach through the video and give her a hug. I give her time and space to cry. She hasn't said a word yet, but I have already learned a great deal about where she is at. I let her know that I see her and understand those tears more than most, as I, too, have been there. By letting that emotion out, she already seems a little lighter. She takes a deep breath, and we begin discussing what she has gone through over the past long 60 days. What happened during birth and pregnancy, what the journeys with her other children have been like, and what she has worked through with other medical professionals. I collect all the puzzle pieces about her baby's symptoms, when they first began, the timing of when they occur, and more. She tells me that her baby had a frenectomy at 4 weeks old and that she has been working with bodyworkers and a tongue-tie savvy International Board Certified Lactation Consultant (IBCLC). This mother has been doing everything right, yet her baby is still struggling and uncomfortable, and mom is still confused and exhausted. We then discuss infant food allergies; I start to see lightbulbs go off in her head as I educate her on current research. I lay out options and different approaches along with their pros and cons. With the knowledge I provide her, she feels more empowered and is able to make an informed decision. She starts to cry again. This time, the tears are different. They are not helpless and painful tears; they are tears of relief that she might be on track to help her baby. They are tears of joy that her breastfeeding journey doesn't have to end here. I tell her that I am truly proud of her and that I am here for her as she navigates this challenging road. I give her tools and resources to make sure she has food to eat so that her body and baby are nourished. She has a plan, and she sees a way forward.
This scenario is a small glimpse into what a family might come to us with. After meeting with thousands of parents dealing with infant food allergies, the commonality seems to be that families are confused by conflicting information and that they are desperate to resolve their baby's symptoms.
Standard Approach
The incidence of infant food allergies, regardless of feeding method, presents ongoing diagnostic and management challenges. Among infants who are exclusively breastfed, various organizations indicate that less than 3% develop allergic reactions to cow's milk proteins specifically (Academy of Breastfeeding Medicine, 2011; Koletzko et al., 2012). However, clinical observations suggest this may be an underestimate, as diagnostic difficulties contribute to potential underreporting.
One significant issue is that infant food allergy definitions remain poorly defined and difficult to officially diagnose. Diagnostic codes for some non-IgE mediated allergies did not exist until 2016, creating historical gaps in accurate reporting (Cianferoni, 2020). Misdiagnosis is common due to the inability to effectively test a variety of allergies in children under 1 year of age. Furthermore, these statistics are often limited to cow's milk protein reactivity, omitting other allergens such as soy, egg, wheat, and other proteins that can trigger reactions.
Non-IgE mediated food allergies encompass delayed reactions that affect the skin as well as the gastrointestinal tract, and often do not have the same trigger foods as their IgE-mediated counterparts (Zhang et al., 2021). These conditions include food protein-induced enterocolitis syndrome (FPIES) and food protein-induced allergic proctocolitis (FPIAP), which can present with symptoms of rash, eczema, reflux, stool changes, colic, and failure to thrive (Nowak-Węgrzyn, 2015).
Current standard care typically involves a recommendation to remove cow's milk protein for several weeks when potential food reactivity is suspected (Academy of Breastfeeding Medicine, 2011). However, parents rarely receive adequate support on how to implement elimination diets accurately and sustainably.
When symptoms do not improve or parents cannot sustain the dietary changes, a hypoallergenic formula recommendation often follows. Medical professionals frequently lack the resources to provide comprehensive guidance on targeted allergens to avoid while still preserving breastfeeding, making the transition to formula appear necessary. However, with the numerous benefits that human milk provides, a more nuanced approach is needed to support lactation sustainability rather than assuming breastfeeding must end.
The intent of an elimination diet is both diagnostic and therapeutic. This rapid response window serves as a critical decision point: if symptoms improve, this confirms the eliminated food is the trigger and continued avoidance is necessary. Conversely, if no improvement occurs within 3–5 days, the excluded food is unlikely to be the culprit, allowing families to resume normal diet or trial a different allergen (Lozinsky et al., 2015). This approach minimizes unnecessary restriction while efficiently identifying true triggers.
Research-Based Solutions
Understanding current research on protein transfer and timing across multiple food allergens is fundamental to developing effective elimination diet strategies. Recent proteomic analysis has revealed that not all ingested proteins enter human milk, and those that do transfer show significant individual variability (Zhu et al., 2019). Importantly, studies across different food proteins demonstrate remarkably consistent timing patterns for both transfer and clearance.
For cow's milk proteins, mass spectrometry analysis shows that beta-lactoglobulin and beta-casein fragments peak in human milk at 2 hours post-ingestion and become undetectable at 6 hours (Picariello et al., 2019). Early peanut protein research by Vadas et al. (2001) first detected peanut allergens in nearly half of participants within the first 2 hours post-consumption. More recent research confirms that peanut allergens can be detected as early as 10 minutes after ingestion, with peak levels within the first hour, and that clearance follows the same 6 to 8 hour timeline (Bernard et al., 2014).
Foundational wheat protein studies by Troncone et al. (1986) and Chirdo et al. (1998) demonstrated that gluten protein was detected in 41 out of 53 breast milk samples within 2 to 4 hours after ingestion, and, after a 3-day wheat-free diet, gliadin was not detectable in any samples. Similarly, earlier egg protein studies found that ovalbumin concentration peaks and clears from human milk within 8 hours of consumption, with daily consumption showing no accumulation over time (Palmer et al., 2008).
These consistent findings across diverse protein sources suggest that similar transfer and clearance patterns may exist for other dietary proteins in human milk. The uniformity of this pattern, with proteins typically clearing within 6 to 8 hours regardless of the food source, challenges conventional recommendations for extended elimination periods and supports more targeted, time-limited approaches to dietary modifications during lactation. Figure 1 illustrates the timeline of dietary protein transfer into human milk and the corresponding patterns of infant reactivity and symptom resolution based on the above research.
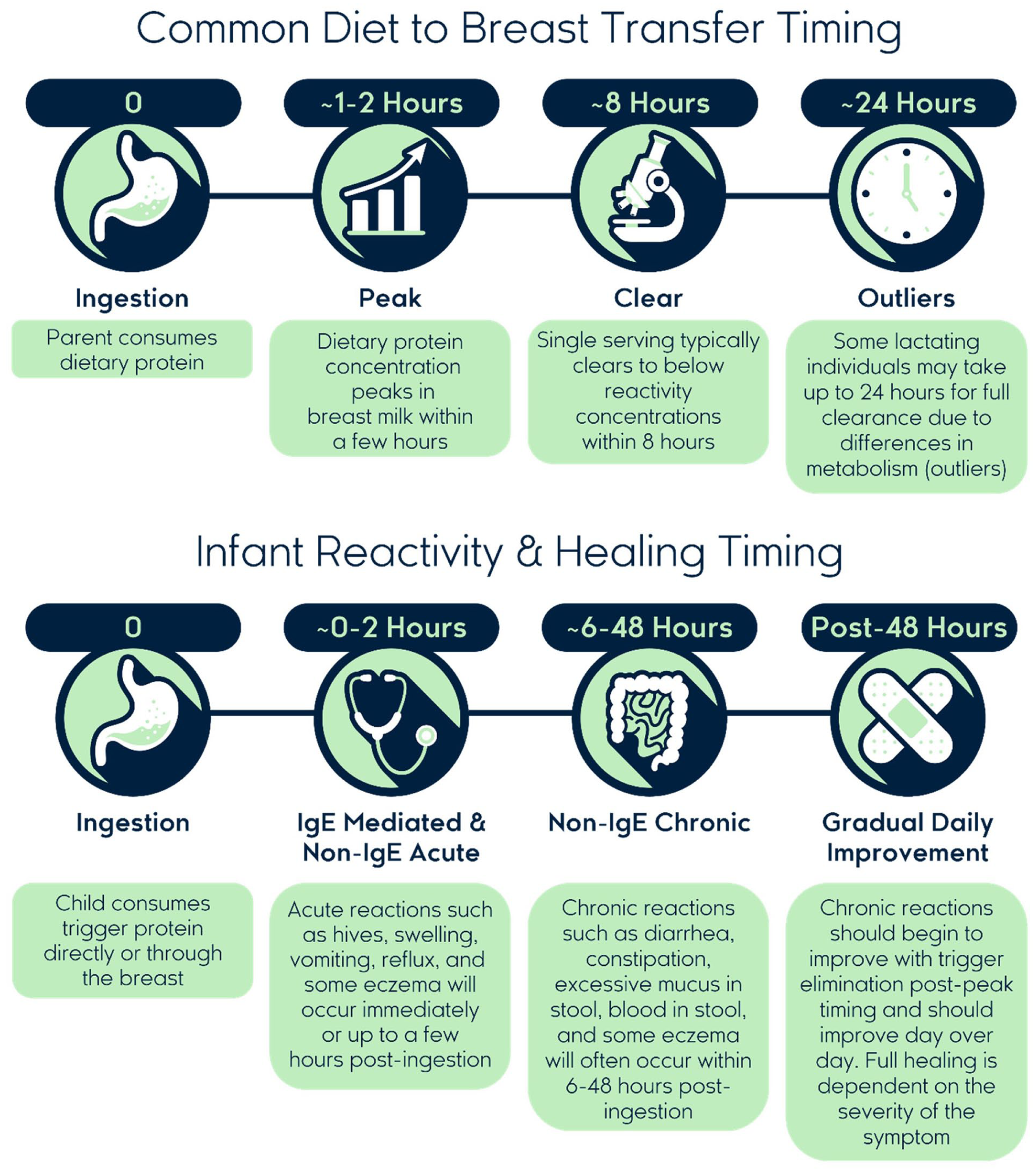
Timeline of dietary protein transfer to breastmilk and infant food allergy symptom patterns.
This research supports evidence-based elimination protocols that focus on the complete removal of specific triggers for shorter durations rather than broad, restrictive diets that may unnecessarily limit maternal nutrition for extended periods. The consistent clearance timing across multiple allergens provides a scientific foundation for more precise and sustainable elimination strategies.
Research indicates that when appropriate trigger foods are completely removed from the maternal diet, infant symptoms typically begin to improve within 72 to 96 hours, with most cases showing complete resolution within days to weeks of elimination diet implementation dependent on the symptom severity (Lozinsky et al., 2015).
Elimination diets during lactation should never be intended as long-term interventions. Extended elimination diets pose significant risks, including maternal nutritional deficiencies, potential impacts on human milk nutritional adequacy, and substantial mental health burden for the entire family (Dupont et al., 2012). Research indicates that elimination diets can lead to feeding difficulties and nutritional concerns, emphasizing the need for careful monitoring and support (Vandenplas et al., 2021).
Comprehensive Assessment
Effective management requires a holistic assessment that prioritizes ruling out other contributing factors before implementing diet changes. Assessment should include evaluation of the dyad’s medical history, feeding patterns, and oral function. Understanding symptom characteristics, including timing, duration, and specific presentation details, provides crucial distinguishing information.
A thorough maternal assessment encompasses medical and mental health status, stress levels, nutritional history, and any previous experiences with disordered eating patterns, as any form of restricted eating, such as an elimination diet, can be triggering for these individuals. For lactating parents, factors such as pumping schedules, milk storage practices, breast milk substitute use, and work arrangements, may influence both elimination diet feasibility and milk supply maintenance.
To facilitate systematic clinical decision-making, IBCLCs can utilize a structured framework that guides assessment and management approaches (Figure 2). This framework emphasizes the importance of comprehensive initial evaluation and establishes clear criteria for determining whether cases can be managed with IBCLC support or require immediate referral to the healthcare team.
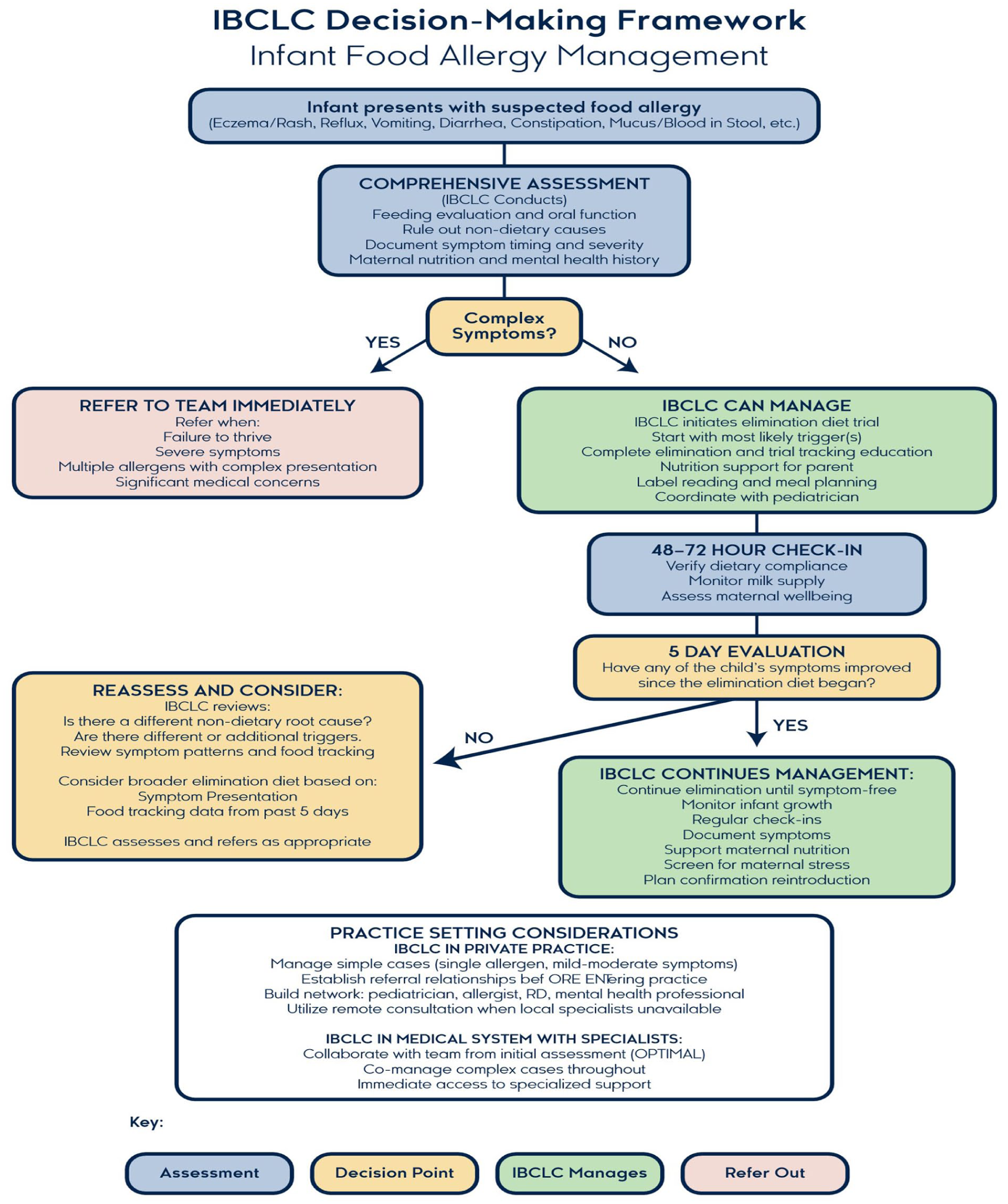
The IBCLC decision-making framework for infant food allergy management.
Monitoring and Support
Successful elimination diet management requires intensive follow-up to reassess symptoms and maternal nutrition status. Clinical protocols should include regular nutritional assessments, milk production monitoring, and mental health screening for lactating parents. Evidence-based reintroduction schedules help minimize the duration of restrictive diets while ensuring infant safety. Regular tolerance reevaluation should involve multidisciplinary healthcare teams, when appropriate, with systematic documentation of symptom patterns, dietary adherence, and infant growth parameters to guide ongoing management decisions.
Interprofessional Collaboration
Thorough care of infant food allergies requires coordination between multiple healthcare disciplines, including pediatricians, allergists, dietitians, lactation specialists, and mental health professionals. This team approach ensures that both immediate symptom management and long-term nutritional and developmental needs are addressed.
IBCLCs play a crucial role in protecting and supporting lactation during elimination diets. Expertise in milk production physiology, feeding assessment, and maternal support enables lactation consultants to provide essential guidance during challenging elimination periods. Regular lactation assessment helps identify potential impacts on infant and maternal health, as well as milk supply, allowing for prompt intervention when needed.
Summary
Current research supports a more layered approach to infant food allergy management that prioritizes comprehensive assessment, evidence-based elimination protocols, and ongoing professional support. Understanding the variability in protein transfer, timing of symptom resolution, and individual family factors enables more targeted and sustainable interventions.
No two management strategies should look identical, as every family's journey involves unique circumstances, symptoms, and goals. The initial approach should avoid extremely restrictive elimination diets and instead implement targeted removals based on complete assessment findings, if deemed fitting. While elimination diets can be effective when properly implemented with adequate support, they require careful monitoring to prevent nutritional deficiencies and psychological burden.
Families deserve evidence-based information, practical resources, and emotional support throughout the diagnostic and management process. With appropriate interventions, many families can successfully navigate infant food allergies while maintaining their breastfeeding goals.
The growing body of research on protein transfer, improved diagnostic capabilities, and innovative support technologies offers hope for more effective and family-centered approaches to infant food allergy management. Continued research and clinical innovation will further improve outcomes for families facing these challenging situations.
Footnotes
Acknowledgements
The authors acknowledge Peter Paullin for creating the figure, and the researchers and families who have shared their experiences to advance understanding in this field.
Author Contributions
Taylor H. Silver: Conceptualization; Writing - original draft; Writing - review & editing.
Trillitye Paullin: Conceptualization; Resources; Supervision; Visualization; Writing - review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors are employees of Free to Feed, Inc., a company that provides educational support and resources to families navigating infant food allergies. This relationship represents a potential conflict of interest with respect to the research, authorship, and/or publication of this article.