
Abstract
Background:
Individuals with hypertensive disorders of pregnancy are at a significantly increased risk for chronic hypertension and premature cardiovascular disease. Although breastfeeding may have cardiovascular benefits, those with hypertensive disorders of pregnancy tend to have lower rates of breastfeeding initiation, duration, and exclusivity. A deeper understanding of their breastfeeding experiences is necessary to inform effective interventions that support lactation.
Research Aim:
This study aimed to explore breastfeeding challenges, enablers, and factors influencing breastfeeding confidence among individuals with hypertensive disorders of pregnancy.
Method:
This study employs a descriptive, qualitative approach. Semi-structured telephone interviews were conducted between 2 and 8 months postpartum with a convenience sub-sample of 18 individuals enrolled in a pilot randomized controlled trial of a breastfeeding support intervention in Quebec, Canada. The interviews were audio-recorded, transcribed, and analyzed using qualitative content analysis. Data were coded and grouped under three categories related to the main interview questions (breastfeeding challenges, enablers, and factors influencing breastfeeding confidence).
Results:
Perinatal complications, struggles with milk supply, high rates of formula supplementation, and lack of consistent or skilled breastfeeding support challenged early breastfeeding experiences. Breastfeeding enablers included hands-on support with feedings, accessible breastfeeding information and support, and being determined to breastfeed. Discouragement to breastfeed from family or health professionals diminished breastfeeding confidence whereas learning from the breastfeeding experiences of others and positive reinforcement for breastfeeding efforts helped build breastfeeding confidence.
Conclusions:
Skilled, proactive lactation support targeting breastfeeding confidence may help optimize breastfeeding outcomes among individuals with hypertensive disorders of pregnancy, potentially mitigating their longer-term cardiovascular risks.
Keywords
Background
Hypertensive disorders of pregnancy (HDP), including chronic hypertension, gestational hypertension, and preeclampsia/eclampsia (Brown et al., 2018), affect up to 15% of pregnancies and remain one of the leading causes of maternal and neonatal morbidity and mortality worldwide (Garovic et al., 2020). Beyond its immediate health implications, HDP is associated with a two- to three-fold increased risk for the development of maternal chronic hypertension and premature cardiovascular disease (CVD; Coutinho et al., 2018; Wu et al., 2020). Although this elevated incidence of CVD may be mediated in part by other cardiometabolic risk factors (Ju et al., 2022; Patti et al., 2018), there is mounting evidence of accelerated endothelial dysfunction and vascular impairment initiated in pregnancy that persists months to years post-HDP (Dayan et al., 2018; Grand’Maison et al., 2016). As HDP is now a well-recognized sex-specific risk factor for premature CVD, targeted postpartum interventions promoting maternal heart health are warranted (Lui et al., 2019; Yu et al., 2020).
Robust evidence for the significant maternal cardiovascular benefits of breastfeeding is mounting (Jacobson et al., 2018; Nguyen et al., 2019; Peters et al., 2017). A recent meta-analysis involving data from more than 1.1 million parous individuals found that any lactation was associated with relative risk reductions of 11%, 14%, 12% and 17% for CVD, congestive heart disease, stroke and fatal CVD events, respectively, with greater risk reductions for longer lifetime durations of breastfeeding (Tschiderer et al., 2022). These findings support the role of lactation in “re-setting” the metabolic changes of pregnancy via mobilization of stored fat and glucose to fuel milk production, re-establishing normal lipid and glucose homeostasis (Stuebe, 2015; Stuebe & Rich-Edwards, 2009). Emerging research has also uncovered direct effects of oxytocin on the cardiovascular system, including vasodilation, inhibition of inflammation, and angiogenesis of smooth muscle and endothelial cells (Jankowski et al., 2020; Reiss et al., 2019).
Although breastfeeding has been shown to significantly reduce blood pressure and metabolic markers following HDP-affected pregnancy (Countouris et al., 2016; Magnus et al., 2023; Yu et al., 2020), investigators consistently find that individuals with HDP have lower rates of breastfeeding initiation and duration than their normotensive counterparts (Burgess et al., 2021; Horsley et al., 2022; Strapasson et al., 2018). Several risk factors associated with HDP may contribute to suboptimal breastfeeding outcomes, including underlying diabetes, primiparity, preterm birth, and Cesarean delivery (Burgess, 2021; Cordero et al., 2012; Demirci et al., 2018; Leeners, 2005). However, the relationship between HDP and breastfeeding remains understudied, and there is scant literature on the breastfeeding experiences of individuals with HDP. Burgess et al. (2021) underscored the need for more qualitative studies to explore perceived barriers to breastfeeding and how healthcare professionals can better support and encourage lactation among those with HDP. As breastfeeding self-efficacy (i.e., confidence in one’s perceived ability to breastfeed), has been identified as a potent modifiable predictor of breastfeeding success (Brockway et al., 2017; Galipeau et al., 2018), a deeper understanding of factors influencing breastfeeding confidence among those with HDP may also help inform their needs for breastfeeding support. Therefore, the aim of this study was to explore breastfeeding challenges, enablers, and factors influencing breastfeeding confidence, among individuals with HDP.
Key Messages
Although individuals with hypertensive disorders of pregnancy may benefit in particular from the cardio-protective effects of lactation, little is known about their breastfeeding experiences and needs related to lactation support.
Individuals with hypertensive disorders of pregnancy reported breastfeeding challenges related to insufficient milk supply and lack of skilled breastfeeding support, particularly during the postpartum hospital stay.
Readily available hands-on support, guidance for enhancing milk supply, encouragement, or self-motivation to persist with breastfeeding were perceived as key enablers for enhancing breastfeeding success.
Method
Design
This descriptive study was a qualitative content analysis of interview data (Graneheim & Lundman, 2004), embedded within a single-center pilot randomized controlled trial (RCT) of a breastfeeding self-efficacy-based intervention (BSEI) to improve lactation and blood pressure outcomes post-HDP (BP-MOM study, ISRCTN.com, # 18352227, registered on January 29, 2019), in Montreal, Quebec, Canada. This analysis was designed to gain more in-depth information from a sub-sample of BP-MOM participants about their specific needs and perceptions related to breastfeeding support, to help inform a larger trial. Ethical approval was obtained from the Research Ethics Board of the McGill University Health Centre (study protocol # BP-MOM 2019-4726, Aug 8, 2019). Details of the BP-MOM pilot trial intervention and outcomes are published elsewhere (Dayan et al., 2023).
Setting
This study was conducted in the province of Quebec, Canada, a high-income setting with a multi-cultural population and universal health insurance coverage. Whereas breastfeeding initiation rates are high (89%) in Quebec, they remain below the Canadian national average for exclusive (26% vs. 36%) or any breastfeeding (54% vs. 62%) up to 6 months (Ricci et al., 2023). In Quebec, postpartum hospitalization for those with HDP is typically 24 hours longer than the standard 24- to 36-hour stay for uncomplicated vaginal birth or 72 hours for Cesarean delivery. Breastfeeding support resources freely available to all families include in-hospital perinatal nurses with basic breastfeeding training, telephone or home-visit contact by a community-based nurse within 72 hours of hospital discharge, government-sponsored booklets and websites on postpartum care, and community-based breastfeeding peer support programs. International Board-Certified Lactation Consultants (IBCLCs) may be accessed for free in some hospitals or community-based settings, or as fee-for-service consultants. The BP-MOM study was conducted in a tertiary university teaching hospital with a high-risk obstetrics department that included follow-up visits at a specialized Maternal Cardiovascular Health clinic.
Sample
All participants in this study were enrolled in the BP-MOM pilot trial during their postpartum hospital stay and provided written consent to be contacted for a future interview about their perceptions of breastfeeding support. Inclusion criteria for the BP-MOM study included a diagnosis of HDP (Brown et al., 2018), age ≥ 18 years, singleton live birth delivered at ≥ 34 weeks’ gestation, oral and written fluency in English or French, phone and internet access, and initiated breastfeeding or milk expression. Exclusion criteria included maternal intensive care unit stay of > 24 hours, severe psychiatric illness, and maternal or infant contraindications to breastfeeding or conditions known to interfere with successful lactation (e.g., breast reduction surgery; infant with a cleft palate). Participants randomly assigned to the control group received usual hospital and community breastfeeding support, whereas those in the BSEI group additionally received support from an IBCLC trained in BSE theory consisting of up to two in-hospital counseling sessions and a telephone counseling “booster” session at 3 months. The counseling sessions involved an assessment of the participants’ current breastfeeding goals and performance as well as their level of breastfeeding self-efficacy using the 14-item Breastfeeding Self-Efficacy Scale–Short Form (Dennis, 2003), followed by tailored strategies to address any lactation challenges as well as low areas of breastfeeding confidence. The IBCLC also telephoned the BSEI participants weekly for the first 6 weeks post-hospital discharge to check in and follow-up on any breastfeeding issues and, was available via telephone or email for retroactive support to 6 months postpartum, as needed. All participants who completed the final study follow-up measures at 12 months were given a $25 CAN ($18 US) pharmacy gift care as a token of appreciation.
For this sub-study, research staff invited a convenience sample of the participants to take part in the interview during their recruitment into the BP-MOM pilot study or when scheduling their follow-up visits at the Maternal Cardiovascular Health clinic. Participants in both the intervention and control groups were eligible. The research staff described the study aim and interview process, and if the participant agreed, scheduled the interview to take place when the participant was at least 2 months postpartum. We aimed to interview up to 18 of the pilot study participants (i.e., 40% of the sample) as Hennink et al. (2017) found that code saturation is typically reached after nine qualitative interviews where a minimum of 16 are needed to approach meaning saturation.
Data Collection
Audio-recorded, semi-structured telephone interviews were conducted between September 2019 and February 2020 by author CB, a bilingual (English/French) research assistant with a bachelor’s degree in psychology. CB received training in interviewing skills from senior team members, who provided additional feedback on the interview transcripts. Participants were reminded that they would be asked about the breastfeeding challenges they had experienced to date and the kinds of support they found helpful, and that their answers would be kept strictly confidential. Breastfeeding in this study was defined as feeding directly at the breast or providing expressed human milk. The interview guide (see the online Supplemental Material) was developed by two senior members of the research team and piloted with a BP-MOM study participant to ensure clarity. Interview questions explored the participant’s current breastfeeding status, any significant challenges to breastfeeding, types of breastfeeding support received or desired, and factors that increased or decreased their confidence to breastfeed. Sociodemographic data were obtained at recruitment into the BP-MOM study. The interviews lasted an average of 26 minutes (range = 15–37 min). CB transcribed the audio recordings verbatim in their source language and verified the transcripts for accuracy. All transcripts were anonymized and de-identified and stored in password-protected files only accessible by the research team.
Data Analysis
Demographic data were summarized using descriptive statistics, with mean (SD) for continuous variables and numbers (%) for categorical data. The interview data were analyzed using a qualitative content analysis approach with constant comparisons (Elo & Kyngas, 2008) by three bilingual members of the research team (SS: a senior researcher with expertise in qualitative research and lactation support; SC: a doctoral student in nursing with a personal history of breastfeeding; and CB). Transcript data were coded in their source language (English or French) through a combined deductive and inductive process (Elo & Kyngas, 2008). First, a general categorical framework was used to group the interview data under three categories corresponding with the study’s main interview questions (i.e., breastfeeding challenges, enablers, and factors influencing breastfeeding confidence). The transcripts were then read and reread to highlight words or phrases that reflected issues relating to each of these main categories. The highlighted words and phrases were assigned descriptive codes that were compared and merged across the first few coded transcripts to generate a preliminary coding framework (Saldaña, 2013). The framework was refined with each subsequent transcript by adding new codes as needed and grouping codes into broader sub-categories within each of the three main category headings. All transcripts were initially coded by SC or CB and then re-coded by SS. To enhance trustworthiness of the analysis, the coders met regularly to review the emerging categorical framework, collapse or reorganize codes and sub-categories as needed, and achieve consensus on the final data analysis structure. Recruitment was conducted concurrently with data coding, and we achieved saturation of emerging codes when our target sample was reached (Fusch & Ness, 2015).
The individual transcripts were stored and coded in Microsoft Word. Microsoft Excel was used to map the codes and sub-categories under the three main categories. Finally, representative quotations were extracted from the individual transcripts to illustrate each sub-category; French quotes were translated into English for publication purposes.
Results
Characteristics of the Sample
Eighteen participants were interviewed between 2 and 8 months postpartum, and most were still breastfeeding at the time of their interview. Ten participants (58%) were in the control group in the pilot study (their codes denoted by “C”) and eight (44%) were in the intervention group (denoted by “I”). Participants were aged 29–49, all reported being non-smokers, and almost all were university-educated. The majority were diagnosed with preeclampsia, approximately half of the participants had a Caesarean birth and one-third had pre-existing or gestational diabetes. The participants’ infants were born between 35–40.4 weeks of gestational age and weighed on average 3084 g. More than half the infants were placed on a hypoglycemia prevention protocol at birth and/or were supplemented with artificial milk at least once during their hospital stay (Table 1).
Characteristics of Participants (N = 18).
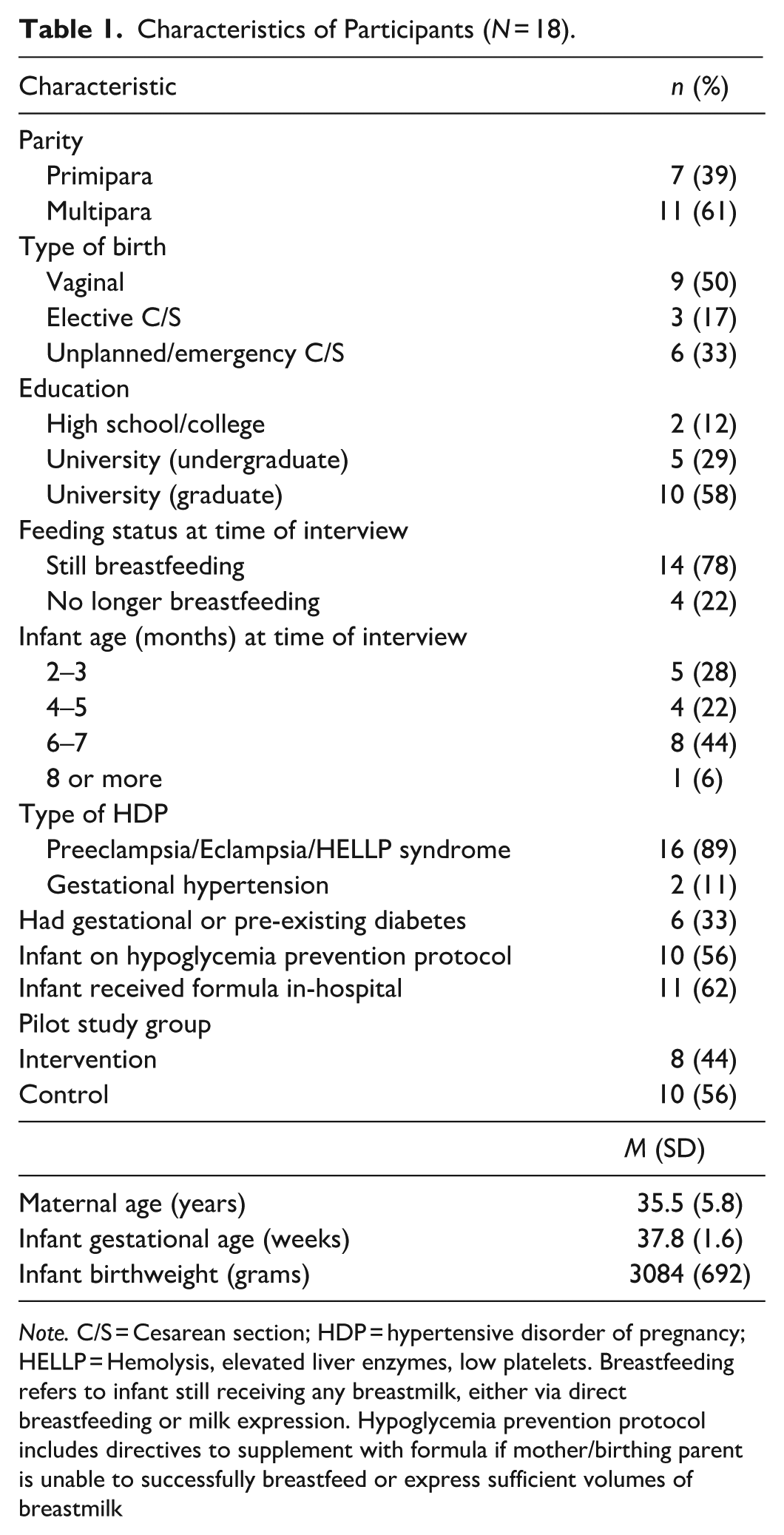
Note. C/S = Cesarean section; HDP = hypertensive disorder of pregnancy; HELLP = Hemolysis, elevated liver enzymes, low platelets. Breastfeeding refers to infant still receiving any breastmilk, either via direct breastfeeding or milk expression. Hypoglycemia prevention protocol includes directives to supplement with formula if mother/birthing parent is unable to successfully breastfeed or express sufficient volumes of breastmilk
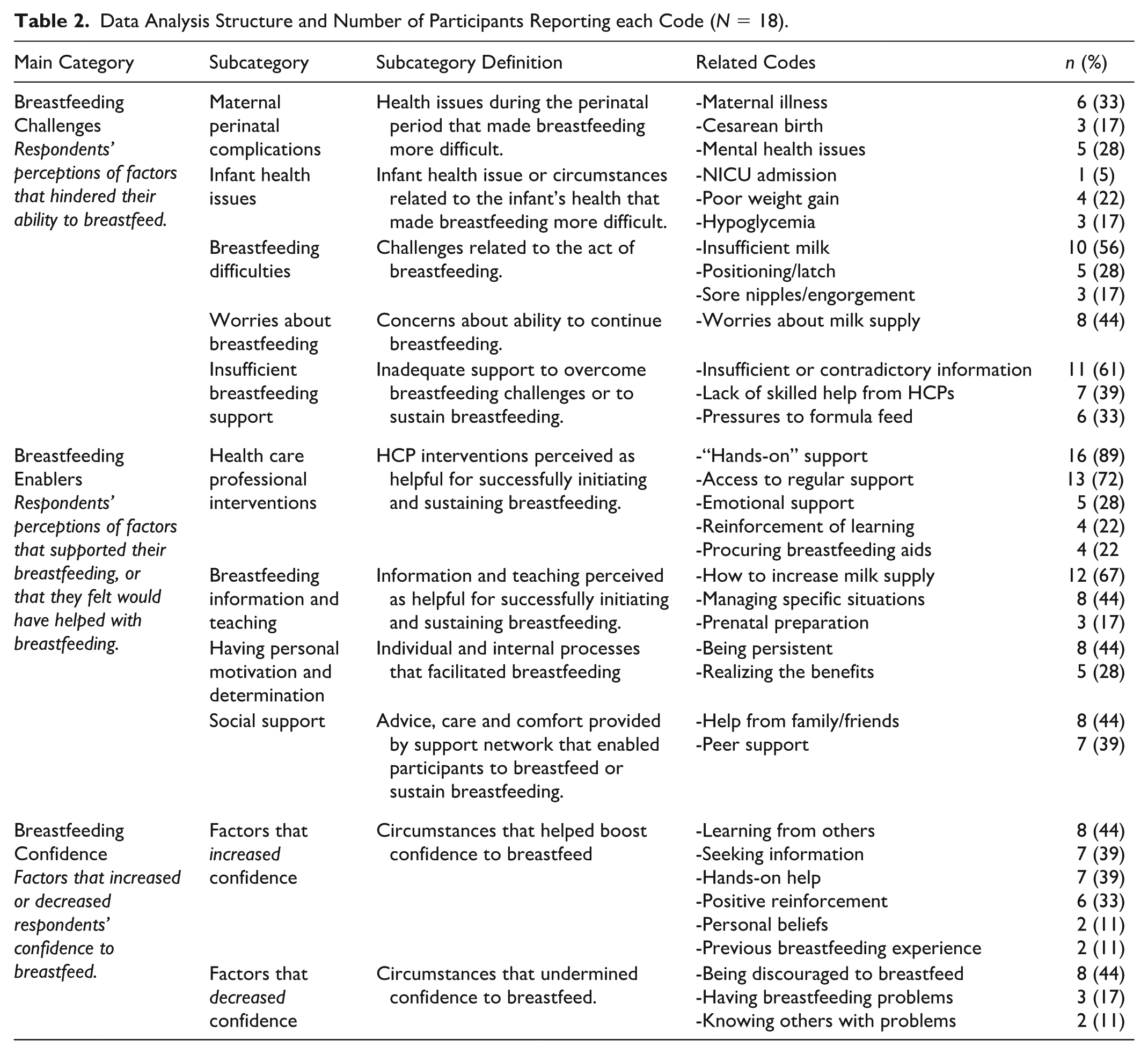
Categories
Coded findings were grouped into subcategories relating to the study’s main interview questions: (1) Breastfeeding challenges (factors that hindered participants’ ability to breastfeed); (2) Breastfeeding enablers (factors that either helped or would have been helpful to support breastfeeding), and (3) Breastfeeding confidence (factors that increased or decreased the participants’ confidence). The data analysis structure and number of participants who reported data related to each code are summarized in Table 2.
Data Analysis Structure and Number of Participants Reporting each Code (N = 18).
Breastfeeding Challenges
Maternal perinatal complications
Several participants described how their hypertensive condition interfered with the initiation of breastfeeding: “Because when you have high blood pressure, you don’t feel good after the birth, so to add on the stress of not being able to feed the baby properly, I think just makes the whole situation harder” (C-13). Pain, weakness and immobility associated with Cesarean birth further challenged early breastfeeding experiences. Some participants described how side effects of medications used to treat their high blood pressure or pre-eclampsia (e.g., dizziness, peripheral neuropathy) made breastfeeding more difficult: “I also had some neurological issues. . . . I had my left hand frozen, so that would be a side effect of labetalol” (C-10). One participant weaned at 7 months following treatment for deep vein thrombosis, a longer-term risk of HDP: “I stopped [breastfeeding] right away when I started taking heparin, but that was a misconception of mine.” (I-03). Five (28%) participants also identified mental health issues including anxiety or postpartum depression as significant challenges to breastfeeding: “I had a depression, so everything connected together, it was like impossible for me” (C-09).
Infant health issues
Infant-related breastfeeding challenges reported by participants included increased risk for hypoglycemia and poor weight gain. For example, as several factors associated with HDP (e.g., prenatal use of beta-blockers, maternal diabetes, preterm birth) enhance the risk for newborn hypoglycemia, many of the participants’ infants were placed on the hospital’s newborn hypoglycemia prevention protocol at birth. This often led to early formula supplementation that undermined breastfeeding plans, as reported by one participant:
For women with high blood pressure who, for example, have received treatment right from the start, the baby remains under surveillance. . . . So, I think that’s the challenge, right at the beginning . . . because she’s going to be forced to give the formula to her baby, even if there’s no drop in glucose. (I-05)
Several participants also described how poor infant weight gain resulted in the need for formula supplementation, contributing to early weaning in some cases: “She basically wasn’t gaining any weight, like I had to give her formula anyways, so I just kept with that one” (C-18). Infant admission to the neonatal Intensive Care Unit (NICU) at birth also disrupted the initiation of breastfeeding, as reported by one participant whose infant required monitoring due to maternal prenatal hypercalcemia (a risk factor for preeclampsia): “My baby was in intensive care for the first 2 days, and within 2 hours of being born, he was fed formula” (C-11).
Breastfeeding difficulties
Only a few participants reported experiencing major problems with common breastfeeding issues, including sore nipples, engorgement, or difficulties with latch-on (related to flat nipples, or tongue-tie). However, more than half the participants (61%) identified insufficient milk supply as an issue, with several describing experiences with low milk production despite concerted attempts to enhance milk production: “So even though I took medication, domperidone, fenugreek and all that, my milk supply was still low” (C-18). Descriptions of poor supply included indicators such as excessive infant crying, low milk volumes when pumping, and infant weight loss: “Our doctor told us also for her 4 months appointment, and she was lighter than I thought. . . . She was in the 40th percentile. . . . I am worried now that I won’t be able to meet her demands” (I-04). Participants further described how worries about milk supply added stress to their postpartum experience: “The C-section [Cesarean section] was difficult for the first few days and then it was good, but this issue [insufficient milk] is like something permanent . . . a challenge that is always with you. This is the most difficult part for me” (C-15).
Insufficient breastfeeding support
Insufficient or contradictory information from healthcare professionals (HCP) about breastfeeding was a commonly reported challenge: “Due to HDP complications] I stayed a little longer in the hospital but the nurses told you different things, the pediatrician, luckily it wasn’t my first [breastfeeding experience] so I knew a little more, and I was more confident” (I-01). Several participants described feeling unprepared for the potential challenges of breastfeeding post-HDP: “I also was hospitalized on and off for a lot of my pregnancy . . . no one had mentioned to me that because I have preeclampsia and because I’m having a C-section that it will be harder to breastfeed” (C-18).
Several participants discussed how breastfeeding support was not readily available during the postpartum hospital stay: “At the hospital, the nurses came to see me for a maximum of 5 minutes and would then leave. . . . I would have liked someone to stay with me just for breastfeeding, until the end to show me the signs” (C-09). One intervention group participant with flat nipples noted a lack of skilled support “until I met [the study’s IBCLC] who came to see me at the hospital, she was the one who encouraged me . . . but the hospital nurse, the delivery room nurse, and the [hospital’s] lactation consultant didn’t help me too much” (I-05). A third of the participants further reported feeling pressured by HCPs to supplement with formula, for example when staff lacked skills to address their feeding issues: “and then every feeding, they were just telling me, ‘well if she’s not latching, just give her the bottle” (C-18). For some, pressures to supplement in the face of feeding struggles continued post-discharge from family members: “My mother-in-law, it’s like ‘You could give her bottles. . . . You look tired, you should stop breastfeeding’” (I-01).
Breastfeeding Enablers
HCP interventions
Almost all the participants described the critical importance of receiving hands-on breastfeeding help and reassurance from HCPs including hospital and/or community nurses, a lactation support specialist, or (in one case) their pediatrician. Technical interventions that were judged to be helpful included physical help with positioning and observational assessment of infant latch and suckling: “She [hospital’s IBCLC] showed us how to check to make sure the baby was swallowing, and different positions to hold the baby that would encourage her to eat more comfortably” (C-13), as well as assisting with milk expression:
[The study IBCLC] was able to show me how to hand express. . . . It was useful to have somebody show me that technique and just give me the reassurance that I did have plenty of colostrum and things at that stage were looking like the way they should. (I-07)
Practical support from HCPs also included procuring and demonstrating breastfeeding aids including nipple creams, breast pumps or supplemental nursing systems; and monitoring the infant’s weight gain: “The [community] nurse gave me the supplemental system, the syringe, and everything” (C-15).
Most participants acknowledged the importance of accessible and pro-active breastfeeding support from HCPs, as noted by an intervention group participant: “She [study IBCLC] called every week to see how it was going, answered any of my questions, just having access to her was reassuring” (I-04). Participants cited multiple ways in which HCPs were (or could be) consistently available, including regular “check-in” rounds by postpartum hospital nurses; follow-up home visits by community nurses; or having email, phone or virtual access to lactation specialists. As one participant who had an emergency c-section for preeclampsia described:
[Hospital support] was crucial, because I was exhausted, I was stressed, and in pain, and so having nurses around us even in the night helping me when the baby was crying to show us, to watch how I was feeding and correct it, was immensely helpful. And when we came back home, we had the [community] nurse coming to see us and my milk had come already and it was very reassuring to hear from her that everything was okay, that the baby is feeding well, that the latch is proper. (C-17)
Several participants described how caring attitudes and emotional support provided by HCPs helped them overcome their breastfeeding struggles: “I kind of flipped out at one point, and then I talked to [a lactation] consultant about it and she had some reassuring words, so that kind of gave me hope again” (C-11).
Breastfeeding information
Many participants discussed the importance of receiving breastfeeding information, especially on how to enhance milk supply. Helpful information included pumping and storage of human milk; expectations for milk volumes; and strategies to increase supply, for example infant re-positioning, food and herbal supplements, feeding frequencies, breast massage and co-sleeping with baby. Other useful information included tips for managing blocked ducts, engorgement, and sore nipples: “The majority of my friends don’t breastfeed, they gave up. They didn’t have the same kind of knowledge that I did, like [the study IBCLC] gave me. So, it really helped encourage me to persevere through it [sore nipples]” (I-02).
Participants reported sourcing breastfeeding information from a wide variety of resources including hospital and community-based HCPs, written materials (e.g., pamphlets, government-issued booklets), videos, and online websites or breastfeeding groups. A few participants also raised the importance of receiving accurate information prenatally to prepare for potential breastfeeding challenges: “Something reliable that has the same basic information to read before they [women with HDP] give birth, because it definitely helped me having read some of the things before” (I-06).
Having personal motivation or determination
Many participants discussed how important it was to remain committed and persistent with breastfeeding to help endure challenges: “I really wanted to breastfeed. I mean like formula was the last resort. To get my milk supply, I pumped, and I pumped. . . . I think that also makes a difference, right?” (I-02). Helpful personal strategies for persisting with breastfeeding included setting longer-term goals, being patient while “getting the hang of it” and keeping volumes of supplemental feeds to a minimum. Several participants discussed how knowing the benefits of breastfeeding helped them maintain their determination to continue, including the maternal cardiovascular benefits: “One thing that I would have never known was the benefit regarding your blood pressure, if it wasn’t for the fact that I was in the study. . . . We always talk about the benefits to the baby” (I-08). Other rewards of breastfeeding reported by participants included enjoying the close contact with their infant, the convenience and being able to use breastfeeding to “take a break.”
Social support
Several participants described how family members or friends provided emotional and/or practical support that enabled them to manage their breastfeeding challenges. Family members were supportive by helping the participants to “calm down,” helping latch the infant, reinforcing teachings given by HCPs, or freeing the participant to breastfeed by doing tasks around the house: “I have my mom here and I think she is my number one support. . . . Having somebody physically here helping me and also getting resources, like reading material, to know how to feed and to increase the milk flow” (C-12). Friends who were also breastfeeding provided advice, resources—including websites for information and support—and helpful products including nipple creams or galactagogue teas. Some participants noted the importance of sharing stories with other new parents in breastfeeding peer support groups, with one suggesting an online group for those with HPD: “A Facebook group or something like that where all of us who have the same condition, the high blood pressure, preeclampsia and breastfeeding could join together” (I-04).
Breastfeeding Confidence
Factors that increased confidence
Participants most commonly identified seeking breastfeeding information from various sources or learning from family or friends (who had positive breastfeeding experiences) as factors that boosted their breastfeeding confidence:
I think friends’ advice who also had babies were helpful and made me feel more confident, like what to ask for. . .just having people share their best tips that worked for them gave me confidence that I could do it. (C-13)
Several participants reported that receiving hands-on breastfeeding support increased their breastfeeding confidence, as described by one participant: “At the hospital, when [the study IBCLC] came, she completely boosted my confidence when she helped me. . . . After that, I was struggling when I got home and the nurse from the CLSC [the community clinic] came and she boosted my confidence again” (I-04). Participants also described how their confidence levels increased when they received positive reinforcement that feedings were going well (e.g., validation that their infant was latched well or was gaining weight) and encouragement for their efforts from HCPs or others: “It was my friend . . . and my husband. They tried to keep my morale up, even when I was tired, and encouraged me not to give up. They would say ‘Oh, you made 60 ml today, bravo!’” (C-14). A few participants also noted personal factors that contributed to their confidence, for example, previous experience with breastfeeding or having strong beliefs in the importance of breastfeeding: “I got this very strong conviction from the nurses that really helps me now to resist this pressure of ‘Oh, you should try giving some formula or just switch to formula all together, it is so much easier.’” (C-17).
Factors that decreased confidence
The most commonly-reported factor undermining breastfeeding confidence was being actively discouraged by others to breastfeed, especially in response to challenges with milk supply: “My partner was too impatient when he heard the baby cry, saying ‘Come on, let’s give him the bottle, it’s not working’ and my mother was the same, ‘Give him the bottle, you don’t have enough milk’” (C-11). Some participants felt indirect discouragement from HCPs who did not actively promote breast- over bottle-feeding: “She (MD) was like telling me ‘You’re doing the best you can, it doesn’t matter if you bottle-feed or not’” (C-18), or from others who were uncomfortable with public breastfeeding: “Having people look at me like, ‘oh, shouldn’t you cover yourself up a bit more?’” (I-08). Finally, a few participants noted that their confidence decreased when they experienced breastfeeding difficulties or knew others who had encountered breastfeeding problems: “I think knowing a handful of people that had trouble breastfeeding made it a bit more stressful” (I-06).
Discussion
This study explored breastfeeding challenges and enablers among a sub-sample of individuals with HDP enrolled in a pilot RCT of a breastfeeding self-efficacy-based support intervention. The most-commonly reported challenges related to insufficient milk supply and lack of consistent and skilled breastfeeding support. Readily available hands-on support, guidance for enhancing milk supply and being encouraged to persist with breastfeeding were perceived as key to overcoming early lactation difficulties. Although these findings are not unique to individuals with HDP, they underscore the importance of targeted support for optimizing breastfeeding success among populations at greater risk for perinatal complications that may challenge breastfeeding. Our findings also help validate the appropriateness of key components of our pilot study’s BSEI intervention, including skilled in-hospital assessment and counseling, pro-active community-based follow-up, and a focus on breastfeeding confidence-building.
Previous authors have identified milk supply challenges and lower rates of breastfeeding duration and exclusivity among those with HDP (Burgess, 2021; Demirci et al., 2018; Horsley et al., 2022; Strapasson et al., 2018). Insufficient milk (whether “real” or “perceived”) is associated with a constellation of risk factors across multiple domains (e.g., maternity ward practices, biomedical, psychosocial) that may impede the onset or maintenance of lactation (Huang et al., 2021; Segura-Pérez et al., 2022). For example, half the study participants delivered via a Cesarean section and a majority also supplemented in-hospital with formula, which are both independent risk factors that may interfere with the establishment of milk supply (Li et al., 2021; Pérez-Escamilla et al., 2022). Previous studies have reported higher in-hospital supplementation rates among those with HDP as a result of maternal–infant separation due to Cesarean delivery, maternal sedation during postpartum seizure prophylaxis with magnesium sulfate, and/or maternal or infant ICU admission (Cordero et al., 2020; Strapasson et al., 2018). Our findings add that those with HDP may perceive more pressures to supplement their infants with formula due to increased risks for neonatal hypoglycemia, including prenatal exposure to maternal beta blockers (Bateman et al, 2016), maternal diabetes (Lin et al., 2021), and preterm birth (Arfandi et al., 2023).
Several biomedical factors may also explain higher reported rates of insufficient milk among those with HDP. For example, Demirci et al. (2018) hypothesized that the administration of diuretics for treatment of hypertension and/or HDP-related postpartum edema may interfere with the fluid balance required for lactogenesis. HDP risk factors include metabolic conditions including obesity, polycystic ovarian syndrome, and diabetes (Pan et al., 2021; Umesawa & Kobashi, 2017), which may compromise lactation via altered hormonal (e.g., insulin, prolactin) dynamics (Rassie et al., 2021). Preeclampsia is a multisystem inflammatory condition characterized by impaired vascularization of the placenta. Prenatal supplementation with the amino acid L-arginine has been shown to improve placental vascularization among those with HDP (Goto, 2021) as well as mammary gland vascularity and milk production in animal models (Ding et al., 2019; Sevrin et al., 2021), suggesting that the inflammation and anti-angiogenesis involved in HDP may negatively affect lactogenesis. Further research with objective measures of maternal milk volumes is needed to better understand the potential influence of HPD on lactation.
Our findings support that breastfeeding self-efficacy-focused support may be particularly helpful for overcoming breastfeeding challenges and boosting confidence related to lactation performance. Maternal breastfeeding confidence is consistently found to be protective against perceived insufficient milk and worries about infant hunger (Huang et al., 2021; Segura-Pérez et al., 2022; Vilar-Compte et al., 2022). Kent et al. (2020) found that reassurance and targeted advice from lactation consultants (e.g., increasing feeding frequencies; use of breast compression) reduced perceptions of insufficient milk. Educating both parents and their family members about normal infant behaviors, and regular infant weight checks, may reassure concerns about low supply (Huang et al., 2021; DiTomasso et al., 2022). Antenatal milk expression may further boost confidence in milk supply, enhance lactogenesis, and collect milk in anticipation of HDP-related complications that may delay breastfeeding initiation (Demirci et al., 2018). Sandsæter et al. (2019) found that breastfeeding helped compensate for maternal feelings of failure and guilt following pregnancy complicated by HDP, suggesting that effective lactation support may also contribute to maternal sense of mastery more broadly among those with high-risk pregnancies.
Although the study intervention did not include antenatal counseling, participants raised the importance of receiving prenatal information on potential lactation challenges associated with HDP, as well as the cardioprotective benefits of lactation. Individuals with HDP or other medically complex pregnancies are less likely to intend to breastfeed (Burgess et al., 2021; Kozhimannil et al., 2014), and Cordero et al. (2012) identified prenatal breastfeeding intention as the strongest predictor of breastfeeding initiation among individuals with severe preeclampsia. Many individuals with HDP are not aware of their longer-term cardiovascular risks (Burgess & Feliu, 2019; Pfaller et al., 2024), and knowledge that lactation may positively affect their lifelong cardiometabolic health may enhance breastfeeding intentions and perseverance in the face of lactation challenges (Ross-Cowdery et al., 2017). Prenatal counseling on the safety of HDP medications during lactation as well as tips for managing lactation in the event of potential HDP-related complications may also help families better prepare to initiate breastfeeding.
Participant perceptions of factors influencing their breastfeeding confidence and outcomes were consistent with breastfeeding self-efficacy theory. Derived from social cognitive theory (Bandura, 1977), breastfeeding self-efficacy is hypothesized to be influenced by four main sources of information: performance accomplishments, verbal persuasion, vicarious learning, and physiological/affective states (Dennis, 1999). Consistent with our findings, previous qualitative studies with the general population have found that mothers/birth parents prefer non-contradictory and realistic information about infant feeding; a continuity of breastfeeding support that is easily and flexibly available; and practical support and demonstrations, including being observed through a whole feed and receiving feedback on their breastfeeding techniques (Bengough et al., 2022; Rojas-García et al., 2023). Encouragement or discouragement of breastfeeding clearly influenced breastfeeding efforts, highlighting the key influence of positive reinforcement for helping to boost confidence and persistence with breastfeeding. Participants also valued learning about breastfeeding from their social network or breastfeeding support groups, reflecting the positive influence of peer support on breastfeeding outcomes (Chang et al., 2022). Online support groups for individuals with HDP may facilitate sharing of breastfeeding success stories and advice for managing lactation challenges (Reicher & Spatz, 2024). Finally, physical symptoms associated with HDP or its treatment may impede breastfeeding initiation, highlighting the need to assess and support physical recovery post-HDP. Contrary to calls for a more “hands-off” approach to breastfeeding support (Schafer & Genna, 2015), some participants appreciated direct physical assistance with lactation, perhaps due to their compromised health status.
Limitations
Participants were self-selected from a small sample of individual with HDP recruited into a single-site feasibility study of breastfeeding support. Participants may also have provided socially desirable responses related to their breastfeeding experiences, especially intervention group participants who were still receiving support from the study’s IBCLC. Each participant was interviewed only once and at varying stages postpartum, resulting in heterogeneous responses. Finally, interviews were conducted in both of Canada’s official languages (English or French) and coded in their source language, which may have biased the interpretation of some findings. However, all investigators involved in the analysis were bilingual, and a professional translation application (DeepL®) was used to support the translation of participant quotes into English.
Conclusion
As the cardiometabolic benefits of breastfeeding may mediate the longer-term CVD risks associated with HDP, interventions to enhance breastfeeding outcomes among those with HDP may have lifelong positive effects on both infant and maternal health. Tailored breastfeeding support for those with HDP can begin prenatally, and should include specific guidance for optimizing milk supply, ensure a continuity of skilled breastfeeding support post-hospital discharge, as needed, and link families with breastfeeding peer-support resources. More in-depth qualitative research with a greater diversity of individuals with HDP is needed to better understand how best to support lactation among this important obstetrical population.
Supplemental Material
sj-docx-1-jhl-10.1177_08903344251369419 – Supplemental material for A Descriptive Qualitative Study of Breastfeeding Challenges, Enablers and Confidence Among Women With Hypertensive Disorders of Pregnancy
Supplemental material, sj-docx-1-jhl-10.1177_08903344251369419 for A Descriptive Qualitative Study of Breastfeeding Challenges, Enablers and Confidence Among Women With Hypertensive Disorders of Pregnancy by Sonia Semenic, Sonia A. Castiglione, Carla Benea, Deborah Da Costa and Natalie Dayan in Journal of Human Lactation
Footnotes
Acknowledgements
The authors wish to acknowledge all the members of the BP-MOM pilot study team, as well as the individuals who generously gave their time to participate in this study.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by a Heart and Stroke Foundation (Quebec)-McGill University Early Career Professorship in Heart and Brain Health, and the McGill University Health Center Department of Nursing.
Disclosures and Conflicts of Interest
This paper’s second author (SC) is a doctoral student being co-supervised by the paper’s first author (SS). The authors declared no other potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary Material may be found in the “Supplemental material”tab in the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.