
Abstract
Background:
Breastfeeding is strongly promoted by health authorities, but there is little research on whether health professionals provide best-practice care for women experiencing mastitis/breast abscess.
Research Aim:
To explore management of mastitis/breast abscess in hospital emergency departments (EDs).
Methods:
Medical records of patients presented to hospital EDs in Australia, Brazil, Croatia, Germany and Türkiye with lactational mastitis/abscess between 2017 and 2023 were reviewed. Demographic and clinical information (including symptoms, management, and investigations) was extracted and analyzed.
Results:
A total of 580 women with mastitis/breast abscess (646 Emergency Department presentations, mostly in the first 8 weeks postpartum) were identified during the study period. The majority of the women had symptoms of mastitis/breast abscess (breast pain, lump, and inflammation) for > 48 hours before presenting in the Emergency Department. In Australia, culture and sensitivity testing of milk was available for 44% (146/331) of presentations. S. aureus was the most common bacteria isolated (33%, n = 48), of which 6% (n = 3) were methicillin-resistant. The use of diagnostic ultrasound varied between sites, from 5% (3/65) in Croatia to 82% (40/49) in Germany. Breast abscesses were mostly managed by ultrasound-guided aspiration in Australia, whereas incision and drainage was standard care in Germany. Amoxicillin/clavulanate was most commonly prescribed in Croatia (57%, 31/54) and Türkiye (69%, 28/42), whereas flucloxacillin, cephalexin, or cefuroxime was primarily used in Australia (86%, 272/322), Brazil (62%, 66/106), or Germany (80%, 33/41), respectively.
Conclusions:
The management of mastitis/breast abscess varied considerably between countries. International evidence-based guidelines for the management of lactational mastitis are urgently needed.
Keywords
Key Messages
There is a significant gap in best-practice care for women experiencing breastfeeding problems, particularly in the management of lactation mastitis.
Audit studies are needed to understand if current management of mastitis and breast abscesses follows evidence-based guidelines, including appropriate antibiotic use and supportive measures to enable women to continue breastfeeding.
An audit study across five countries revealed inconsistencies in the ordering of blood tests, microbiological testing, use of diagnostic ultrasound, and treatment approaches, including antibiotic prescription and management of breast abscesses.
Our study confirms the need for standardized care practices to ensure optimal treatment outcomes.
Background
Breastfeeding is strongly promoted by health authorities globally (Victora et al., 2016), but there has been little focus on health professionals providing best-practice care for women experiencing breastfeeding difficulties. The management of lactational mastitis can be used as an illustration of how health professionals understand and manage breastfeeding issues (Amir & Ingram, 2008).
Lactational mastitis is diagnosed when a lactating person experiences a red, hard, painful area of the breast associated with fever and/or systemic symptoms (Radke, 2022; Scott, 2022). Mastitis may be managed in the community, by community nurses, general practitioners, private obstetricians, women’s health physiotherapists, pharmacists, or in hospital emergency departments (ED). While mild cases often resolve with symptomatic management, and most cases are managed in the community, more severe cases of mastitis may require hospital admission and treatment with intravenous antibiotics. A breast abscess (painful collection of pus within the breast requiring drainage) is a possible complication of mastitis (Morozova et al., 2023; Patani et al., 2018).
There is a lack of robust research on the management of mastitis and randomized trials evaluating the treatment of mastitis are scant (Jahanfar et al., 2013). Current evidence is mostly based on expert opinion as summarized below.
Use of Antibiotics for Mastitis
Firstline management involves education that inflammation does not imply infection, and advising maternal rest, analgesia, cool packs, and continued breastfeeding (Mitchell et al., 2022; Royal Women’s Hospital, 2023). The World Health Organization (WHO, 2000) review of mastitis concluded that antibiotics should be started if symptoms persist for > 24 hours. Other organizations have maintained this recommendation (Dixon & Adetola, 2023; Royal Women’s Hospital, 2023). A population-based database study in Taiwan identified that 79% of women with medically diagnosed mastitis were prescribed antibiotics (Lin et al., 2023).
The organism most commonly associated with lactational mastitis is Staphylococcus aureus (S. aureus; Lukassek et al., 2019; Rimoldi et al., 2020). Importantly, isolates of S. aureus resistant to penicillinase-stable β-lactams have been identified (generally referred to as methicillin-resistant S. aureus [MRSA]) since 1960 (Harkins et al., 2017). Women and children are among the groups predisposed to MRSA, and increasing isolation of MRSA in cases of mastitis and breast abscesses has been reported (Rimoldi et al., 2020; Salmanov et al., 2020).
Appropriate Use of Investigations
While not done routinely, culture and sensitivity testing of human milk is useful in cases of severe infection or poor response to initial antibiotics (Dixon & Adetola, 2023; Mitchell et al., 2022). Diagnostic breast ultrasound is used if local symptoms persist after antibiotic treatment to identify a breast abscess or fluid collection (Morozova et al., 2023). While breast cancer usually occurs in older women, inflammatory breast cancer (the “most lethal breast cancer”) can occur during lactation and the clinical and ultrasound appearance is similar to mastitis (Morozova et al., 2023).
Management of Breast Abscess
While traditional management of breast abscesses involved hospital admission and incision and open drainage with general anesthesia, ultrasound-guided needle aspiration is now considered standard treatment (Courtney et al., 2024). Needle aspiration is cost-effective and reduces the risk of breast fistula, while supporting continuous breastfeeding and improved patient satisfaction (Zhou et al., 2023).
Supporting Women to Continue Breastfeeding
Women with mastitis should be supported to continue breastfeeding (or pumping/expressing) because it is safe for the infant, and sudden cessation of breastfeeding increases women’s risk of developing a breast abscess (Scott, 2022). Continued breastfeeding is also recommended for women with a breast abscess (Mitchell et al., 2022).
Best practice care for women with mastitis includes supporting the mother to continue breastfeeding, prescribing the correct antibiotic appropriately, and ordering investigations if indicated. Findings from a recent Australian study suggested that general practitioners largely followed the Australian Therapeutic Guidelines when prescribing antibiotics for the management of mastitis (Grzeskowiak et al., 2024). However, studies reporting antibiotic selection in other countries are scant. Results of a recent large audit of management of mastitis and breast abscesses in 69 hospitals in the United Kingdom and Ireland showed that “amoxicillin/clavulanate and flucloxacillin were the first-line antibiotics” (Courtney et al., 2024). Further, variation in practice was seen in the management of breast abscesses, with high rates of incision and drainage of breast abscesses in some centers (Courtney et al., 2024).
In order to address the paucity in research on the medical care of lactating women, we set out to explore current practices around the management of mastitis in hospital emergency departments in five countries, using clinical audits.
Methods
Research Design
A retrospective cross-sectional study was conducted through an audit of medical records of women diagnosed with lactational mastitis and/or abscess who presented to the hospital ED in Australia, Brazil, Croatia, Germany, and Türkiye. We chose this study design since a “clinical audit is a way to find out if healthcare is being provided in line with standards and lets care providers and patients know where their service is doing well and where there could be improvements” (National Health Service, 2016). The first author invited other researchers with an interest in the topic to collect data in their maternity services. We aimed to use routinely collected data to provide an international snapshot of current practices.
Ethics approval was received from the human research ethics committees of Royal Women’s Hospital, Australia (AQA 23/05), Federal University of Sao Paulo, Brazil and the Brazilian hospital service (3.621.829), University Hospital of Split, Croatia (2181-147/01/06/M.S.-22-03), IRB, Medical School REGIOMED Coburg, Germany, and KTO Karatay University, Türkiye (2022/040). Written informed consent was waived by all ethics committees.
Setting and Relevant Context
The Royal Women’s Hospital, Melbourne,
The three
In
The Regiomed clinic in Coburg,
In
Sample
Women with a diagnosis of lactational mastitis or abscess, who presented to the above hospital ED during the study period, were included in the study. ICD-10 codes were used to identify relevant patients. The codes used were O91 codes for lactational mastitis, including O91.1B (abscess) and O91.2 (inflammatory mastitis without bacteria). All medical records of relevant patients were reviewed and excluded if the diagnosis of mastitis/breast abscess was coded incorrectly (e.g., nipple/breast candida infection) or occurred in a non-lactating patient (e.g., infected breast cyst or postoperative infection after breast surgery).
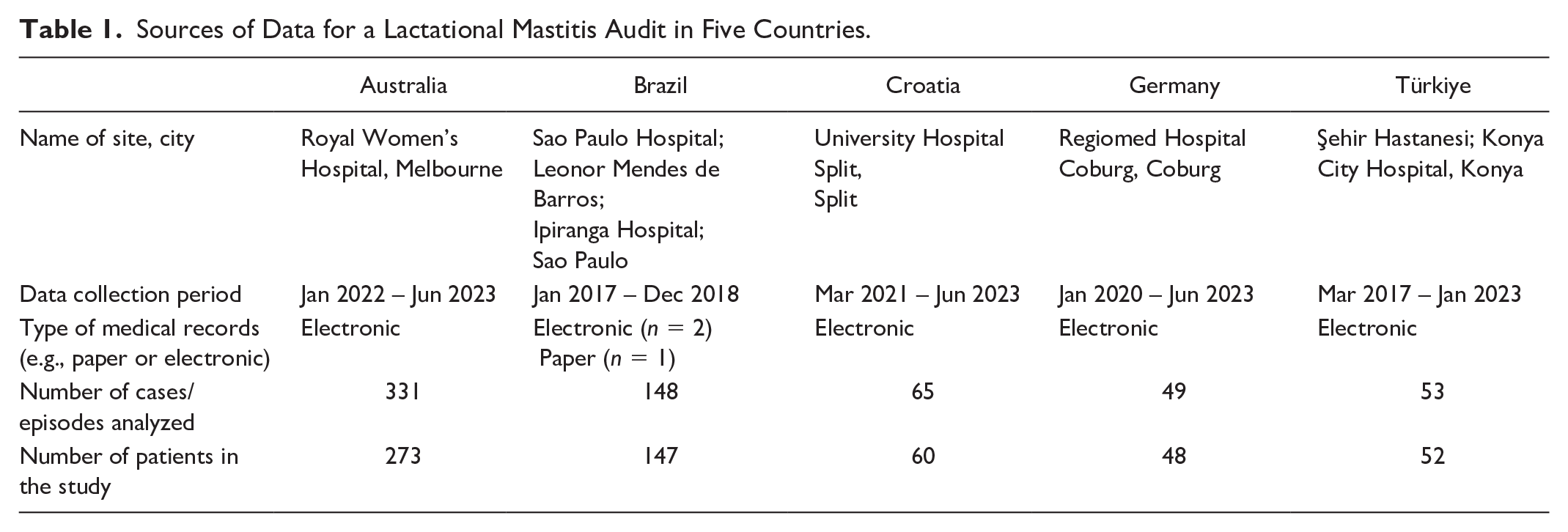
We estimated 50 to 100 records at each site and considered that it would be feasible to collect data from approximately a 12-month period without outside funding. A previous single-center audit of mastitis used data from a 12-month period, and included 107 women (Amir et al., 1999). The final sample size for each site is shown in Table 1, and was 50 to 60 records in Croatia, Germany and Türkiye, 148 in Brazil and 331 in Australia. As the study is descriptive in nature, the proposed sample size was anticipated to be adequate for the study aim.
Sources of Data for a Lactational Mastitis Audit in Five Countries.
Measurement
An audit form was designed based on an earlier audit (Amir et al., 1999), and other data items were added to enable evaluation of the management of mastitis/breast abscess (available in supplementary material). Data collected included patients’ age, parity, history of breast surgery, history of mastitis, method of birth, infants’ age, method of infant feeding, temperature, reported signs and symptoms, duration of symptoms, evidence of nipple trauma, radiological and microbiological results, C-reactive protein (CRP), details of antibiotic therapy, analgesia, and abscess management, breastfeeding advice, and details of hospital admission.
For the Royal Women’s Hospital in Australia, we also recorded the number of women who gave birth at the hospital or elsewhere (in-born/out-born), who had an infant in the Neonatal Intensive Care Unit, and who received intravenous antibiotics in the ED but were not admitted.
Data Collection
Data were collected between 2017 and 2023, and varied between sites since data were collected as part of local student projects or unfunded staff projects (see Table 1 for dates for each site). Table 1 also shows the type of medical record (paper or electronic) at each site, and the number of patients and total presentations. Hospital identification number and date of birth were recorded for each entry to avoid duplication error, but no other personal details were extracted. All data were de-identified and pooled prior to analysis.
Data abstraction was completed by three researchers in Australia (LHA, MHMN, WJ), who worked together on the first 10 records to ensure consistency; two researchers in Brazil (MJMDS, MMO), with training and checking by second researcher (KPC); two researchers in Croatia (LD, MD) who were trained by a more experienced researcher (IZG) prior to data collection; one researcher in Germany (MR), also trained by IZG; and two researchers in Türkiye (SK, KG), with data checked by BD. The team held monthly online meetings to discuss how to collect and interpret unclear variables.
Study data were collected and managed using REDCap electronic data capture tools hosted at Universidade Federal de São Paulo, Brazil (Harris et al., 2009, 2019). REDCap (Research Electronic Data Capture) is a secure, web-based software platform designed to support data capture for research studies. If REDCap access was unavailable, a hard copy form was used and data entered later.
Data Analysis
Descriptive statistics were used to report the characteristics of women with mastitis/breast abscess, the signs and symptoms, investigations ordered, and management documented in the medical record. Microbiological results are reported where available. Details of the management of breast abscess were summarized. We report the numerator and denominator for all variables that are recorded; missing data are reported as “not recorded” for important variables such as temperature. The analysis was planned to be descriptive only, with no comparisons between hospital sites. We used the Wilcoxon-Mann Whitney or Kruskal-Wallis tests to explore the relationship between available CRP levels and the following: duration of symptoms prior to presentation, subjective fever, lethargy, rigor/shivering, and abscess.
Results
A total of 580 women with mastitis and/or breast abscess (646 ED presentations) were identified during the study period and included in the analysis. Patient characteristics are shown in Table 2. The youngest patients were in Brazil with a median age of 26 years (IQR = 23–31), and the oldest were in Australia, with a median age of 33 years (IQR = 30–36). Maternal age at other sites as follows: Türkiye, 27 years (IQR = 24–32); Croatia, 31 years (IQR = 27–34), and Germany, 32 years (IQR = 28–34). Primiparous women (138/217, 64%) were more likely to present than multiparous women in Australia (79/217, 36%), but this was not seen in the other countries, possibly due to missing data. In the Australian ED presentations, 69% (228/331) had in-born infants and 13% (43/331) had an infant in the Neonatal Intensive Care Unit/Special Care Nursery.
Patient Characteristics of Women With Mastitis/Breast Abscess.
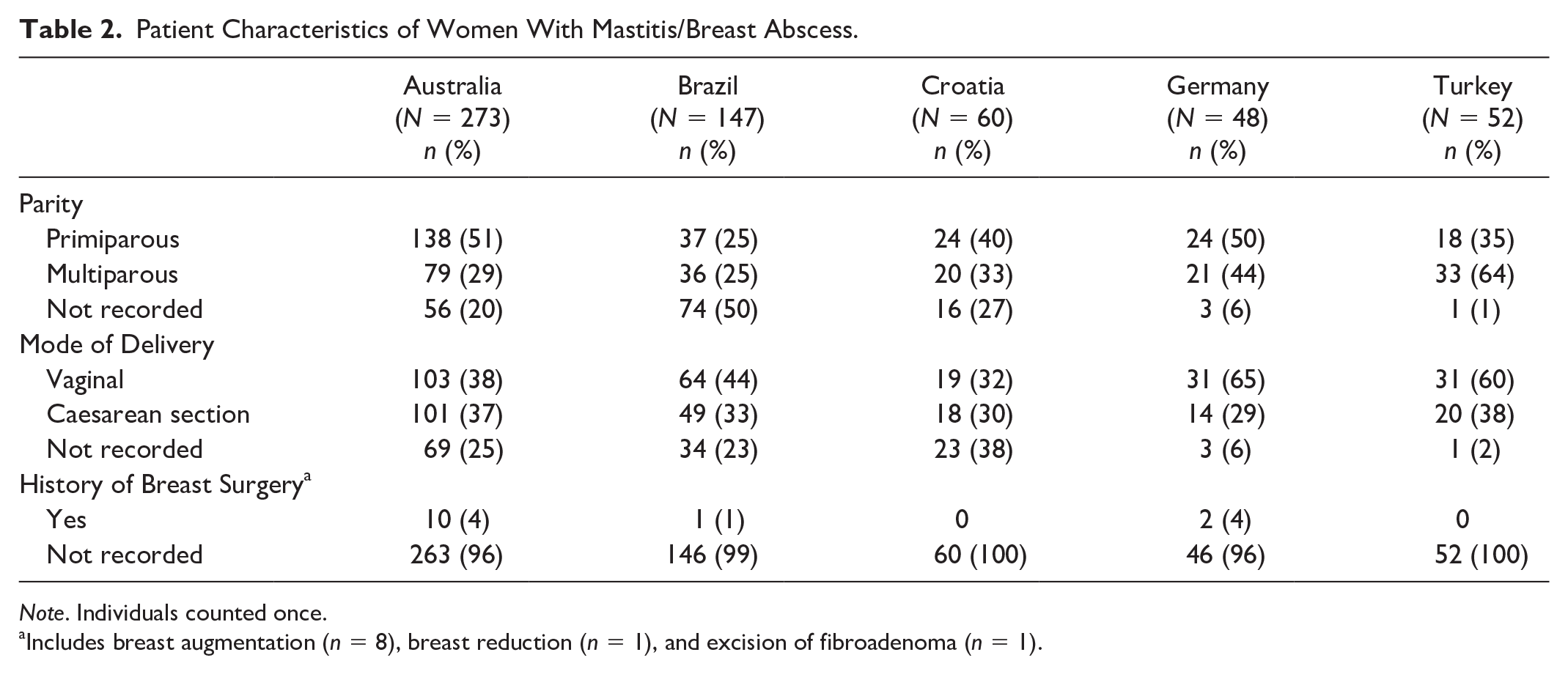
Note. Individuals counted once.
Includes breast augmentation (n = 8), breast reduction (n = 1), and excision of fibroadenoma (n = 1).
Clinical presentation details are shown in Table 3. In all sites, the highest proportion of presentations were in the first 8 weeks postpartum. Most women had symptoms of mastitis (or breast abscess) for more than 48 hours before presentation, although this information was missing in 8% to 46% of medical records. While patient temperature was well recorded, the presence of fever ranged from 82% in Croatia to 16% in Brazil.
Clinical Presentations of Mastitis or Breast Abscess.
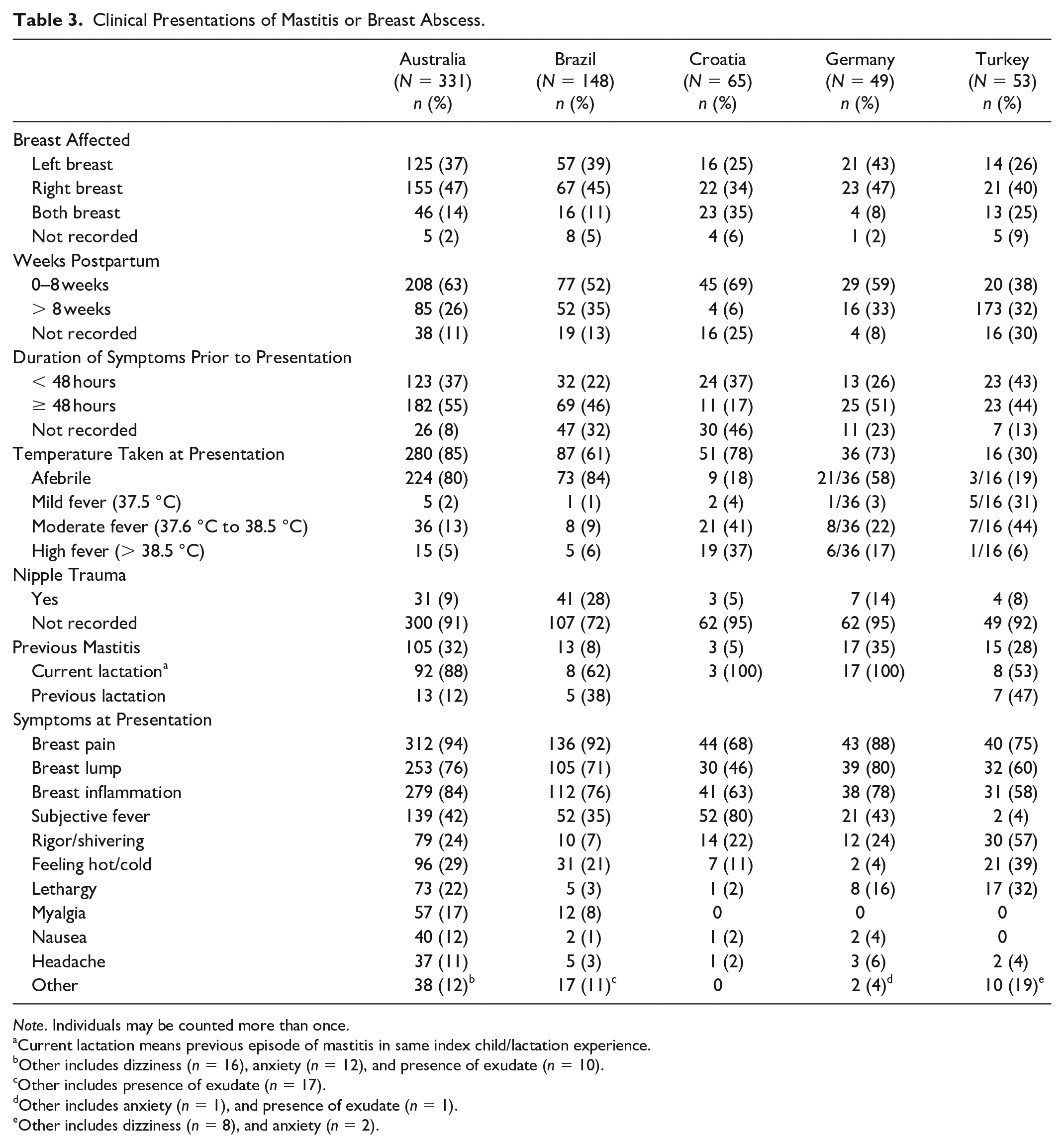
Note. Individuals may be counted more than once.
Current lactation means previous episode of mastitis in same index child/lactation experience.
Other includes dizziness (n = 16), anxiety (n = 12), and presence of exudate (n = 10).
Other includes presence of exudate (n = 17).
Other includes anxiety (n = 1), and presence of exudate (n = 1).
Other includes dizziness (n = 8), and anxiety (n = 2).
The top 10 signs and symptoms recorded are also shown in Table 3. Breast pain, breast lump and breast inflammation were recorded in the majority of patients. Other common symptoms were subjective fever, rigor/shivering and lethargy. The notes also documented myalgia, nausea, headache, anxiety, and dizziness.
Breast abscesses were identified in 46/331 (14%) presentations in Australia, 19/148 (13%) in Brazil, 1/65 (2%) in Croatia, 23/49 (47%) in Germany, and 5/53 (9%) in Türkiye. The use of ultrasound to diagnose breast abscess varied between sites, from 5% (3/65) in Croatia to 82% (40/49) in Germany (Table 4). Most of the abscesses in our study were identified by ultrasound. Of the five cases of abscess which were not identified by ultrasound, one presented as a ruptured abscess (Australia), whilst identification of the other four were unspecified (one in Croatia and three in Germany). Breast abscesses were mostly managed by ultrasound-guided aspiration in Australia (36/46, 78%), of which five required two aspirations and two required three aspirations (Table 5). Incision and drainage was standard care in Germany (19/23, 83%) and Brazil (8/19, 42%). Of the three incision and drainage cases in Australia, two were performed after previous ultrasound-guided aspiration failed to resolve the abscess.
Investigations Undertaken to Aid Diagnosis of Lactational Mastitis.
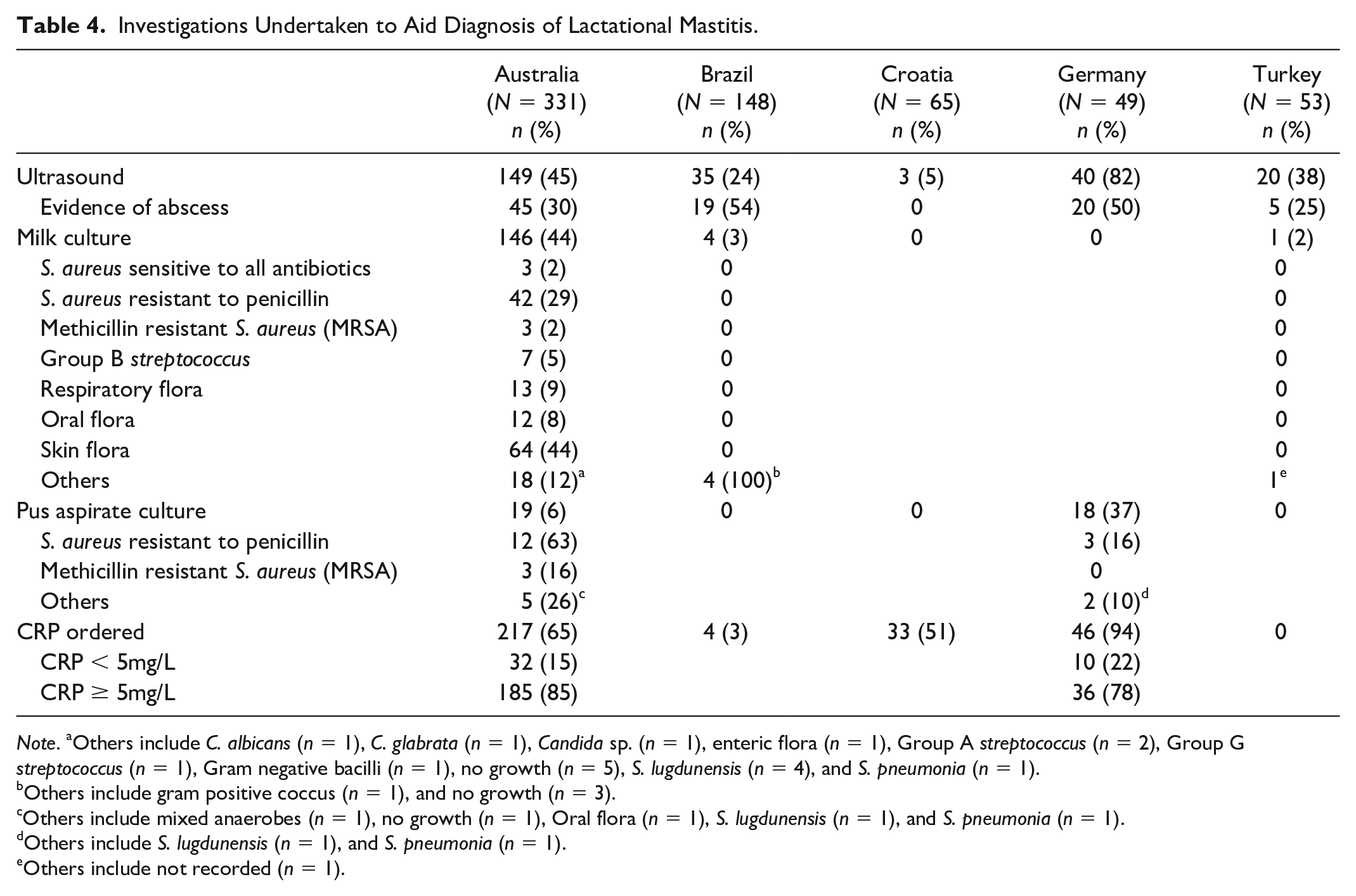
Note. aOthers include C. albicans (n = 1), C. glabrata (n = 1), Candida sp. (n = 1), enteric flora (n = 1), Group A streptococcus (n = 2), Group G streptococcus (n = 1), Gram negative bacilli (n = 1), no growth (n = 5), S. lugdunensis (n = 4), and S. pneumonia (n = 1).
Others include gram positive coccus (n = 1), and no growth (n = 3).
Others include mixed anaerobes (n = 1), no growth (n = 1), Oral flora (n = 1), S. lugdunensis (n = 1), and S. pneumonia (n = 1).
Others include S. lugdunensis (n = 1), and S. pneumonia (n = 1).
Others include not recorded (n = 1).
Management of Lactational Mastitis and Breast Abscess.
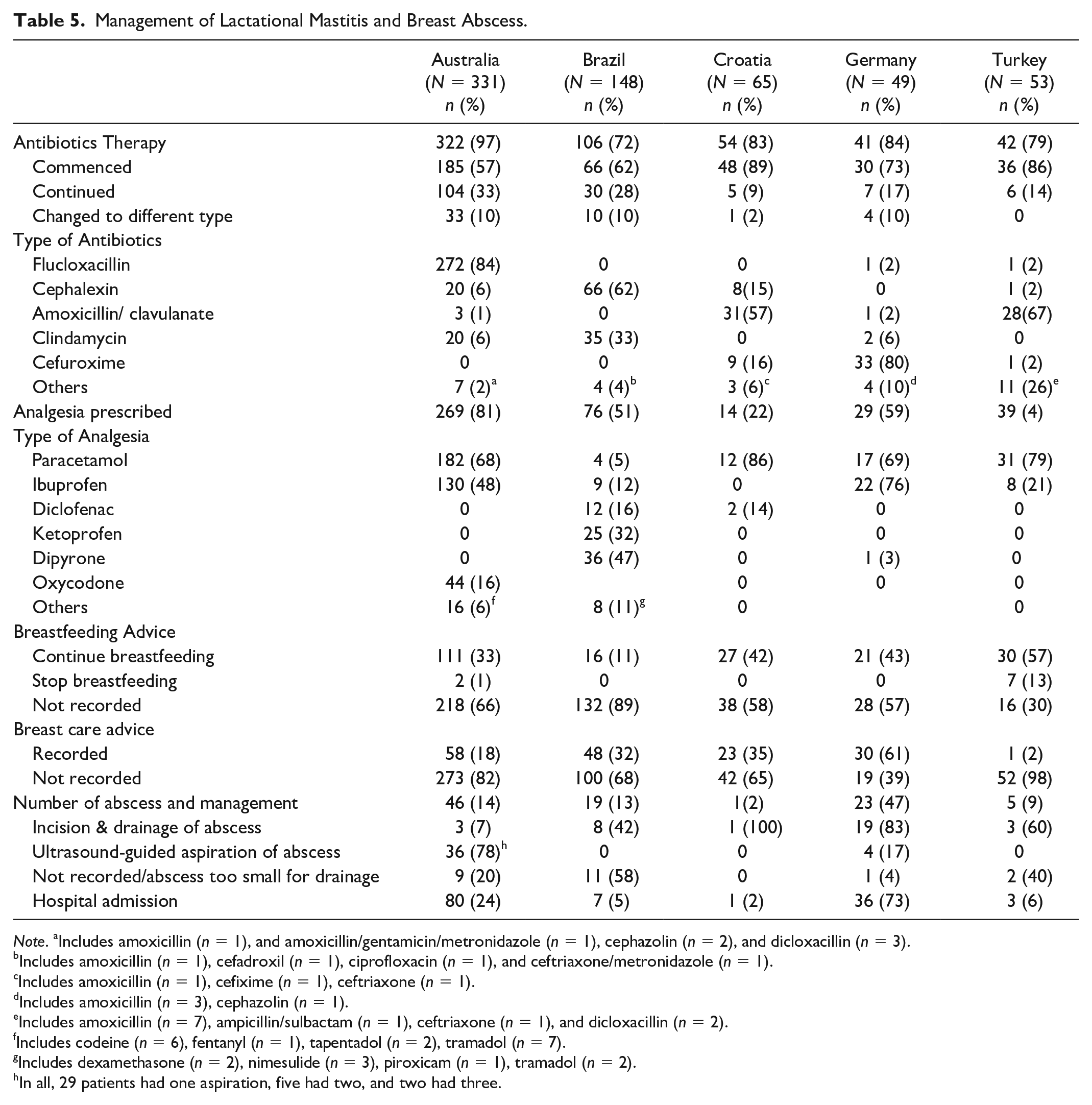
Note. aIncludes amoxicillin (n = 1), and amoxicillin/gentamicin/metronidazole (n = 1), cephazolin (n = 2), and dicloxacillin (n = 3).
Includes amoxicillin (n = 1), cefadroxil (n = 1), ciprofloxacin (n = 1), and ceftriaxone/metronidazole (n = 1).
Includes amoxicillin (n = 1), cefixime (n = 1), ceftriaxone (n = 1).
Includes amoxicillin (n = 3), cephazolin (n = 1).
Includes amoxicillin (n = 7), ampicillin/sulbactam (n = 1), ceftriaxone (n = 1), and dicloxacillin (n = 2).
Includes codeine (n = 6), fentanyl (n = 1), tapentadol (n = 2), tramadol (n = 7).
Includes dexamethasone (n = 2), nimesulide (n = 3), piroxicam (n = 1), tramadol (n = 2).
In all, 29 patients had one aspiration, five had two, and two had three.
Microbiology investigations also varied between study sites. No human milk or pus aspirate samples were recorded in Croatia, and milk samples were collected in only four presentations in Brazil and one in Turkey. In Australia, culture and sensitivity testing of milk was available for 44% (146/331) of presentations. S. aureus was the most common bacteria isolated: 33% (48/146). Of these 48 S. aureus isolates, 3 (6%) were MRSA. There were 19 pus aspirates from breast abscesses in Australia and 18 in Germany. For the Australian data, the most common isolate was S. aureus resistant to penicillin (12/19, 63%). The complete microbiology results are presented in Table 4.
CRP levels were ordered frequently in some EDs and less frequently in others: 94% (46/49) of cases in Germany, 65% (217/331) in Australia, and none in Türkiye (Table 4). CRP levels were reported for Germany and Australia, of which 36/46 (78%) and 185/217 (85%), respectively, were elevated (≥ 5mg/L). Combining the CRP data from Australia and Germany, the median (interquartile range, IQR) CRP levels, was determined to be 35 (IQR = 10–77) mg/L. The median (IQR) CRP levels was observed to be the highest when taken within 24 to < 48 hours of onset of symptoms, albeit not statistically significant (Figure 1). Higher median CRP levels were observed amongst patients reporting subjective fever compared to those who did not (44 [IQR = 17–92] mg/L vs. 18.5 [IQR = 5–53.5] mg/L; p = 0.001). Similarly, the median CRP levels of patients who had lethargy or rigor/shivering were higher than those without (46 [IQR = 22–122] mg/L vs. 20 [IQR = 8.5–83] mg/L; p = 0.098 or 44 [IQR = 22–122] mg/L vs. 26 [IQR = 9–77] mg/L; p = 0.117), respectively, although these differences were not statistically significant. Notably, the median CRP levels did not differ statistically amongst patients with or without abscess (30 [IQR = 6 –96) mg/L vs. 36 [IQR = 11.5–73] mg/L; p = 0.672).
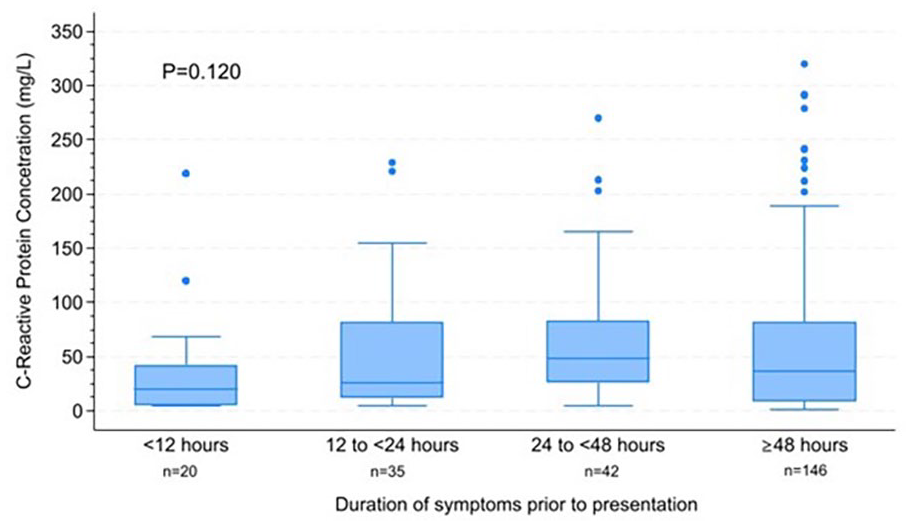
C-Reactive Protein (CRP) Levels Stratified by Duration of Symptoms Prior to Presentation. Kruskal-Wallis Test was Used to Evaluate the Statistical Significance of CRP Levels Across Different Duration of Symptoms Prior to Presentation.
Table 5 shows antibiotic prescriptions. At all sites, most women received antibiotic therapy. The most commonly prescribed antibiotic in Croatia and Türkiye was amoxicillin/clavulanate (57% [31/54] and 67% [28/42], respectively). Flucloxacillin was prescribed in 84% (273/322) of presentations in Australia, cefalexin in 62% (66/106) in Brazil, and cefuroxime in 80% (33/41) in Germany. Single-dose intravenous antibiotic was administered in 16% (52/331) of the ED presentations not requiring hospital admission in Australia.
Analgesia was prescribed in most ED presentations (Table 5). Paracetamol and ibuprofen were used commonly, while dipyrone was also used in Brazil (47%, 36/76). Lastly, the proportion of presentations that resulted in hospital admission ranged from 2% (1/65) in Croatia to 24% (79/331) in Australia and 73% (36/49) in Germany. The median duration of hospital admission in Australia and Germany was 2 days (IQR = 2–4) and 4 days (IQR = 3–6), respectively.
Discussion
Our international audit of women presenting to hospital ED confirms that most breast infections occur in the first 4 to 8 weeks postpartum (Lin et al., 2023; Lukassek et al., 2019; Wilson et al., 2020). The most common symptoms and signs recorded were those of breast inflammation and feeling feverish, consistent with clinical descriptions of mastitis (Amir et al., 2021; Radke, 2022; Scott, 2022).
Antibiotic prescription was high in all sites, ranging from 72% in Brazil to 97% in Australia. In Australia, the Therapeutic Guidelines provide best practice advice for clinicians about the appropriate use of medicines. The Therapeutic Guidelines: Antibiotic have recommended dicloxacillin or flucloxacillin to treat mastitis since at least 1998 (Joyner, 1998; Therapeutic Guidelines: Antibiotic, 2020). In the Australian ED, flucloxacillin was prescribed in 85% of cases, whereas cephalexin was highest in Brazil (62%), cefuroxime (80%) in Germany, and amoxicillin/clavulanate was highest in Croatia (57%) and Türkiye (67%). The use of broad-spectrum antibiotics in most sites is likely related to the lack of national guidelines in many countries. Where available, local antibiogram and/or antibiotic susceptibility data should be consulted to inform a more targeted choice of empirical antimicrobial therapy.
The diagnosis of lactational mastitis is made clinically, and the need for investigations varies with the presentation. Whilst diagnostic ultrasound is not routinely required in cases of mastitis, it may be indicated if an area of the breast is fluctuant or inflammation/hardness is not improving with antibiotic treatment (Scott, 2022). Some of the differences seen between the five settings relate to the clinical care pathways in each country; higher rates of breast abscess in some settings may be due to the practice of community referrals to a hospital ED only after initial management of mastitis has been instituted in the primary care setting and when abscess is suspected. Where primary care health workers do not commonly treat mastitis, patients present to EDs earlier, explaining the shorter duration of symptoms and fewer initial investigations.
Microbiological investigations were very low in all settings, except Australia. Culture and sensitivity of human milk is recommended when patients are not responding to prescribed antibiotics or MRSA prevalence is high (Dixon & Adetola, 2023; Mitchell et al., 2022). Since only 6% of S. aureus isolates in the Australian sample were MRSA, the threshold for milk culture and sensitivity may be too low in that ED site, while this investigation seems overlooked in other settings. Other studies have found higher rates of MRSA in breast abscess than in mastitis, for example, in Italy 91% of S. aureus associated with breast abscess was MRSA compared to 19% in mastitis (Rimoldi et al., 2020). Similarly, of the few MRSA isolated in our audit, a higher proportion was observed in breast abscesses than in mastitis (16% compared to 2% in Australian data).
Similar to that reported by Courtney et al. (2024), our data indicate that ultrasound-guided needle aspiration is the standard treatment of breast abscesses in Australia. Only 3/45 (7%) cases in Australia were managed by incision and drainage, compared to 19/20 (95%) in Germany and 3/5 (60%) in Türkiye. Data from a study of 64 Italian women with breast abscesses indicate that none needed incision and drainage (Pileri et al., 2022). Whilst most of the breast abscess cases (30/40, 75%) managed by aspiration in our audit resolved with a single aspiration, recurrent aspiration may be necessary (Mitchell et al., 2022). A recent study in Malaysia reported the median number of aspirations for lactational breast abscesses was two, with a range from one to seven (Lee et al., 2023). Drainage of abscess by means of percutaneous drain insertion has been suggested as an alternative (Mitchell et al., 2022), but none were recorded in our audit.
CRP plays important roles in host defense against invading pathogens, autoimmunity, and inflammation (Rizo-Tellez et al., 2023). It is used as a biomarker of inflammation, and may identify disease progression (Rizo-Tellez et al., 2023) or the need for treatment, for example, antibiotic use for respiratory infections (Zhang et al., 2022). The role of CRP in the management of mastitis, however, remains to be fully elucidated. Few studies have investigated CRP levels in mastitis and it is rarely used outside hospital settings (Fetherston et al., 2006; Grzeskowiak et al., 2024; Osterman & Rahm, 2000). Osterman and Rahm (2000) reported serum CRP levels in women with mastitis according to the type of bacteria isolated in their milk, although they found no difference in the CRP levels between patients with skin flora isolates in milk and those with potentially pathogenic bacteria. In their study of 14 women with mastitis, Fetherston et al. (2006) reported that CRP levels were the highest when measured on Day 2 of mastitis, similar to our findings. Further, CRP levels increased according to the severity of both the breast and systemic symptoms (Fetherston et al., 2006). Whilst subjective fever was associated with higher CRP levels in our study, further exploration is needed to assess the usefulness of this investigation in the diagnosis or treatment of mastitis.
Analgesia was not reported in all consultations, although it may have been undocumented, as most analgesics are available without prescription (Amir et al., 2024). Paracetamol was the most common analgesic in three sites, although ibuprofen is a safe anti-inflammatory medication generally recommended for management of mastitis (Mitchell et al., 2022).
Limitations
Audit studies are limited by the need to use data collected for clinical purposes rather than aimed at answering specific research questions. This audit was further limited by using data from different countries, where pathways to ED presentation varied. We did not plan to use statistical methods to compare findings between sites because of the expected differences. Each study site is not necessarily representative of the management of mastitis and breast abscess in the wider community or country.
Conclusions
In our audit of mastitis and breast abscess in EDs in five countries, most cases occurred in the first 8 weeks postpartum and presented with signs and symptoms of inflammation and fever. High rates of antibiotics were prescribed, and the type of antibiotic varied between countries. Consistent with other studies, the most common organism isolated from human milk was S. aureus, but no milk cultures were ordered at some sites. Breast abscesses were managed appropriately in Australia with ultrasound-guided needle aspiration, whereas incision and drainage common at some other sites. International evidence-based guidelines for the management of mastitis and breast abscesses are urgently needed.
Supplemental Material
sj-docx-1-jhl-10.1177_08903344251338245 – Supplemental material for Management of Mastitis in the Hospital Setting: An International Audit Study
Supplemental material, sj-docx-1-jhl-10.1177_08903344251338245 for Management of Mastitis in the Hospital Setting: An International Audit Study by Lisa H. Amir, Kelly P. Coca, Marcia Juliana Mello Da Silva, Marcia Massumi Okada, Güliz Onat Demir, Busra Duran, Süleyman Kargin, Kübra Güllü, Lara Delic, Magdalena Dragicevic, Maria Rosenbauer, Mee-Har Michelle Ngan, Wirawan Jeong, Moni Rani Saha and Irena Zakarija-Grkovic in Journal of Human Lactation
Footnotes
Acknowledgements
Thank you to the nurses Gabriely Thays Caserta and Paula Dias for supporting data collection in Brazil.
Author Contributions
Disclosures and Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No funding was received for this project. KPC has research productivity scholarships of the National Council for Scientific and Technological Development (CNPq).
Supplemental Material
Supplementary Material may be found in the “Supplemental material” tab in the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.