
Abstract
Introduction:
Non-puerperal adoptive lactation sometimes requires long preparation and substantial expense for pharmacological intervention to be successful, which are not feasible in refugee camps. Here we report two case studies of non-puerperal adoptive breastfeeding of two infants in the Rohingya Refugee Camp of Cox’s Bazar, Bangladesh.
Main Issue:
Two non-pregnant, non-breastfeeding caregivers with previous experience of breastfeeding brought two adopted infants—one a 12-day-old female with severe acute malnutrition, and the other a 2-day-old male with normal anthropometric measurements—to a nutritional stabilization center for feeding. After counseling, both families opted for adoptive lactation.
Management:
Both infants were treated with a modified Action Against Hunger protocol of in-patient management of severe acute malnutrition using the supplementary suckling technique, a procedure to feed the baby with supplementary feed. Diluted F100 was used as the supplementary feed; the energy and protein gained from it were just enough to maintain body physiology and were not responsible for any weight gain. When the infants gained weight, indicating that the caregivers were producing milk, we reduced the supplementary feed as per protocol guidelines. The caregivers were prescribed domperidone and counseled on their ability to breastfeed the infants. The cases required 35 days and 20 days, respectively, for the full establishment of breastfeeding.
Conclusion:
This is the first report of successful adoptive breastfeeding in a refugee camp. With proper counseling and motivation of the caregiver, induced lactation can be started without a preparatory period and with very low-cost intervention.
Introduction
Lack of exclusive breastfeeding and early weaning are two significant causes of undernutrition (Govender et al., 2021), and are widespread in the Rohingya refugee camp in Cox’s Bazar, Bangladesh (Action Against Hunger [ACF], 2018). This is particularly true for babies who are adopted after their biological mother’s death or who are abandoned for any reason. Non-puerperal adoptive breastfeeding can be lifesaving for these adopted infants (Pretorius et al., 2021).
Breastfeeding means a child has received human milk (either directly from the breast or expressed) (Labbok & Starling, 2012). Exclusive breastfeeding and relactation, where a biological mother resumes nursing after a pause, have been promoted to address malnutrition in refugee camps (ACF International, 2011). However, in refugee camps, there have been no documented instances of induced lactation for adoptive nursing in which a non-pregnant, non-breastfeeding caregiver nurses an infant due to the absence of the biological mother. Procedures for non-puerperal breastfeeding include non-pharmacological methods (e.g., breast pumping, nipple stimulation, letting the baby suckle the breast), use of local herbs or foods, pharmacological methods (e.g., use of hormone, metoclopramide, or domperidone) or a combination of these methods. Induced lactation and non-puerperal breastfeeding may require a long time for preparation, sometimes as long as 6 months, and substantial expense (Lawrence, 2021; Lopez-Bassols et al., 2021), none of which are likely to be available in emergency refugee contexts.
Here we report two successful cases of adoptive, non-puerperal breastfeeding in Rohingya Refugee Camp, using the supplementary suckling technique (SST). The adoptive mothers have given informed written consent for the publication of these case studies and have approved the case studies as submitted. We will refer to the adoptive mothers as the “caregivers” and the babies as the “infants” throughout the article.
History and Observational Assessment
Case 1
In December 2018, a 25-year-old female presented with a 12-day-old female (assigned sex) infant to a nutritional stabilization center (SC) in the Rohingya refugee camp of Cox’s Bazar, Bangladesh. Following the death of the biological mother, the infant was adopted by the caregiver and was initially fed rice water and powdered milk. On examination, the infant had all newborn reflexes present, no edema or wasting, 1.745 kg weight, 44.7 cm length, and < −3 SD weight-for-length Z score, indicating severe acute malnutrition (SAM). The caregiver weighed 73.3 kg and had no known diseases. The breast examination revealed no concerning findings. She had one 7-year-old boy and another 4-year-old girl. She breastfed both children for approximately 2 years following their births and had last nursed 2 years ago. During previous nursing periods, she had no breastfeeding issues, had not used a breast pump or any food/ herbal supplements, and had ceased to produce milk within several weeks of stopping breastfeeding. The entire family of the caregiver were refugees and lived in a makeshift camp.
Case 2
In February 2019, a 27-year-old female presented with a 2-day-old male (assigned sex) infant to the same SC, whom she had found abandoned 2 days previously in a graveyard. Her sister breastfed the infant for the next 2 days, but her husband objected due to social stigma. On examination, the infant had all newborn reflexes present, 3.190 kg weight, 50.5 cm length, and > −1 SD weight-for-length Z score. The caregiver had three female children of 12, 11, and 9 years. She breastfed all her children for approximately 2 years following their birth and had last nursed 7 years ago. The history of previous nursing periods and findings of breast examination were same as in Case 1. She weighed 57.2 kg and had no known disease. The entire family of the caregiver were refugees and lived in a makeshift camp.
In summary, two adopted infants were brought to the SC by non-breastfeeding caregivers who had previous experience of breastfeeding. One of the infants had SAM and the other had normal anthropometric measurements.
Management
Case 1
The timeline of the management is illustrated in Figure 1. A medical doctor counseled the caregiver’s family, including her partner and in-laws, on the possibility of formula feeding and adoptive breastfeeding, following which they decided to opt for adoptive breastfeeding.
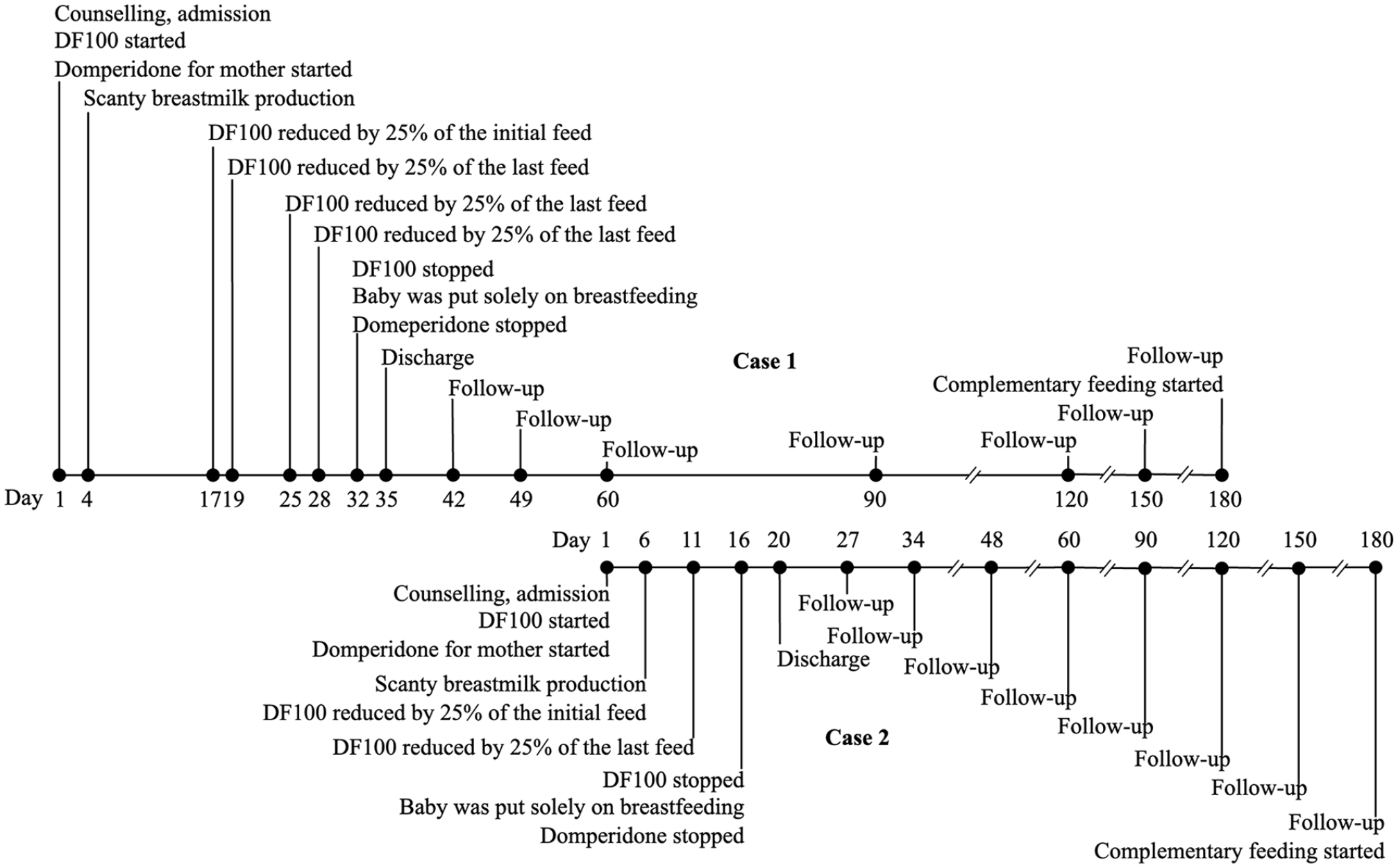
Timeline of the Case Studies.
We managed the infant and the caregiver dyad by a modified protocol for in-patient management of SAM for less than 6 months (Action Against Hunger International 2011). The infant was started on supplementary feeding of 130 ml/kg/day of diluted F100 (DF100) in eight divided doses per day. F100 is a feeding formula used to manage more than 6-month-old children with SAM, providing 100 kcal energy and 2.9 g protein per 100 ml. DF100 is a diluted form of F100 used to manage less than 6-month-old children with SAM, and it provides 77 kcal energy and 2.2 g protein per 100 ml. The energy produced by the amount of DF100 provided was only enough to maintain the body’s physiology but not for weight gain. We used SST to provide the DF100, wherein the feed was kept in a syringe below the nipple. One end of an eight-gauge nasogastric tube was attached to the tip of the syringe, and the other end was attached just above the nipple. Both the nipple and the tip of the tube were inserted into the infant’s mouth during breastfeeding such that when the infant sucked the nipple, DF100 came out of the tube (see Figure 2). The infant was breastfed every 3 hours for at least 20 min using this technique and directly breastfed if the infant wanted extra feeding. Trained nurses prepared DF100 before each feed and thoroughly cleaned all equipment before and after each feed following the United Nations Children’s Fund (UNICEF) guidelines (UNICEF Supply Toolbox, 2020).

Adoptive Mother Breastfeeding the Baby by Supplementary Suckling Technique.
The infant was weighed every morning and was found to be gaining weight, indicating that the infant was getting the caregiver’s milk as DF100 was insufficient for weight gain. When the infant gained ≥ 20 g/day weight for 2 consecutive days, we decreased the amount of DF100 by 25% of the initial feed. For example, if the initial feed was 35 ml/feed, it was reduced to 27 ml/feed after ≥ 20 g/day weight gain for 2 consecutive days. After that, the feed was decreased by 25% of the last feed after each successive maintenance weight gain (i.e., ≥ 10 g/day for 2 consecutive days). For example, if the last feed was 27 ml/feed, it was reduced to 21 ml/feed after ≥ 10 g/day weight gain for 2 consecutive days. This reduction of 25% after each successive maintenance weight gain was continued until all supplementary feeding was stopped.
The infant was also given cotrimoxazole (20 mg of sulfamethoxazole + 4 mg of trimethoprim per kg of body weight orally twice daily) for 7 days as a routine antibiotic for SAM. The caregiver was given a high-quality diet (2500 kcal/day), domperidone 10 mg 3 times daily until full breastfeeding was established, a single dose of vitamin A 200,000 IU, and treated for worm infestation with albendazole.
Case 2
The timeline of the management is illustrated in Figure 1. The infant and the caregiver were managed by the same modified protocol.
Outcomes
Case 1
The caregiver started to produce drops of milk from Day 4. On Day 32, all supplementary feeding was stopped, and the infant was kept solely on breastfeeding. Domperidone for the caregiver was also stopped; no side effect of domperidone was reported. They were discharged on Day 35 after the infant gained satisfactory weight (≥ 10 g/day) for 2 consecutive days only on breastfeeding (see Figure 3). The dyad was initially on weekly follow-ups until the infant reached 2 months, followed by monthly follow-ups until the infant reached 6 months. In every follow-up visit, a medical doctor and a nurse examined the dyad thoroughly, took the infant’s anthropometric measurements, and checked the attachment and positioning of the infant during breastfeeding. The infant was solely breastfeeding directly from the caregiver’s breast before starting complementary feeding at 6 months.
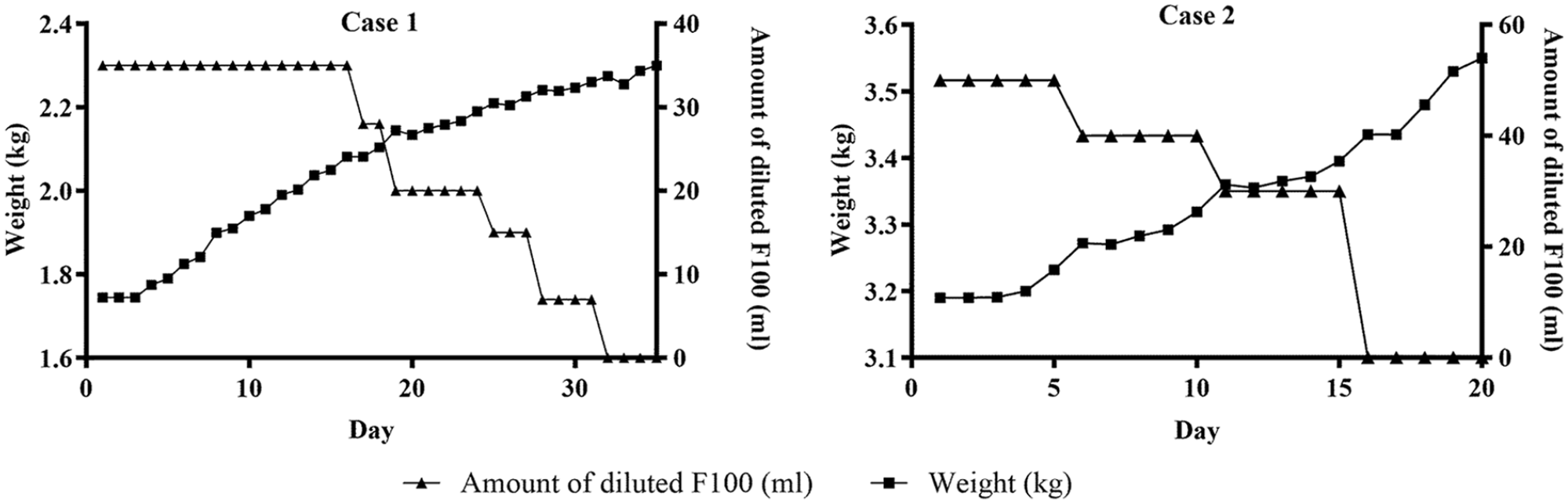
Trends of Weight Gain and Amount of Diluted F100 Given Over the Treatment Period.
Case 2
The caregiver started producing drops of breastmilk on Day 4. On Day 16, we stopped all supplementary feeding, and the infant was kept solely on breastfeeding. Domperidone for the caregiver was also stopped. They were discharged on Day 20 after satisfactory weight gain solely from breastfeeding (see Figure 3). The dyad was followed up as Case 1.
Discussion
Non-puerperal breastfeeding is an accepted and practiced method of breastfeeding in some cultures (Lawrence, 2021), and SST is used routinely to treat SAM patients, but the incorporation of non-puerperal breastfeeding using SST in refugee camps has not been reported in the literature.
The ACF International’s protocol for the management of SAM for less than 6 month old infants was modified on two issues. Originally, the protocol advised reducing DF100 to 50% after achieving an initial weight gain of 20 g/day for 2 consecutive days, and then discontinuing supplementary feeding entirely upon achieving maintenance weight gain (≥ 10 g/day for 2 consecutive days). However, in cases where maintenance weight gain was not achieved after decreasing DF100 to 50%, the supplementary feed should be increased to 75% for 2 days, and then lowered back to 50%. In the modified protocol, we reduced DF100 to 75% after an initial weight gain of 20 g/day for 2 days, as opposed to the recommended 50%. Furthermore, we reduced the supplementary feed by 25% of the last amount (instead of discontinuing it entirely) following each successive maintenance weight gain (≥ 10 g/day for 2 consecutive days).
The second modification involved opting for domperidone due to its availability, deviating from the recommended use of metoclopramide in the protocol. Domperidone and metoclopramide are dopamine antagonist galactagogues, which can increase the prolactin level and, therefore, can lead to an increase in the milk supply (Asztalos, 2018; Drugs and Lactation Database, 2021). Despite the United States Food and Drug Administration (FDA) cautioning against domperidone use (FDA, 2004) and the Academy of Breastfeeding Medicine advocating for cautious galactagogue use rather than outright recommendation (Brodribb & The Academy of Breastfeeding Medicine, 2018), domperidone is still employed to boost lactation due to its relatively low risk of side effects and good tolerability (Asztalos, 2018; Drugs and Lactation Database, 2021). Some experts also support domperidone’s use in healthy mothers to enhance milk production (Grzeskowiak et al., 2018, 2019).
It may seem striking that the Case 2 caregiver required approximately 3 weeks to start sufficient milk production, whereas Case 1 required 5 weeks, although the Case 2 caregiver last nursed 7 years previously and the Case 1 caregiver nursed only 2 years previously. Case 2 was admitted into the SC when Case 1 was already on follow-up. A session for the caregiver family of Case 2 with Case 1 was arranged on the 1st day, instilling confidence in the second caregiver. This change in mindset likely contributed to her early success, as breastfeeding essentially depends on the mother’s motivation and perception of her ability to breastfeed. Again, the strong support of the caregiver’s family and the staff of the SC might have played a crucial role on this occasion (Hassan et al., 2021).
Domperidone and nasogastric tubes comprised the primary expenses in the management of these cases. Bangladesh, a low-income country, benefits from affordable generic drug production. Domperidone, for example, costs approximately $3 for 100 tablets, is widely accessible, and is provided at no cost in government hospitals. In humanitarian settings like refugee camps, healthcare is universally provided for free both by governments and humanitarian agencies. The inaccessibility of domperidone and nasogastric tubes can, however, limit the applicability of the methods we used in other situations.
A skilled team of doctors and nurses oversaw both cases, carefully measuring and preparing the feed every 3 hours. Additionally, to address the families’ concerns for their other children, both families were permitted to remain in the SC throughout the treatment. However, offering these conditions may not be feasible in all refugee camps.
Most of the reported studies indicate that adoptive breastfeeding requires a preparation period. We found that if the caregiver is motivated enough, the process can be started immediately without any lag period, and full breastfeeding can be established within a month. In addition, SST can be a useful procedure for initiating breastfeeding and may be used in normal settings as well.
Footnotes
Acknowledgements
We thank Yonas Mesele, Tajkera Noor, Md. Zahid Hassan Zihad, and Dipankar Das of Action Against Hunger (ACF), Bangladesh Mission, for their guidance during the case management. We also thank Hannah Leah Elbo Morito and Tariq Agbabiaka of Hannover Medical School, Germany, for their assistance in writing the manuscript.
Author Contributions
Data Availability Statement
The dataset used and analyzed during the current study is available from the corresponding author of this article and Action Against Hunger (ACF), Bangladesh Mission. The dataset is available from the corresponding author on reasonable request, subject to the approval of ACF, Bangladesh Mission.
Disclosures and Conflicts of Interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The first two authors (HS and RK) were directly involved in case management as the lead physician and nurse, respectively. JM provided technical supervision during the case management.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors did not receive any specific funding for this study. The nutritional stabilization center in which the cases were managed was, however, funded by the United Nations Refugee Agency (UNHCR) under the project entitled “comprehensive nutrition and mental health project to address undernutrition and human sufferings among vulnerable populations living in camps and settlements in Ukhia and Teknaf, Cox’s Bazar” in 2018 and “multisector integrated interventions of nutrition, WaSH, and mental health activities” in 2019, and by Bureau of Population, Refugees, and Migration (BPRM) of U.S. Department of State under the project entitled “improving access to humanitarian services for Myanmar refugees and undocumented Myanmar nationals in Cox’s Bazar” in 2018–2019.