
Abstract
Background:
Breastfeeding is very important for maternal and infant health. With first pregnancies, many pregnant people face obstacles to achieving their breastfeeding goals.
Research Aims:
We aimed to investigate the outcomes of a breastfeeding education program and nurse-led online breastfeeding counseling system (BMUM) on breastfeeding self-efficacy, attitudes about breastfeeding, breastfeeding problems, breastfeeding frequencies and postpartum depression.
Methods:
This study was a randomized controlled trial. Participants were randomly assigned to the intervention group (n = 36), or control group (n = 36). Assessments were conducted during pregnancy, between 32- and 37-weeks gestation, and on postpartum Day 1, Week 1, Week 3, and 6 months.
Results:
The means of the Breastfeeding Self-Efficacy–Short Form scores, and the Infant Feeding Attitude Scale (IIFAS) scores were similar between the groups at the first assessment (p = 0.733). IIFAS scores in the intervention group were significantly higher in the follow-up measurements on postpartum Day 1, Week 1, Week 3, and 6 months compared to scores in the control group (p = 0.006; p = 0.000; p = 0.002; p = 0.001) Edinburgh Postpartum Depression Scale (EPDS) scores were similar between the two groups at 1 week (p = 0.678). EPDS scores were significantly higher in the control group on Day 1 and at 3 and 6 months postpartum (p = 0.000; p = 0.038; p = 0.042). There was no statistically significant difference in breastfeeding problems between the two groups (p > 0.05 across breastfeeding problems examined). The mean values of breastfeeding frequency were similar between groups on Day 1, and significantly higher in the intervention group on follow-up measurements.
Conclusion:
The results of this intervention appear to promote positive attitudes toward breastfeeding and decrease feelings of postpartum depression. However, further randomized controlled trials are needed to support our outcomes.
Key Messages
Primiparas mothers can face many obstacles in achieving their breastfeeding goals.
The Breastfeeding Training Program and Nurse-led Breastfeeding Online Counseling System (BMUM) was associated with an increase in breastfeeding self-efficacy and infant feeding attitudes and a decrease in postpartum depression.
Participants receiving support from the BMUM program nursed more frequently.
Background
Breastfeeding is undoubtedly the gold standard for nutrition in the first 12 months of life (Krol & Grossmann, 2018). Breastfeeding has short- and long-term benefits. Infants who are breastfed have lower rates of mortality and morbidity from infectious diseases (Victora et al., 2016). It enhances the psychological wellbeing of both mother and child (Krol & Grossmann, 2018) and is positively associated with maternal attachment (López-Fernández et al., 2022).
The rate of exclusive breastfeeding in the first 6 months was 48% worldwide based on 2015 to 2021 data (United Nations Children’s Fund [UNICEF], 2022). Although breastfeeding is common practice in Turkey, the rate of exclusive breastfeeding during the first 6 months after birth is low. According to the 2018 Turkey Demographic and Health Survey (TDHS) Data (2018), 41% of children younger than 6 months were exclusively breastfed.
Self-efficacy in breastfeeding is one of the potentially modifiable factors that is consistently linked with positive breastfeeding outcomes (Husin et al., 2017). Breastfeeding education programs have positive effects on breastfeeding self-efficacy (Chipojola et al., 2020; Iliadou et al., 2018).
In a study conducted by Gianni et al. (2019) 70.3% of their participants reported breastfeeding difficulties, including cracked nipples, a sense of insufficient milk, soreness, and exhaustion. Blixt et al. (2019) also reported that mothers have difficulties breastfeeding, especially in the first few days after birth, and with discharge from their birthing facilities. They concluded that breastfeeding requires professional, technical, and individualized support and education. Inadequate breastfeeding frequency can also lead to premature cessation of breastfeeding (Çınar, 2018).
Postpartum depression may occur during the postpartum period (Cristescu et al., 2015). In Turkey the cultural expectation is that for 40 days a postpartum woman is not left alone. First-degree relatives help the new mother with breastfeeding and the care of her baby during this time. This support has been shown to be effective in reducing the risk of postpartum depression (Öztürk et al., 2012). Limited social support may lead to feelings of loneliness and exhaustion and may increase susceptibility to postpartum depression. Monitoring and giving feedback to mothers can enhance self-efficacy, learning motivation, and performance (Shafaei et al., 2020). Providing education on health topics, including breastfeeding, is a vital part of a nurse's professional role (Blixt et al., 2019). Nurses working in the field of women's health are at the forefront of health services in promoting breastfeeding, and providing education and counseling for breastfeeding problems.
The conceptual framework for this study was based on Bandura’s social cognitive theory, which highlights self-efficacy and behavioral competence (Bandura, 2001). Dennis applied these constructs to her breastfeeding self-efficacy theory (Dennis, 1999). To improve self-efficacy and personal empowerment, proper techniques and educational interventions can be helpful (Hannula et al., 2008). Professional support and feedback received from health professionals plays an important role in increasing breastfeeding self-efficacy (Brockway et al., 2017; Wood et al., 2017; Yang et al., 2016). Zubaran and Foresti (2013) found that postpartum depression rates were lower when participants had high levels of breastfeeding self-efficacy. In addition, continuous support can reduce postpartum depression. During the postpartum period, the lack of opportunities to consult with healthcare professionals or friends, the absence of support from parents or other family members after birth (Tsuno et al., 2022), and lack of decision-making in breastfeeding choices (Harris et al., 2023) can lead to postpartum depression.
The aim of this study was to investigate the effectiveness of a prenatal breastfeeding workshop and an online breastfeeding counseling system on breastfeeding self-efficacy, attitudes about breastfeeding, breastfeeding problems, breastfeeding frequencies, and postpartum depression. We hypothesized that the intervention would have a positive effect on breastfeeding self-efficacy, breastfeeding problems, postpartum depression, and breastfeeding frequency.
Methods
Research Design
This was a randomized controlled trial. The study received ethical approval from the Kastamonu University Ethics Committee (No: 4/6/September 16, 2020). This manuscript follows the Consolidated Standards of Reporting Trials (CONSORT) reporting guidelines for randomized studies.
Setting and Relevant Context
There are three hospitals in Kastamonu—two private hospitals and one state hospital—providing maternity care services. This study was conducted in the state funded hospital which has the largest patient population, providing care for most of the births in this region. The hospital has been certified as a Baby-Friendly hospital since 2019. Prenatal and postpartum care is typically provided by midwives and nurses. Women who have had an uncomplicated vaginal delivery stay in the hospital for 24 hours while those who have had a Cesarean section normally stay for 48 hours. One week after birth, mothers are routinely checked for postpartum status in the hospital where they gave birth. During these routine visits, family physicians will check on the general health status of infant(s) and the mother, including assessment for breastfeeding status and breastfeeding problems. According to the Turkish Demographic and Health Survey Data (TNSA, 2018), the rate of breastfeeding in the 1st hour after birth is 71.3%, and the rate of exclusive breastfeeding during the first 6 months of life is 41%. It is expected that women exclusively breastfeed for 6 months (including the 6th month). In our area, after 6 months, parents are educated to introduce complementary food in addition to breastmilk for their babies.
Sample
Women were recruited during their prenatal appointments. The study's concept and purpose were explained by a nurse researcher. Only primiparous women aged 18 to 35 years old, with a singleton pregnancy between 32- and 37-weeks of gestation, who wanted to nurse their baby, and were willing to participate in the workshop program, were eligible for the study. Exclusion criteria were as follows: having a chronic illness, having preterm labor or an abnormal fetal screening, having a psychiatric disorder or an anxiety disorder, having any other high-risk complications.
G*Power (Version 3.1.7) software was used to calculate the sample size. Given that the main purpose of the study was to compare the intervention and control groups, the independent sample t- test was used in the power analysis. A 5% type-one error, 80% power, and 20% type-two error were used in the calculation. Küçükoğlu and Çelebioğlu’s (2014) study and Cohen Standard effect sizes were used for effect size. In Küçükoğlu and Çelebioğlu’s study, the breastfeeding self-efficacy mean of the control group was 39.70 (SD = 12.21), while that of the intervention group was 65.8 (SD = 17.37). Accordingly, a difference greater than 0.8 was expected between the two groups. For the difference test between two means, the moderate effect was determined by Cohen as at least 0.50. In the study, a standard effect size of 0.7, which represents a value between these two effect levels, was determined. The reason for this was to take into account smaller differences and to work with a larger sample. The required minimum sample size was calculated as 68 women in total, and 34 women for each group.
Randomization
Permuted block randomization was used to assign eligible participants to the intervention or control groups. Women were randomly assigned to the intervention group or the standard care group in a 1:1 ratio after giving their informed consent. Research Randomizer software (https://www.randomizer.org.) was used to generate a randomized list by applying a simple randomization technique to each participant's assignment. An independent nurse, who was not involved in conducting the study or control conditions at any point, did the allocation (Figure 1).
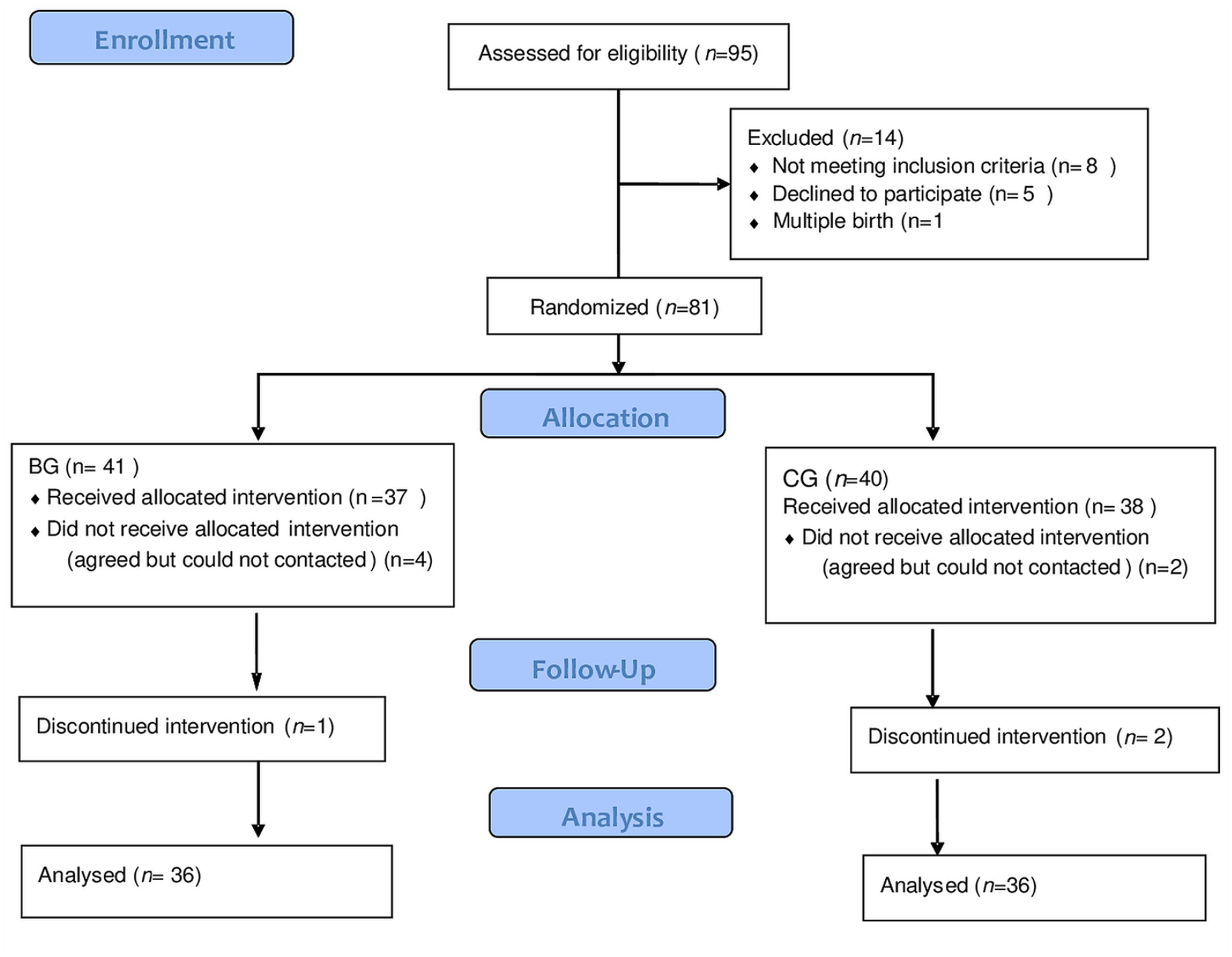
Flow Chart of the Study Sample.
Standard care was given to both groups based on the Baby-Friendly Hospital Intervention Standards. Pamphlets about breastfeeding were given as part of usual prenatal care. Participants who wanted to learn more about pregnancy, breastfeeding, and childbirth attended an antenatal pregnancy school. Within 30 minutes after delivery, the mother and infant were placed together for physical contact and breastfeeding. After receiving postpartum care services, the lactation nurse provided breastfeeding counseling once a day and organized breastfeeding support in line with the needs of each individual participant until discharge. When participants came for a routine check-up, they were evaluated together with their baby, and reported any problems with their breasts and breastfeeding to the family physician during that visit.
Intervention
Breastfeeding Education Program
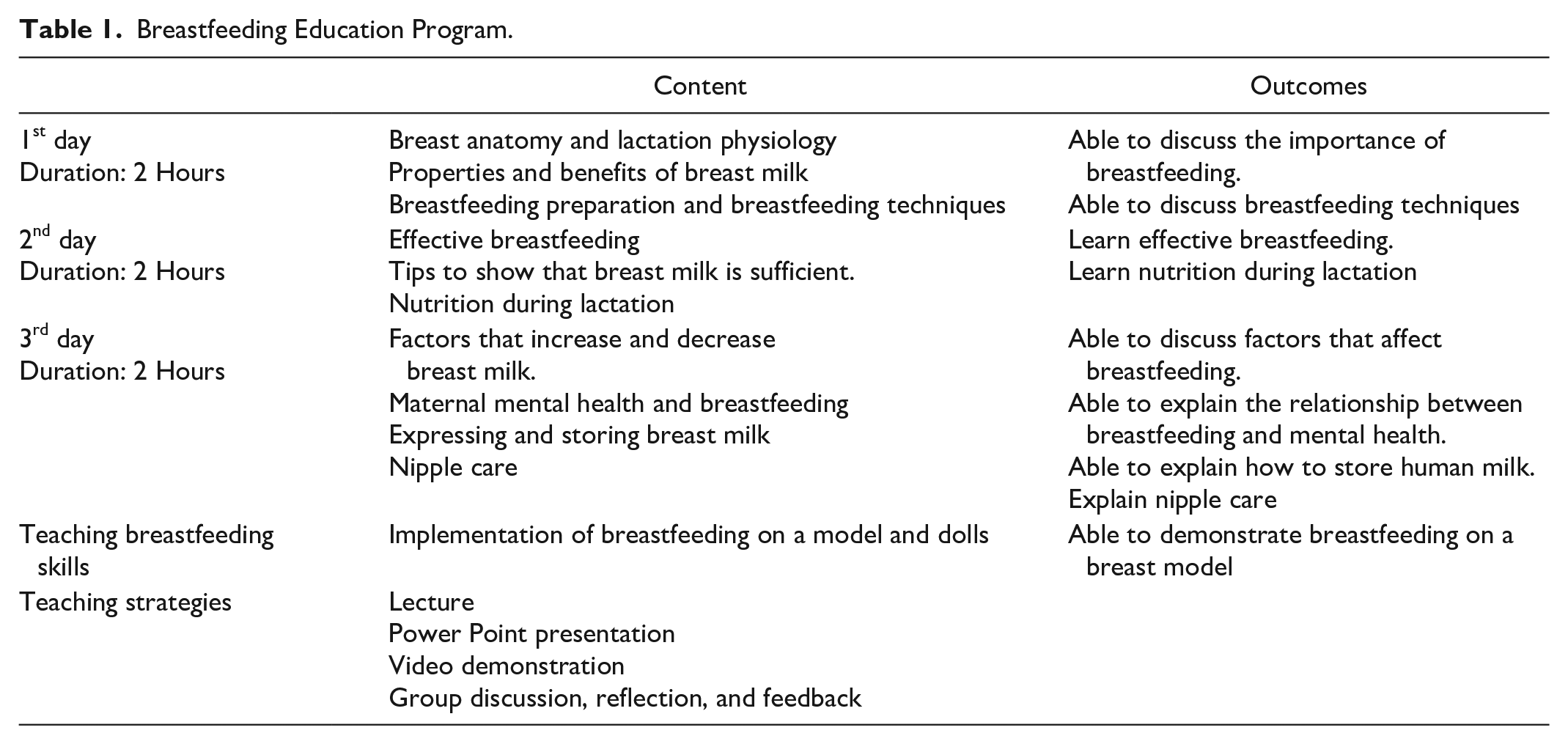
The intervention group participants, in addition to standard care, attended a breastfeeding workshop. Between 32 and 37 weeks of pregnancy, a 2-hour breastfeeding class was offered, with small groups of five women attending each interactive session. The workshop included 2 hours of education on each of 3 days (Table 1).
Breastfeeding Education Program.
In the second stage we developed a web-based online tracking system (BMUM). BMUM is a web-based program that can work with small devices like a laptop, tablet, or smartphone. The system was created using cutting-edge web technology (HTML5, CSS, PHP, and JavaScript). Furthermore, the MySQL database was used to store and manage the data. We employed a responsive user interface to decrease user-interface complications, making it simple to run and interact with, even for those with no previous website expertise.
Participants in the intervention group were contacted through the system via standardized educational emails. During the time of the study sessions, participating mothers were able to access the system as often as they required. The system included many counseling topics: the benefits of breastfeeding, the mechanism of lactation, breastfeeding techniques, breastfeeding problems and their solutions, coping with negative emotions (feelings of loneliness, inadequacy, burnout) during breastfeeding, contraindications to breastfeeding, and human milk storage.
To assess content validity before presentation to the participants, all of the educational topics were evaluated by a national certified lactation consultant (certified by the Istanbul University Faculty of Medicine) as well as three experts in the field of maternal and child health care nursing outside of the study team. Educational components were modified according to their recommendations.
Consultancy on breastfeeding was provided in accordance with a checklist that was created by consensus agreement among the researchers. A Skype link was added to the online system so that participants could remotely show the researchers the problems they were experiencing. The program evaluated participants’ emotional/physiological wellbeing and breastfeeding status during the 6 months of study participation after their baby had been born. If nipple or breastfeeding problems were encountered on Day 1 or in the 1st week after birth, researchers would follow-up with intervention participants. Breastfeeding duration was followed for all participants. In the intervention group, participants expressed their breastfeeding problems online and received emotional support or education on coping strategies. The researchers, whose aim was to provide continuous support, contacted the participants daily through the system or invited them by phone to enter the system. Each day, participants were evaluated and queried about which counseling subjects were of interest. In addition, the women also contacted the chat section at any hour. Urgent issues were answered immediately, and a suitable day and time was determined for more detailed consultation. The women did not communicate with each other.
Participants in the intervention arm who could not cope with their problems were provided with online live support, and if the problem was not resolved, appropriate advice was given when they received their routine checkup. Throughout care and during the study, breastfeeding practices were encouraged. In the 3rd and 6th months, interviews focused on the promotion and continuation of breastfeeding, and any factors that might prevent breastfeeding. For 6 months, participants were supported and encouraged to develop a positive attitude towards breastfeeding, to give only human milk, and not to use complementary food. (Figure 2).
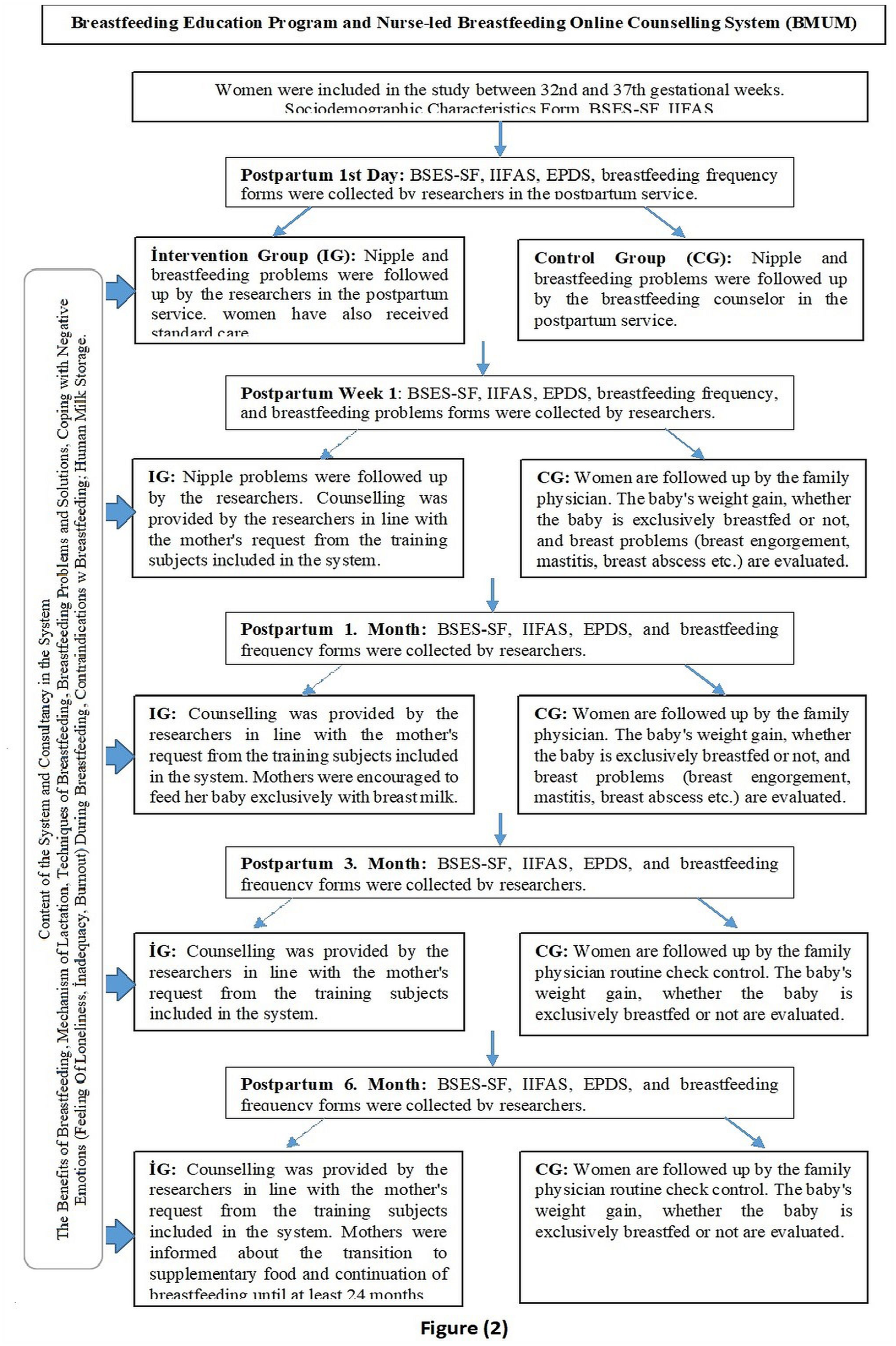
BMUM System.
Data Collection
The study was conducted between September 2020 and April 2022. Demographic data were collected at a single time point, prenatally, between 32 and 37 weeks of gestation. All participants intended to breastfeed, but intended breastfeeding frequency was collected as well as age, education, employment, income level, and gestational week.
Breastfeeding self-efficacy was assessed using the Breastfeeding Self-Efficacy Scale–Short form) created by Dennis (2003) and translated into Turkish by Aluş Tokat et al. (2010). The scale included 14 items. Participants rated their self-efficacy on a 5-point Likert scale for each item ranging from 1 “no confidence” to 5 “extreme confidence.” Total possible scores ranged from 14 to 70, with higher scores indicating greater breastfeeding self-efficacy. The Turkish version of BSES-SF had a Cronbach’s alpha reliability of 0.86; and for this study it was 0.89.
Parents' feeding attitudes were measured using the Iowa Infant Feeding Attitude Scale (IIFAS; Mora et al., 1999). It was adapted into Turkish by Ekşioğlu et al. (2016). Higher scores indicated a more favorable attitude toward newborn feeding. Each of the 17 items was assessed on a 5-point Likert scale from 1 to 5, with 1 indicating “strongly disagree” and 5 indicating “strongly agree.” The Cronbach’s Alpha internal consistency coefficient of the scale was 0.71 and was 0.68 for this study.
The presence and/or risk of depression in the postpartum period was measured using the Edinburgh Postpartum Depression Scale (EPDS), a 10-item self-report scale developed by Cox and Holden in 1987. The total possible score ranges from 0 to 30, with higher scores suggesting a higher level of depression symptoms. The EPDS is scored on a 4-point scale from 0 “no” to 3 “most of the time.” The Turkish validity and reliability study of the EPDS was performed by Engindeniz et al. (1996) and the internal consistency Cronbach’s Alpha value of the scale was found to be 0.79; it was 0.80 for this study.
To measure the presence of breastfeeding problems, the researchers created a form using the related literature (Feenstra et al., 2018) that consisted of 10 closed ended questions and one open-ended question about breast problems experienced. Three experts in obstetric and gynecologic nursing from outside of the study team assessed content validity. Necessary revisions were made, and the form was finalized. It was pilot tested with 10 pregnant women who were not included in the study, and no changes were made. Participants also filled in a diary to record the number of breastfeeding sessions for the previous day. Data collection times for intervention and control groups are shown in Table 2.
Data Collection Tools and Data Collection Times.
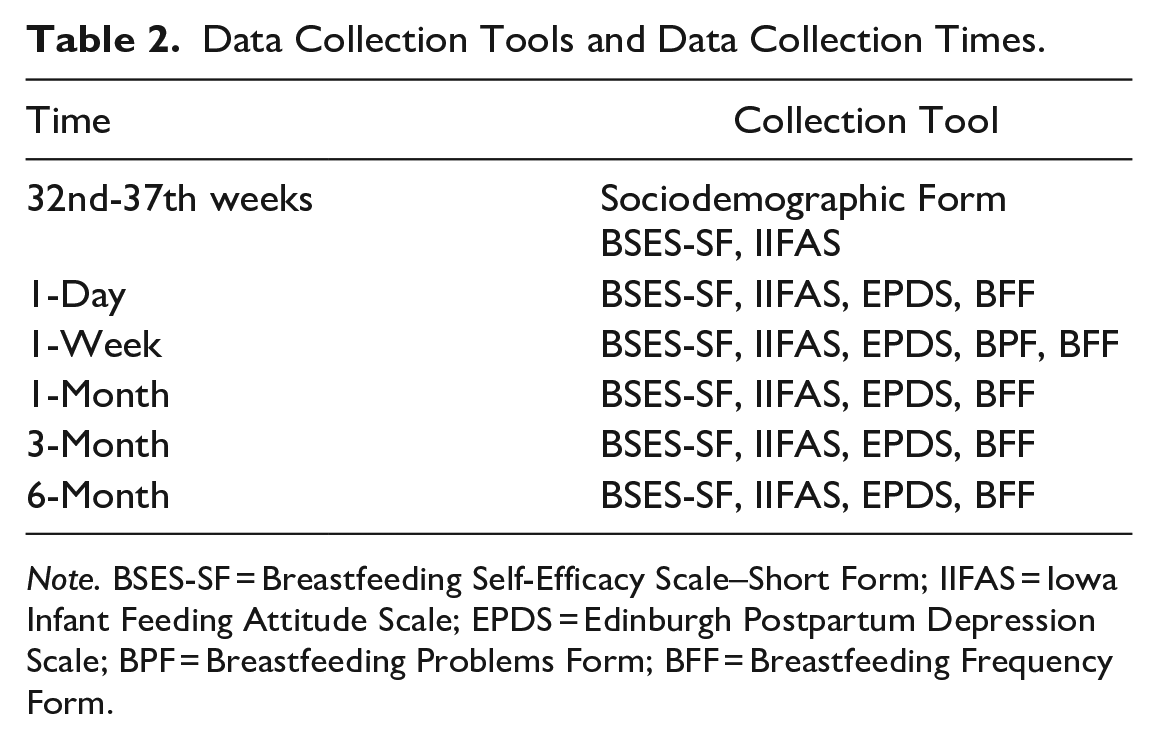
Note. BSES-SF = Breastfeeding Self-Efficacy Scale–Short Form; IIFAS = Iowa Infant Feeding Attitude Scale; EPDS = Edinburgh Postpartum Depression Scale; BPF = Breastfeeding Problems Form; BFF = Breastfeeding Frequency Form.
Data Analysis
Sociodemographic data were summarized as numbers, percentages, and means and standard deviations (SD). The Shapiro-Wilk normality test was used to determine tests for use in further analyses. As the variables in the sample were normally distributed, parametric tests were used for the analyses. For categorical data, differences between groups were compared using chi-square tests. A Fisher’s Exact test was used when variables had cell(s) with an expected frequency < 5 and independent t-tests were used to compare individual variables between the intervention and control groups.
Mixed Model ANOVA was used to asses comparisons between groups’ BSES-SF, IIFAS, and EPDS scores over time. These analyses were performed using SPSS (Version 22.0). For all the analyses, the level of a statistically significant difference was specified as p < 0.05.
Results
Characteristics of the Participants
There were no statistically significant differences in socio-demographic characteristics between the two study groups (Table 3). When the groups were compared, the mean age of the intervention group was 34.02 (SD = 3.95) and the mean age of the control group was 32.86 (SD = 3.28; p = 0.178).
Socio-Demographic Characteristics of Participants (N = 72).
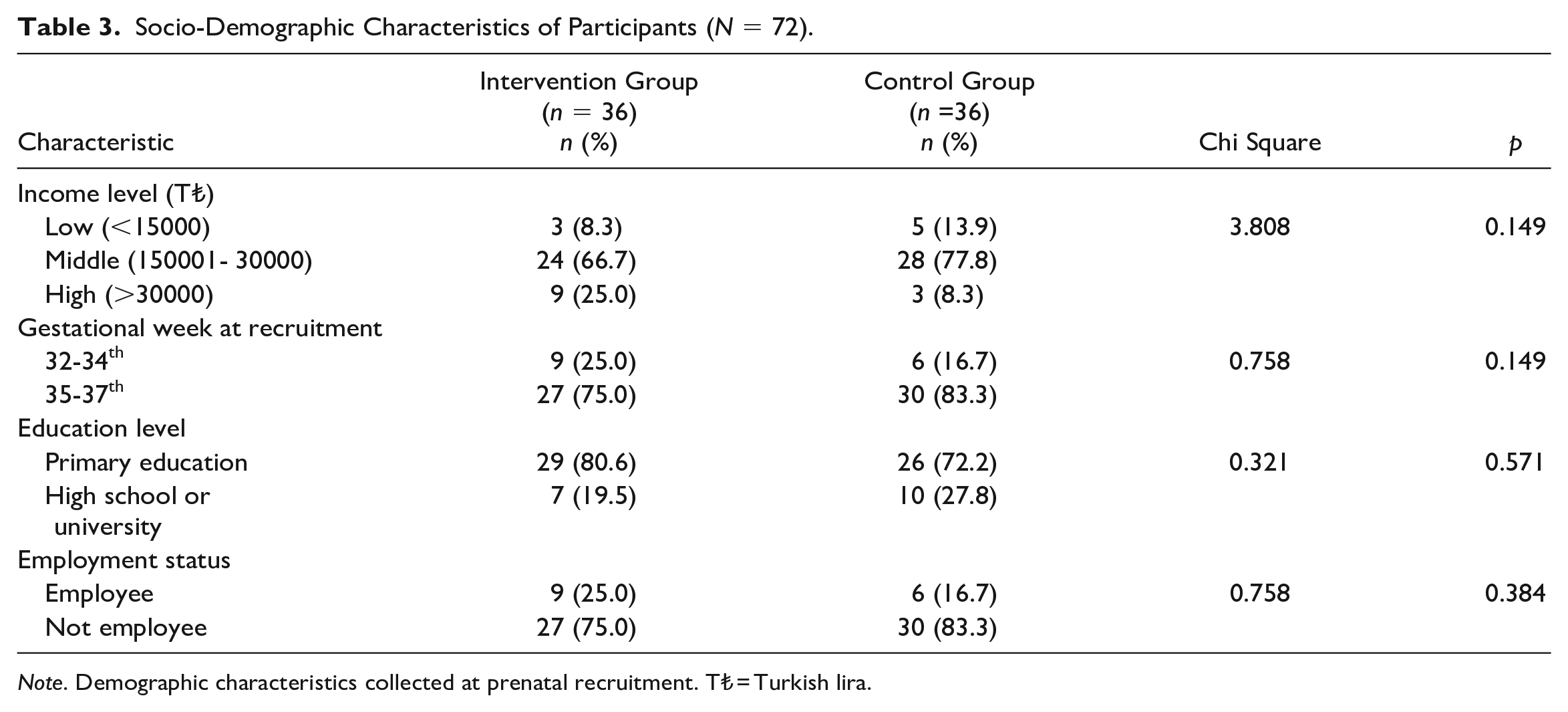
Note. Demographic characteristics collected at prenatal recruitment. T₺ = Turkish lira.
Breastfeeding Self Efficacy and Parent Feeding Attitudes
At baseline (between 32- and 37- weeks of gestation), there was no significant difference in mean BSES-SF or IIFAS scores between the two groups. But the intervention group had higher mean scores at 1 day, 1 week, 3 months, and 6 months, compared to the control group (Table 4).
Comparison of Mean Scores on the Breastfeeding Self-Efficacy Scale–Short Form (BSES-SF), Iowa Infant Feeding Attitude Scale (IIFAS), and Edinburgh Postpartum Depression Scale (EPDS) Over Time for the Intervention and Control Group (N = 72).
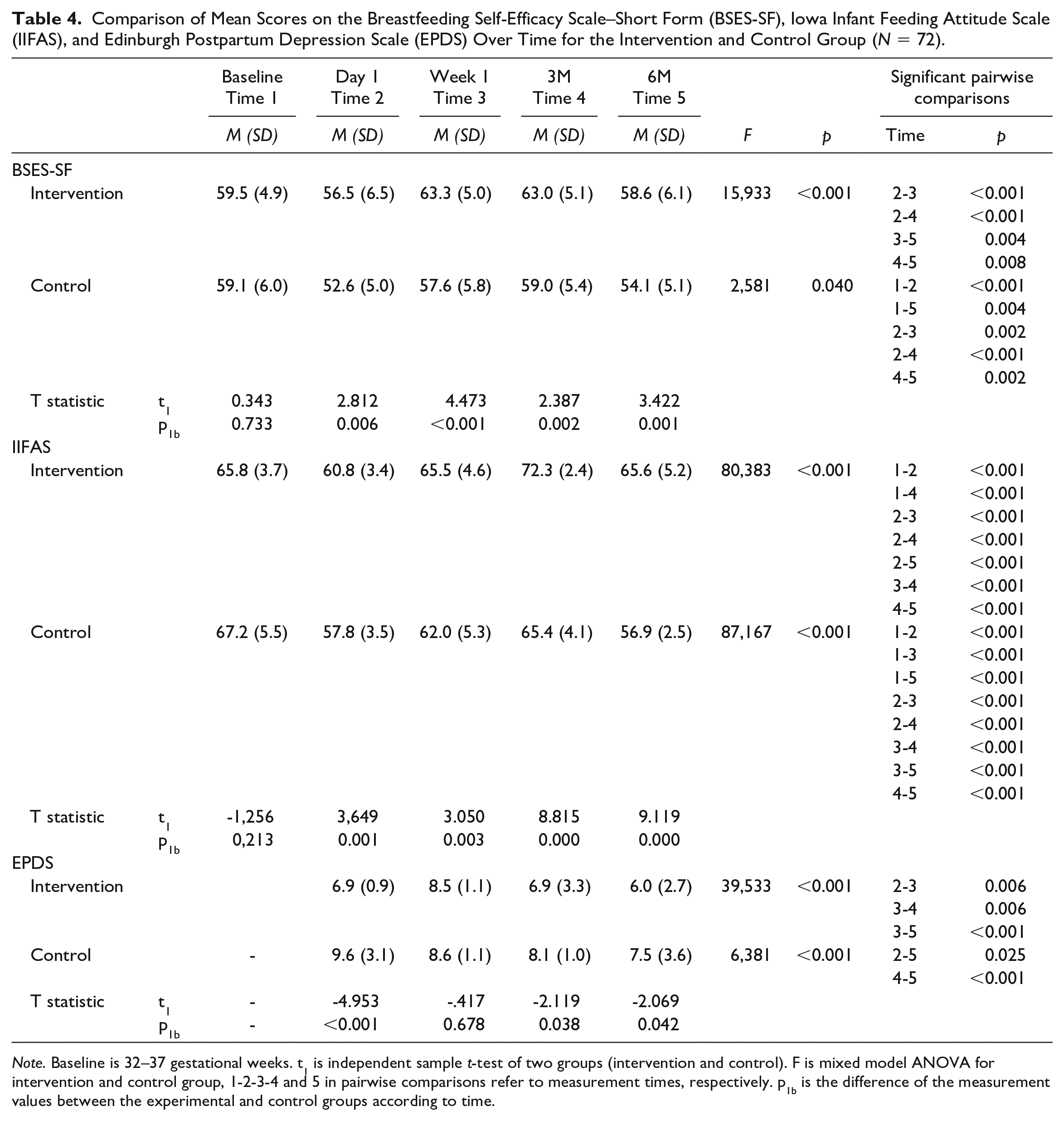
Note. Baseline is 32–37 gestational weeks. t1 is independent sample t-test of two groups (intervention and control). F is mixed model ANOVA for intervention and control group, 1-2-3-4 and 5 in pairwise comparisons refer to measurement times, respectively. p1b is the difference of the measurement values between the experimental and control groups according to time.
Postpartum Depression
Although between group comparisons of EPDS scores did not show a statistically significant difference between the intervention and control group at Week 1, (p = 0.638) EPDS scores in the intervention group were significantly lower on the 1st day and at 3 and 6 months, compared to the control group (Table 4).
Breastfeeding Problems and Frequency
Table 5 shows the number and percentage of each breastfeeding problem in the control and intervention groups. None of breastfeeding problems differed significantly between the control and intervention groups.
Breastfeeding Problems by Group (N = 72).
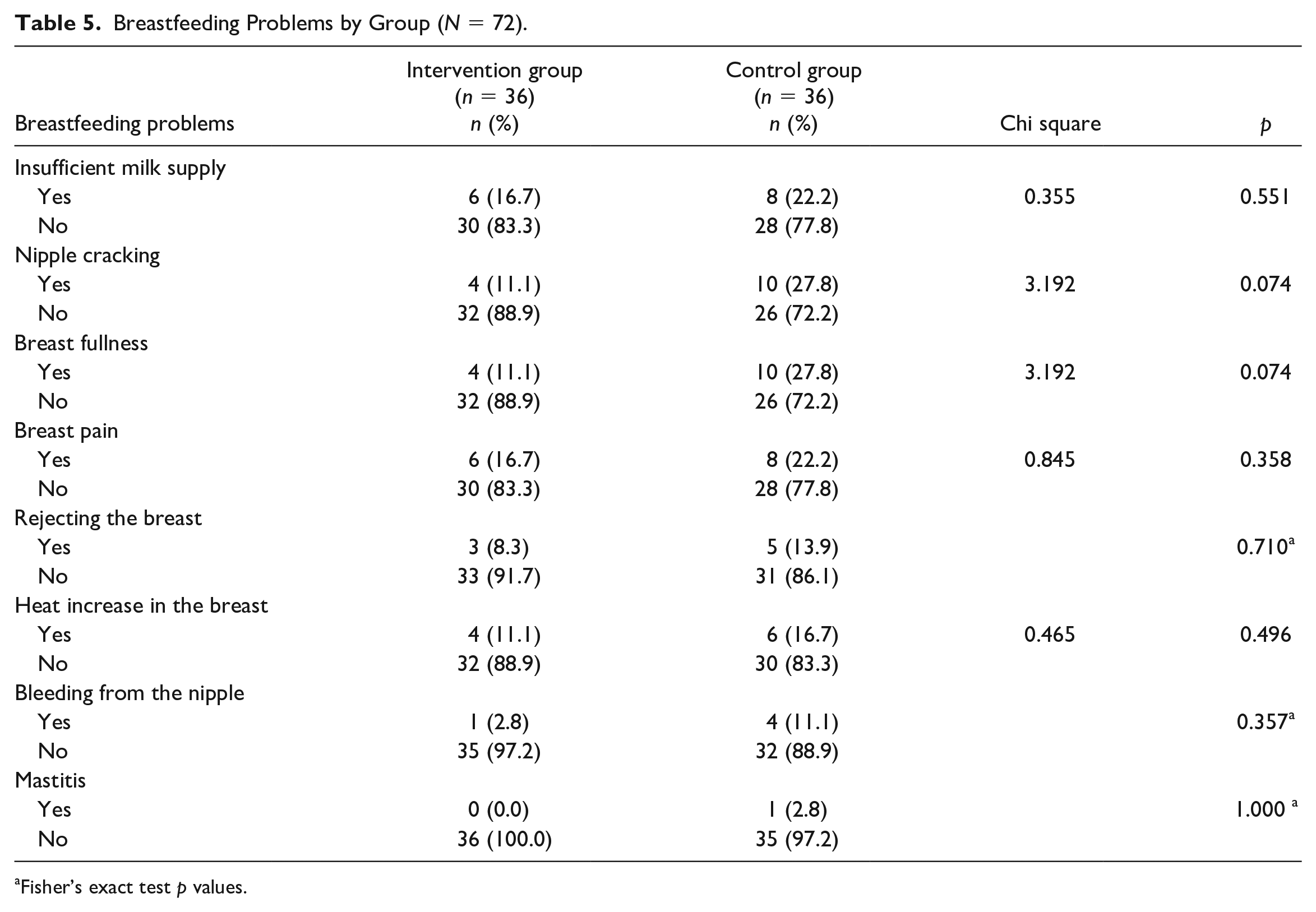
Fisher’s exact test p values.
Table 6 shows the means and SD of breastfeeding frequency in the control and intervention groups at each collection time. The difference on the 1st day was not statistically significant, whereas the difference in all other periods (1st week, 1st month, 3rd, and 6th month) were significantly different. The breastfeeding frequency of the intervention group in all periods was higher than the control group (Table 6).
Breastfeeding Frequencies of Participants in Comparison Group (N = 72).
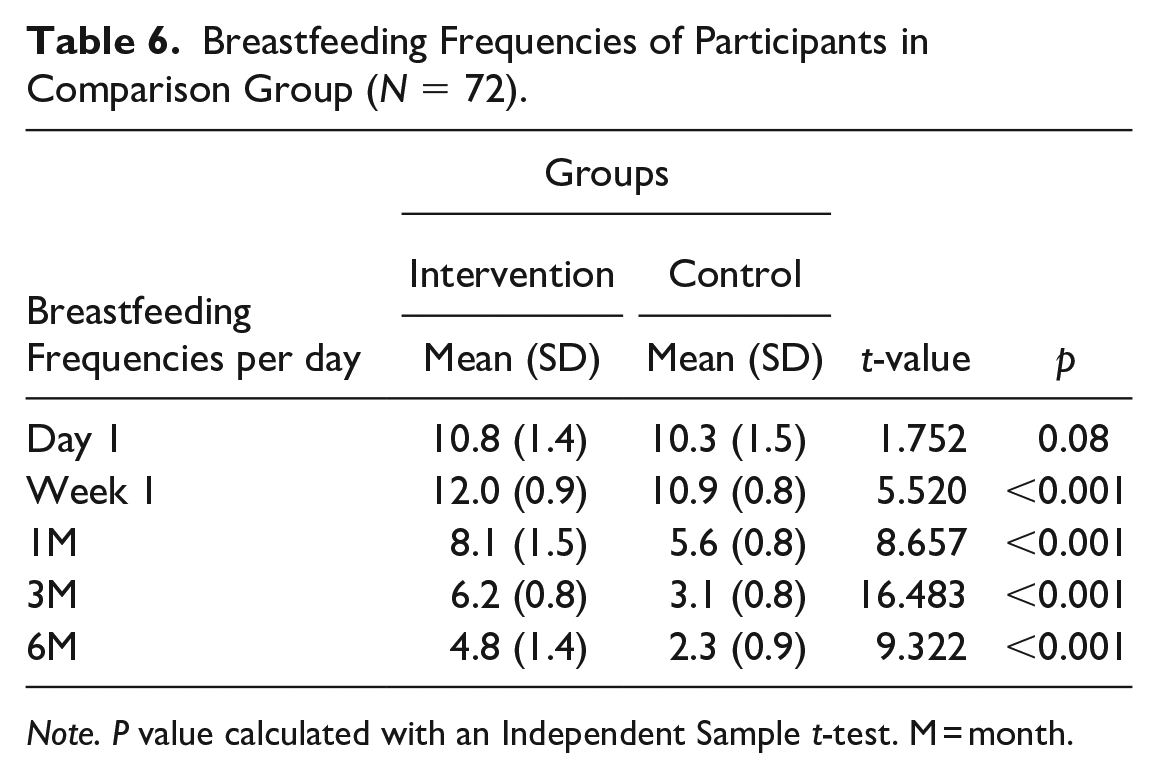
Note. P value calculated with an Independent Sample t-test. M = month.
Discussion
Educational and supportive interventions in primiparous women with no breastfeeding experience are very important in initiating and maintaining breastfeeding and increasing breastfeeding self-efficacy (Wong et al., 2021). In our study, BSES-SF mean scores were similar at baseline between the control group and the intervention group but significantly better at all timepoints tested in the control group after online breastfeeding support. In other studies of breastfeeding education in the postpartum period, breastfeeding self-efficacy levels of participants also increased (Lee et al., 2019; Piro & Ahmed, 2020; Tseng et al., 2020). Similarly, our results indicated a difference in IIFAS scores after baseline, once education had been provided, which is similar to a study by Tseng et al. (2020), whose data also supported that infant feeding attitude scores improved after birth in women who participated in an integrated breastfeeding education program.
Breastfeeding is a cost-effective and healthy behavior and reduces the risk of postpartum depression in women (Toledo et al., 2022). Zhao et al. (2021) found that supportive individualized counseling provided by nurses was effective in reducing the risk of postpartum depression. In our study, there was no significant difference in EPDS mean scores at the 1-week assessment, but the EPDS mean scores on postpartum Day 1, and at 3 and 6 months, were higher in the control group. In our study results, breastfeeding self-efficacy in the intervention group was found to be high, and postpartum depression levels were low similar to other studies (Palancı Ay & Aktaş, 2021; Zubaran & Foresti, 2013)
In one study, Taiwanese postpartum women who stayed at their parents’ home and had their own mothers take care of them experienced less depression. In this study, as the level of postpartum social support received by women increased, the risk of postpartum depressive symptoms decreased (Heh et al., 2004). We hypothesize that providing online follow-up support to the participants in the intervention group facilitated their adaptation to their new lives and enabled them to cope with the process more easily.
Health professionals should develop appropriate interventions for breast problems during breastfeeding to help mothers and their families to continue healthy breastfeeding practices (Huda et al., 2022). Babakazo et al. (2022) found that the most common breastfeeding problems experienced were nipple cracking or soreness, insufficient milk production, and breast engorgement. Researchers have found that effective breastfeeding education positively affects breast pain and breast fullness (Huda et al., 2022; Lucas et al., 2019). Giving women the right information and skills, like how to correctly position and grip the breast, can help them breastfeed their babies properly and enhance their self-confidence, helping them avoid breast engorgement (Tseng et al., 2020). There were no statistically significant differences in any of the breastfeeding problems (e.g., insufficient milk supply, nipple cracking, breast fullness, breast pain, rejecting the breast, or heat increase in the breast) between the experimental and control groups. This would suggest that the development of correct breastfeeding behavior developed over time rather than due to the intervention provided. This result is important as it indicates that the nurses/researchers were helpful emotionally, but not with the physical improvement in breastfeeding practices.
In the 1st month after birth, the typical frequency of breastfeeding is eight to 12 times in 24 hours, and the duration of breastfeeding is generally 20–45 minutes (Niazi et al., 2019). In our study, no statistically significant difference was found in the breastfeeding frequency of the women in the intervention and control group on the 1st day. However, the frequency of breastfeeding at the other four follow-up times was statistically significantly higher in the intervention group. Aylyyewa and Topatan (2022), as with our study results, found that education and counseling integrated into the existing health system are effective in increasing the frequency of breastfeeding and breastfeeding behaviors of primiparous mothers in the first 6 months after birth.
Limitations
This study has some limitations. The results were based on the women’s self-reporting. Providing continuous support to the intervention group could have caused the Hawthorne effect. The total duration of interaction per women in intervention group was not measured. The study did not follow the control group for the same amount of time as the intervention group. Researchers did not have any indication whether or not participants in the control group received breastfeeding classes or specialized support during the study. Researchers also did not have information on the content and duration of the breastfeeding education given to the participants in the control group and how the education was evaluated, so it is unclear how the education provided in the study was different between the participants in the different arms of the study. Although participants’ problems were followed up by the researchers, we do not have data on how often they sought treatment for their problems.
Conclusion
A breastfeeding workshop and supportive counseling with online follow-up may help in promoting improvements in breastfeeding self-efficacy and attitude toward infant feeding, decreased postpartum depression, and increased frequency of breastfeeding. The program was not found to be effective in decreasing breastfeeding problems. This system can be recommended for clinical use as it is easy to use and provides continuous support. However, further randomized controlled trials are needed to validate the findings of this study.
Footnotes
Author Contributions
Disclosures and Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.