
Abstract
Introduction:
Human lactation should be taken into account as an important issue for the international agenda. Despite advances in lactation information and knowledge, insufficient milk production is still a concern for mothers and health practitioners, including International Board Certified Lactation Consultants and others. Primary hypogalactia, or insufficient milk production is uncommon, but should be considered when there is poor weight gain and decreased urine output in infants despite good latch-on and suckling, or anatomic differences in the physical exam of the lactating breast.
Main Issue:
This case series presents three cases illustrating insufficient milk production resulting in infants who experienced significant dehydration and poor weight gain.
Management:
Primary hypoplasia was diagnosed by means of a thorough interview and physical examination that entailed a consultation with a physician who was also an International Board Certified Lactation Consultant.
Conclusion:
Awareness of an infant’s feeding needs and proper evaluation of a child’s health status is paramount if health care providers are to identify the important factors contributing to breastfeeding problems. In some instances, breastfeeding goals cannot be achieved, and then the provider’s role becomes support in coming to terms with persistent insufficient milk production, and coordinating appropriate supplementation to meet each baby’s nutritional needs.
Keywords
Introduction
Human milk is the ideal food for infants. The World Health Organization (WHO, 2017), recommends that children initiate breastfeeding within the 1st hour of life, that they are exclusively breastfed for the first 6 months of life, and continue to be breastfed, along with other foods, beginning at 6 months and for up to 2 years and beyond. Human milk provides the nutrients needed by the infant. In addition to antibodies that help reduce the risk of infectious diseases, human milk reduces the likelihood of obesity and Type 2 diabetes later in life, and supports sensory, motor, cognitive, and affective development in general (Meek et al., 2022).
Despite recommendations from the WHO, the United States Centers for Disease Control and Prevention (U.S. CDC, 2022), the American Academy of Pediatrics (AAP), and the Mexican Ministry of Health (SSA), exclusive breastfeeding in Mexico remains below 30% nationwide (González-Castell et al., 2020). Insufficient milk production is the most common reason for premature cessation of breastfeeding (Ericson & Palmér, 2020). Insufficient milk production, or hypogalactia, can be temporary or permanent and may be associated with maternal or infant issues, or lactation management. Milk production relies on three primary components: effective infant suckling, the capacity of the breast in terms of milk production, and milk ejection or let-down reflex (Gardner et al., 2019).
Breast hypoplasia, hormonal irregularities, or breast surgery (e.g. breast reduction) are primary reasons for hypogalactia—the physical inability to develop the milk production required for adequate infant growth (Galipeau et al., 2017). Breast hypoplasia can present with characteristics that include widely separated, tubular, or asymmetrical breasts (Grella et al., 2022). The risk of hypoplasia and hypogalactia is higher when women do not show breast changes during pregnancy. Women with mammary hypoplasia can have normal hormonal levels and innervation, but, in cases where the relationship with hypogalactia is established, may have glandular tissue insufficient for achieving adequate milk production. Some authors consider hypoplasia as a primary cause of failed Lactogenesis II (Arbour & Kessler, 2013).
Normal functional lactation requires an interaction of reproductive and metabolic hormones which stimulates milk duct development during pregnancy and secretory activation postpartum (Pillay & Davis, 2021). The production of milk is divided into three stages: Lactogenesis I (15–20 weeks of gestation); Lactogenesis II (48–72 hours after the delivery of the placenta); and Lactogenesis III, (galactopoesis; Mullen et al., 2022). Hypogalactia is a complex clinical healthcare problem that requires medical and social care. The diagnosis of this condition during lactation management is becoming more frequent worldwide, which suggests a need to know the risk factors and the best strategies for timely identification (Gromnatska et al., 2022).
Since a reduction in milk production can lead to undesirable sequelae in the infant (e.g., dehydration, electrolyte abnormalities, and poor weight gain), assessing for breastfeeding problems is an essential part of newborn care (Nakstad et al., 2022). In cases of insufficient milk production, the breastfeeding dyad needs to be examined to establish contributors which could be anatomical, structural, hormonal, functional, or psychological.
In Mexico, the regulated processes of caring for the pregnant patient (Norma Oficial Mexicana NOM-007-SSA2-2016 and Norma Oficial Mexicana PROY-NOM-050-SSA2-2018) state that a physical exam, including breast examination, should be carried out by health personnel in the first prenatal care consultation (de la Federación, 2016). During this consultation, information on the benefits of breastfeeding and the risks of using human milk substitutes is recommended, along with the development of skills for breastfeeding (de la Federación, 2018).
There are very few articles in the literature on the identification of primary hypogalactia prenatally or postpartum, or management of identified cases. The women discussed in the cases presented here have given written consent for the publication of their cases, and have read and approved of the submitted manuscript.
History and Observational Assessment
We present a case series of three mothers whose infants suffered significant dehydration and poor weight gain in the latter half of 2018 in Jalisco, Mexico. We describe each dyad’s feeding practices and difficulties. Primary hypoplasia was diagnosed by means of a thorough interview and physical examination in consultation with an International Board Certified Lactation Consultant who was also a physician. The referral for clinical care specifically for this complication came either through their medical and family support network, or because of the information obtained during prenatal education.
Each participant completed a survey for information on the social, psychological, emotional, and family factors of their case. We additionally reported previous medical history, course of pregnancy, type of birth, medical history of the baby, information on suckling, anatomical examination of the breast, and lactation management. The main factors evaluated in the cases are shown in Table 1.
Characteristics of the Case Series, History of Breastfeeding, and Alterations of the Mother and the Infant.
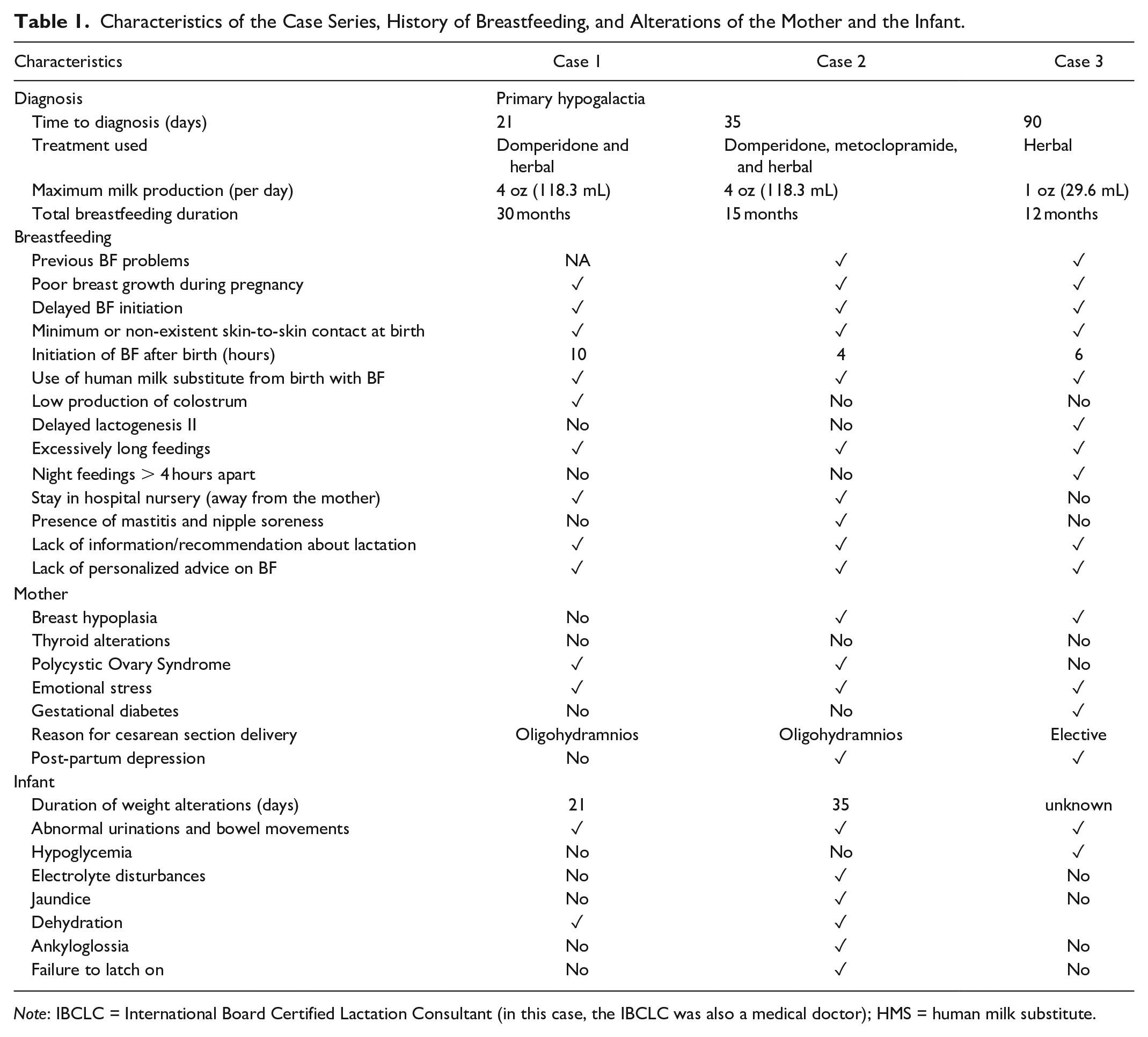
Note: IBCLC = International Board Certified Lactation Consultant (in this case, the IBCLC was also a medical doctor); HMS = human milk substitute.
Case 1
The first case we present was a 36-year-old primiparous mother who was also a nutritionist. Her history was significant for having been diagnosed with transient hyperthyroidism before pregnancy, for which she received treatment for a year, with adequate control. She had also been treated for an ovarian cyst and underwent cervical conization for papilloma. During her pregnancy she experienced fatigue and emotional stress. Her first sonogram revealed a retroplacental hematoma that required bed rest. She gave birth to a healthy boy at 41 weeks who weighed 3,350 g and had an Apgar score of 9 at 1 and 5 min. He was born via Cesarean section due to oligohydramnios and prolonged labor. After the delivery, there was no delay in umbilical cord clamping, and there was no skin-to-skin contact. First contact with the baby for skin-to-skin contact and breast stimulation was 10 hours after birth. During hospitalization the baby was nursed and bottle fed with a human milk substitute (HMS). After discharge, the case participant attempted exclusive breastfeeding. She reported barriers to breastfeeding including low family support and lack of information from health personnel in the hospital. At 2 weeks of age, her son had not regained his birth weight (gaining only 100 g in 3 weeks), urination and bowel movements were scarce (less than four diapers per day), and the feedings were excessively long (up to 3 hours).
Case 2
The second case we present was a 32-year-old mother of two children, who was also a nutritionist. She had a previous history of being diagnosed with polycystic ovarian syndrome (PCOS). Her PCOS was accompanied by irregular menstrual periods, and therefore was treated with contraceptives. She had a family history of thyroid problems, but her thyroid tests were normal before and during pregnancy. She had a history of insufficient milk production with her previous baby, which was managed with partial breastfeeding from the beginning using HMS. During the current pregnancy she experienced emotional stress and fatigue but her pregnancy had no medical complications. She delivered a healthy boy at 38 weeks weighing 3,185 g. His Apgar score was 9 at 1 and 5 min. He was born by Cesarean section due to oligohydramnios. After the delivery, there was no delay in umbilical cord clamping and the skin-to-skin contact lasted a few minutes. The baby stayed in the hospital nursery for the first 4 hours after delivery and for 2 nights, and was bottle fed with HMS. Metabolic, hearing, and cardiac screenings were within normal ranges. The case participant had little family or social support for breastfeeding, and had symptoms of postpartum depression in the first weeks. She was treated with sertraline until 8 months postpartum. Her depression was compounded by her difficulty with breastfeeding. The baby was diagnosed with ankyloglossia and was treated with a frenotomy at 1 month of age, but feeding difficulties persisted, resulting in poor weight gain and jaundice.
Case 3
The third case we present was a 28-year-old multiparous mother who had a history of difficulty feeding her previous baby. During this pregnancy she was diagnosed with gestational diabetes and was treated with dietary modifications. She delivered a healthy boy at 37.5 weeks, who weighed 2,700 g. His Apgar score was 8 at 1 and 5 min. He was born via Cesarean section. After the delivery, there was no delay in umbilical cord clamping, and no skin-to-skin contact. The first contact with the baby was 6 hours after birth. During that time, the baby was in the hospital nursery and was bottle fed with HMS. After that, skin-to-skin contact was established along with rooming-in. When she was discharged, she attempted exclusive breastfeeding. She had good family and social support for breastfeeding. She reported long feedings greater than 4 hours apart during nighttime hours. Urination and bowel movements were scarce (less than four diapers per day) and the baby showed symptoms of hypoglycemia.
Management
Case 1
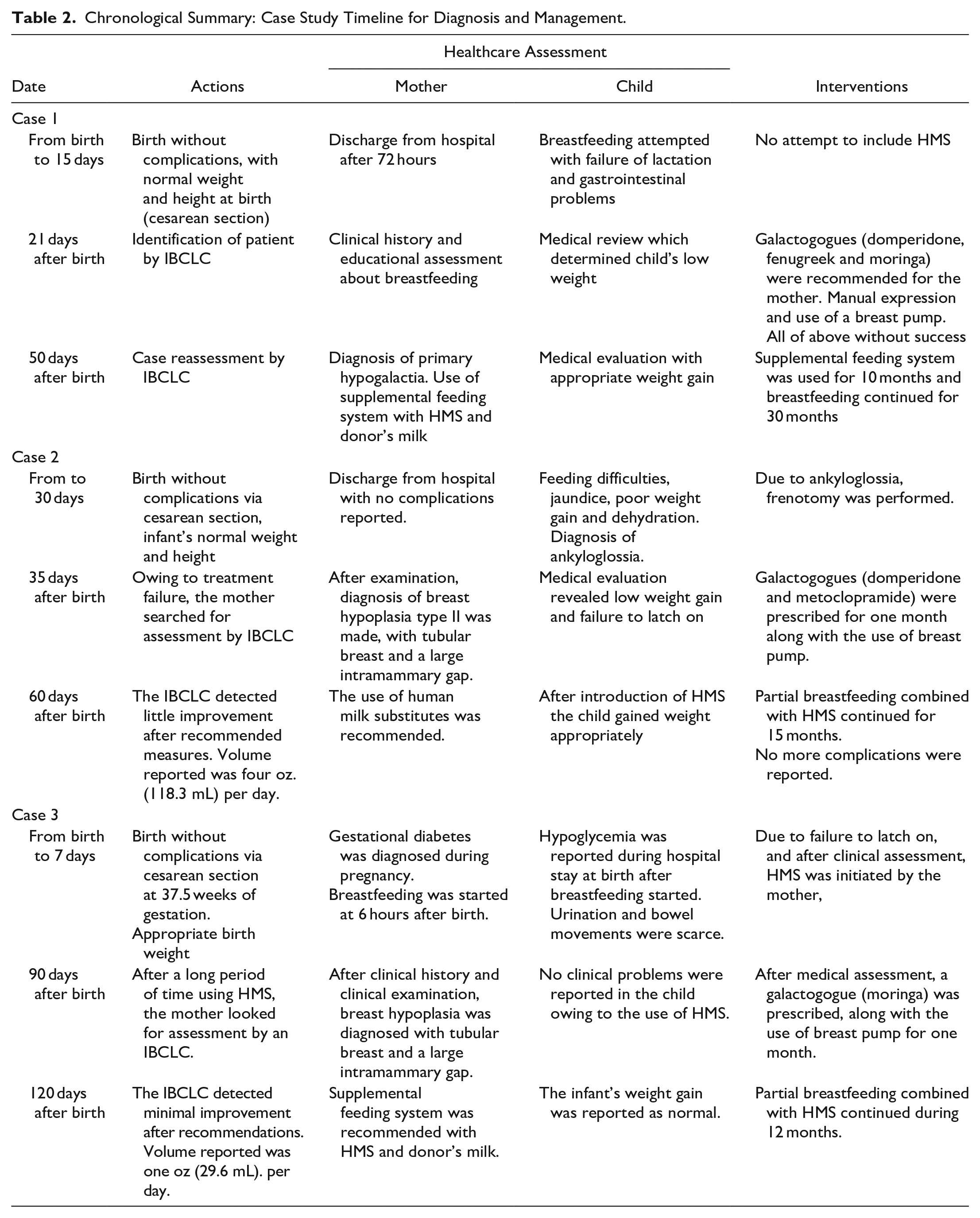
At 3 weeks postpartum, the case participant consulted an MD International Board Certified Lactation Consultant (IBCLC) who determined that the infant was properly positioned during breastfeeding and the latch was appropriate. She started galactogogues (domperidone 20 mg every 8 hours for 1 month (Lawrence & Lawrence, 2021), fenugreek, and moringa) and milk expression both manually and with a non-electric breast pump. Since milk production did not increase with these techniques, she was diagnosed with primary hypogalactia, and consequently proceeded to use a supplemental feeding system with HMS and donor milk for 10 months. Almost 80% of the baby’s intake was with human milk, consisting of both mother’s own milk and donor milk. Breastfeeding continued for 30 months with appropriate weight gain. At 4 years of age he was very healthy (Table 2).
Chronological Summary: Case Study Timeline for Diagnosis and Management.
Case 2
At 35 days postpartum, the case participant consulted an MD IBCLC, and an examination revealed breast hypoplasia Type II with tubular breasts and a large intermammary gap. The participant experienced the feedings as being excessively long, and the infant’s urination and bowel movements were scarce. During evaluation, the infant was unable to latch effectively to the breast and mastitis was identified. The case participant was diagnosed with primary hypogalactia, and pumping was recommended using a breast pump. She started galactogogues (domperidone 20 mg every 8 hours) for 1 month. There was little improvement with this treatment, with a maximum volume production of 4 oz (118.3 mL) per day. The case participant recognized the need to use HMS to prevent complications in the baby, so she continued partial breastfeeding with a HMS for 15 months. The baby gained weight appropriately and at 4 years old was healthy (Table 2).
Case 3
The baby had received HMS since the 1st week due to an inability to latch to the breast. The participant consulted an IBCLC at 3 months postpartum, and the examination revealed breast hypoplasia. The participant had not experienced any engorgement during pregnancy or during the lactation period. Her breasts were tubular and had a large intermammary gap. She also reported low production of colostrum and a delay in Lactogenesis II. She started taking galactogogues (moringa) and to express milk manually and with a breast pump. There was little improvement with this treatment, with a maximum production volume of 1 oz (29.6 mL) per day. She used a supplemental feeding system with HMS and donor milk for 12 months. The infant’s weight gain was normal (Table 2).
Outcome
The first case participant had emotional stress during pregnancy and postpartum. As a primiparous mother, she would likely have benefited from greater vigilance and information about breastfeeding. She had a late onset of lactation, early stimulation of the breast was not initiated, production of colostrum or milk was not evaluated early in her postpartum period, and she reported no education about what excessively long feedings or scarce urination and stools could mean. This had serious repercussions on the baby’s growth and resulted in poor weight gain which was not identified until the 3rd week of life.
Emotional and stress related difficulties were identified and treated in Case 2, but the primary issue lay in the undiagnosed breast hypoplasia that could have been identified as early as the first pregnancy. The baby had little weight gain in the 1st month after birth, a condition that led to an alteration of blood parameters, jaundice, and dehydration. The MD IBCLC in the postpartum period with her second child was the first healthcare provider who identified the anatomical condition of the breast, which was the problem underlying low production of milk and the resultant slow infant weight gain.
There were two reasons that the participant in Case 3 supplemented with HMS: delayed Lactogenesis II and primary glandular insufficiency. Less than 5% of breastfeeding people experience complete or almost complete failure of lactation, presenting real insufficient milk supply (RIMS; Sultana et al., 2013). In this case, the shape of the breasts, poor breast growth during pregnancy, minimal evidence of secretory activation, and delayed lactogenesis (more than 5 days) were all indicators of this condition. In addition, the baby had little weight gain in the 1st month compared to his birth weight.
In all three cases there was complete adherence to, and tolerance of, the management regime proposed by the IBCLC. In both the second and third cases, it is clear that including lactation as a part of the medical history as well as performing a breast assessment during prenatal visits could have been decisive in identifying the anatomical alteration that put both participants at risk for insufficient milk production. Early identification could have additionally reduced risks to the baby's health.
These cases illustrate the complications that can occur when participants do not receive optimal support for breastfeeding and a prompt diagnosis of hypoplasia. It is possible they might have had better results in increasing milk production and improving their breastfeeding experiences had the diagnoses been applied earlier. Since milk production is multifactorial (Table 1), timely and specific support produces better results for both the case participant and the infant.
Discussion
Clinical evaluation can be considered the cornerstone in identifying rare conditions such as hypogalactia. Early prenatal care is recognized as a critical time to initiate an open dialogue about breastfeeding. The American College of Obstetricians and Gynecologists (ACOG), in its opinion for the delivery of prenatal breastfeeding education, recommends that lactation support begins at the first prenatal appointment and is reinforced and expanded in subsequent visits (ACOG Committee on Health Care for Underserved Women & Committee on Obstetric Practice, 2007).
IBCLCs play a positive role in supporting breastfeeding and are associated with increased rates and duration of breastfeeding (Haase et al., 2019). However, in Mexico there are only 117 IBCLCs. Jalisco, the state in Mexico where this study took place, has only 14 (ACCLAM, Directory, 2023). Additionally, there is no mention of this medical specialty in national infant feeding projects (Norma Oficial Mexicana PROY-NOM-050-SSA2-2018; de la Federación, 2018).
There is a clear need to implement new strategies that improve the processes of prenatal care and lactation in Mexico. Standards of prenatal care (de la Federación, 2016) recommend the completion of an early clinical history and complete physical examination, including the breasts, yet this is not consistently implemented in practice. Human lactation education programs for health care providers should emphasize the importance and impact of conditions that may increase the risks for difficulties with breastfeeding.
Human milk and breastfeeding should be the first option for newborns. The right conditions to best support successful exclusive breastfeeding can be facilitated by health professionals to enable proper growth and development and maintain the optimal health of the infant. Early identification of hypogalactia, appropriate information, and effective use of techniques to manage or treat the condition can support sustained production for long periods of time. Appropriate treatment can also reduce postpartum stress related to difficult breastfeeding, which, in turn, improves the health status in the breastfeeding dyad. Implementation of specific protocols and strategies for women with mammary gland hypoplasia are needed to provide adequate and efficient lactation care.
The present study reports only three cases in a country with almost 60 million women, of whom 24% are within their reproductive years. Particularly in developing countries, healthcare might not have efficient systems for screening and follow-up. Our goal is to draw attention to the need for human lactation to be a part of public policy and to underscore the assessment and treatment skills of the IBCLC for conditions such as hypogalactia.
Footnotes
Author Contributions
Disclosures and Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.