
Abstract
In 2015, Miriam Labbok, MD, MPH, entrusted Chele Marmet with the task of writing a chapter on the early history of the lactation consultant profession for the public health textbook she was preparing about lactation, saying, “I invited you to author it because you conceptualized and pioneered the profession, and there is nobody else I could ask who could do it justice,” (M. Labbok, personal communication, June 28, 2015). Chele Marmet envisioned the allied health field of lactation consulting, complete with international educational standards, professional organizations, and a scope of practice. She was an active contributing founder of the International Lactation Consultant Association, developed hundreds of test questions for the early International Board of Lactation Consultant Examiners (IBCLE), and co-founded the first academic (BA and MA) lactation education program, The Lactation Institute, to name only a few of her many innovations and contributions to the field of lactation we know today—a field that has grown exponentially globally since those early days in the 1970s when Chele began creating our profession. Her academic background in speech and hearing gave her the orientation to delve into infants’ oral-motor function. Additional education and experience followed as her passion for helping breastfeeding families grew. This is the first part of her interview; the second part will follow in the next JHL issue. Fortunately, Chele is working on her memoir, which will detail topics we could only briefly discuss in this interview. It was my honor to interview Chele Marmet.
Joan E. Dodgson
Keywords
(This interview has been transcribed with minor editing for ease of reading. CM = Chele Marmet, JD = Joan Dodgson).
Interview
Chele, how did you first become interested in breastfeeding?
When I was 9, my mother “banished” her visiting friend to my bedroom to feed her 2-month-old baby. I had no idea why anyone had to leave the camaraderie around the kitchen table to feed a baby in a bedroom. Until that time, I had only observed babies being bottle-fed. After I showed her how to get to my room, she invited me to stay and keep her company. Although we talked the whole time she breastfed, I watched their continuous silent communication—through their eyes and body language. It was gorgeous! I immediately knew babies were meant to be breastfed and that I would breastfeed my babies.
My next exposure to breastfeeding didn’t occur until I was 22. I had just returned to Saint Louis from 2 years of living in Tokyo, Japan, when my cousin, Francine, invited me to accompany her to a La Leche League (LLL) meeting in August of 1966. After that meeting, I had no further exposure to breastfeeding until I put my first baby to my breast in August of 1968. I experienced the usual problems common to that “era”—separation from my baby after birth, which led to engorgement. My baby requested frequent feedings, which my mother and grandmother insisted meant I must not have enough milk. Thankfully, my breastfeeding-experienced cousin’s advice, “Just keep breastfeeding,” got me through all those early problems. After that, my baby breastfed well until she self-weaned at 9.5 months.
My second baby, born 17 months later (February 1970), and my third (June 1973), were a huge breastfeeding challenge because of an anatomical nipple anomaly (that I later labeled a dimpled nipple—not inverted), which caused pain and bleeding. To this day, I’m not sure why the dimpled nipple did not cause pain with my first, though she did spit up blood one time, so I clearly had the problem with her, too.
Chele Marmet BS, MA, IBCLC (Retired), FILCA

Breastfeeding women turned to you for help; how did they find you?
Joan E. Dodgson, PhD, MPH, FAAN

It is hard today to imagine the late 1960s and early 1970s breastfeeding desert (U.S. Department of Health, Education, and Welfare, 1979; U.S. Office of the Surgeon General et al., 2011). In 1968, I did not know even one other person currently breastfeeding in St. Louis, Missouri (the large, Midwestern U.S. city where I was born, raised, and lived). Consequently, it was unsurprising that at 3 months postpartum, when I was breastfeeding my first child, word had spread that I was “a very experienced breastfeeder.” From then on, I got calls for help from all over the country. They found me by word of mouth. I never sought it out, advertised, or charged money for my time. I willingly shared the knowledge, albeit very limited, from my babies’ tutelage, my formal education, and previous experiences from all the dyads with whom I had worked. When I did not know how to help mothers over the phone, I invited those who lived within driving range of my home for an in-person visit with their baby, in the hope that I could provide better help.
In what ways did your undergraduate degree from Washington University’s (St. Louis) Central Institute for the Deaf (CID), in speech and hearing, contribute to your success during these early days working with breastfeeding mothers?
My education at CID greatly enhanced my ability to help breastfeeding dyads clinically. I had had 5 half-days a week during my junior year of upper-division anatomy and physiology. We had to learn how to teach a profoundly deaf child to lip read and then position their oral anatomy to produce intelligible sounds so they could “listen, talk, read, and succeed” (CID, 2023). I learned to focus on anatomy, the correct and incorrect functions. This applied to figuring out how to fit a mother’s breast and a baby’s mouth together to function properly for breastfeeding. I was able to approach helping dyads at these sessions in a clinical (hands-on) fashion. I learned so much from helping those mothers and babies. I could not always solve their problems, but I was sadly aware that there was no one more knowledgeable that could help them.
Most of our friends and my parents’ friends were physicians. My husband was an Obstetrics and Gyneacology (OB/GYN) resident when our first was born, and in practice when our second was born. I knew that not one of them had any knowledge, education, or experience with breastfeeding. Because of contact with local LLL Leaders, I knew their role was to provide basic breastfeeding education and mother-to-mother support. They were not trained or expected to function clinically. Personally, when local LLL Leaders had no idea how to solve my bleeding nipple problems, I was referred to a LLL Founder, who dealt with the medically related problems. The Founder suggested I walk around the block daily during our first phone conversation and during the second call that I wean my second baby from the problem breast/nipple, which sadly I did. I continued breastfeeding him on one breast until he self-weaned 2 years later. The Founder never mentioned that I could relactate. I suspect that in 1970, she didn’t know that was possible. I knew of no one to whom I could refer the breastfeeding problems I encountered.
Can you give us an example of how your personal experiences with breastfeeding improved your skill in helping others?
When my first baby was about 5 and a half months old, I returned to half-day teaching at CID. I tried many times to hand express my milk, on my own and from written descriptions of the skill available at that time, to leave milk for my baby during work hours. I only managed to cause skin burns, bruising, and pain. With my second and third baby, I knew skill with hand expression would allow me to rest my sore, bleeding nipple.
Shortly after child three was born in 1973, I “finally” figured out a pain-free, effective manual expression technique and how to cup-feed the expressed milk to him. I was unwilling to waste that precious milk I had expressed or resort to bottle feeding, which I strongly suspected would cause issues. I used a flexible soup bowl to catch my milk and cup-feed it back to him. Because he didn’t always need milk from both breasts, I eventually had over 100 8 oz. baby bottles full of milk in my freezer. About 2 years after he weaned (at 3 years and 4 months), the administrative head of LLL of Southern California (CA) phoned to ask me if the University of California, Los Angeles (UCLA) Hospital could have a few bottles of my milk. They had a 4-month-old baby who was dying—unable to digest every available formula. Someone finally suggested they try breastmilk. That baby kept my milk down without a problem. I donated all of the rest of my 2 to 5-year-old milk to keep that baby alive while they searched for more donor milk.
Soon after that, I started teaching hand expression to others—both at LLL meetings and to professionals a couple of years later, when invited to lecture. As this technique became more widely used, it became known as the “Marmet Technique.” When people requested the technique in writing, I struggled to “translate” a manual skill into written words, but when I finally accomplished this, others could easily read and convert it into an effective and safe manual skill (Marmet, 1978, reprinted often and in major textbooks); subsequently, it was included in many books and translated into many languages. Eventually, through a combination of my personal experiences, both working while breastfeeding and my painful bleeding nipple battles, many benefitted.
JD: How did your move to Los Angeles (LA), CA, influence your breastfeeding work?
In 1970, the move to LA gave me a much larger population base and a city with great creative energy. Mothers with breastfeeding concerns continued to find me. I provided frequent phone help and saw dyads with complex breastfeeding problems, including prematurity, relactation, induced lactation, and newborn deaths. Many of these complex situations required using equipment then available, for example, feeding tube devices and electric breast pumps (Marmet & Shell, 1988a).
My clinical breastfeeding workload, which started in late 1968 when my first was 3 months old, continued to grow exponentially after I became a LLL Leader in March 1975. Mothers needing breastfeeding help found me through referrals from physicians, hospital personnel, LLL Leaders and mothers’ word of mouth. I was inundated. In addition, I received many invitations to lecture in hospitals to nurses and physicians throughout Southern CA. I also lectured to many other groups, for example, LLL Leaders all over Southern CA, midwives, other health professionals and, annually, Dr. Derrick Jelliffe’s UCLA School of Public Health masters and doctoral students (1975–1992).
In what other ways did your practice expand?
In late 1975, under the La Leche League International (LLLI) banner, I opened a breast pump depot for the first quality electric breast pump company in the United States. I had four pumps for greater LA. When I rented a breast pump to a mother, each personal pump kit had written instructions, in seven languages, about how to attach all the pieces and plug the pump in, but zero instructions about how to best use the pump physiologically. The second mother who rented a pump from me, phoned a week later, and said, “This pump you rented me is making my preemie sick.” One of the NICU nurses had told her the pump was why her baby was sick. The mother then said, “I could sue you; I could sue LLL of Southern CA, and I could sue LLLI—and I just might.” I did my best to calm her and said I would get back to her as soon as possible. Then I phoned the U.S. head of the breast pump company and asked him to overnight a brand new, untouched-by-human-hands pump to me, which he did. I then spoke to Edwina Froechlich, one of LLLI’s seven Founding Mothers. I asked her if LLLI had insurance for its Leaders, and she said she would check into it. LLLI, of course, had no insurance for Leaders. I arranged for a local pathologist to examine the problematic pump, which I had exchanged for the brand-new electric breast pump. Though he found some milk backed up into tubing inside the pump (the result of incorrect usage), the tests he ran on the pump (inside and out) were negative for contamination concerns. There was clearly no cause for the concerns raised about the pump. The reactions were because it was a new piece of equipment, and the baby was not thriving. I also arranged for a local pediatrician, who had privileges at the hospital the baby was in, to check the baby’s records to determine if the breast pump could have caused a problem with the baby’s health. He confirmed there was nothing. The baby improved on his own, and the threatened lawsuit blew over; however, what came from this early incident was that I suggested the following to Edwina. If LLL Leaders were going to work with sick/hospitalized babies and/or mothers and equipment, LLLI needed insurance to protect Leaders from lawsuits, and needed to create a training program for Leaders so they were prepared to provide educated, special circumstance care.
Edwina said to me in response, “I’ll work on the insurance. You write the training program.” That was one of the defining moments for me on the path to creating the lactation consultant profession. From then on, I started keeping detailed records of every phone call and consultation and began researching how and when each specific piece of equipment (e.g., pumps, feeding tube devices) was needed and best used. For example, [regarding] pump usage, I started by suggesting each mother try two methods, which I determined and then explained, and get back to me about which worked better to physiologically establish/increase/decrease/maintain her milk supply, depending on that mother’s needs. I also did this research and record keeping with positional variations and sucking issues (Marmet & Shell, 1984, 1990a).
Another development that stemmed from this whole incident was that I suggested to the U.S. head of the breast pump company that they might consider including instructions in each personal pump kit explaining how the pump should be used physiologically. After I verbally shared some of my research findings with him, I was invited to write those instructions, which I did. My instruction about the physiologic use of breast pumps was included in every personal pump kit sold by several major breast pump companies in multiple languages (e.g., English, German, and Spanish) for over 20 years (starting in 1978). These instructions also were included in books and pamphlets, which hospitals copied (mostly without permission) until they became ubiquitous.
Initially, you tried to work through LLLI to professionalize lactation care. What happened?
In July of 1977, after 1.5 years of clinical research and data collection, the summation of my records of all the breastfeeding dyads I had worked with was hand-delivered to Edwina Froehlich at LLLI. The cover letter suggested that LLLI create a Lactation Consultant department and provide formal education to interested, experienced LLL Leaders to train them to work with what I then called special circumstance breastfeeding. I waited anxiously to hear back from LLLI but received no response. Over the next few months, I realized what I had proposed was beyond the scope of LLLI’s mission: To provide mother-to-mother support and basic breastfeeding information.
I was now in the unique position of having developed a new body of knowledge gained from my 9 years of experience working through problems with special circumstance breastfeeding dyads and formal clinical research (Marmet & Shell, 1988a). Each month, I grew increasingly overwhelmed with far more than full-time work, all pro bono. I could not care for all the mothers who needed breastfeeding help beyond what LLL Leaders were trained or expected to provide. Also, I realized that by functioning alone, I was scratching the surface of all I wanted to learn to enable me to provide better help to breastfeeding dyads. For this growth to occur, I needed peers.
During the early fall of 1977, like the previous year, I spent a 12-hour day at Cedars Sinai Medical Center, a large LA teaching hospital. I provided in-services for all nurses and most physicians, who worked in maternity services and NICU [neonatal intensive care unit], introducing them to basic clinical breastfeeding skills (Figure 1). Although, in both years, my lectures at Cedars were highly praised and evaluated, I observed that no change had been affected by receiving the previous year’s in-service. I felt exceedingly frustrated since I realized that my second “annual” in-service at this hospital was unlikely to produce better results. That night, as I walked to my car, I had my “lightbulb moment.” I knew, with absolute certainty, that we needed a new professional, the Lactation Consultant, who would be thoroughly trained, preferably with a university master’s degree in lactation consulting. It needed to be a technique-oriented, education-oriented, allied health profession. I knew that to effect change, hospital staff must learn to trust and appreciate this new allied medical professional. I knew they would also be hired to work in clinics, research, and private practice and would be needed worldwide.
Now the giant question was, how does one go from an epiphany to creating a living, breathing, new allied health field? Later that evening, I said to my husband, “I’m going to create a new profession, lactation consulting.” His now infamous response was, “Who would pay for breastfeeding care?” To Ellen Shell, my co-LLL Leader (since April 1975), I said, “I have a brilliant idea, and you have to do it with me!” She says, “Little did I realize that it was going to take the rest of my life.”
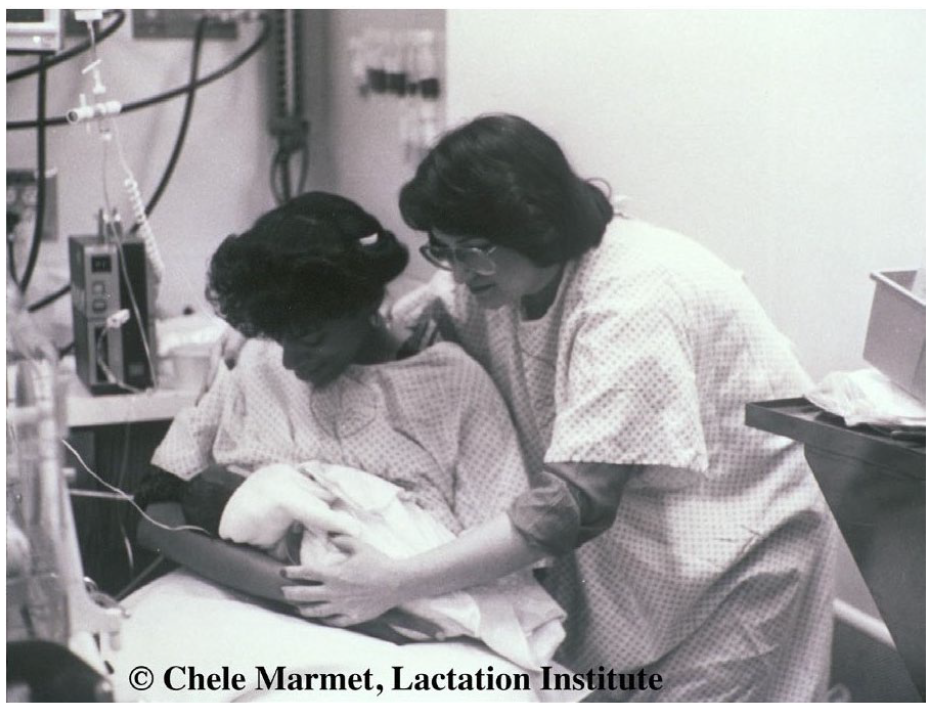
Chele Marmet, Teaching a Mom and Infant Their First Latch-On in the NICU (October 1977).
This was an enormous undertaking. What steps did you take first and why?
Ellen and I put our heads together for the next 2 years. We both agreed that to operate a graduate-level educational program, we each had to have a graduate degree. Our first thought was to earn degrees in registered nursing, which we were more than willing to do. We researched every nursing school program within driving distance of our homes. We learned, among other things, that while some educational requirements of these programs aligned, a large percentage diverged from what I knew by experience we needed to learn. It was only then that we investigated other fields of study.
We realized that the closest related professions to the one I envisioned were speech and language pathology, occupational therapy, and physical therapy (in that order). Other medical and allied medical professions (e.g., nursing and dietetics), along with many other degreed professions (e.g., public health, normal and abnormal child development, psychology, anatomy and physiology, pathology, toxicology, and education), also had aspects of what the LC would need to know (Marmet & Shell, 1988b). Mother-to-mother support counseling also provided a vital body of knowledge. Therefore, the educational program we planned to develop had to encompass aspects of all of these, as well as the art and science of breastfeeding, counseling breastfeeding dyads, and more (Marmet & Shell, 1988a).
For the previous 4 years, I had presented lectures to Dr. Derrick Jelliffe’s graduate classes in the School of Public Health at UCLA. Dr. Jelliffe worked closely with the World Health Organization (WHO) and was widely recognized as one of the world’s foremost experts in infant nutrition. He was also head of the Maternal/Child Division of Public Health at UCLA. He had created lactation support programs worldwide, detailed in his seminal book, Human Milk in the Modern World (Jelliffe & Jelliffe 1978). His work has influenced generations of breastfeeding advocates and program planners. Ellen and I hoped he would be an ally and guide us.
In the summer of 1978, we scheduled a meeting with Dr. Jelliffe, for which we created a one-page outline of the profession I was envisioning, and detailed why and what was needed. It was brief but thorough. Ellen and I shared it with Dr. Jelliffe and asked about being admitted to his Master of Public Health program at UCLA. His response, in his very proper English accent, was, “You must do this. There is nothing like this, and the world needs it. You must do this now! You are welcome in my MPH program now or any time in the future, but you must start the LC profession now!” When Dr. Jelliffe mentioned that his MPH program was only full-time, I said, “I can’t do that with a husband, three young kids, plus other current commitments.” He replied, “You definitely need a master’s degree to do what you have proposed, but it doesn’t matter what you get your master’s degree in, or where, as long as it is from a fully accredited institution. You must, however, start this profession now. Then, figure out how to get your master’s. The world needs lactation consultants now.” His enthusiasm inspired us to move forward with as much speed as our family responsibilities allowed.
Please talk us through the process you followed, step-by-step.
After our meeting with Dr. Jelliffe, the ideas Ellen and I had coalesced into our first task, the formation of a nonprofit, educational, allied health organization to serve as the role model for this new profession. Then, we tackled two significant projects. First, we needed to incorporate it as a nonprofit organization. We spoke to attorneys, seeking help with this endeavor, but could not afford their services. We asked them about the possibility of us writing our incorporation paperwork. Every attorney we spoke to said it could not be done. So, we bought a book on incorporating and proved them wrong.
We had three specific goals, which were delineated in our articles of incorporation:
To train LCs at a master’s degree level and, as soon as possible, affiliate with an accredited university so that we could offer a degree educational program.
To work clinically with breastfeeding dyads, especially those experiencing unusual problems.
To do clinical research and publicly share results.
This is how we defined the parameters of the LC professional in our incorporation papers: A lactation consultant (LC) is a professional breastfeeding expert qualified to provide education and consultation in all aspects of routine and special circumstance breastfeeding. An LC is trained to act independently to develop a treatment plan for each breastfeeding situation. A team approach between the physician and the LC provides optimum care, recognizing that the breastfeeding dyad must remain under the medical care of the attending physician(s). Employment options for lactation consultants include working in a physician’s office, breastfeeding clinic, private practice, public health agency, or hospital. (Marmet & Shell, 1979, p. 4)
Next, we had to select a name for our budding organization. After much thought, we chose a name that defined what we intended to become: The Lactation Institute and Breastfeeding Clinic (LI). To some, it seemed grandiose to think of this idea we were developing as an institute, but we knew that we needed to provide the model for this new profession.
Ellen flew to Sacramento (CA’s state capital) and told the officials about all the sick babies we would help. They stamped all the necessary documents that same day for our nonprofit incorporation in CA. Our formal paperwork from CA arrived soon after, followed by the federal documents several months later. (The U.S. incorporation paperwork was automatic based on our CA status.)
The second project was even more challenging—getting insurance for our non-existent profession. We must have talked to a thousand agents and insurance company officials to find one that would provide coverage to meet our specific needs. Ellen and I knew it would cost a small fortune and decided to share this financial commitment personally. We also knew the policy would take several months to be written and finalized, but we could not start without it. During this year (1978–1979) of foundational preparation, because I had so many requests for breastfeeding consults, I also trained Ellen to function clinically so that, when we opened our doors, she could provide breastfeeding consults.
At the July 1979 LLLI International Conference, I had a private meeting with Edwina Froehlich to inform her of our plans to initiate a new allied health professional to work clinically with breastfeeding dyads: The LC. We discussed all the preparatory work Ellen and I had been doing for the last 2 years. She gave me LLLI’s blessing. I kept LLLI well informed about our progress, including how we were training LCs and functioning clinically.
In preparation for opening our doors, we had to set service fees. After much thought, we decided that setting our fees at the same rate as a speech pathologist or an occupational therapist would be too high for our profession’s initiation. Instead, we set our fees in the mid-range of what a variety of private lessons cost hourly, for example, tennis, piano, or math tutoring. We charged a flat fee for the 2-hour initial consultation, and follow-up appointments were scheduled for 1 hour at 60% of the initial fee.
By October of 1979, we finally had insurance coverage in writing, in addition to our incorporation papers, and so we officially opened the LI doors, using rooms in our homes. My first task was hiring an answering service and teaching them how to answer the phone. Then, I spoke to all the physicians, healthcare professionals, hospital personnel, and LLL Leaders who had been referring mothers to me about opening the LI. Though we had no facility, no staff (other than Ellen and me), no library, and no financial backing (except from our husbands), I shared my vision with them of what we were in the process of creating (a new allied health profession: Lactation consulting). I also informed them that services would now have fees for the first time.
We contacted the answering service several times a day to check for messages. After 3 months, they laughed at us each time we checked in because we did not get a single referral, despite my having seen breastfeeding dyads all day, 6 to 7 days a week, for the past few years. The moment I told those who referred moms that I was going to charge for the same services that had been pro bono, they stopped referring. Instead of worrying, I used that time to map out the specifics of our educational program. I created our first formal clinical charting forms, the academic subjects we needed to cover with future students, syllabi, and reference materials, and even prepared some lectures and assignments. After 3 months, the LI phone started ringing again when people realized that breastfeeding dyads needed our services—although we were now charging.
How did your planning process evolve?
Our strategizing during the planning phase was so thorough that we never had to vary the basics of the way we operated. In making decisions, we always asked ourselves what was best for babies and mothers rather than what was good for us, the LI, or even the LC profession. We asked ourselves this question as we developed ideas for how to grow the profession, and every time a new issue arose. In retrospect, I think this was one of the most critical determinants of our success.
When did you start accepting students?
We started with one student in the early fall of 1979 who had been waiting in the wings. I had previously worked clinically with her so that after two unsuccessful breastfeeding attempts, she could fully breastfeed her third baby despite his being premature, very sick, and in the NICU for 3 months. When I shared my vision and plans with her, she was excited to be the LI’s first student. We did not have a formal training program during those first 3 months. However, I educated her, as I had Ellen, one-on-one, during that time, and she continued with us for several years, as a student and eventually as clinical faculty, until her family moved to the East Coast and then back to Europe several years later. She has been credited with taking the profession to Europe.
The LI gained four more students in the first week of January 1980. All were degreed LLL Leaders, two of which were in microbiology. Two of these first five students were born and educated in Europe. Several months later, two more students, both nurses, joined us (Figure 2). After that, our students came from a wide variety of educational backgrounds. Though most were nurses or registered dieticians, backgrounds always varied (from engineering to ancient history). Our early students came from all over Southern CA and a few moved to LA from the Western United States to study with us.

The First Lactation Institute Faculty, Staff and Student Celebration (December 1981).
Please explain how your educational program continued to develop.
In January 1980, we started our formal educational program, which required one full didactic day a week for 12 months. Classes were held at Ellen’s house because it was the most centrally located for our students. The clinical education requirements included observing, sharing, and doing consults solo. This education took longer than the year’s didactic work because, to function safely, each student had to have gained sufficient supervised LC expertise with a wide variety of specified problems (Marmet & Shell, 1988b, 1990b). This included common and uncommon problems, which meant waiting for those with specific problems to schedule consults. Initially, we scheduled consults in both of our homes, depending on the location easiest for the breastfeeding dyad, and then notified all our students. Those who could come did. Then, we started scheduling most consults at Ellen’s house. First, we used one bedroom daily for consults. Over the next few months, we grew and required all of Ellen’s house 5 days a week. By the Summer of 1982, her husband said he wanted his house back; we temporarily rented a small house while we searched for office space with a landlord willing to build it to our specifications.
We continued to didactically educate our students 1 day a week until mid 1983. We always left time each didactic day to cover anything that had come up during the week’s clinical experiences. In addition to being in charge of all educational administrative responsibilities, I was also doing the lion’s share of the research and lectures. However, even when I presented material, we all learned together in those first few years. When appropriate, I assigned teaching topics to students who had the most experience. For example, one student had a degree in microbiology, so she researched and presented hormones of pregnancy and lactation. Select medical consulting board members also presented topics, for example, Dr. Jelliffe spent a half day lecturing on public health, annually. Over the course of 4 weeks, we covered each topic until it was done, which sometimes took a day and sometimes 4 days. As topics came up in discussion that piqued our interest, we added new subjects to our list of what we wanted to study and learn. It was a fluid, living curriculum in those first couple of years. Also, 3 days a week, I functioned in numerous faculty capacities in our Breastfeeding Clinic, which was already known as a referral center for high-risk-for-breastfeeding-failure problems. Ellen was in charge of operational administration and covered administrative issues with staff and students. We both worked 7 days a week around our families’ needs.
When our students’ didactic and clinical requirements had been met, samples of their charting skills were submitted and reviewed, and clinical skill levels were observed and evaluated for their ability to function solo; then, their academic and clinical records were presented to our certification board. According to our bylaws, the certification board was comprised of two physicians (one OB-GYN, one pediatrician), one Registered Nurse, Ellen, and me. Four of the five had to sign off on each student. This certification board was designed as a stopgap to ensure high-quality academic knowledge and clinical skills until formal degree programs and state or national certification boards were in place to certify candidates. Starting in September 1983, the program required two full didactic days a week plus clinical.
The Lactation Institute logo is very compelling. How was it created?
Ellen wanted our logo to be a tree like the one in a framed picture she loved (and still has). I wanted our logo to depict breast anatomy. So, we took Ellen’s picture and my anatomical idea to LLL Leader and artist Rosie Weisel, and she went to work. I visited Rosie’s home multiple times during the next couple of months. After each of Rosie’s renditions, I would take it home and work on and modify her drawing. Then I’d take it back to Rosie, and she would create the next version, each time polishing my drawings and making my suggestions part of an artistic rendition. We wanted an artistically depicted image that would stand the test of time incorporating accurate anatomy and Ellen’s tree. Rosie wanted to please us and create a professional-looking logo (Figure 3). Many years later, after Peter Hartmann, PhD, and his team published their ultrasound research on breast anatomy (Ramsay et al., 2005) I met some of them at a conference. They shared that our logo was the only anatomically correct depiction of the breast they had seen in cross-section drawings. Our logo has stood the test of time!
Lactation Institute Brochure (May 1983–May 1984).
When did you and Ellen pursue your graduate degrees?
Shortly after the LI was operational, Ellen and I returned to fulfilling our goal of attaining our master’s degrees. After researching many master’s degree programs, we decided to apply. We were accepted at Pacific Oaks College (PO) in Pasadena, CA, which was available as a part-time program. They offered a degree in human development with two specializations: College teaching and educational administration. We felt a double major would benefit the work we were doing. We added a third specialization after starting our studies: Infant and toddler development. All three programs of study were perfect for our educational and practical needs. This decision was fortuitous because key PO faculty members got to know us and, in a few short years, welcomed establishing bachelor’s and master’s degree programs (in human development with a specialization in lactation consulting) in conjunction with the LI. Starting March 1985, our academic partnership operated and granted degrees for over 22 years. This affiliation proved a tremendous help in spreading and developing the professionalization of lactation consultancy.
You and Ellen accomplished so much in a relatively short time. When did you realize that this work was being appreciated nationally?
In January of 1980, we realized that word had spread nationally when Jan Riordan, a nurse and LLL Leader from Kansas, traveled to Los Angeles to visit the LI. She was gathering material for her first book, A Practical Guide to Breastfeeding (Riordan, 1983), aimed at teaching nurses about breastfeeding. Her research included personal visits with the tiny handful of MDs, RNs, and researchers working in some way professionally with breastfeeding. However, we were the only ones officially functioning as LCs. Among the many issues we discussed was how we each had dreamed of a professional association because contact between people functioning professionally is so important. We decided to put our lists together of all those already, or interested in, functioning professionally in lactation care or research. At Jan’s insistence, since the LI was already computerized, Ellen and I wrote a letter to everyone on the combined list (about 35–40 people) to see if there was any interest in starting a professional lactation association. We received a very minimal response; I realized the timing was too early. However, having a professional association remained one of my goals. So, I continued adding to this list every time the LI was contacted by someone interested in the LI educational program or was functioning professionally in lactation. This file was later used as the core of the first mailing list for creating a professional association for LCs (later named the International Lactation Consultants Association; ILCA). Jan shared details she had learned about the LI and LC profession with LLLI and many others she interviewed for her book. As she traveled, our work and my vision spread. Jan’s book contained the first nationally published information about the LI and the LC profession.
Chele, thank you. We have covered a lot of the early years of your work. This seems like a good place to stop the first part of our interview. The second part will continue chronologically with your journey, as the LC profession begins to take shape internationally. It will be published in the next issue of JHL.
Supplemental Material
sj-docx-1-jhl-10.1177_08903344231213655 – Supplemental material for The Conception and Birth of the Lactation Consultant Profession (1977–1983): An Interview With Chele Marmet (Part I)
Supplemental material, sj-docx-1-jhl-10.1177_08903344231213655 for The Conception and Birth of the Lactation Consultant Profession (1977–1983): An Interview With Chele Marmet (Part I) by Chele Marmet and Joan E. Dodgson in Journal of Human Lactation
Footnotes
Acknowledgements
Chele Marmet thanks Ellen Shell, MA, for the years of friendship, subject matter expertise, and collaboration in so many aspects of our profession’s evolution. The authors thank Lora Cash, BA, for her invaluable contributions to preparing this manuscript, and Leon Gross, PhD, for reviewing and editing an early draft.
Author Contributions
Disclosures and Conflicts of Interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Joan E. Dodgson was the JHL Editor in Chief when this article was solicited. Authors have no conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary Material may be found in the “Supplemental material” tab in the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.