
Abstract
Late preterm infants have lower breastfeeding rates than term infants, yet few published interventions or guidelines exist to guide hospitals in managing them in the non-intensive nursery setting. Here we describe the development and implementation of an interdisciplinary, hospital-based, breastfeeding support program among late preterm infants not requiring intensive care. The Early Bloomer Program includes an order set applied at birth, immediate lactation consultation, availability of donor milk, parent education on late preterm infants, hand expression teaching and kit including spoon and video link, and daily interdisciplinary team huddles. The program was developed with staff input using Diffusion of Innovation Theory, and implemented first among early adopters before expanding to all postpartum nurses. Nursing staff received education on late preterm infant physiology and feeding, and trainings on the Early Bloomers program through various learning modalities during the year leading up to implementation. To further understand the strengths and weakness of the program, we surveyed nurses (n = 43). Nurses reported that they were more attentive to the needs of late preterm infants, more confident in their care, and more aware of possible complications and feeding needs. Areas noted in need of improvement included lack of overnight lactation consults and little involvement of labor and delivery staff in the program. The Early Bloomers program increased confidence in care and was well received by nurses. Well-designed clinical studies are needed to identify effective breastfeeding support practices for late preterm infants.
Key Messages
Late preterm birth (34–36 weeks gestation) is rising in the United States, particularly among racial/ethnic minoritized groups.
Late preterm infants have lower rates of receipt of human milk compared to term infants.
We describe the design and implementation of a nurse-driven intervention to support human milk feeding among late preterm infants at a safety-net hospital.
Background
In the United States, the rate of late preterm birth (34.0–36.6 weeks gestation) increased from 2015 to 2018, driven predominantly by an increase in late preterm births among non-Hispanic Black and Hispanic populations (Stewart & Barfield, 2019). Breastfeeding is strongly recommended in all preterm infants to promote improved outcomes (World Health Organization, 2022). However, any and exclusive breastfeeding is lower among late preterm infants (LPI) compared to infants born at term (≥ 37 weeks gestation). Breastfeeding rates are even lower among non-Hispanic Black LPI populations, among whom only 66% initiate breastfeeding, compared with 79% non-Hispanic white LPI populations (Chiang et al., 2019). This disparity highlights the urgency of identifying practices to support breastfeeding in this vulnerable population experiencing late preterm births.
Etiologies of lower breastfeeding rates among LPI are multifactorial. They include neurodevelopmental prematurity (e.g., hypotonicity, easy fatigue, disordered wake-sleep cycles) which inhibits organized and effective feeding, and medical problems associated with late preterm birth (e.g., respiratory distress, hyperbilirubinemia, hypothermia, hypoglycemia) which often lead to reduced opportunities for direct breastfeeding and/or separation during the early postpartum period (Meier et al., 2013; Stewart & Barfield, 2019). Despite this medical and developmental vulnerability, many LPIs are cared for in non-intensive, postpartum care settings without the higher staffing ratios, specialized nursing care, and feeding protocols of neonatal intensive care units (Boyle et al., 2015; Ishiguro et al., 2009). Additionally, the extent of lactation support policies tailored to the needs of LPI in non-intensive settings are not known.
Late preterm infants have been called “the great pretenders” as they appear similar to term infants in non-intensive newborn care, yet the risk for complications is higher and they may require additional care and surveillance, particularly around feeding (Boyle et al., 2015; Stewart & Barfield, 2019). Nursing guidelines exist to manage overall care of LPI (e.g., delayed bath, frequent vital sign measurements, feeding schedules; Baker, 2015). They have been implemented in a limited number of non-intensive care settings (Busch et al., 2021; Lober et al., 2021). Published clinical lactation guidelines for LPIs are based primarily on expert opinion or evidence from term infants (Boies & Vaucher, 2016; Cartwright et al., 2017). It is plausible that greater support would increase breastfeeding rates among LPIs. In a large national sample of LPIs in the United States, increasing the number of breastfeeding support practices was associated with higher odds of breastfeeding (Goyal et al., 2014). A recent systematic review also identified higher rates of LPI breastfeeding with professional support, although the small number of studies to date led to overall inconclusive review findings (Dib et al., 2022). One published intervention in a non-intensive setting implemented multidisciplinary breastfeeding support, parental education, and clinical protocol modifications for LPIs, and found increased breastfeeding rates in a post-hoc chart review (Estalella et al., 2020). These findings point to the acceptability of LPI breastfeeding support programs, but, overall, there is a paucity of information to guide institutions in implementing breastfeeding support for LPIs in the non-intensive care setting.
In light of these gaps in the evidence base, and the growing incidence of late preterm delivery among non-Hispanic Black and Hispanic populations in particular, our institution implemented a nursing-driven program to support LPI breastfeeding. Here we present the development, implementation, and nursing staff experiences of this program.
The “Early Bloomer” Program
Setting and Population
This intervention was conducted at an urban hospital with approximately 2,800 annual births. In 2019, 85% of mothers were government insured (indicating low income status), and more than two-thirds were from racially minoritized groups. The Mother Baby Unit (MBU) consists of 30 postpartum private rooms with a Level III Neonatal Intensive Care Unit (NICU) on the same floor. The hospital is Baby-Friendly certified. Routine newborn care includes immediate skin-to-skin holding, rooming in, and couplet care. Pasteurized human donor milk was introduced to the MBU in 2016 for LPIs. At baseline, we had two full time International Board Certified Lactation Consultants (IBCLC) dedicated to the MBU.
Approximately eight to 15 births per month were late preterm in 2019. Among these, all infants 34.6 weeks gestational age or younger were admitted to the NICU for their entire hospital stay. Those born at 36 weeks or greater were admitted to the MBU, and those born at 35.0 to 35.6 weeks first went to the NICU and, once observed and determined to be stable (12–24 hr), were considered for transfer to the MBU.
Program Design
Prior to implementing the “Early Bloomer” (EB) program in 2019, LPIs and their unique needs were not specifically recognized in MBU policy. While lactation consult and occupational therapist referrals were often placed, this was based on need identified by MBU staff, not automatic protocols for all LPIs. Donor milk had been offered for all LPIs since 2016, but the consent process was burdensome, requiring the signature of an attending physician at the bedside. Prior to implementation of the program, nurses had no official training in the unique medical problems of LPI, and late preterm birth was not considered when making nursing assignments.
To address these gaps in care and staff training, the initial design of the LPI program began in August 2017 with the convening of a multidisciplinary task force including MBU and NICU nurses, nurse managers, nurse educators, IBCLCs, and a pediatric nurse practitioner. The task force reviewed existing professional organization guidance (e.g., the Association of Women's Health, Obstetric and Neonatal Nurses’ [AWHONN] Late Preterm Protocol) and developed a comprehensive clinical guideline for the care of LPI, in which lactation support was substantially emphasized. The task force framed the clinical guideline using the theory of Diffusion of Innovation, (Rogers, 2003), which has five stages: (1) awareness, (2) persuasion, (3) decision, (4) implementation, and (5) continuation. Awareness, persuasion, and decision were promoted by nursing staff involvement, feedback, and communication at all stages of design and implementation. This was facilitated by previously incorporated shared governance practices across the nursing administration. Diffusion of Innovation was applied to the EB program through identification of nursing champions and solicitation of staff input into the program. All staff were invited to participate. To elicit a breadth of ideas staff were given multiple opportunities to provide input by participating in conversations and responding to questions like “What is your dream for LPI care?” and “ What would you love to have in an LPI policy?”
The Early Bloomer program aimed to increase human milk feeding (mother’s own milk and donor milk), and reduce hospital readmission among LPI. The program did this upon initial implimentation via staff training on the unique needs of LPI, parent education and support on differences in feeding and care compared to term infants, infant feeding team huddles, and workflow considerations. Diffusion of Innovation posits that early adopters are identified to help more rapidly diffuse new ideas into a larger group. We therefore identified “champion” nurses. These nurses implemented EB prior to dissemination to other staff, and then served as peer-educators in the following waves of implementation. Early adopters were identified by IBCLCs, and early implementation of the policy was highlighted in daily team rounds in front of other nurses (dissemination stage of Diffusion of Innovation). Finally, IBCLCs also checked in and did additional education with late adopters or cases in which they identified that more training and support was needed (continuation stage of Diffusion of Innovation).
Education for MBU nursing staff on the Early Bloomer Program was offered over a year and a half, using different modalities: competency days, distribution of articles, small group huddles involving unit staff and task force members, and in-services by inpatient IBCLCs and unit educators. Sessions introduced staff to the program’s components, order set, and materials. Nurse education focused on LPI’s neurodevelopmental prematurity, common pathology, and feeding challenges, as well as supporting frequent hand expression of milk. Over the implementation period, 90% of MBU nurses received EB training. Since then, EB training has been incorporated into the competency-based education that all newly hired nurses receive, which includes a full day shadowing an IBCLC as well as preceptor-led trainings.
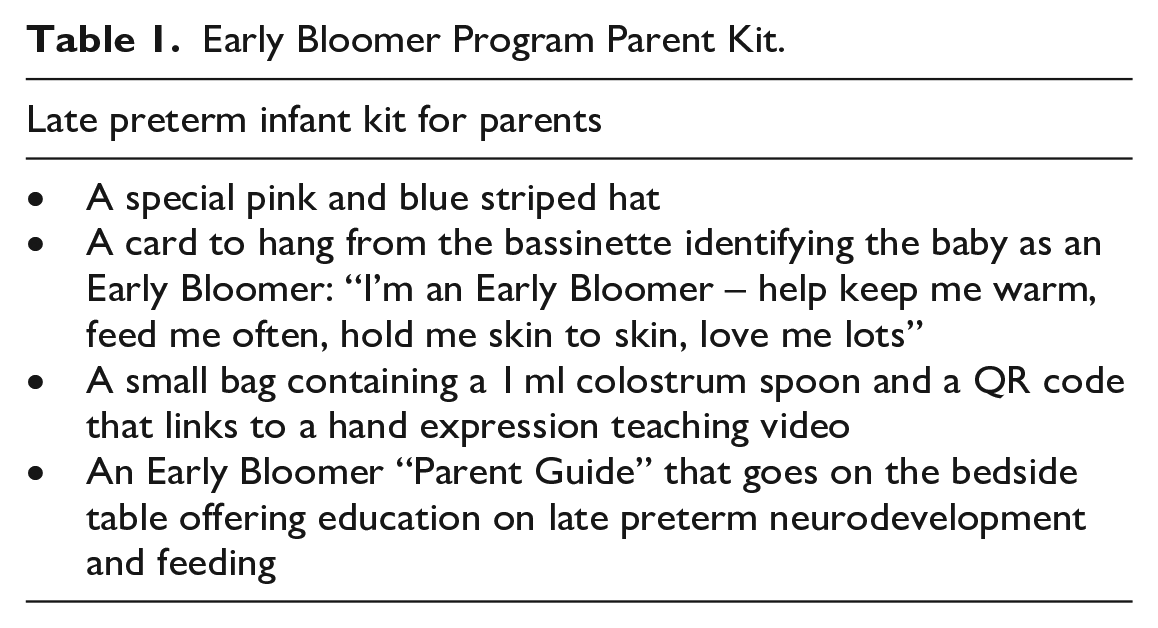
The program emphasizes parent education and interdisciplinary feeding support. Parents are given “swag bags” with educational resources on unique needs of LPIs and materials to support early hand expression and breastfeeding (Table 1). Feeding protocols emphasize hand expression, offering donor milk when mother’s milk is not readily available and ensuring feeding every 2–3 hrs. The donor milk protocol was modified to allow postpartum nurses to complete the consent with patients, rather than requiring physician input. Feeding support was augmented via early automatic lactation consults and bedside teaching by nurses. Additionally, for every dyad, a team huddle to address feeding was conducted at 12 hr of life and then as needed, and attended by the nurse, attending physician, IBCLC, parents and other members of the care team.
Early Bloomer Program Parent Kit.
The program enhanced unit-wide attention to LPIs by identification of late preterm gestation as higher need on daily nurse assignments (previously only opioid-exposed newborns were identified on assignments). Physical reminders were also implemented: infants received a unique striped newborn hat, and an “Early Bloomer” sign was put on the crib. Finally, the program included an electronic order set to be placed by the newborn admitting provider (Table 2) which operationalized the guidelines by automatically including orders for lactation consultation, occupational therapy consult, delayed bath, and vital sign measurements every 4 hr throughout hospitalization.
Early Bloomer Program Order Set.
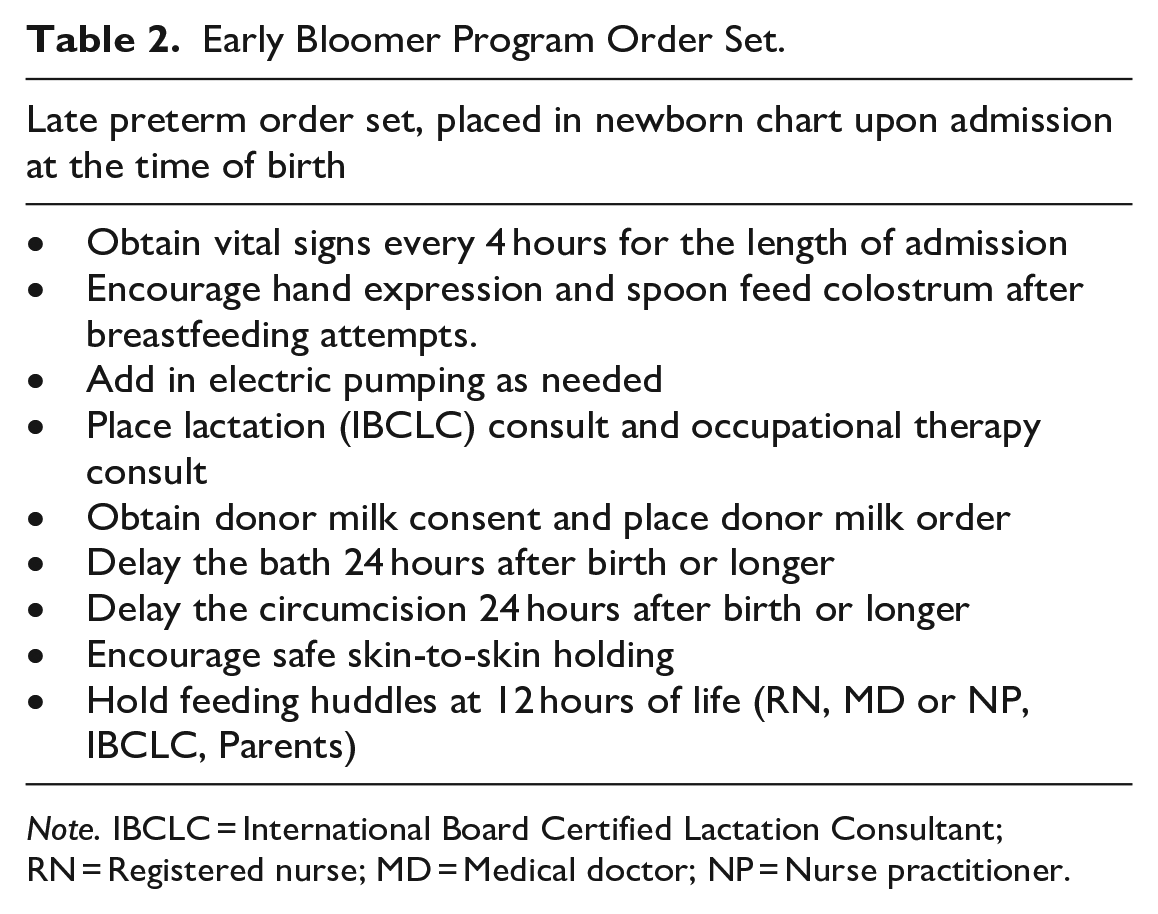
Note. IBCLC = International Board Certified Lactation Consultant; RN = Registered nurse; MD = Medical doctor; NP = Nurse practitioner.
The program, which continues to date, has built-in checks to ensure it is being implemented for each LPI dyad. The nurse manager, who monitors all admissions, checks that the EB protocol is being followed at daily interdisciplinary unit team meetings, and that staff assignments are made accounting for additional demands of caring for LPIs. Finally, IBCLCs assess whether EB application is being implemented and regularly discuss the protocol with nurses when consulted for LPIs.
Program Implementation
The Early Bloomer Program was launched on April 1, 2019. Keeping with a spring-time theme and in an attempt to make it fun and create a buzz, the nurse manager gave out Early Bloomer flower hats to staff. Pictures were posted on the MBU Nursing Facebook page. Regular meetings with MBU staff reviewing current and recent LPI cases identified areas in need of improvement and additions to the program over the first few weeks of implementation. Through this process the 12-hr team huddle was added, responding to a need for improved team and patient communication. Additionally, the order set was revised, and the swag bag was tested and modified.
Nursing Staff Perspectives
In the 2nd year of program implementation (January 2021), we sent an anonymous online questionnaire to all MBU nursing staff, with a 79.6% response rate. The questionnaire included questions about familiarity and satisfaction with the program, confidence carrying it out, and open-ended questions about their experiences with the program and LPI breastfeeding support.
The 43 respondents were all postpartum mother–baby nurses. They had a mean of 10.1 years (SD = 11.5) working on a mother–baby unit, and they reported having cared for a mean of 10.0 (SD = 11.6) LPIs since the program began. Among respondents, 95% reported they were moderately or very familiar with the program, and 95% reported they were somewhat or very confident providing breastfeeding support to LPIs. In write-in responses, nurses reported that they were more attentive to the needs of LPIs, more confident in their care, and more aware of possible complications and feeding needs. Three major themes emerged, as follows.
First, nurses reported increased confidence caring for LPIs due to the program’s education on LPI pathophysiology and its effect on their skills. Nurses noted that they were more confident and better able to help prevent complications through better “understanding of physiology at this gestation and their needs.” Many described using this knowledge to help educate parents, finding confidence in their work by “teaching moms about their late preterm baby and the difficulties they may experience breastfeeding their baby.” Others found the skills to support breastfeeding to be the most important: “my ability and experience to support moms with positioning, waking techniques, pumping, hand expression etc.”
Second, nurses found the program components facilitated improved care for LPIs. Many nurses described specific aspects of the policy as helping them to confidently care for LPIs. The order set helped keep track of different parts of the policy “so I don't have to try to memorize everything.” Many remarked on the special striped newborn hats, crib signs, and notations on daily patient assignments “to visually make everyone aware baby is an Early Bloomer.”
For some, the very existence of a policy was important: “I am confident by following the policy,” said one nurse. Many remarked that teaching hand expression to mothers and making feeding plans with the entire team were important aspects of the care they provided. One nurse commented that the program helped her support LPI breastfeeding by ensuring “a solid feeding plan determined in collaboration with pediatricians, lactation [consult service], mom and myself; early recognition if things aren’t going well; and frequent check-in by myself or lactation with mom to assist/evaluate feedings.”
Third, nurses reported continued barriers to breastfeeding support, including lack of overnight lactation consults and no involvement of labor and delivery staff in the program. Many nurses noted that they would like overnight staffing of the lactation consult service to help them to continue feeding plans that had been made during the day. Several respondents also brought up concerns that LPIs required closer attention and early breastfeeding support while still in the labor and delivery (L and D) suite. One nurse wrote,
My biggest concern is babies remaining in couplet care on L and D. . . . The Early Bloomers sometimes arrive to [the MBU] cold and with low sugars. The Early Bloomers can be forgotten because they are quiet, cute. Staff education on L and D would be helpful.
Another suggested: “More support or teaching with L and D nurses to empower them to learn and become more comfortable with hand expression.” Others also commented on the need for more time with a LPI, and suggested having fewer assigned patients if one were late preterm.
This program was not designed as research or quality improvement, and thus this report should not be interpreted as evidence of the efficacy of our approach. Limitations include lack of clinical outcome data, comparison group, or quality metric monitoring. Furthermore, it is limited to the experience of a single hospital.
Conclusion
The Early Bloomer Program is notable as a nursing-designed and nursing-driven program for LPIs in the non-intensive care setting. Nursing staff at our institution found that the program’s training and clinical care policies helped them confidently provide breastfeeding support for LPIs. The application of the theory of Diffusion of Innovation may have helped engage staff and promote the adoption of the EB program. We hope that this report may guide other institutions in developing LPI policies. Future interventions should solicit input from parents of LPIs in program development, and consider the inclusion of labor and delivery staff in the program. Given the dearth of research on LPIs, there is an urgent need for well-designed studies, specifically randomized controlled trials, to identify hospital-based strategies to equitably increase breastfeeding in this growing population.
Footnotes
Acknowledgements
We are grateful to all the patients who have entrusted us with their care; the nursing staff, administration, and providers who have integrated the Early Bloomer program into their daily practice and given feedback on the program; and Ha Uen Kim, MPH, for her assistance in reviewing surveys.
Author Contributions
Disclosures and Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Standish was funded by a HRSA T-32 fellowship at the time of conducting surveys with nursing staff.