
Abstract
Background:
Human milk and colostrum have been well studied; however, limited data are available on the variations in macronutrient content when compared across different infant weight categories for infants with similar gestational ages.
Research Aims:
To compare the colostrum macronutrient content of participants who delivered term infants classified as small for gestational age, appropriate for gestational age, and large for gestational age.
Methods:
In this exploratory cross-sectional observational study (N = 252), colostrum (on postpartum Day 2) was collected and categorized by gestational weight group. The protein, fat, carbohydrate, and energy levels of colostrum were measured using a mid-infrared human milk analyzer. Values were dichotomized at the median and compared using logistic regression.
Results:
Median colostrum protein content was significantly higher in the small for gestational age (4.8 [IQR = 3–6.4] gr/dl) and large for gestational age (4.4 [IQR = 3.5–5.3] g/dl) groups compared to the appropriate for gestational age group (2.8 [IQR = 2.1–3.7] g/dl; p < 0.001). Median carbohydrate content was significantly higher in the large for gestational age group (5.3 [IQR = 4.2–6] g/dl) than appropriate for gestational age group (4.5 [IQR = 3.5–5.3] g/dl; p = 0.002). In multivariate analysis, being SGA or LGA was independently associated with higher milk protein content (OR 4.68; 95% CI [2.25, 9.77; p < 0.001; and OR 6.76; 95% CI [3.30, 13.87]; p < 0.001, respectively). Only being LGA was associated with higher carbohydrate content (OR 2.74; 95% CI [1.46, 5.16]; p = 0.002).
Conclusion:
Colostrum macronutrient content varies depending on whether the birthweight is small or large for gestational age. Studies are needed to investigate these potential associations and the clinical consequences of this relationship.
Key Messages
The colostrum of preterm infants varies from that of term infants, but we know less about how macronutrient content varies among term babies of different gestational sizes.
Colostrum protein levels are significantly higher in mothers of infants born small or large for gestational age compared to those born appropriate for gestational age.
Carbohydrate content in colostrum is significantly elevated in mothers of large for gestational age infants.
Birthweight for gestational age is associated with variations in colostrum macronutrient content, highlighting the need for further research into its clinical implications.
Background
Human milk is the gold standard nutrition for newborn infants because it meets their biological and physiological needs. It contains macro- and micronutrients, along with bioactive substances, including hormones, growth factors, enzymes, and immunoglobulins (Martin et al., 2016; Yi & Kim, 2021). Colostrum is the initial human milk produced by the breast in the first few days after birth, and it serves as complete nutrition for newborns. Typically expressed in only two 10 ml amounts per feeding, it contains a high concentration of proteins. The first nutritional support for an exclusively breastfed newborn is provided through colostrum; therefore, the nutritional content of colostrum holds important biological significance. Initiating breastfeeding immediately after birth and ensuring frequent breastfeeding is crucial for all infants (Adamkin, 2011).
The macronutrient composition of human milk is dynamic and can vary both within and between individuals (Paulaviciene et al., 2020; Thakur et al., 2021). Previous studies have demonstrated that this variability is influenced by several factors, including the gestational age at birth, postnatal age, gender, maternal body mass index (BMI), parity, mode of delivery, and maternal nutrition (Bulut et al., 2019; Burianova et al., 2019; Dizdar et al., 2014; Keikha et al., 2017; Mangel et al., 2020; Sahin et al., 2020). Most previous research has focused on examining the macronutrient content of human milk in the context of pregnancy complications, particularly prematurity. Reviews and meta-analyses on this topic have reported that the human milk of mothers with preterm infants contains higher levels of macronutrients and energy in the first days of life compared to that of term infants (Bulut et al., 2019; Gidrewicz and Fenton, 2014; Sahin et al., 2020). Although the mechanism of this difference and the benefits it provides have not been fully clarified, it is thought to be due to the high needs of the newborn during this period, facilitating adaptation to postnatal life (Li et al., 2022).
The macronutrient content of human milk has been extensively studied; however, the relationship between birthweight variations and the macronutrient content of human milk in small for gestational age (SGA) or large for gestational age (LGA) groups has not been thoroughly investigated. Infants born as SGA or LGA may demonstrate different metabolic demands and growth patterns compared to those born appropriate for gestational age (AGA; Dunn et al., 2021; Kosmeri et al., 2023; Zhang et al., 2024). Therefore, understanding how the macronutrient levels of colostrum vary according to birthweight for gestational age can provide insights into the tailored nutritional needs of birthweight alterations at both extremes, whether SGA or LGA infants.
Only a few studies have explored the macronutrient content of human milk from mothers of AGA and SGA infants (Arsić et al., 2012; Bobiński et al., 2013; Correia et al., 2023). In their study, Correia et al. (2023) found no differences between AGA and SGA groups in preterm infants, except for weak evidence of an association with lower fat content in infants with fetal growth restriction. Limited data exist comparing the nutritional content of human milk by categorizing infants into groups—AGA, SGA, and LGA—based on birthweight and gestational age (Arsić et al., 2012; Bobiński et al., 2013). Only one study has assessed potential differences in the macronutrient content of mothers' mature milk among infants born SGA, AGA, and LGA. They reported no significant differences among the three groups (Phattraprayoon et al., 2018).
However, no study has yet compared the colostrum macronutrient content of AGA, SGA, and LGA groups among term infants. Therefore, this study aims to compare the colostrum macronutrient content of mothers who delivered term infants classified as SGA, AGA, and LGA.
Methods
Research Design
This was a cross-sectional, observational study. The study was conducted in accordance with the principles of the Declaration of Helsinki. Approval for the study was obtained from the Local Ethics Committee of Zekai Tahir Burak Maternity Teaching Hospital.
Setting and Relevant Context
The hospital in which this study occurred is a public hospital that receives patients from many provinces of Turkey. Full resources are dedicated to obstetrics and the neonatal intensive care unit. It manages approximately 20,000–25,000 deliveries annually and serves as a referral center, particularly for high-risk pregnancies. The patient group served exhibits a homogeneous structure, primarily comprising low- to middle-income individuals with similar socioeconomic status. In routine care, infants not requiring intensive care are monitored alongside their mothers and are usually discharged within 2 days of a vaginal delivery and 3 days after a Cesarean delivery.
The hospital is certified as a Baby Friendly hospital, supporting exclusive breastfeeding. Pregnant women receive information about human milk and breastfeeding through antenatal pregnancy education classes and follow-ups. After birth, infants are immediately initiated into exclusive breastfeeding, and frequent breastfeeding is encouraged by ensuring that the mother and the infant stay in the same room. Throughout this process, lactation support providers—nurses who are also nationally certified lactation consultants—support the mother. Additionally, nurses who care for both the mother and infant provide breastfeeding assistance until their discharge from the hospital.
Sample
The target population for this study was lactating Turkish mothers of term infants. The study included participants who were over 18 years of age, healthy, and clinically stable. Their infants were born at ≥ 37 weeks of gestation, were healthy, and exclusively breastfed after delivery. Breastfeeding throughout our study was defined as the infant receiving human milk (directly from the breast or expressed) according to World Health Organization (WHO) definitions for infant feeding. Exclusive breastfeeding was defined as the infant receiving only human milk from the mother and no other nutrients (WHO, 2023).
Exclusion criteria included preterm birth which is defined as the birth of a baby < 37 weeks of gestation, multiple pregnancy, pregnancy-related conditions (gestational diabetes, preeclampsia/eclampsia, gestational hypertension, HELLP syndrome, infection), chronic illnesses (diabetes mellitus, hypertension, any inflammatory disease), delivery complications (excessive bleeding), alcohol or drug abuse, and active/passive smoking during pregnancy. Insufficient lactation (inability to provide an adequate milk sample within the planned time period), and early discharge (before 24 hours) were also grounds for exclusion. Additionally, participants for whom information on pre-pregnancy maternal weight, maternal height, and maternal weight at the time of delivery was missing were excluded from the study. All participants enrolled in the study exclusively breastfed their infants.
The study involved a total of 252 participants, divided into three groups based on their infants' birthweights: SGA group (n = 57), AGA group (n = 122), and LGA group (n = 73). A formal sample size calculation was not performed due to the exploratory nature of the study. However, the number of participants in the dataset was deemed sufficient for the analysis based on the existing data and the scope of the investigation.
Measurement
The demographic data of the participants, including age (years), mode of delivery, gravidity, parity, BMI at birth (kg/m2), and gestational weight gain (the difference between pre-pregnancy weight and weight just before birth, kg), were recorded by the researchers from medical files. Additionally, demographic data for newborn infants, including birthweight (grams), gestational age (weeks), sex, and Apgar scores (1/5 minutes), were recorded from medical files. All infants were weighed naked with an electronic scale after birth, before the first feeding. Infants weighing below the 10th percentile for their gestational age were classified as SGA. Infants weighing between the 10th and 90th percentile for their gestational age were classified as AGA, while those weighing greater than the 90th percentile for their gestational age were classified as LGA (Fenton et al., 2013).
The mid-infrared human milk analyzer (HMA) developed by MIRISTM (Uppsala, Sweden) quantitatively measures the concentration of fat, protein, and carbohydrate in human milk (in g/dl). It also provides calculated values for energy (in kcal/dl). The results of true protein, fat, carbohydrate, and energy levels of the colostrum were recorded using MIRIS HMA™. The analyzer has been approved by the International Organization for Standardization (ISO) 9622:1999. The reliability of the MIRIS HMA™ analyzer in our study was ensured through regular calibration according to manufacturer guidelines and by conducting internal quality control checks during data collection. Each milk sample was analyzed in duplicate to ensure consistency and reproducibility of results. Each sample was analyzed twice to confirm the results. All measurements were directly derived from the spectral analysis of each milk sample without modification. Cut-off points specific to macronutrient concentrations were not applicable in this context, as the analyzer provided continuous quantitative data.
Data Collection
The study was conducted from April 1 to September 30, 2014. On the first postpartum day, researchers informed participants who met the study inclusion criteria about the protocol, and consent was obtained before colostrum was collected on the second postpartum day. The maternal and neonatal data were obtained and recorded by the researcher from medical files. In the morning (9–11 am) of the second postnatal day, after feeding the infant, 3–4 ml of colostrum samples were manually expressed from either the left or right breast by the mother herself, with assistance from the researcher or a lactation support provider. Colostrum collection was performed using Eppendorf tubes. Fresh samples were analyzed immediately after collection, within 2 hours, without freezing. A cold-carrying bag was used during transportation for the colostrum samples. Participant identities were anonymized by assigning identifiers to each participant. Personal details such as names and contact information were kept separate from research data. Only authorized personnel involved in the study had access to identifiable participant information.
Data Analysis
Descriptive analysis was performed to describe the demographic characteristics of the participants and colostrum macronutrient content. The normality of the distribution of continuous variables was assessed through the Kolmogorov–Smirnov or Shapiro–Wilk tests. All continuous variables were non-normally distributed and were expressed as medians (interquartile range), counts, and percentages (%). Categorical variables were compared using the Chi-square test. Continuous variables were compared using the Mann Whitney U test or Kruskal Wallis test if non-normally distributed.
For the multivariable-adjusted analysis, we initially dichotomized milk component (protein, carbohydrate, fat) levels based on the median, and we used the dichotomized variable (low vs. high) as the dependent variable in the logistic regression analysis. The possible confounding factors were further entered into the regression analysis to determine independent predictors of colostral protein, carbohydrate, and fat content. We have included gestational age, gender, route of delivery, maternal age, maternal BMI, and gestational weight gain, as well as SGA and LGA, as confounders in the model to determine the independent contribution of the factors for milk composition. Hosmer Lemeshow goodness-of-fit statistics were used to assess model fit. All analyses were performed using SPSS (Version 22.0). A p < 0.05 was considered statistically significant.
Results
Characteristics of the Sample
The demographic data of the maternal and neonatal participants are detailed in Table 1. The median (IQR) macronutrient contents of colostrum, categorized by the groups, are presented in Table 2. Colostrum median protein levels were 4.8 (IQR = 3–6.4) g/dl, 2.8 (IQR = 2.1–3.7) g/dl, and 4.4 (IQR = 3.5–5.3) g/dl for the SGA, AGA, and LGA groups, respectively. Colostrum protein content was significantly higher in the SGA and LGA groups than in the AGA group (Mann Whitney U test; p < 0.001 for both SGA vs. AGA and LGA vs. AGA; Table 2). There were no significant differences observed in colostrum fat content among the groups (Median 2.4 [IQR = 1.8–3.2], Median 2 [IQR = 1.4–3.1], Median 2.5 [IQR = 1.8–3.2] g/dl) for SGA, AGA, LGA, respectively (Kruskall Wallis test; p = 0.074). Carbohydrate levels were higher in the LGA and SGA groups than in the AGA group, but only the difference between the LGA and AGA groups was significant (Mann Whitney U test; p < 0.001 for LGA vs. AGA; Median 4.7 [IQR = 3.8–5.8], Median 4.5 [IQR = 3.5–5.3], Median 5.3 [IQR = 4.2–6] g/dl); SGA, AGA, LGA, respectively (Kruskall Wallis test; p = 0.002). Median (IQR) energy levels were significantly higher in the SGA and LGA groups compared to the AGA group (Mann Whitney U test; p < 0.001 for both SGA vs. AGA and LGA vs. AGA; Median 64 [IQR = 55–77], Median 55.5 [IQR = 49–67], Median 68 [IQR = 58–72] kcal/dl) for SGA, AGA, LGA, respectively (Kruskall Wallis test; p < 0.001; Table 3). All median macronutrient and energy measurements are comparatively illustrated in Figure 1.
Demographic Characteristics of the Study Groups (N = 252).
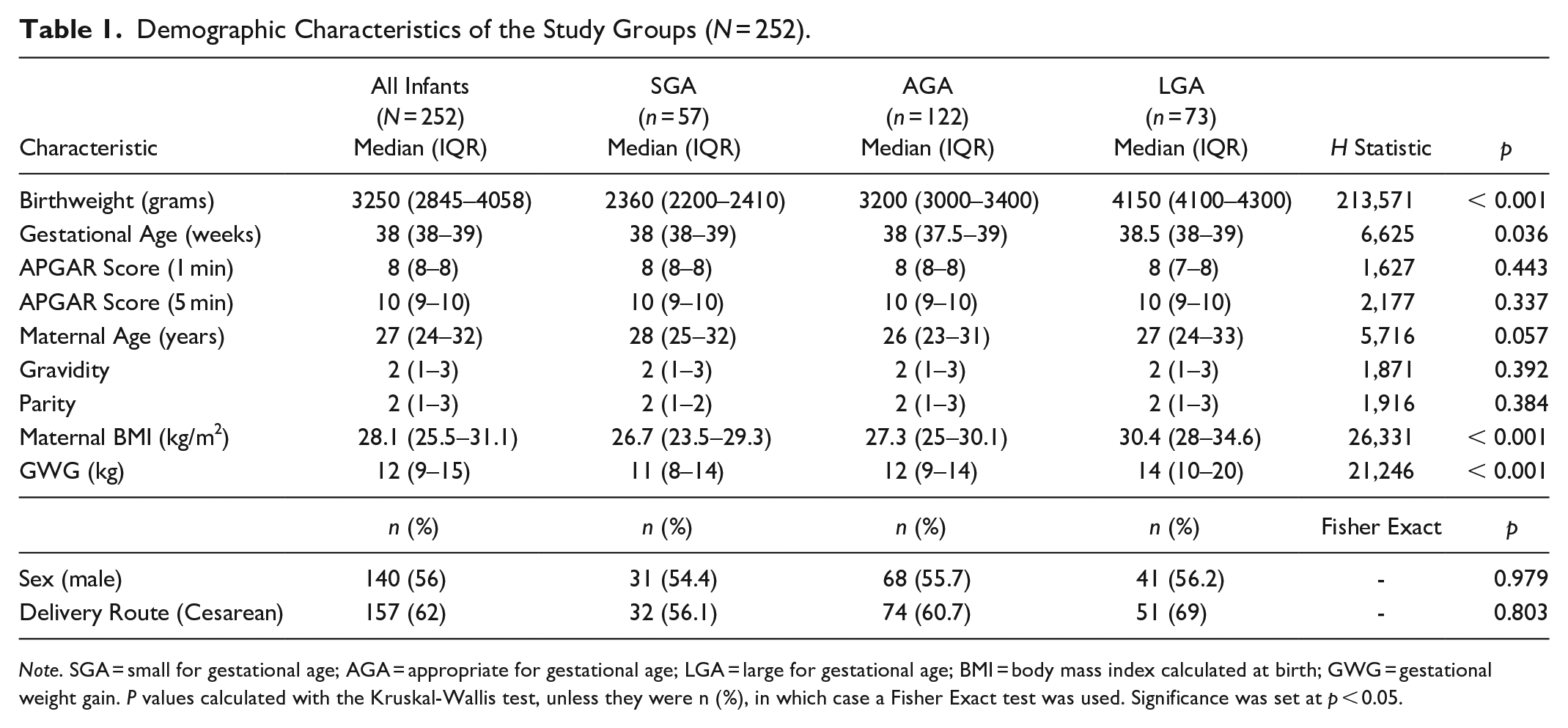
Note. SGA = small for gestational age; AGA = appropriate for gestational age; LGA = large for gestational age; BMI = body mass index calculated at birth; GWG = gestational weight gain. P values calculated with the Kruskal-Wallis test, unless they were n (%), in which case a Fisher Exact test was used. Significance was set at p < 0.05.
Colostrum Protein, Fat, Carbohydrate, and Energy Levels in Study Groups (N = 252).
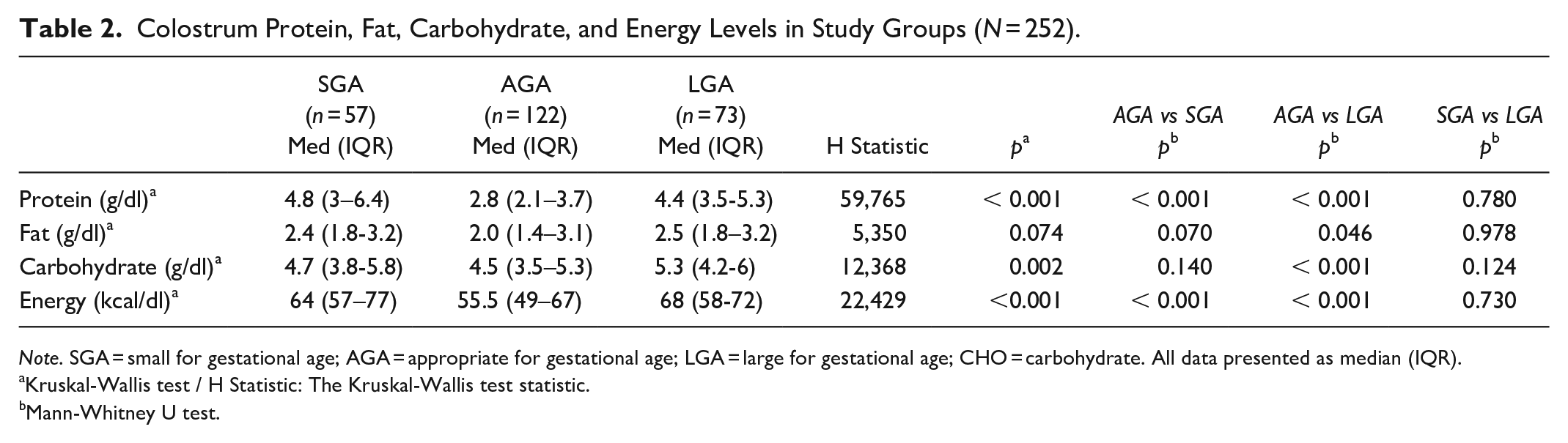
Note. SGA = small for gestational age; AGA = appropriate for gestational age; LGA = large for gestational age; CHO = carbohydrate. All data presented as median (IQR).
Kruskal-Wallis test / H Statistic: The Kruskal-Wallis test statistic.
Mann-Whitney U test.
Logistic Regression Analysis for Independent Predictors of Higher Colostrum Protein, Carbohydrate, and Fat Content (N = 252).
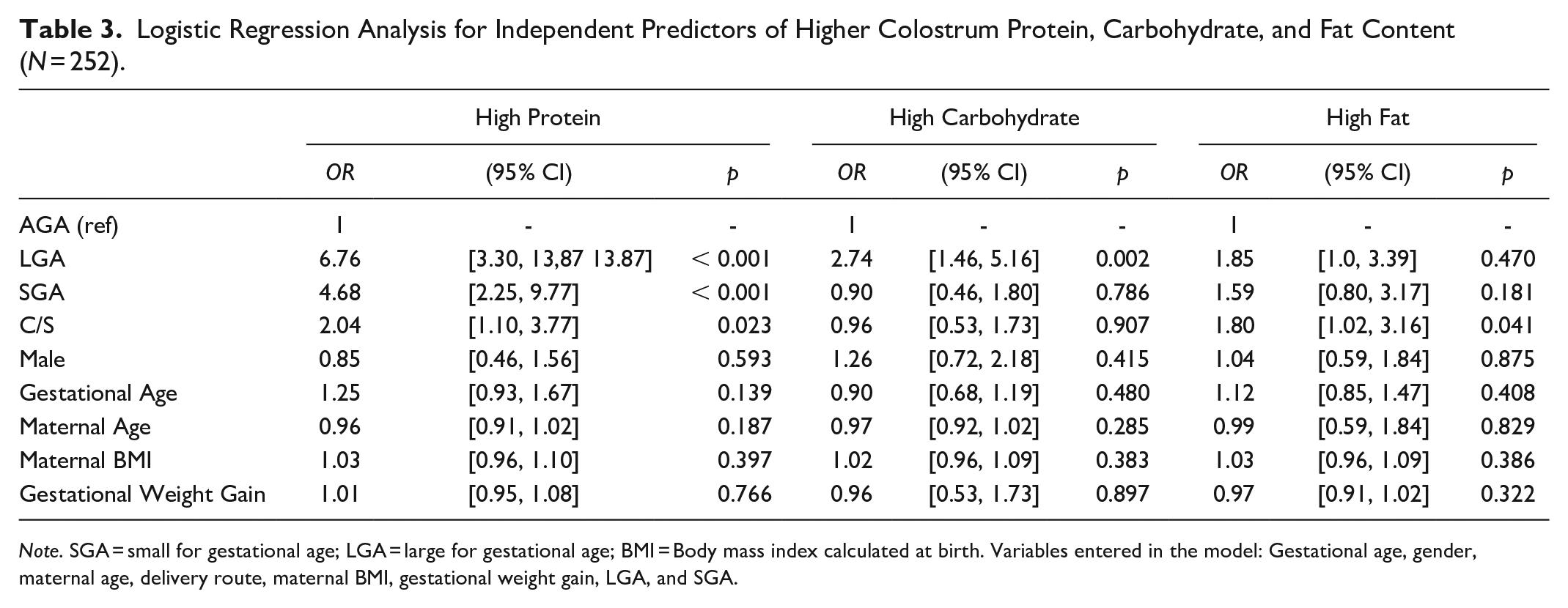
Note. SGA = small for gestational age; LGA = large for gestational age; BMI = Body mass index calculated at birth. Variables entered in the model: Gestational age, gender, maternal age, delivery route, maternal BMI, gestational weight gain, LGA, and SGA.
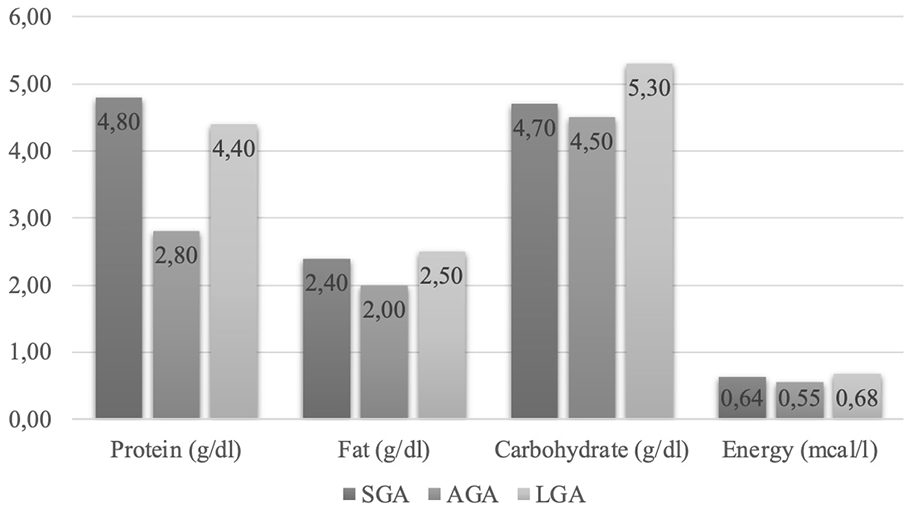
Median Macronutrient and Energy Levels of Colostrum.
Multivariate analysis was performed using gestational age, gender, maternal age and BMI, delivery route, gestational weight gain, and status of birthweight for gestational age (SGA and LGA). Being SGA or LGA were found to be independently associated with higher colostrum protein content (OR 4.68; 95% CI [2.25, 9.77]; p < 0.001; OR 6.76; 95% CI [3.30, 13.87]; p < 0.001; OR 2.04; 95% CI [1.10, 3.77]; p = 0.02, respectively). Additionally, being LGA was found to be independently associated with higher colostrum carbohydrate content in the multivariate analyses (OR 2.74; 95% CI [1.46, 5.16]; p = 0.002; Table 3).
Discussion
In this study, we found that participants with SGA and LGA infants had higher protein and energy content in their colostrum compared to participants with AGA infants. Additionally, participants with LGA infants had higher carbohydrate content in their colostrum compared to those with AGA infants. Furthermore, being SGA or LGA was independently associated with higher colostrum protein content, and being LGA was also independently associated with higher colostrum carbohydrate content. These data may suggest that alterations in birthweight for gestational age could influence the macronutrient composition of colostrum.
Bobiński et al. (2013) reported that maternal physiology during pregnancy prepares the mammary gland to produce milk tailored to the infant's condition, likely influenced by placental functions and fetal programming. The finding that maternal colostrum protein levels are higher in preterm infants compared to term infants also supports the idea that human milk composition dynamically adapts to the needs of the infant (Bulut et al., 2019; Sahin et al., 2020; Thakur et al., 2021). Studies on SGA and LGA infants have demonstrated that alterations in birthweight are associated with diverse morbidities, such as feeding difficulties and hypoglycemia, and that these infants may exhibit different metabolic demands and growth patterns (Adamkin, 2017; Bartal et al., 2021; Bora & Deori, 2019; Chauhan et al., 2017; Dunn et al., 2021; Kosmeri et al., 2023; Wight & the Academy of Breastfeeding Medicine, 2021; Zhang et al., 2024). Only one study has examined potential differences in the macronutrient content of mature milk among infants born SGA, AGA, and LGA, reporting no significant differences among the groups (Phattraprayoon et al., 2018). To our knowledge, no study has specifically evaluated the macronutrient content of colostrum in SGA and LGA infants. In our study, the higher colostrum protein levels observed in the SGA and LGA groups may indicate the increased needs of the infants compared to AGA groups. However, the types of proteins responsible for this difference may be the primary determinants of clinical significance. Small differences in certain key protein components may have significant clinical effects on growth, development, and immunity. Since we did not evaluate the types of colostral proteins, we are unable to comment on this aspect with our data.
Lipid, the most variable and second-largest macromolecule in human milk, is influenced by factors including the stage of lactation, maternal diet, maternal BMI, and weight gain during pregnancy (Bahreynian et al., 2020; Ballard & Morrow, 2013; Burianova et al., 2019). Studies evaluating the free fatty acid content in the milk of participants with AGA and SGA infants have reported conflicting results. Arsić et al. (2012) and Bobiński et al. (2013) found that low birthweight affects the free fatty acid content in mature milk, while Lubertzky et al. (2016) and Domany et al. (2015) did not observe any differences in fat content or fatty acid composition among the colostrum, transitional milk, and mature milk of participants with SGA infants compared to those with AGA infants. Similarly, in our study, despite differences in maternal BMI and weight gain during pregnancy between the LGA and AGA or SGA groups, we did not find any statistically significant differences in colostrum fat content.
The carbohydrate content in human milk is the least variable among macronutrients. In some publications, carbohydrate content in human milk has been associated with the mother's diet and obesity (Nurani et al., 2023). In our study, we found that the colostrum carbohydrate content in the LGA group was significantly higher than in the AGA and SGA groups, and being LGA was independently associated with higher colostrum carbohydrate content. While colostrum fat content was similar, energy levels were higher in the SGA and LGA groups compared to the AGA group. This is because, although fat is the primary component of colostrum's energy content, protein and carbohydrate contents also contribute to the higher energy levels.
At present, the exact mechanisms underlying the relationship between birthweight alterations for gestational age and macronutrient content cannot be fully explained. It is possible that these differences result from fetal programming which alters the protein or carbohydrate content of colostrum, potentially related to the infant’s needs. It is clear that colostrum adapts to different pregnancy environments. Considering the influence of birthweight for gestational age on the macronutrient content of colostrum may be beneficial for optimal feeding strategies. The protective effect of our findings against nutritional problems and hypoglycemia in the first days is not yet known. The underlying causal pathway explaining our findings remains unclear and warrants further investigation in future studies. While each mother's milk is uniquely produced for her baby, the findings of similar studies may prove useful in the selection of donors from milk banks. This can be particularly beneficial in cases where a newborn does not have access to their own mother’s milk, allowing for a more appropriate match to meet the infant's needs.
Limitations
The study has several limitations. First, maternal diet and socioeconomic status were not assessed. Additionally, only one sample was taken from each mother, and the potential variability associated with diurnal rhythm was not evaluated. Furthermore, human milk monitoring was not conducted longitudinally, and the growth patterns of infants were not assessed. Therefore, the clinical influence of variations in macronutrient content could not be thoroughly investigated. The fact that colostral protein types were not identified is another limitation of the study. The lack of data on these aspects prevents us from fully understanding the clinical implications of protein variations. Moreover, micronutrients and other biologically active components of colostrum were not included in the evaluation. Also, conducting the study on a specific group with a relatively small number of participants limits its generalizability. Another notable limitation is that our hospital, serving as a referral center for high-risk pregnancies, experiences elevated rates of cesarean sections. The data for this study were collected in 2014. Although this might be considered a limitation, we feel that there have not been significant changes that would have affected the applicability of the results to our current times.
Conclusion
This study demonstrates that the macronutrient composition of colostrum, particularly protein and carbohydrate content, differs according to birthweight-for-gestational-age classification. These findings suggest a potential adaptive mechanism in human milk that aligns with the metabolic needs of the newborn. Future research should aim to clarify the biological mechanisms driving these differences and evaluate their short- and long-term impacts on infant growth and development. Additionally, insights from such studies may contribute to optimizing donor milk selection and individualized neonatal nutritional strategies.
Footnotes
Author’s Note
All authors were affiliated at Zekai Tahir Burak Maternity Teaching Hospital at the time the study was conducted.
Author Contributions
Disclosures and Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.