
Abstract
The climate crisis is an emerging global challenge that poses potential risks to breastfeeding practices and outcomes. There are multifaceted effects of climate change affecting the breastfeeding dyad across environmental, societal, and human health dimensions. Breastfeeding support in the face of climate change will require solutions at the structural level—healthcare, community, and workplace settings—and at the mother-infant dyad level. Breastfeeding can additionally be an adaptive response to crisis situations and can mitigate some of the environmental challenges associated with climate change. Despite the undeniable significance of climate change on breastfeeding (and vice versa), our perspective as experts in the field is that this topic has not been systematically addressed. Although we highlight some of the challenges, potential solutions, and co-benefits of breastfeeding in the context of climate change, there are numerous issues that could be further explored and necessitate additional preparedness planning.
Key Messages
The climate crisis is looming and will affect maternal and child health outcomes.
Breastfeeding can contribute to climate resilience but may also be threatened by climate change.
An understanding of the complex interactions between climate change and the First Food landscape is paramount.
According to the World Health Organization (WHO, 2021), The Lancet Countdown (Watts et al., 2018), and an editorial published in over 200 medical journals (Atwoli et al., 2021), climate change is the greatest threat to human health in this century. Human-induced climate change, a consequence of burning fossil fuels beginning in the 1850s, is leading to more severe floods, hurricanes, wildfires, and heat waves. These weather events have caused increased damage to infrastructure; additional mortality and morbidity; human migration and displacement; damaged livelihoods; increased mental health issues; and increased inequality (Intergovernmental Panel on Climate Change, 2022). The climate crisis is clearly upon us. Strategies to address mitigation, adaptation, and resilience are urgently needed.
Climate change is already significantly affecting human health, including maternal and child health. The National Climate and Health Assessment divides climate influences into seven broad categories: heat-related illness, poor air quality, extreme weather events, vector-borne diseases, food- and water-related infections, nutrition, and mental health (United States Global Change Research Program, 2023). While mechanisms are still unclear, extreme heat, in combination with air pollution, has also had adverse effects on pregnancies, including increased preterm deliveries, low birth weights, and stillbirths (Bekkar et al., 2020). Although the American College of Obstetricians and Gynecologists (ACOG) and the International Federation of Gynecology and Obstetrics (FIGO) have raised concerns about the potential implications of the climate crisis on maternal and neonatal health outcomes (ACOG, 2021; ACOG Committee on Obstetric Practice, 2021; Di Renzo et al., 2015), research on climate effects on lactation is still evolving.
Commercial milk formula may have limited benefit in climate emergencies due to frequent supply chain interruptions, risk of contaminated water supplies and loss of power necessary for cleaning bottles. In addition to the potential contaminants in commercial milk formula (e.g., drugs, pesticides, mycotoxins, and heavy metals), production has a high carbon footprint (generating greenhouse gases from the dairy operation phase through manufacturing, packaging, transportation, and disposal), making use of commercial milk formula a contributor to the climate crisis as well as suboptimal as an adaptation strategy (de Mendonca Pereira, et al., 2020) (Ji et al., 2009) (LaKind et al., 2023) (Langman et al., 2009).
Breastfeeding, in contrast, provides an opportunity for mitigation, adaptation, and community resiliency, in addition to the well-known health benefits for lactating parents and infants. Exploring the environmental, social, and health aspects of climate change is foundational to ensuring that optimal systems are in place to maximize breastfeeding for lactating parents and their infants in the climate crisis.
Multidimensional Climate Influences and Human Health
Climate change exerts multifaceted effects across environmental, societal, and health dimensions. Environmental aspects include extreme temperatures, natural disasters, and agricultural influences. Society, particularly vulnerable groups, is affected through displacement, loss of livelihood, and conflict. Finally, health effects of climate change include heat-related conditions, exposure to pollutants, changes in disease patterns, and heightened mental health challenges.
Environmental Influences
Extreme Temperatures
Elevated temperatures and prolonged heat waves during pregnancy can have significant repercussions on breastfeeding. In an extremely hot climate, pregnant women face an increased risk of premature birth, stillbirth, low birth weight, and pre-eclampsia (Bekkar et al., 2020; DeNicola et al., 2019; Lusambili & Nakstad, 2023). Premature birth could have direct effects on a parent’s ability to breastfeed as infants may require advanced or critical care, parents may be unable to express sufficient milk for their vulnerable newborns, and low birth weight may lead to concerns about weight gain and the need for supplementation, and result in over-reliance on commercial milk formula. Furthermore, heat and pollutants are associated with congenital anomalies, including heart defects and cataracts, which may also introduce challenges to exclusive breastfeeding (Van Zutphen et al., 2012; Zhang W., et al., 2019). In the setting of chronic heat exposure, breastfed newborns can suffer from dehydration, both from free water loss and insufficient human milk production to replace that deficit (Lusambili & Nakstad, 2023). Additionally, there is some evidence that extreme heat also makes it more difficult to exclusively breastfeed, especially for newborns less than 3 months of age (Part et al., 2022). Thus, extreme temperatures may contribute to reduced breastfeeding frequency and duration.
Natural Disasters and Changes in Precipitation
Climate change-induced disasters are increasing in frequency and severity. Communities have varying levels of resiliency and inherent risk. In a study of the Gulf Coast of the United States, urban areas experienced high breastfeeding initiation rates but were also the most at risk for disasters, whereas many rural communities may have generally faced less risk for extreme events but exhibited more social vulnerability and less resilience should a disaster strike (Grubesic & Durbin, 2022).
In the wake of a climate disaster, the results of one study demonstrated that women and children were 14 times more likely to die (Gaard, 2017). Hurricanes, floods, and wildfires can disrupt the healthcare delivery system, upending care on multiple fronts, including postnatal care and infant follow-up appointments. Families can be directly harmed by injury from debris, building collapse, and flooding, and can be displaced by home damage. Increased rainfall and flooding may contaminate water sources, increasing the risk of waterborne diseases (especially for infants reliant on commercial milk formula). (Emergency Nutrition Network) Wildfire exposure may be associated with adverse birth outcomes, including prematurity, low birth weight, birth defects, and increased gestational diabetes mellitus and hypertension. Furthermore, inappropriate distribution and marketing of commercial milk formula following wildfire evacuation has been shown to decrease rates of breastfeeding (DeYoung et al., 2018).
During times of disaster, pediatricians and other health care workers may be required to triage more urgent issues eroding breastfeeding support infrastructure. These circumstances can leave mothers with limited knowledge or resources, leading to decreased breastfeeding self-efficacy and an over-reliance on commercial milk formula (Ratnayake Mudiyanselage et al., 2022).
Agricultural and Nutrition Influences
In the face of increasing levels of atmospheric carbon dioxide (CO2), some staple crops including wheat, rice, and pulses, contain decreased quantities of iron, zinc, and protein compared to baseline CO2 levels (M. R. Smith & Myers, 2018). These alterations can be expected to push millions more women and children into deficient nutrient states, particularly those whose diets are already marginal and contain minimal animal proteins (Al-Jawaldeh et al., 2022; Blakstad & Smith, 2020; Macdiarmid & Whybrow, 2019; Myers et al., 2017; Swinburn et al., 2019). These changes are not expected to significantly compromise infant nutrition during the first 6 months of exclusive breastfeeding, as breastfeeding is protective in supporting the infant’s needs for full-term healthy newborns despite restrictions in maternal diet (Dewey et al., 2002). However, iron supplementation may be necessary for infants born prematurely or with low birth weight (Dewey et al., 2004), conditions that may be exacerbated by maternal undernutrition, and infants with decreased access to complementary foods rich in the iron, zinc, and protein necessary in addition to continued breastfeeding to maintain a healthy micronutrient status during the second half of infancy (Obbagy et al., 2019). Furthermore, health effects can be anticipated in the lactating individual, including iron deficiency anemia and wasting as a result of these nutritional changes.
Social Aspects
Vulnerable Populations
Socially and medically vulnerable populations are most at risk of harm induced by climate change but have the least agency and voice. Pregnant people and infants, particularly those of color and those living in low-income communities globally, are among the populations most vulnerable to the adverse affects of the climate crisis (Bekkar et al., 2020; Kuehn & McCormick, 2017; Parry et al., 2007; United Nations Climate Change, 2022). Ecological and social determinants of health determine 80% of patient outcomes and have historical grounding in colonialism, imperialism, capitalism, and other interlocking systems of oppression within political ecology, which views human practices—including breastfeeding and climate factors—as inextricably tied together in a larger economic-social-political system (Reno & Hyder, 2018; Zadkovic et al., 2021).
Displacement, Loss of Livelihood, Conflict
Over the long-term, climate hazards can upend agricultural communities leading to loss of livelihoods and loss of livability in highly exposed regions. The result is often mass climate migration and civil conflict with desertification of land and the inability to successfully grow crops. This leads not only to malnutrition from decreased access to food, but also the possibility of violence and trauma from civil strife (Palinkas & Wong, 2020; Ramadan & Ataallah, 2021; Reichman, 2022; van Daalen et al., 2021). Among this extremely vulnerable population, breastfeeding infants have a somewhat more secured means of consistent nutrition than infants reliant on formula.
Health Aspects
The multifaceted health effects of climate change encompass an array of factors. These include elevated risks associated with heat exposure and health effects arising from the presence of particulate matter and ground-level ozone; the influence of environmental pollutants; shifts in disease patterns, particularly infections; and the significance of mental health challenges in the context of a changing climate.
Health Effects From Heat, Particulate Matter and Ground Level Ozone
The health affects of climate change can be seen in virtually every organ system, (United States Centers for Disease Control and Prevention [CDC], 2022a, Climate and Health Program). Worsening rates of heart attacks, strokes, and pulmonary disease, new onset kidney disease of unknown cause, and many more health outcomes are recognized as results of a changing climate. (Du et al., 2016; Shah et al., 2015)
Environmental Pollutants
Fossil fuel combustion produces both the greenhouse gases that contribute to climate change and air pollution (including particulate matter 2.5 [PM 2.5], ozone, sulfur dioxide, nitrogen dioxide, and others) that leads to adverse health outcomes.
While influences of constituents of air pollution and their resultant effects on human health are being actively studied, a common disease pathway relies on the systemic absorption of the particles and molecules which can cross the distal alveoli and circulate in the bloodstream, leading to myriad downstream effects (K. H. Kim, et al., 2015). The pathophysiologic mechanisms are hypothesized as follows: (1) oxidative stress from nitrogen dioxide (NO2), ozone (O3), and particulate matter (PM); Carré et al., 2017; Hong et al., 2016; Kim et al., 2018), (2) inflammatory effects from PM, heavy metals, NO2 (Calderon-Garciduenas, 2008; Hampel, et al., 2015; Hong et al., 2016; Thompson et al., 2010; Zhao et al., 2019); (3) genotoxic effects from PM, polycyclic aromatic hydrocarbons, benzopyrene (Bełcik et al., 2018; Sram et al., 2013; Zielinska & Hamulka, 2019); (4) induction of the coagulation system (Baccarelli et al, 2007); (5) epigenetic changes (Alfano et al., 2018; Kim, 2018; Zielinska & Hamulka, 2019); (6) tumor promotion of mutant cells (Hill et al., 2023); (7) endocrine disruption from polycyclic aromatic hydrocarbons, PM-heavy metals, NO2 (Carré et al., 2017; deBont, 2019; Huang et al., 2017); (8) downregulation of antimicrobial proteins (Zhang S., et al., 2019); (9) altered immune system response (Herr et al., 2010; D. Kim et al., 2018; Liu et al., 2019; Zhao et al., 2019); (10) activation of stress systems (hypothalamus–pituitary–adrenal and sympathetic–adrenal–medullary axes; Li et al., 2017; Zielinska & Hamulka, 2019); and (11) vitamin D deficiency by directly blocking ultraviolet B photons and indirectly by decreasing outdoor activity (Mousavi et al., 2019). All these mechanisms can influence downstream processes, leading to disease across multiple systems that can affect breastfeeding parents, infants, and children (Al-Kindi et al., 2020; J. B. Kim et al., 2020; Lin et al., 2023; Shen et al., 2021).
Exposure to PM2.5 (particulate matter with fine, inhalable particles less than 2.5 micrometers in diameter) is estimated to contribute to one in five premature deaths (Vohra et al., 2021). First trimester exposure to PM2.5 and other air pollutant constituents (ammonium, sulfate, nitrate, organic carbon, soil dust, and black carbon) has been inversely associated with intelligence, an effect mitigated by longer breastfeeding duration (Cheng et al., 2023; Sun et al., 2023). Pregnant women, infants and children are especially vulnerable to the influences of air pollution, which is projected to cost 1% of gross domestic product (
Geocoding particulate matter has identified changes to the maternal microbiome—regardless of race or socioeconomic status—that are associated with preterm delivery and may affect the ontogeny of the infant’s immune system (Just et al., 2020) (Dawod et al., 2021) (Lopez Leyva et al., 2022). Pollutants, including heavy metals in particulate matter, polycyclic aromatic hydrocarbons, pesticides, and persistent organic pollutants, can contaminate human milk and pose health threats to both mothers and infants (Péter et al., 2015; Zielinska & Hamulka, 2019). Nevertheless, human milk components, including long-chain polyunsaturated fatty acids (LC PUFA), antioxidant vitamins, carotenoids, flavonoids, immunoglobulins, and cytokines, offset the potential harm of human milk pollutants and result in better health outcomes for mother and baby (Péter et al., 2015; Zielinska & Hamulka, 2019). More research is needed to understand the full scope of environmental toxins on breastfeeding, human milk, and associated infant health outcomes.
Changes in Infectious Patterns
Risk for various infections increases with climate change. Low breastfeeding rates in countries at high-risk for climate change contribute to preventable child deaths, diarrhea, and pneumonia (Chalupka et al., 2023). Vector-borne illnesses have expanded into regions that were not previously hospitable, increasing exposure to un-inoculated populations. Natural disasters can also increase potential exposure to food-or water-borne infection. Crowding resulting from displacement and use of shelters can promote the spread of common infections, including respiratory and gastrointestinal viruses.
In a large diarrheal outbreak in Botswana that coincided with heavy rains, almost all of the children hospitalized during the outbreak were not breastfed (88%) and under 2 years old (97%) (Creek et al., 2010). Infections from commercial milk formula or bottle contamination pose significant infant risks even in the absence of environmental pressures (Martín-Carrasco et al., 2023). Opportunistic and other pathogens can cause a range of serious diseases, from meningitis and brain abscesses to necrotizing enterocolitis (Gottlieb, 2022; Norberg, et al., 2012; US CDC, 2022). Rare contaminants may have little broader public health concern but pose a significant risk to infants. (Friedemann, 2007).
Mental Health
Increased stress and anxiety from any cause, including climate-related factors, can affect breastfeeding (Olson & Metz, 2020). Climate disasters are associated with post-traumatic stress disorder (PTSD). Heat has been associated with increased anxiety and depression along with increased violence (Anderson, 1989; B. S. Levy & Sidel, 2014; B. S. Levy et al., 2017; Palinkas & Wong, 2020). Mental health has been adversely affected, and one study has shown that women who have been evacuated from a wildfire more frequently stop breastfeeding (Evans et al, 2022). Air pollution itself may affect mental health (Abed Al Ahad et al., 2022; Hu, 2021).
There are increased episodes of gun violence and other forms of violence, including interpersonal abuse with extreme heat (Chersich et al., 2019; Lyons et al., 2022; Sanz-Barbero et al., 2018). For those dependent on agriculture or with other livelihoods dependent on nature, instability of reliable income and job security can add to family stress, interpersonal violence, and substance abuse or alcoholism among partners (Scarpa et al., 2022).
The effects of ecoanxiety and solastalgia may be experienced by individuals of any gender and age but could be particularly intense for parents who recognize that they have a new life to protect and care for (Olson & Metz, 2020). These factors can increase postpartum depression and reduce maternal–infant bonding. Overarching concerns related to eco-anxiety can overwhelm postpartum parents with existing maternal stresses and allostatic load, elevating the need to develop tools that will predict communities and individuals who are experiencing the highest levels of climate-related hazards with a goal of reducing stress and increasing resilience (Barkin et al., 2022; Olson & Metz, 2020).
Solutions Include Mitigation, Adaptation, Resilience
An article in the 2023 Lancet Breastfeeding Series by Pérez-Escamilla et al. (2023) introduces a revised breastfeeding framework (see Figure 1). The framework categorizes breastfeeding determinants into three key levels: Structural, Settings, and Mother-Infant Dyad. To effectively address the challenges climate change poses to breastfeeding, solutions must be implemented across all three of these levels.
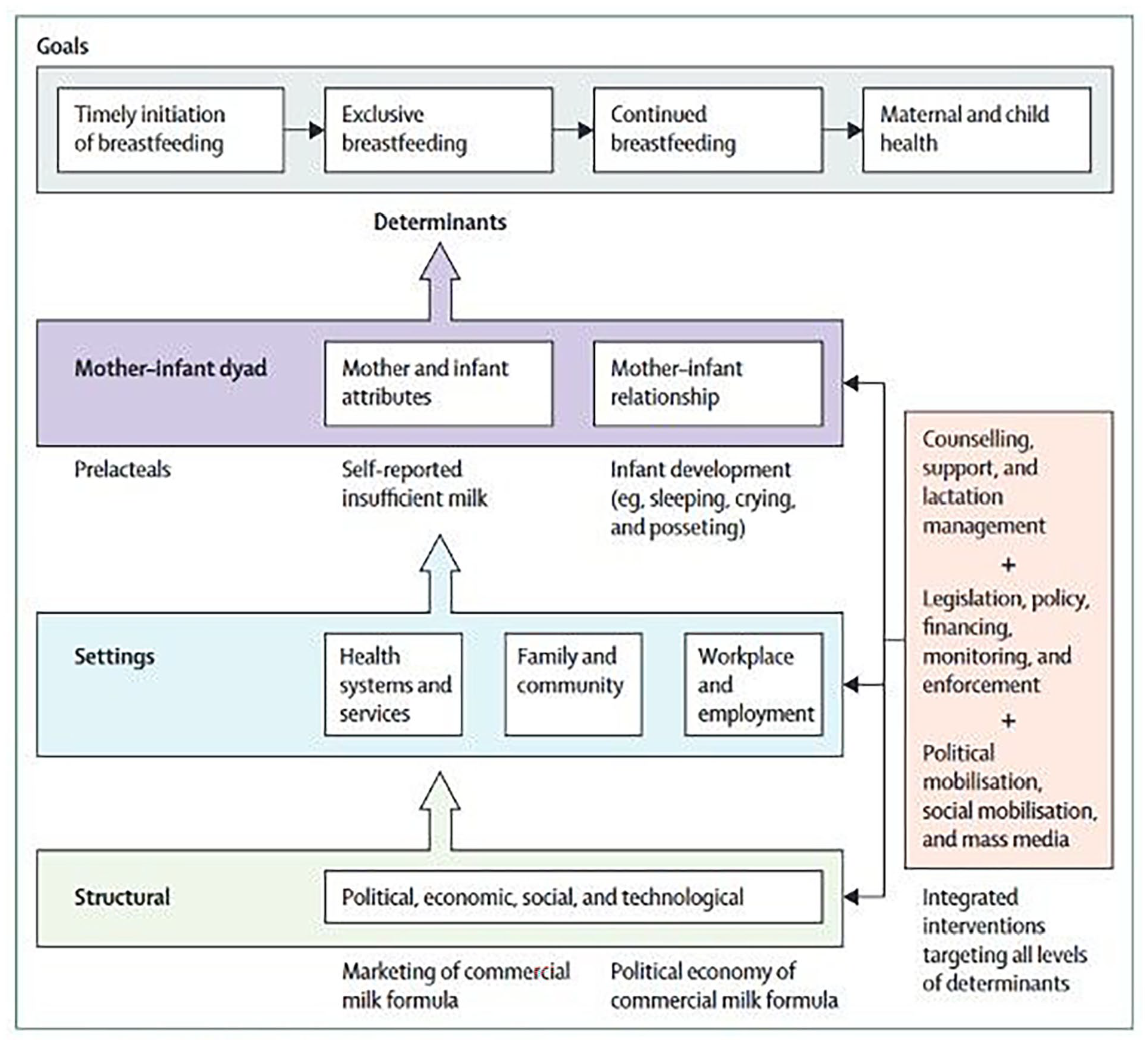
The 2023 Lancet Breastfeeding Series Framework.
Structural Solutions
Structural solutions involve drawing lessons from both COVID-19 and non-climate-related disasters, alongside the development of comprehensive healthcare policies at the system level.
Learning From COVID and Non-Climate-Related Disasters
Lessons from the pandemic can inform strategies for addressing breastfeeding support in the context of climate change. The pandemic, characterized by social isolation and decreased in-person resources, had significant affects on breastfeeding support.
During the Covid-19 pandemic, the United States Centers for Disease Control and Prevention (U.S. CDC) reported a 17.9% decrease in in-person lactation support and most (72.9%) U. S. hospitals reported discharging mothers and newborns less than 48 hours after birth (Perrine et al., 2020). Despite these strains on the system, 48.7% still provided virtual breastfeeding consultation (Perrine et al., 2020; Spatz, 2021). Telemedicine options and flexibility in meeting patients’ needs are important in changing environmental conditions, but also depend on access to energy and technology. One key takeaway from the pandemic may be to embrace opportunities for virtual breastfeeding guidance while still expanding in-person technical breastfeeding assistance (Berveiller et al., 2020; Spatz, 2021; Stuebe, 2020). In one multi-country study of five nations (Thailand, the United Kingdom, South Korea, Taiwan, and Brazil), authors describe online support groups and in-person or telephone contact with healthcare workers as associated with increased odds of achieving the intended or longer breastfeeding duration (Chien et al., 2022).
Lessons can also be learned from natural disasters unrelated to climate change. Earthquakes have been associated with increased Cesarean deliveries due to uncertainty about birth timing and fear of hospital collapse. During these disasters formula distribution increased and efforts to support breastfeeding decreased. Discharge from hospitals can be expedited leaving patients with no “home” upon discharge (Bengin et al., 2010; Lawrence, 2011). This is an example of data that can help to inform the anticipatory development of climate action plans to support breastfeeding and lactating women through other disasters or disruptions.
System-Level Healthcare Policy
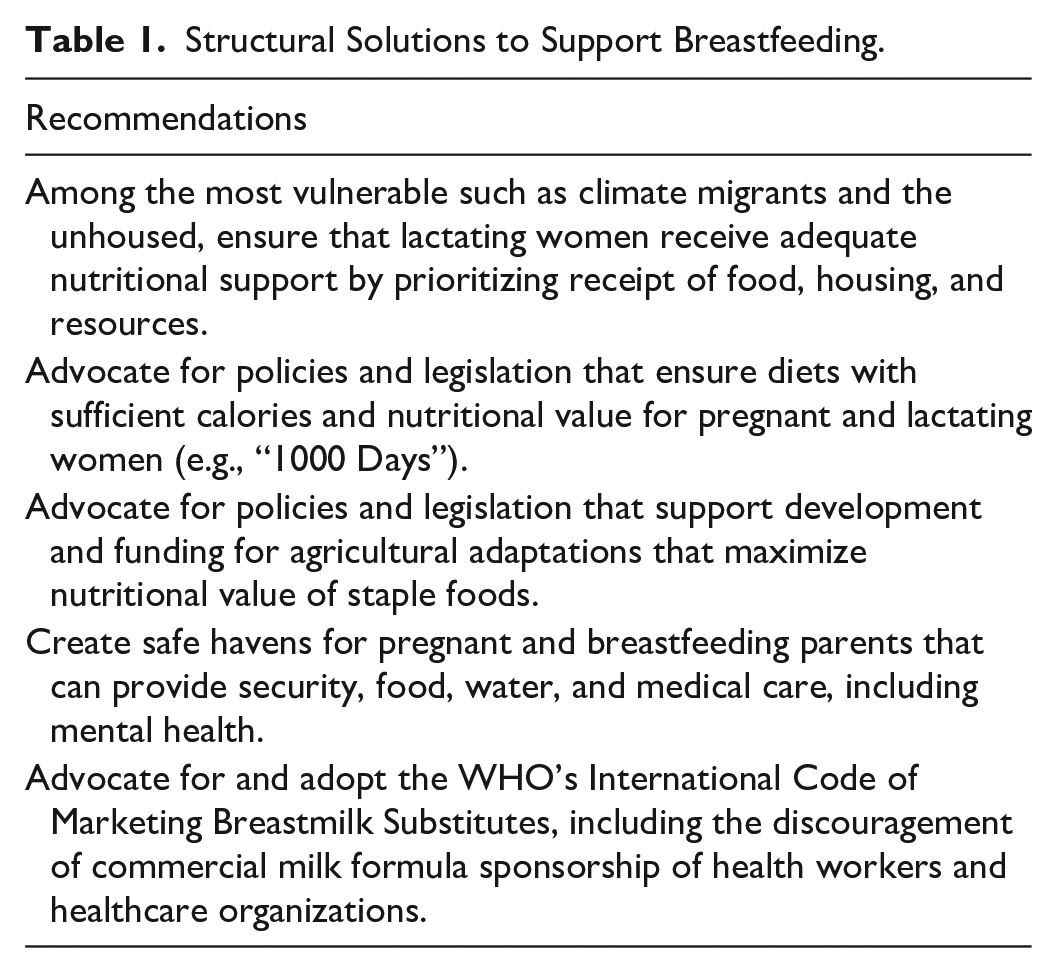
Incorporating the necessary constituents and complexity into climate action plans requires input from many stakeholders in health, business, government, and the community, and must be generated by iterative co-production of plans, incorporating a systems-thinking approach. Lactation experts have opportunities to partner with others across sectors and disciplines to facilitate adaptation, mitigation, and resiliency strategies that support the needs of breastfeeding mothers and infants (Table 1).
Structural Solutions to Support Breastfeeding.
Emphasis on Preventative Care Through Policy
Planning for infant feeding in the face of climate change includes consideration of the best use of resources. Many healthcare systems are over-reliant on curative care. In the United States, only 12% of healthcare spending is directed at preventative services (Baker et al., 2023). Similarly, the ability to rapidly recover and rebuild after climate disasters will require greater investment in preventative services (Brennan et al., 2020).
Ecological and agricultural approaches can inform efforts to understand the influences of maternal nutrition on breastfeeding by examining contextual factors, including the community, the healthcare system, and societal and environmental contexts more broadly (Tiedje et al., 2002). The interplay of these socio-environmental conditions can influence maternal breastfeeding practices (Sellen, 2001). Extreme weather events, for example, may result in parents migrating, leading to a lack of housing, or a lack of private spaces for breastfeeding. Addressing these and the exhaustion, stress, and decreased fluid and nutritional intake (Hwang et al., 2021) concomitant with migration are factors that should be prioritized among aid groups. At the intersection of natural disasters and cultural norms, lactating parents should receive adequate nutritional and societal support to protect, promote, and support breastfeeding.
The epidemics of obesity, undernutrition, and climate change interact to produce shared threats to child health. Even within the United States, the world’s wealthiest economy, around 11% of children are food insecure (Agostoni et al., 2023; Ullmann et al., 2022). Preventative measures taken in the short term to address these issues are important for mitigation, future adaptation, and resilience. The epidemic of obesity, which can affect lactating parents, for instance, has environmental effects. Specifically, there is a bidirectional relationship between adiposity and global warming as people will have less adaptive thermogenesis at higher ambient temperatures and become less physically active, while also increasing their carbon footprint (Koch et al., 2021; Swinburn et al., 2019). An emphasis on breastfeeding would be anticipated to reduce the number of overweight children, producing healthier weight populations (Myr, 2008).
Agricultural strategies should also be employed in prevention efforts. In the face of climate change induced compromised staple food quality, selecting cultivars with maximally accessible iron, zinc, and protein, optimizing agricultural techniques, and biofortifying and/or supplementing maternal diets are some strategies to address the potential adverse effects.
Utilization of Technology
Technological advances can be assessed for opportunities to build resilience into infrastructure in anticipation of natural disasters and other influences from gradual progressive changes, including warming temperatures. Either a heat wave or an acute storm event may lead to grid failure or power outages. Solutions must be tailored to the specific community since urban and rural communities have divergent profiles that require tailored resilience strategies. Rural areas, for instance, experience more social vulnerability and less resilience should a disaster strike (Grubesic & Durbin, 2022), whereas urban areas and environmental justice communities also have multiple overlaying risk factors, including urban heat islands, poor water quality, and concentrated air pollution from industrial and transportation sources. (Baker et al., 2023; LeClair et al., 2021; Levy & Hernández, 2022; Resnik, 2022).
Safe Havens Policies
Governments, relief agencies, and other nonprofits should create safe havens for pregnant and breastfeeding mothers that can provide security, food, water, and medical care, including mental health.
Adapt WHO International Code for Marketing of Breastmilk Substitutes
The major challenge in breastfeeding identified in the aftermath of natural disasters has been the violation of The International Code for Marketing of Breastmilk Substitutes by aid organizations and governments (Hwang et al., 2021). Legacy practices, including solicitation of commercial milk formula donations, can have detrimental effects. Unfortunately, many aid workers are unfamiliar with infant feeding in emergencies (IFE) programs, leading to the unsolicited provision of commercial milk formula. Alternative practices are needed, including soliciting support for and promoting lactation disaster relief organizations, milk banks and wet nurse programs (CDC, 2023a; Infant Feeding in Emergencies Core Group, 2017; Marinelli, 2020; United Nations Office for Coordination of Humanitarian Affairs, 2015). Furthermore, to ensure responsible and safe infant feeding practices in disaster settings, infants who are not breastfed should undergo assessment by a qualified health or nutrition worker. In cases where commercial milk formula is necessary, it is crucial to implement effective practices in distribution to minimize inappropriate usage. In cases where commercial milk formula is needed, it should be purchased. Donations should not be accepted (Gribble & Palmquist, 2022).
Settings Solutions
Family and Community
Family and community solutions should be tailored to specific contextual circumstances and identify and utilize funding sources to support community planning endeavors. In these efforts, it is important to consider social justice principles and promote food sovereignty to address the unique needs and strengths of each community.
Planning Based on Contextual Circumstances
The contextual circumstances of country, region, and people, as well as the unique vulnerabilities, resiliency, and adaptive capacity in each area, influences the uptake of breastfeeding. Well-designed climate action plans will integrate these complex variables and include explicit planning designed to maximize health for mothers and infants. The framework demands strengthening healthcare systems as well as critical societal and community infrastructure, particularly in vulnerable regions prone to climate-related disaster.
Utilizing Funding Sources
Policy discussions should include financial considerations. As with many preventative health measures, adaptation and mitigation of climate effects are more cost-effective than addressing the consequences of climate disasters (United States National Oceanic and Atmospheric Administration National Centers for Environmental Information, 2023; Newburger, 2022; United States Environmental Protection Agency Office of Air and Radiation, 2011). Politicians, public health officials, and healthcare professionals should be familiar with climate resilience funding, for example, the Green Climate Fund (n.d.), to rapidly rebuild healthcare infrastructure, including breastfeeding support services.
Food Sovereignty and Social Justice
There is growing policy interest in social justice issues related to health and food. Health and gender inequities in the food system are accentuated with breastfeeding (Weiler et al., 2015). Sourcing food proximate to communities, when feasible, will be an important aspect of community resilience and food security in the setting of natural disasters. (Tomori, 2023) Local food acquisition has the additional benefit of decreasing transportation-related greenhouse gas expenditures. Food sovereignty, especially among indigenous communities, acknowledges the importance of core domains of community ownership, traditional food knowledge, inclusion/promotion of cultural foods, and environmental/intervention sustainability. This can involve local food procurement, innovation hubs, and several types of greenhouses including hydroponics and vertical farming, to work towards a more localized food system (Millenburg et al., 2023). Maintaining maternal nutrition through attention to, and inclusion of, traditional food knowledge as well as innovative agricultural practices can support parents and infants (Abdul et al., 2023).
Healthcare Systems and Services
Healthcare systems and services should be given careful consideration. Prioritizing telehealth, optimizing the healthcare workforce and care models, addressing climate-related social determinants of health, providing training and education for healthcare workers, and establishing plans for redundancy, are important to ensure robust healthcare services in the face of climate change challenges (Table 2).
Healthcare Systems and Services Solutions.

Note. Adapted in part from “Preparedness Checklist for Pediatric Practices” by the American Association of Pediatrics (2013), American Academy of Pediatrics. (2020). & “Lactation & Infant Feeding In Emergencies (L.I.F.E.) Support – Basic Kit v 1.2” by the Carolina Global Breastfeeding Institute (2018 September)., (https://sph.unc.edu/cgbi/cgbi-resources-l-i-f-e-support-basic-kit/) & “Infant and Young Child Feeding in Emergencies Jefferson County Colorado”, by Jefferson County Colorado Public Health (2023), (Infant and Young Child Feeding in Emergencies, Jefferson County, CO (CDC 2022b), (International Lactation Consultant Association, 2009).
Telehealth
Planning for the medical needs of lactating parents and infants in emergency situations is crucial. In developed countries with a strong internet infrastructure and a dependable energy source, telehealth may allow ongoing breastfeeding support which may be unavailable in developing areas.
Optimizing the Workforce and Care Models
In emergency situations, it is essential for healthcare workers to collaborate cohesively and allocate resources and expertise effectively to enhance the overall response. When rescue workers and urgent care providers are addressing acute needs, and physicians are triaging complex conditions during an extreme weather event, midwives, nurses, lactation support professionals and other trained lactation specialists play a pivotal role in providing effective support to women in need (Mohapatra & Samantaray, 2023; Renfrew et al., 2014). Relying on the expertise of healthcare professionals from diverse backgrounds and specialties guarantees improved access to care for parents and children (Fernandez Turienzo et al., 2021; Sacks et al., 2022; Turner et al., 2022).
An emphasis on integrating the full spectrum of healthcare professionals in response can potentially mitigate the effects of climate change on breastfeeding in various ways. In higher-resourced countries, for example, increased integration of midwives into the formal healthcare system has been found to be a key determinant of optimal maternal-newborn outcomes (Vedam et al., 2018). Health systems that utilize services described as “midwife-led” lead to better breastfeeding outcomes (Baker et al., 2023). In lower-resourced countries, shortages of healthcare providers can be ameliorated through increased training and incorporation of midwives to the healthcare workforce (Nove et al., 2021; Sangy et al., 2023). Developing community health worker labor forces can support preventative health goals as well as improve responses in humanitarian emergencies, particularly among marginalized populations (United States Breastfeeding Committee, n.d.). Centralization of resources can limit accessibility and increase transportation requirements, whereas expansion of services and utilization of midwives, nurses, advanced practice providers, community health workers, lactation support providers, and others, can mitigate the concentration of healthcare professionals in large centers (Chesnel et al, 2021; Grant et al., 2018; Szucs et al., 2009).
Evaluate Climate-Related Social Determinants of Health
Clinicians should assess access to air conditioning or advise on local cooling stations. Individuals' circumstances will weigh heavily into available options for mothers and their infants to adapt to climate events. During heat waves, for instance, air conditioning and cooling centers are very effective means of reducing adverse health events. Their benefits are limited though, due to scarcity of access in many situations. In urban areas, they may worsen ambient temperatures (i.e., causing worsening of urban heat island effects; Jay et al., 2021).
Sustainable heat-reducing interventions, including increasing shade exposure, use of electric fans (at least up to 38 °C), sponging of skin with water from a spray bottle or sponge, taking physical activity breaks, and removing or modifying clothing, are both beneficial and more available (CDC, 2020; Jay et al., 2021).
Training and Education for Health Workers
Education and awareness regarding the climate health influences on women, children, and breastfeeding is critical, not only for patients, but also for healthcare professionals, communities, and policymakers to promote and prioritize during disasters and periods between disasters. Informational campaigns can disseminate accurate knowledge in advance of climate effects to create a culture that values breastfeeding so that targeted support of breastfeeding can be augmented during a disaster. Training emergency workers to support breastfeeding, and providing culturally sensitive peer support personnel to help mothers continue breastfeeding helps to overcome the effects that disasters can have on disruption of lactation (Dall’Oglio et al., 2020).
Planning for Redundancy
Creating redundancy through multiple and overlapping systems can ensure patient care even if one aspect of a system fails. Combining community birth centers and hospitals, for example, with telehealth, primary care, midwives, lactation experts, nurses, and aides, can deliver care to meet the needs of mothers in a community. (Fox et al., 2019; Office of the Assistant Secretary for Health [OASH], 2023)
Redundant planning for infant nutrition is also necessary: Breastfeeding, banked human milk, cross-nursing, wet nursing and, (in hopefully rare circumstances) commercial milk formula, will all require consideration to ensure adequate infant nutrition in the unpredictable crises that are before us.
Employment and Workplace
The parental costs of breastfeeding must also be factored into policy solutions. While many consider breastfeeding to be “free,” investment in the time and energy of lactating needs to be considered, as well as the cost of the healthworkers who help support breastfeeding. Breastfeeding is not the sole responsibility of the lactating parent, but rather a result of a socio-ecological framework of support that includes health systems, communities, workplace, and employment (Pérez-Escamilla et al., 2023). Societies should value the work of women, yet the unpaid “care work” of women is largely unmeasured and under-recognized (Baker et al., 2023). While work is often cited as the main reason for not breastfeeding, prematurely weaning from breastfeeding, or expressing milk, many countries have yet to develop policies that provide paid leave for mothering and parenting (Chai et al., 2018). Other industrialized countries that have national paid maternity-leave policies of 12 weeks or more have benefited from increased breastfeeding initiation and duration and the improved mental and physical health of both mothers and children. (Navarro-Rosenblatt & Garmendia, 2018; Van Niel et al., 2020). A society that attributes value to the work of women and offsets the costs of breastfeeding will be automatically more resilient to environmental changes already affecting society.
Breastfeeding Dyad Solutions
Healthcare providers have various opportunities to influence the breastfeeding dyad in anticipation of, or response to, disasters. These include disaster planning, education, and healthcare support, along with specialized considerations, including milk sharing and expression. Almost half of lactating parents globally lack confidence in breastfeeding and self-report insufficient milk supply, leading to the introduction of commercial milk formula and premature weaning (Pérez-Escamilla et al., 2023). Effectively communicating to help in achieving personal breastfeeding goals, as well as conveying evidence-based information about the value of breastfeeding both in ordinary and extraordinary circumstances, including extreme weather events, should be incorporated in parental healthcare visits.
Milk Sharing
Donor milk from wet nurses or from milk banks may be a viable alternative if a parent is unable to breastfeed their child, whether due to illness, separation, death, or lactation insufficiency, whether or not it pertains to climate change (Nove et al., 2021). Breastfeeding is recommended under most conditions; however, there are some contraindications to breastfeeding, including those who have HIV and are not on antiretroviral therapy (ART), and/or do not have a suppressed viral load during pregnancy (at a minimum during third trimester), delivery, and postpartum, mothers with HTLV I and II, mothers using illicit drugs, and mothers with suspected or confirmed Ebola. (CDC, 2023b). There are also those who have conditions that require temporary cessation of breastfeeding, including untreated brucellosis or certain medications. In both circumstances, an alternative to feeding commercial milk formula may be donor milk if it can be accessed in a timely manner. Using donor milk from a human milk bank may be cost-prohibitive but is safe and well-established, and milk sharing has increased in popularity (Haiden & Ziegler, 2016). While the safety of milk sharing cannot be fully assured, healthcare practitioners can play important roles in providing counseling to families choosing this option (Kullmann et al., 2022). Unregulated human milk sharing is not recommended under routine circumstances and could introduce infection or contamination. Thus, regulation of the milk-sharing process should be established before a climate disaster (Martino & Spatz, 2014; Spatz, 2016; Spatz, 2021).
Wet nursing and cross-nursing are culturally acceptable practices in many communities. While wet nurses are not considered to have the same social status as the employer, cross-nursing, including milk sharing between arranged individuals, involves breastfeeding between equals and may represent a more egalitarian practice (Thorley, 2008). Wet nursing commonly occurs within families (Azad et al., 2019), which supports its potential egalitarian and communal nature. There are divergent opinions on the practice of milk sharing in the Western world compared to other global areas. Human milk, fed at the breast, provides a unique and fundamental role in the development of a healthy and protective microbiome (Ames et al., 2023; Chong et al., 2022). Comparatively, pasteurized donor human milk is associated with a less protective microbiome than direct breastfeeding; however, it is better than commercial milk formula. It is not known to what extent milk sharing protects or disrupts the development of the infant’s microbiome and resulting immune system. Nevertheless, in the setting of natural disasters, milk sharing may become a more important and acceptable alternative to recommend.
Milk Expression
For parents and babies who cannot or choose not to directly breastfeed but want the benefits of human milk, milk expression is recommended. Milk expression is also necessary during disaster management to help increase supply for those who wish to re-lactate or induce lactation. Since electricity is often compromised during natural disasters, using electric breast pumps may not be an option. Either manual breast pumps or manual/hand expression can be taught to successfully maintain or increase supply. Proper technique is important to avoid nipple and breast trauma which may lead to abrasions and infection. Expressed milk must be properly stored to avoid contamination and permit maximum use of what has been expressed over time. Human milk may be used 4 hours after expression or 4 days after refrigeration. In disaster settings, refrigeration may be scarce and freezing milk even more difficult (Eglash et al., 2017).Extreme heat may affect the durability of human milk without refrigeration, and recommendations may need to be modified (Peters et al., 2016).
Education and Support for Mothers
Health care and emergency support providers can assist mothers who have weaned, or in some cases, mothers who have never breastfed, to re-lactate or induce lactation, although effectively trained workers and culturally congruent strategies are needed (Dall’Oglio et al., 2020; Breastfeeding following a Natural Disaster, n.d.).
Recognizing that the effects of climate change can cause or heighten anxiety, interventions to support the breastfeeding dyad should include education about unsettled infant behaviors, self-reported insufficient milk, and low breastfeeding self-efficacy (Pérez-Escamilla et al., 2023). While anticipatory education should be provided to all, it may be even more necessary to stress the benefits of breastfeeding to women in climate-vulnerable conditions to reinforce recognition of the nutritional security and lack of contamination inherent in breastfeeding. Counseling using a narrative approach to deliver information on maternal and infant health threats posed by climate change can be more effective than a didactic format (Adebayo et al., 2020). Information should be tailored to the population at risk. For example, at times of extreme heat, women should be educated about the importance of hydration, limiting caffeine, avoiding prolonged exercise, wearing loose clothing, limiting exposure to extreme heat, and appropriate actions to take during a heat advisory (Table 3).
Breastfeeding Dyad Solutions.
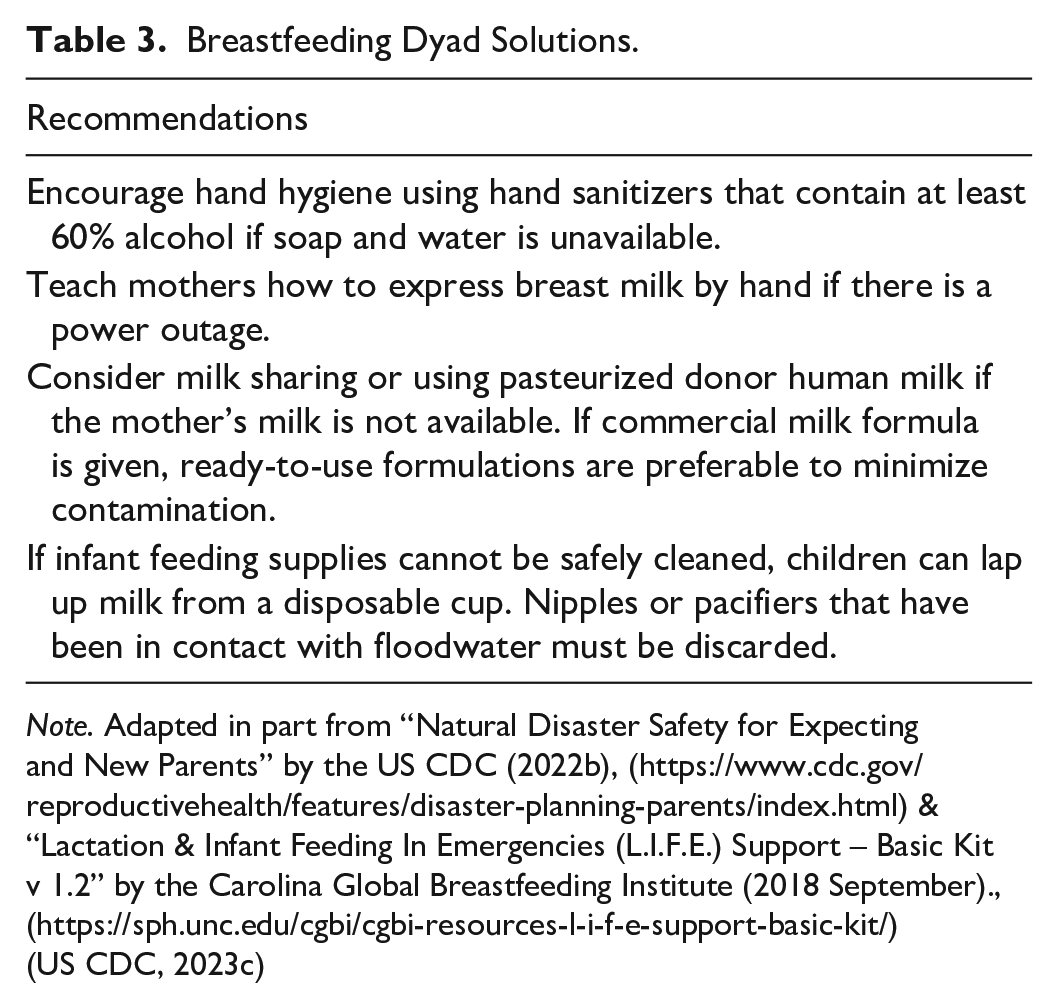
Note. Adapted in part from “Natural Disaster Safety for Expecting and New Parents” by the US CDC (2022b), (https://www.cdc.gov/reproductivehealth/features/disaster-planning-parents/index.html) & “Lactation & Infant Feeding In Emergencies (L.I.F.E.) Support – Basic Kit v 1.2” by the Carolina Global Breastfeeding Institute (2018 September)., (https://sph.unc.edu/cgbi/cgbi-resources-l-i-f-e-support-basic-kit/)
(US CDC, 2023c)
Co-Benefits of Breastfeeding
Placing an emphasis on health co-benefits of breastfeeding can facilitate the creation of regional climate action plans tailored to the needs of the community (de Nazelle, 2021; Ebi et al., 2021).
Facilitation of breastfeeding is independently a mitigation factor for climate change as part of sustainable food systems. Commercial milk formula production has a significant harmful environmental influence, with twice the carbon footprint and greenhouse gas emissions of breastfeeding. (Smith J.P., 2019) Some 13 L of ground water is needed to create one serving (about 240 ml or 8 oz) of commercial milk formula (Pope et al., 2021). In 2017, commercial milk formula products produced 4.2 million tons CO2 equivalents for China alone. Decreased dependence on formula would eliminate waste on many levels. Less water would be used as bottles would not have to be meticulously cleaned. Packaging for commercial milk formula and bottles would be eliminated. Fewer menstrual pads would be required for lactating parents, especially during the first 6 months postpartum, and breastfed children may produce less feces, saving on diapers (Myr, 2008).
Breastfeeding is part of a “triple duty action” to improve dietary quality, population health, and the sustainability of the global food system (Dadhich et al., 2021). A key benefit to breastfeeding that has been seen in multiple settings of natural disasters is the nutritional security it ensures in the short-term with supply chain disruptions. The WHO and the United States Breastfeeding Committee on Infant and Young Child Feeding in Emergency (IYCF-E) guidelines for breastfeeding during natural disasters note that even mothers under duress due to disasters and in conditions of malnutrition can make sufficient milk to nourish their children. (United States Breastfeeding Committee, 2023).
Conclusion
Optimizing breastfeeding practices protects the health of women and children who are already the most vulnerable in the climate crisis. As healthcare professionals, we are among the most trusted in the community to advise on public health policy, provide direct patient counseling, and promote, protect, and support breastfeeding to safeguard human and planetary health and minimize environmental harm. Clinician advocacy is needed at all levels of government and the private sector, as well as at our patients’ bedsides. Collaboration across specialty areas can inform adaptation, mitigation, and resiliency strategies that support breastfeeding couplets. As the climate crisis is upon us, we need to expand the evidence base and develop research questions with the aim of creating a set of guidelines to support breastfeeding practices into the future and to create structural and systems-level approaches to strengthening breastfeeding practices to ensure resilience in the face of global crises.
Supplemental Material
sj-docx-1-jhl-10.1177_08903344231216726 – Supplemental material for The Climate Crisis and Breastfeeding: Opportunities for Resilience
Supplemental material, sj-docx-1-jhl-10.1177_08903344231216726 for The Climate Crisis and Breastfeeding: Opportunities for Resilience by Elizabeth Cerceo, Karen Saxer, Lauren Grossman, Kathleen Shapley-Quinn and Lori Feldman-Winter in Journal of Human Lactation
Footnotes
Editor’s Note
Authors provide an extensive list of references to cover the breadth of this topic.
Author Contributions
Disclosures and Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary Material may be found in the “Supplemental material” tab in the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.