
Abstract
Background:
Breastfeeding is the best source of nutrition for infants. Health literacy is a critical factor affecting breastfeeding rates.
Research Aims:
The aim of this research was to develop and test the Breastfeeding Health Literacy Scale to determine its validity and reliability.
Methods:
This study featured a cross-sectional telephone survey design. Researchers reviewed the literature and used expert opinions to develop the content-validated 30-item Breastfeeding Health Literacy Scale covering five dimensions. We examined internal consistency, exploratory factor analysis, and confirmatory factor analysis to assess reliability and construct validity. A Taiwanese government organization provided potential participants’ contact information. After mailing an invitation letter, researchers phoned all participants to invite participation, obtain oral consent and complete a Breastfeeding Health Literacy Scale and collect demographic data.
Results:
Participants (N = 300) had a mean age of 31.8 (SD = 4.66) years. The item-level content validity index was 0.67 to 1.00 and scale-content validity index was 0.94. After performing exploratory factor analysis, three factors were extracted. Examining content factor analysis for the three factors resulted in χ2/df = 2.05; p < .001; goodness of fit index = 0.90; Comparative Fit Index (CFI) = 0.96; and Root Mean Square Error of Approximation (RMSEA) = 0.06. Cronbach’s alphas on the total scale and the subscales ranged from 0.87 to 0.94. Women with multigravida, breastfeeding information from physicians and nurses, and previous breastfeeding experience had better breastfeeding health literacy.
Conclusions:
Psychometric analysis demonstrated that the newly developed 20-item Breastfeeding Health Literacy Scale is a valid self-assessment instrument. Improving breastfeeding health literacy during pregnancy could help enable breastfeeding success.
Keywords
Key Messages
Health literacy is the capacity of individuals to obtain and understand basic health information and services required to make appropriate health decisions.
The Breastfeeding Health Literacy Scale consists of a broad range of literacy cognitive dimensions to evaluate women’s ability to obtain, understand, and assess breastfeeding-related information and communicate with healthcare providers.
Psychometric analyses of the scale demonstrated that the Breastfeeding Health Literacy Scale had good reliability and validity.
Background
The World Health Organization (WHO, 2022) and the United Nations Children’s Fund (UNICEF) recommend exclusive breastfeeding for the first 6 months of life. Breastfeeding provides the best source of nutrition for all infants. However, only 44% of infants were exclusively breastfed from 2014 to 2020 worldwide (UNICEF, 2021). The percentage of infants aged 0–5 months exclusively breastfed varies from region to region: 55% in Eastern and Southern Africa, 57% in South Asia, 26% in North America, and 41% in Eastern Europe and Central Asia (UNICEF, 2021). In Taiwan, a high breastfeeding initiation rate (83.7%) was reported for newborn infants (Chuang et al., 2010), but the exclusive breastfeeding rate at 6 months fell to 46.2% in 2018 (Health Promotion Administration [HPA], 2019).
Several sociodemographic factors, including young maternal age, low education and income, low maternal breastfeeding self-efficacy, perceived insufficient milk production, nipple pain, Cesarean section, employment status, and weak social support influence breastfeeding cessation (Forster et al., 2006; Meedya et al., 2010; Morrison et al., 2019). Many studies have identified the relationship between breastfeeding rates and maternal feeding knowledge, self-efficacy, attitudes toward breastfeeding, social support, health literacy, and decision-making (Cohen et al., 2018; Forster et al., 2006; Meedya et al., 2010). For example, mothers with prior breastfeeding experience, greater breastfeeding knowledge, and assistance and information from professional hospital staff exhibit a higher breastfeeding rate (Hamze et al., 2019). Conversely, mothers with low or limited general health literacy (HL) are less likely to breastfeed their infants (Hosseini et al., 2019; Mirjalili et al., 2018; Stafford et al., 2016).
The Institute of Medicine (IOM) described HL as the capacity of individuals to obtain and understand basic health information and services required to make appropriate health decisions (Institute of Medicine, 2004). According to the WHO (2009), HL is defined as “the cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand and use information in ways which promote and maintain good health.” The United States National Institutes of Health (NIH, 2021) define HL as the ability of individuals to find, understand, and use information to make health-related decisions. The new definition of HL in Healthy People 2030 emphasizes the ability of individuals to use health information rather than just understand it and to make correct decisions rather than suitable ones (Office of Disease Prevention and Health Promotion [ODPHP], 2022).
Three levels of HL include functional, communicative/interactive, and critical (Nutbeam & Kickbusch, 2000). Functional health literacy involves basic reading and writing abilities, which can be applied to daily life and regular activities. Communicative/interactive health literacy includes a higher level of cognitive and social skills to actively participate in daily activities, obtain new information in different ways, and understand and apply new information to improve the environment, such as communicating with professionals or actively participating in activities to obtain new knowledge. Critical health literacy functions at the highest level of cognitive and social skills and consists of the ability to critique and analyze newly acquired information and use this information to grasp life events and situations. Multiple studies indicate that people with limited health literacy have worse health status and higher rates of hospitalization (American College of Obstetricians and Gynecologists, 2016; Batterham et al., 2016). In addition, low HL leads to decreased use of preventive services, such as mammography and influenza vaccination, and improper interpretation of medication and nutrition labels (Berkman et al., 2011).
Many studies have used the concepts of HL to develop scales that assess HL regarding various health and disease conditions (Azizi et al., 2019; Wei et al., 2017); however, a suitable scale for exploring breastfeeding HL in Taiwan has not yet been developed. A reliable and valid instrument that measures HL for breastfeeding is critical for assessing the influence of breastfeeding HL on decision-making about breastfeeding. Improving breastfeeding HL may increase the breastfeeding rate. Currently, recognition of the importance of breastfeeding HL is limited; additionally, no comprehensive multiple-dimensional assessment scale is available in Taiwan. Hence, the aim of this study was to develop and test the Breastfeeding Health Literacy Scale (BFHLS) and determine its validity and reliability.
Methods
Research Design
This study featured a cross-sectional telephone survey design. This study obtained approval from the Hospital’s Institutional Review Board (No. 21MMHIS296e, 2021/10/12).
Setting and Relevant Content
In Taiwan, the exclusive breastfeeding rate at 6 months was 46.2% in 2018, which is higher than the average rate worldwide (HPA, 2019). Sociodemographic factors, including higher education levels, unemployed status, and higher parity were related to an increased breastfeeding rate (Kuo, 2019). Many resources are available for breastfeeding mothers. For example, the HPA (2019) developed a breastfeeding brochure and established the official breastfeeding website; in addition, many hospitals offer breastfeeding consultations to assist with solving breastfeeding problems. HPA is one of several government organizations that encourage medical institutions to implement prenatal education, including breastfeeding, and subsidize medical institutions for educational guidance fees. Subsidies begin after diagnosis by a doctor confirming pregnancy of less than 17 weeks, and the second subsidy is received once pregnancy is over 29 weeks of gestation.
Sample
The HPA in Taiwan provided potential participants’ contact information for this study. Inclusion criteria were current pregnancy, age ≥ 20 years, and an ability to speak Mandarin. Exclusion criteria included women who could not speak Mandarin. For the purposes of this study to test the reliability and validity of a new scale, the ratio of the number of scale questions to the number of samples was 1:10, and the number of items in this scale was 30 (Tinsley & Tinsley, 1987). A total of 300 participants were required because the revised version of the BFHLS included 30 items. Telephone interviews took 10 min to complete, and each participant received a gift card valued at $4 to compensate for their time and effort participating in this research study.
Measurement
BFHLS Development
Studies have indicated that HL is a multidimensional concept that includes access, understanding, assessment, decision-making, application, communication, and self-efficacy (Azizi et al., 2019; Wei et al., 2017). The current study reviewed the literature, including the Health Literacy Scale for Workers (Azizi et al., 2019) and the Mandarin Multidimensional Health Literacy Questionnaire (Wei et al., 2017), and used expert opinions as the basis for the development of the BFHLS. To focus on breastfeeding health literacy, one item was developed stating, “I can obtain information about my breastfeeding.” The 37-item BFHLS consisted of six subscales, including access (three items), understanding (12 items), assessment (four items), communication or interaction (11 items), decision-making (three items), and self-efficacy (four items).
Content Validity of BFHLS
The draft version of the BFHLS was reviewed by an expert panel of six professionals, including International Board Certified Lactation Consultants (IBCLCs) and professionals in the fields of obstetrics and gynecology, and HL. To guide appropriate modifications of the BFHLS, each expert rated the relevance of every item on a 4-point Likert scale from 1 (very irrelevant) to 4 (very relevant). The item-level content validity index (I-CVI) was calculated based on the proportion of ratings of three or above, given by panel members. The panel suggested removing the subscale of self-efficacy because it was not a key dimension of HL. The I-CVI was calculated again; 30 items with an I-CVI of 0.92 (0.67-1.00) were marked as relevant, and the scale-level content validity index (S-CVI) was 0.94. This 30-item adjusted version of the BFHLS was piloted with a sample of 50 pregnant participants. Feedback obtained from the pilot sample was analyzed, and the questionnaire was revised to increase readability and minimize misinterpretations. This revised version was further reviewed by an expert panel of six professionals to obtain the final 30-item BFHLS with five subscales: access (five items), understanding (12 items), assessment (four items), communication or interaction (five items), and decision-making (four items). Each item was rated on a 5-point Likert scale, from 1 (strongly disagree) to 5 (strongly agree). Higher scores reflect higher breastfeeding HL as perceived by participants.
Data Collection
The data were collected from July to December 2021. After developing the 30-item BFHLS, we obtained access to potential participants from the Health Promotion Administration (HPA), a government organization in Taiwan. In order to encourage medical institutions to implement prenatal education such as breastfeeding, HPA subsidizes each medical institution for education guidance fees. After healthcare providers provide this guidance, they upload their patients’ information, including gestational age, age, addresses, and phone numbers to the HPA. After receiving potential participants’ names and phone numbers from the HPA, we mailed invitation letters to prospective participants and conducted follow-up phone calls to obtain oral consent and provide research objectives, participation benefits, and instructions for completing the research questionnaire. If individuals provided their consent, the research questionnaire was administered by phone. If they responded “no,” they received a thank you message from research staff and the phone call was terminated. A total of 1,200 pregnant participants were recruited, with responses received from 300 participants, a response rate of 25%. All participants provided demographic data (i.e., age, education, marital status, employment, and other socioeconomic information), as well as pregnancy stage, previous breastfeeding experience, and breastfeeding information received from physicians and nurses. Educational levels included high school or less, college/university, postgraduate; employment status included unemployed, part-time, and full-time; marital status included married and unmarried; antenatal care institution included medical centers, regional and district hospitals, and clinics; and previous breastfeeding information from physicians and nurses was classified as yes or no.
Data Analysis
Descriptive statistics were used to summarize demographic characteristics. The normality of data distribution was assessed by examining its skewness and kurtosis values of less than 3 and 8, respectively (Kline, 2005). Content validity was used to evaluate the appropriateness and clarity of the content of each item for the proposed scale. Experts were invited to complete, evaluate, and revise the study questionnaire to establish content validity for the scale and questionnaire clarity. According to Polit and Beck’s (2006) content validity standard recommendation (item-level content validity index, I-CVI) calculation method, experts who score more than 4 points were included as 1 point and those who scored below 2 points are included as 0 points. This method divides the number of experts with a score of 3 or above by the total number of experts. When there are six or more experts, the standard value I-CVIs should not be less than 0.78 (Lynn, 1986). The scale-level content validity index (S-CVI) equals the sum of I-CVI divided by the total number of questions. The recommended standard value should be above 0.80 (Waltz et al., 2010).
We performed exploratory factor analysis (EFA) which used principal component factor analysis with varimax rotation to interpret the maximum amount of variance for participants (Meyers et al., 2017). Items with loading values of less than 0.50 were deleted. Confirmatory factor analysis was conducted using structural equation modeling (SEM) to test HL constructs. Model fitness was assessed using the following fit indices: the chi-square (χ2) value and the degree of freedom ratio (χ2/df), Root Mean Square Error of Approximation (RMSEA), Comparative Fit Index (CFI), and Goodness of Fit Index (GFI). To determine how well the model fit the data, the research team set criteria to include a nonsignificant goodness-of-fit, χ2/df ratio less than 5, and CFI and GFI greater than 0.90. A RMSEA less than 0.08 indicates a good fit between empirical data and the model. Finally, researchers used the Akaike Information Criterion (AIC), a predictive fit index, to compare competing nonhierarchical models fitted to the same data. Model modification was conducted when the proposed model was not acceptable or would not converge. Once the final measurement model was determined, the internal consistency of all subscales was evaluated using Cronbach’s alpha. When examining discriminant validity, estimated correlations between factors should not be excessively high (e.g., > 0.85; Kline, 2005).
The reliability is based on the proposal by DeVellis (1991) stating that Cronbach’s alpha coefficient value must be greater than 0.70, which means that the scale has good internal consistency (between 0.70~0.80 is acceptable, and between 0.80~0.90 is good). A p value of < 0.05 was considered statistically significant.
Results
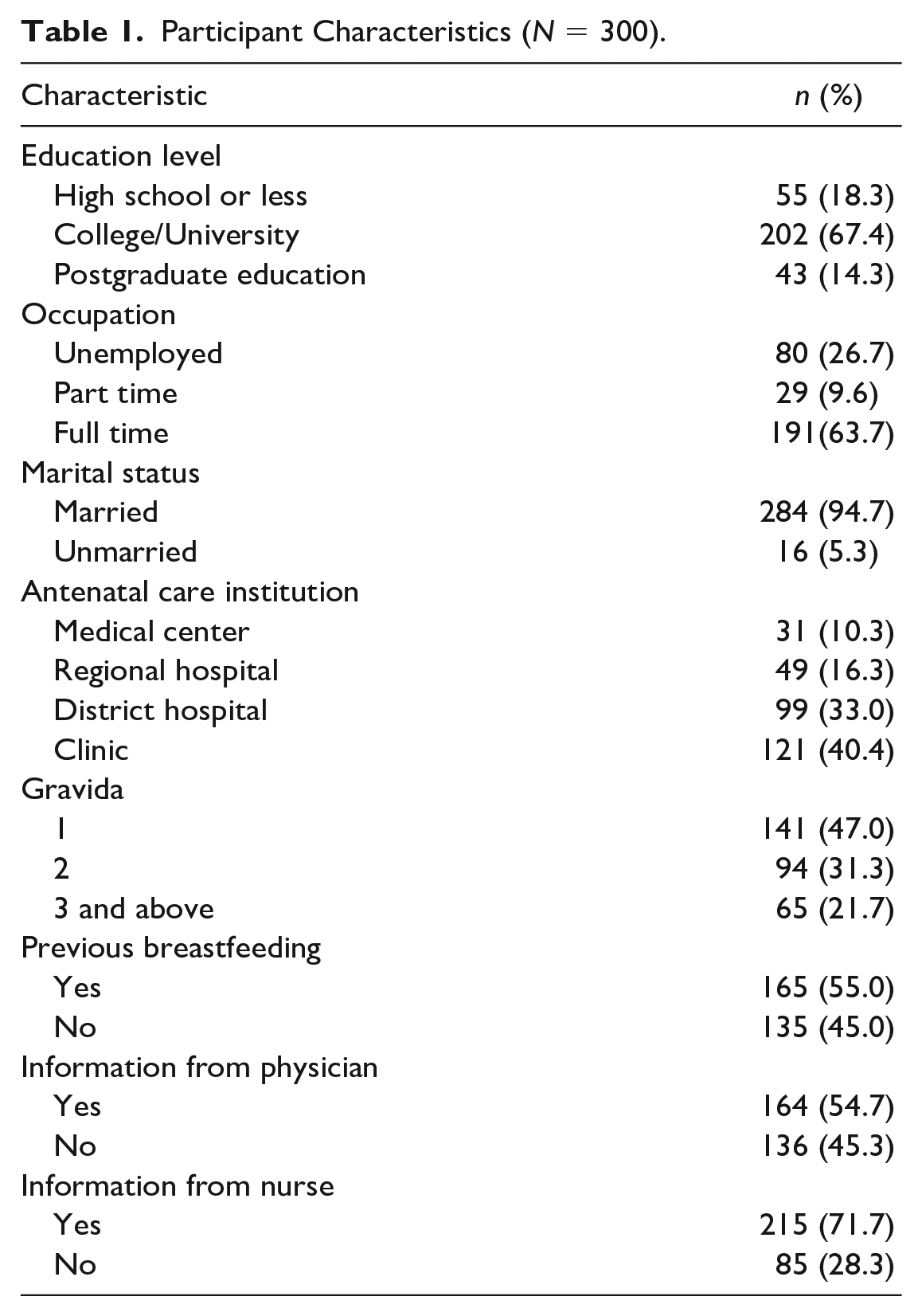
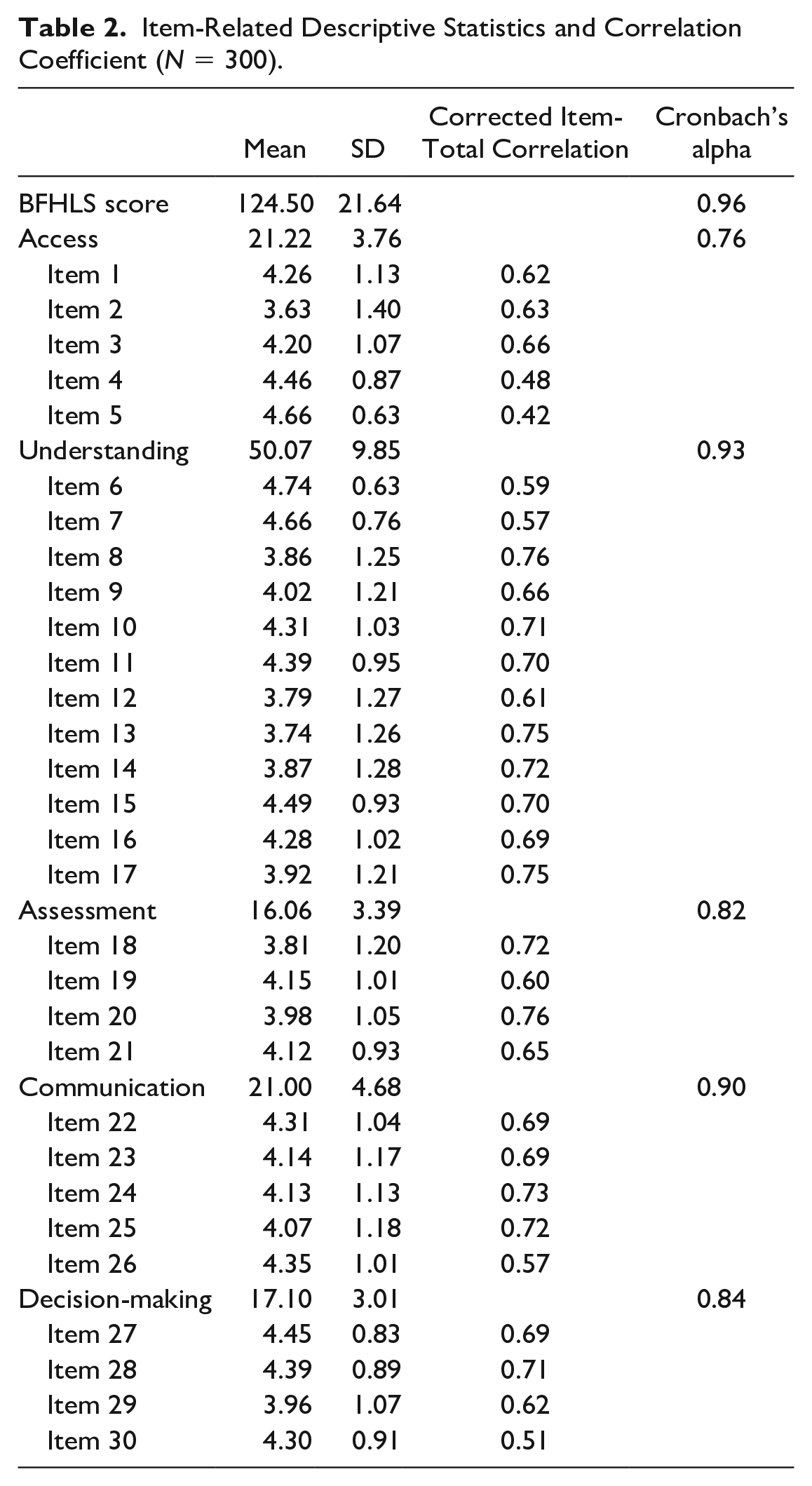
A total of 300 participants were included in this study. As listed in Table 1, participants’ mean age was 31.8 (SD = 4.66) years old, and most were married (94.7%, n = 284). The majority had obtained a college or university education (67.4%, n = 202), and more than half worked full-time (63.7%, n = 191). Approximately half were primigravid (n = 141, 47.0%), and 54.7% (n = 164) and 71.7% (n = 215) reported receiving breastfeeding information from obstetricians and nurses, respectively. Means (SD) across items ranged from 3.6 (1.40) to 4.7 (0.63); mean of BFHLS was 124.5 (SD = 21.64) and ranged from 42 to 150. The item-total correlation was used to examine item discrimination, which ranged from 0.42 to 0.76, and the range of Cronbach’s alpha coefficient was 0.82–0.96 (Table 2). Correlation coefficients between the items ranged from 0.19 to 0.69. The I-CVI was 0.67–1.0, and S-CVI was 0.94. After running the normality of distribution, items 6 and 7 had greater skewness and kurtosis and were deleted.
Participant Characteristics (N = 300).
Item-Related Descriptive Statistics and Correlation Coefficient (N = 300).
Validity
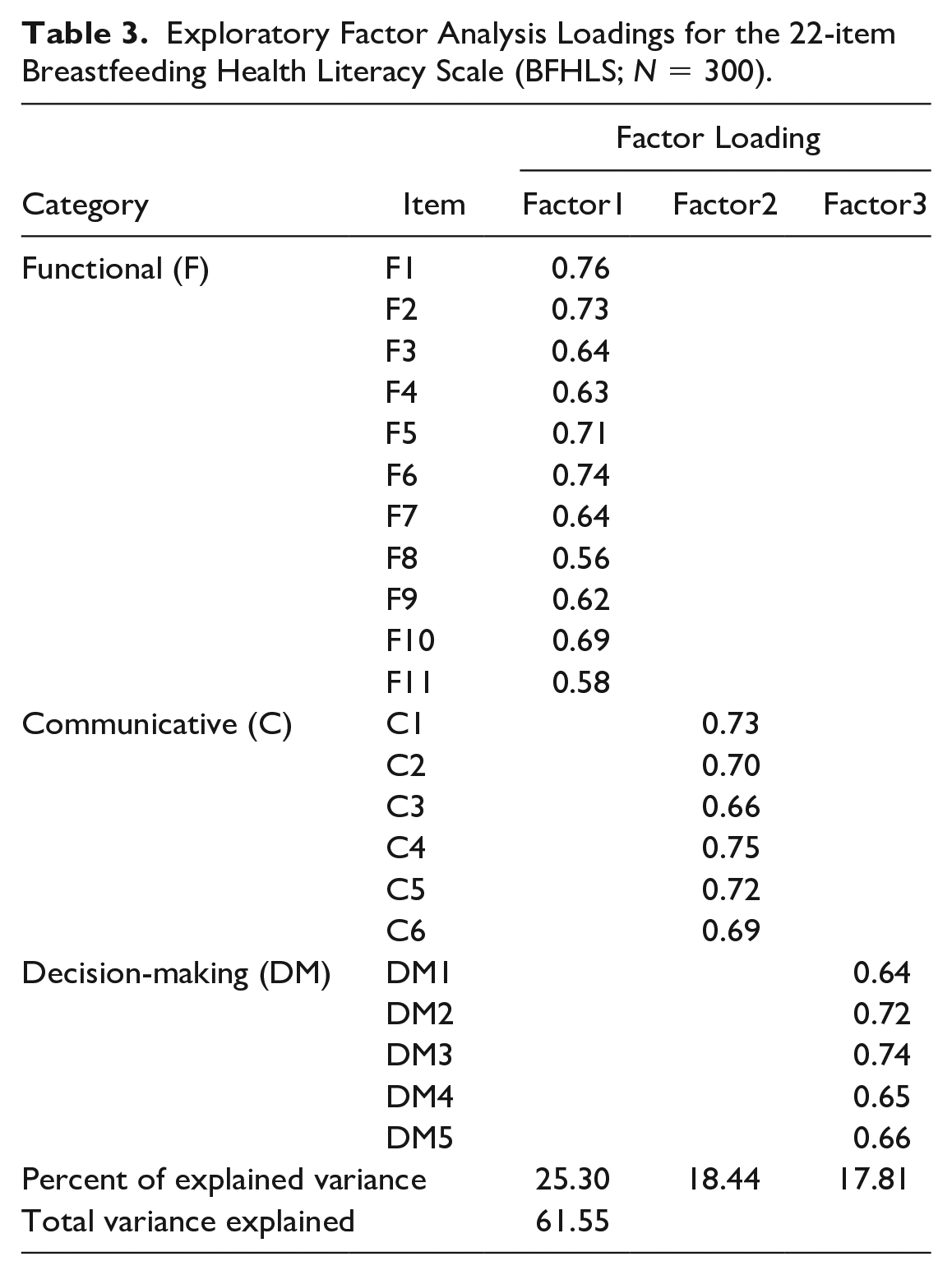
A principal component factor analysis with varimax rotation was conducted for the 28 items. All items had a factor loading higher than 0.50. After running EFA, three factors including 22 items that explained 61.55% of the variance were extracted (see Table 3). We labeled the subscales as follows: functional (11 items), communicative (six items), and decision-making (five items). CFA of the 3-factor model was based on the EFA resulting in χ2/df ratio = 3.04 (p < .001), RMSEA = 0.08, GFI = 0.84, and CFI = 0.92. Results indicated that the model did not fit the data very well. Because some factor loadings were lower than 0.65, the researchers modified the CFA model through an iterative process. Items with large, standardized residual and low factor loading were removed individually. The CFA model was re-estimated and re-examined until all items had factor loadings of at least 0.65. Thus, two items were deleted resulting in χ2/df = 2.05; p < .001; GFI = 0.90; CFI = 0.96; and RMSEA = 0.06, indicating an acceptable fit of the CFA second-order model with 20 items, as displayed in Figure 1. The composite reliability (CR) of the three factors was 0.94, 0.91, and 0.88, respectively. The average variance extraction (AVE) of the three subscales was 0.58, 0.62, and 0.72, respectively. CR was greater than 0.60 and AVE greater than 0.50, indicating that the convergent validity of the construct was adequate (Fornell & Larcker, 1981).
Exploratory Factor Analysis Loadings for the 22-item Breastfeeding Health Literacy Scale (BFHLS; N = 300).
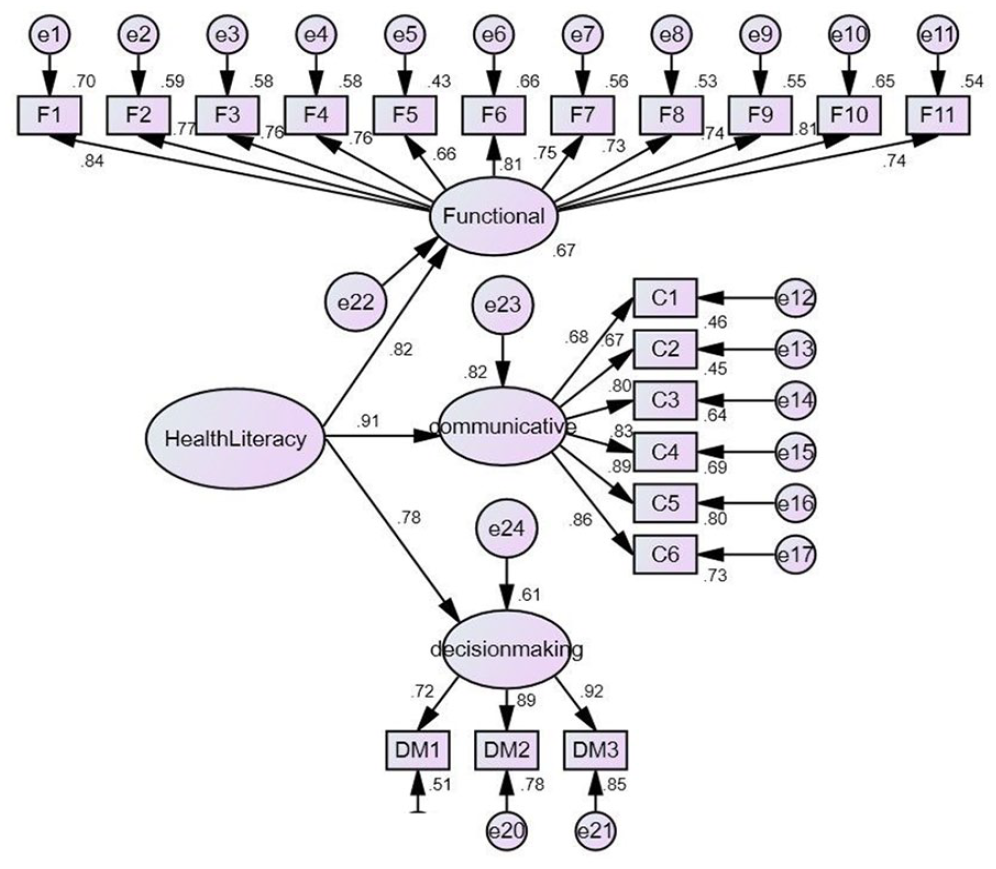
CFA Model.
Reliability
The total score of the remaining 20 items was evaluated, and results revealed that the Cronbach’s alpha of the BFHLS was 0.95 and those of the three subscales ranged from 0.87 to 0.94. Thus, Cronbach’s alpha of all subscales exceeded the minimum acceptable value of 0.70 for internal consistency. Table 4 lists the Pearson correlations between the BFHLS subscales.
Pearson Correlations Between the Breastfeeding Health Literacy Subscales.
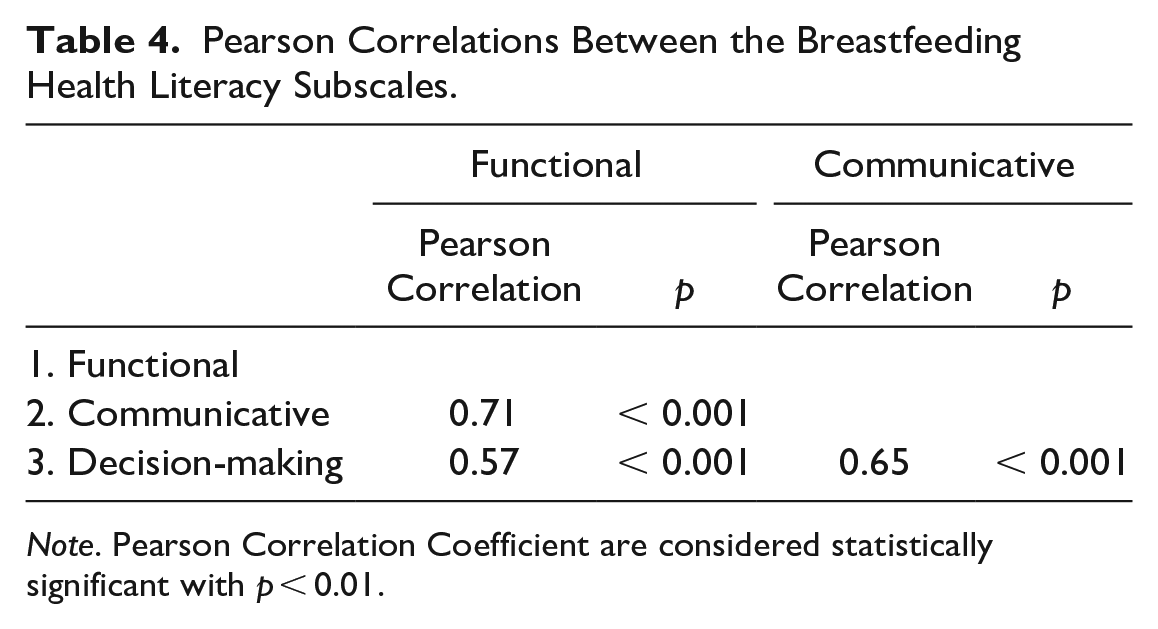
Note. Pearson Correlation Coefficient are considered statistically significant with p < 0.01.
Significant differences in the total score and the scores of the three subscales were observed between primigravid and multigravid participants. The multigravid group exhibited a higher total score on the BFHLS (F = 22.74, p < 0.001) and the three subscales of functional (F = 24.40, p < 0.001), communicative (F = 13.86, p < 0.001), and decision-making (F = 7.13, p < 0.001) than the primigravid group, indicating optimal comparison validity between groups. Breastfeeding information received from obstetricians and nurses and from previous breastfeeding experience also had a significant correlation with the BFHLS, suggesting good predictive validity. Participants who received breastfeeding information from obstetricians exhibited a higher total score on the BFHLS (t = 7.39, p < 0.001) and on the three subscales: functional (t = 5.63, p < 0.001), communicative (t = 8.58, p < 0.001), and decision-making (t = 5.56, p < 0.001), than participants who did not receive information. Participants who received breastfeeding information from nurses exhibited a higher total score on the BFHLS (t = 9.96, p < 0.001) and the three subscales: functional (t = 7.08, p < 0.001), communicative (t = 12.72, p < 0.001), and decision-making (t = 7.05, p < 0.001), than participants who did not receive information. In addition, participants with previous breastfeeding experience exhibited a higher total score on the BFHLS (t = 8.09, p < 0.001) and the three subscales: functional (t = 8.76, p < 0.001), communicative (t = 5.95, p < 0.001), and decision-making (t = 3.88, p < 0.001), than participants who did not have previous experience. However, no significant differences in BFHLS and subscale scores were observed among age, marital status, income, education, and employment groups.
Discussion
This methodological study developed the BFHLS and evaluated its psychometric properties. The initial scale was designed by reviewing existing questionnaires about HL and using expert opinions as the basis for development. The respecified CFA model of the BFHLS can be used to measure breastfeeding HL. Most participants completed the BFHLS within 10 min; therefore, the scale can easily be used for clinical screenings.
Health literacy is a crucial competency necessary for making informed health decisions, obtaining and interpreting health-related information, and improving quality of life (Zarcadoolas et al., 2005). Several factors, including gravidity, receipt of breastfeeding information from obstetricians and nurses, and previous breastfeeding experience, influenced breastfeeding HL. Results of this study are consistent with those of previous studies (Osborn et al., 2011). Women in the lowest HL group were less likely to exclusively breastfeed their children (Stafford et al., 2021).
Parents with previous breastfeeding experience have more knowledge and a better understanding of breastfeeding (Che’Muda et al., 2018). Those who received more education on breastfeeding are more likely to initiate and continue exclusive breastfeeding (Cohen et al., 2018). The research team observed that education level did not have any significant influence on breastfeeding HL, a result that is inconsistent with previous studies (Chung et al., 2015; Vila-Candel et al., 2021). The reason may be that most of our study participants were well educated. Thus, HL could be increased if healthcare providers in antenatal care clinics proactively offered breastfeeding information.
Overall, the final 20-item BFHLS scale showed good internal consistency reliability and satisfactory construct validity, based on the analyses of factorial, convergent, and known group validity. Moreover, the length of this scale is appropriate, and can be used to screen pregnant women’s breastfeeding HL or to assist governments in formulating a breastfeeding health policy that could support improvements in the breastfeeding rate.
The questionnaire was administered by telephone. Telephone interviews are advantageous for both researchers and study participants because they allow coverage of a greater geographic area in a timely fashion, leading to a more efficient data collection process (Gourlay et al., 2021). Moreover, this research method decreases the costs of travel and potential lost time. Telephone interviewing is an effective method of data collection for clinical nursing research when interviewers are properly prepared.
Limitations
Several limitations apply to this study. Telephone interviews have limitations, including the need for interviewers to remain focused and engaged to keep the interview on course and the likelihood of respondents being distracted during the interview. To alleviate these concerns, researchers confirmed respondents’ availability before interviewing. Despite the benefits of telephone interviews, telephone respondents might present themselves in socially desirable ways, introducing bias. Although the average age of our sample was similar to all pregnant women in Taiwan (Ministry of Interior, 2021), our sample may not be generalized to other ethnic groups. Results may be biased because participants' trimester status was not clear in this study and, in addition, moderate to strong correlations were found between each of the subscales. Health literacy is a dynamic process; hence, it is possible that, compared to those in the first trimesters, a participant in the third trimester could have better health literacy. Furthermore, this is a new scale and the first time it was tested with pregnant participants. Therefore, additional and more evidence-based validity tests are necessary for future research (Waltz et al., 2010). For example, we can compare the Iowa Infant Feeding Attitudes Scale (IIFAS) and/or the Breastfeeding Self-Efficacy Scale (BSES) to the BFHLS for determining validity.
Conclusions
The BFHLS is the first instrument that evaluates how pregnant women assess, understand, communicate, and make decisions about breastfeeding. It provides a preliminary understanding of pregnant women’s breastfeeding HL. This newly developed 20-item BFHLS is a valid self-assessment instrument. Improving breastfeeding HL for pregnant women may enable them to adopt breastfeeding behaviors and increase their breastfeeding rate. This scale can provide healthcare providers with valuable information on patients’ breastfeeding HL, thereby guiding them in designing appropriate breastfeeding education. Future development of the scale could include an interactive and situational questionnaire (i.e., a questionnaire based on a breastfeeding situation) to evaluate women’s breastfeeding HL and examine women’s ability to criticize, analyze, and use this information to decide their breastfeeding behavior after delivery.
Footnotes
Author Contributions
Disclosures and Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Health Promotion Administration, Ministry of Health and Welfare (No. C1100409). The content of this research may not represent the opinion of the Health Promotion Administration, Ministry of Health and Welfare.