
Abstract
Background
Mother’s milk improves outcomes. Referral neonatal intensive care units face unique lactation challenges with maternal–infant separation and maternal pump dependency. Little is known about lactation resource allocation in this high-risk population.
Research Aims
To determine differences in human milk outcomes, (1) the proportion of infants fed exclusive or any mother’s milk and (2) recorded number and volume of pumped mothers’ milk bottles, between two models of lactation care in a referral neonatal intensive care unit.
Methods
This retrospective, longitudinal, two-group comparison study utilized medical record individual feeding data for infants admitted at ≤ Day 7 of age and milk room storage records from reactive and proactive care model time periods (April, 2017–March, 2018; May, 2018–April, 2019). The reactive care model (n = 509 infants, 58% male, median birth weight and gestational age of 37 weeks,) involved International Board Certified Lactation Consultant referral for identified lactation problems; whereas, the proactive model (n = 472 infants, 56% male, median birth weight and gestational age 37 weeks) increased International Board Certified Lactation Consultant staffing, who then saw all admissions. Comparisons were performed using chi square, Mann Whitney, and t-tests.
Results
A proactive lactation approach was associated with an increase in the receipt of any mother’s milk from 74.3% to 80.2% (p = .03) among participants in the proactive model group. Additionally, their milk room mean monthly bottle storage increased from 5153 (SD 788) to 6620 (SD 1314) bottles (p < .01).
Conclusions
In this retrospective study at a tertiary referral neonatal intensive care unit, significant improvement inhuman milk outcomes suggests that increased resources for proactive lactation care may improve mother’s milk provision for a high-risk population.
Keywords
Background
Human milk, specifically milk from an infant’s own mother (mothers’ own milk [MOM]), improves short- and long-term outcomes for all infants, leading to recommendations by the World Health Organization (2018) and the American Academy of Pediatrics Section on Breastfeeding (2012) that infants be fed exclusive MOM until 6 months of age. MOM has particular benefits for infants born preterm, and likely also improves outcomes for other infants who require admission to the neonatal intensive care unit (NICU), including those requiring neonatal surgery for congenital gastrointestinal anomalies (Hoban et al., 2020; Meier et al., 2017; Miller et al., 2018; Vohr et al., 2007). Although mothers of ill infants admitted to a NICU ideally would provide MOM during the NICU hospitalization and beyond discharge, pump dependency for lactation initiation and maintenance, maternal-infant separation, and other risk factors including preterm birth, and the associated maternal health conditions like pre-eclampsia, can affect MOM volumes and therefore continued MOM provision (Hoban et al., 2015; Medina Poeliniz et al., 2020; Meier et al., 2016; Parker et al., 2015).
Previously researchers have shown that the primary predictor of MOM receipt at the time of NICU discharge was mother’s achievement of coming to volume (≥ 500mL of pumped MOM daily by postpartum Day 14), as well as meeting earlier threshold pumped MOM volumes, suggesting the urgency of timely pumping and lactation support in the critical early postpartum period (Hill & Aldag, 2005; Hoban et al., 2018; Murase et al., 2014). Initiating pumping in the first hours postpartum and maintaining frequent pumping, even prior to any obvious milk output, does not just stimulate the breast to make milk, but programs the breast for long-term lactation and correlates to long-term lactation success (Meier et al., 2016; Parker et al., 2015). However, most mothers require education and support to encourage timely and frequent pump use, especially when they prenatally had not anticipated being pump dependent.
Although the majority of lactation support literature focuses on improving breastfeeding in the healthy, term population, multiple authors have shown that utilizing International Board Certified Lactation Consultants (IBCLCs) in the NICU increases breastfeeding rates and short-term MOM availability for vulnerable infants (Castrucci et al., 2007; Gharib et al., 2018; Mercado et al., 2019a, 2019Mercado et al., 2019b). Although the presence of IBCLCs appears to improve lactation outcomes in “inborn” NICUs associated with obstetrical services, little has been reported about IBCLC consultation models, specifically timing and scope (all patients, only high-risk patients, only patients with identified problems like low MOM volumes, etc.) and how this may correlate with lactation outcomes. In addition, there is minimal literature specific to “outborn” referral NICUs which, unlike the mostly preterm population seen in inborn NICUs, typically serve a population of high-risk infants of various gestational ages with complex medical needs who are transferred away from their birth hospital and mother (Dweck et al., 2008; Gonzalez et al., 2003; Leeman et al., 2019). The aim of our study was to determine differences in human milk outcomes, (1) the proportion of infants fed exclusive or any mother’s milk and (2) recorded number and volume of pumped mothers’ milk bottles, between two models of lactation care in a referral neonatal intensive care unit.
Method
Research Design
This single center, retrospective, longitudinal, two-group comparison study utilized prospectively collected data from the hospital’s electronic medical record (EMR) system to retrospectively measure feeding outcomes following a clinical practice change that had already occurred. In this two-group comparison study, reactive and proactive care model time periods were examined. The study was approved by the Sick Kids Hospital Research Ethics Board, and all data were de-identified.
Setting and Relevant Context
This study was conducted in a 36-bed urban level III/IV referral NICU in a freestanding children’s hospital in Toronto, Ontario, Canada. It serves and supports a very culturally and socioeconomically diverse population, with nearly 50% of the city foreign born and/or a visible minority (Statistics Canada, 2017). This children’s hospital serves a large geographic catchment that includes urban Toronto as well as rural Ontario. Over 91% of new mothers in Ontario initiate lactation, and rates of exclusive breastfeeding for at least 6 months are 33% for mothers less than 35 years old and 42% for those 35 years and older (Statistics Canada, 2018). Free government-sponsored lactation support in-person, as well as via phone, from nurses and IBCLCs is available to all mothers in Ontario in over 300 languages, as nearly half of Toronto residents do not speak English or French as a first language (Statistics Canada, 2017).
Key Messages
Referral neonatal intensive care units face unique lactation challenges, but little is known about lactation resource allocation in this high-risk population.
A proactive approach to lactation care within the neonatal intensive care unit by an International Board Certified Lactation Consultant, who saw all new admissions, was associated with significant increases in the percentage of infants receiving mother’s own milk.
All mothers of infants admitted to a neonatal intensive care unit should be considered high risk for lactation challenges, even without other recognized concerns.
The NICU is comprised of open bays with six bed spaces per room; parents can visit any time, but overnight accommodation is not typically available. The vast majority of admissions are for complex preterm and term neonates with subspecialty care requirements, particularly those requiring neonatal surgery or neurological evaluation. As the NICU is in a children’s hospital, there is no labor and delivery service or inborn patients; all are born elsewhere and transported for admission.
Sample
As a referral NICU, some infants are admitted weeks to months after birth, so early admissions, in which lactation outcomes are still very modifiable with support, were our focus. Using a convenience sample, all infants admitted to the NICU during the first 7 days of age who had recorded feeding data were included. Data from two 12-month time periods surrounding a practice change in April 2019 were compared: April 2017–March 2018 and May 2018–April 2019; power analysis and sample size calculations were not performed in this retrospective study as the data were defined by the timing of the practice change. During the 24 months of the study, 1077 infants were admitted in the first 7 days of age. Ninety-six were not fed during their NICU stay, typically due to a surgical condition or due to death prior to feeding, so were excluded. The total sample size was 981 patients (91% of all admissions in the 1st week of age during the study period) for analysis: 509 in the Reactive Care Model and 472 in the Proactive Care Model.
The Intervention: Lactation Care Model
In the Reactive Care Model period, 1.9 full time equivalent IBCLC, 5 days a week daytime coverage positions, staffed by dual trained IBCLC registered nurses (RNs), were shared across the 300 bed children’s hospital, in which multiple units other than the NICU also admitted breastfeeding or MOM-fed infants. The NICU also employed a part-time breastfeeding support nurse. Prior to our practice change, bedside RNs were responsible for educating parents about how to use a breast pump, but timing of this education or whether it was even done at all were not standardized. In the Reactive Care Model, since IBCLCs were only called if concerns or lactation issues were noted, it would be very unusual for a mother to be seen in the first days postpartum.
In April 2019, an additional full time IBCLC was hired specifically for the NICU, with the previous IBCLC staff continuing to be shared by the hospital, including the NICU, for 6 days a week daytime coverage. In the NICU during the Proactive Care Model, the goal was for all families to be seen by an IBCLC within 24 hr of admission, facilitated by an automatic referral added to the standard admission order set. In addition to increase staff awareness during the annual nursing education sessions, a lecture was added about the importance of early pumping and lactation support, encouraging nurses to ask about pumping with initial parent phone calls. NICU computer screen savers encouraged staff to wait for MOM to initiate feeds (see Supplemental Material). During the vital first 2 weeks postpartum, families received multiple IBCLC follow-up visits (in-person, or, if not possible, via phone) and nurses reported daily pumped MOM volumes on NICU medical rounds. The initial IBCLC consult included education regarding the importance of MOM, instruction on pump use and recommendations for pumping frequency and duration, hands-on pumping evaluation to ensure proper use and flange fit, and a booklet. After the first 2 weeks, families received IBCLC care as needed based on the IBCLC’s assessment, or families became re-involved when NICU dietitians or nurses identified inadequate MOM volume requiring formula or donor milk supplementation, or when infants were ready for direct breastfeeding.
Families had access to hospital grade double electric breast pumps and pump kits when visiting the NICU, as well as hospital grade loaner pumps for home at no cost (but requiring a small credit card deposit); however, for lower income families, a limited supply of free personal use double electric pumps was available. Families were encouraged to bring all MOM pumped at home to the hospital milk room for storage. Donor milk was available if MOM volume was inadequate for infants born at less than 34 weeks and/or less than 1800 g, as well as for older infants after necrotizing enterocolitis, or cardiac or gastrointestinal surgery.
Measurement
Individual participant level data obtained from the EMR for all infants admitted during their the first 7 days of age were (1) basic demographics (birth weight, birth gestational age, age at admission), and (2) daily feeding data to determine type of feeds throughout the NICU stay (Table 1). Internal hospital milk room databases quantified number of bottles, as well as milliliters of pumped MOM (weighed at time of bottle drop off on scientific scales [Ohaus; New Jersey, USA] to the nearest gram and converted estimating 1 g = 1 ml after subtracting the weight of standard hospital-issued containers) stored for mothers of infants admitted to the NICU (pooled data, which included all infants admitted that month regardless of age at admission) for each month in question (Hill & Johnson, 2007); individual milk storage data for each mother was not available retrospectively so this convenience sample was utilized. Hospital milk room data, which to our knowledge have not been utilized in the literature, are updated for clinical use on a daily basis. Valid data are critical as they are used by the medical team to determine what they should order for feeds (e.g., formula or DM if no MOM is stored).
Definitions, Level of Measurement, and Analysis Conducted for Each Study Variable.
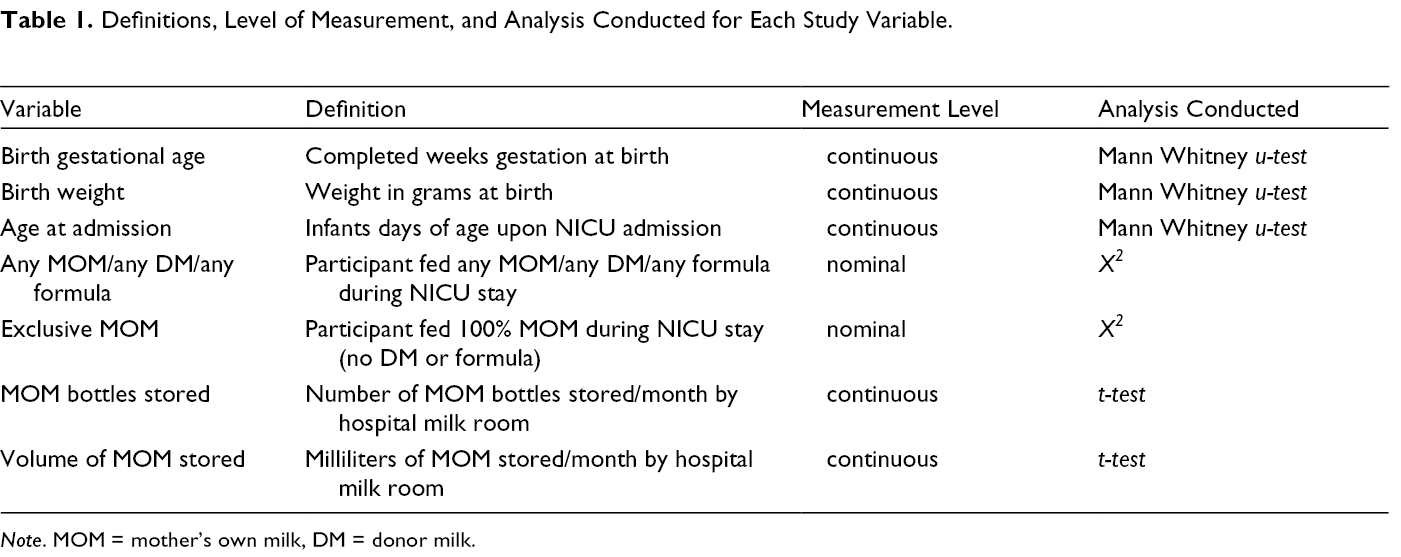
Note. MOM = mother’s own milk, DM = donor milk.
Data Collection
Written informed consent was waived by the hospital research ethics board given the de-identified retrospective nature of the study. With their approval, a list of patients admitted in the first 7 days of age during the relevant eras was obtained by the NICU data systems manager using search criteria based on the hospital EMR. Using this list, individual level data was then pulled from the EMR by the data manager. Each participant was assigned a study identifier and the medical record number was removed to anonymize data, with no linking data retained. For hospital milk room data, it was not possible to specify the above patient criteria. Therefore, we utilized pooled, anonymized milk room data that prospectively records (for clinical use) daily bottle storage intake and volume of excess MOM stored and/or fortified for all NICU patients (not just those admitted in the first 7 days of life) during the relevant eras. Anonymized data were entered into Microsoft Excel (2013) and stored on a password protected computer in a secured locked hospital office.
Data Analysis
Demographics and feeding categories during NICU stay were compared between the two eras using Mann Whitney u-testing given non-normal data distribution (Table 1). Student’s t-test was used to compare milk room bottle numbers and volumes between eras given normally distributed data. Significance for all analyses was determined based on two-tailed tests with a standard of p < .05 and a 95% confidence interval. SPSS (Version 26) and Microsoft Excel (2013) were used for analyses.
Results
Participants did not vary by care model by gestational age, birthweight, or age at admission (Table 2). Feeding outcomes for the entire NICU stay (Table 3) showed an increase in any MOM provision for infants admitted in the first 7 days of age. When stored MOM bottles and MOM bottle volumes were studied (Table 4) for all admissions including those older than 7 days of age, mean monthly bottle intake increased by nearly 1500 bottles to the highest levels ever recorded by the milk storage room, despite having slightly fewer admissions with recorded feeding data in the proactive versus reactive care model time periods (500 vs. 544 infants). Mean monthly total stored volume non-significantly increased.
Infant Characteristics (N = 981).
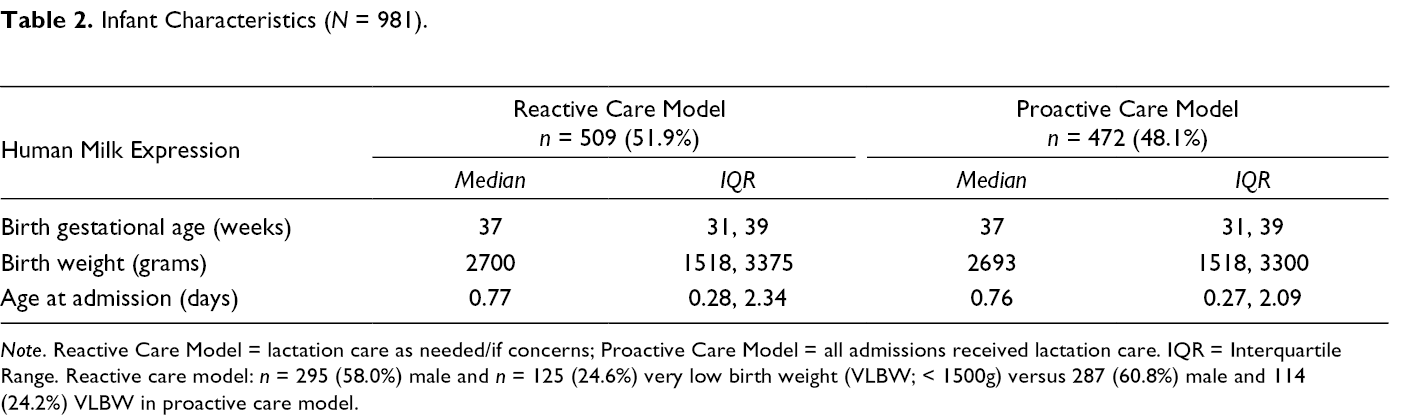
Note. Reactive Care Model = lactation care as needed/if concerns; Proactive Care Model = all admissions received lactation care. IQR = Interquartile Range. Reactive care model: n = 295 (58.0%) male and n = 125 (24.6%) very low birth weight (VLBW; < 1500g) versus 287 (60.8%) male and 114 (24.2%) VLBW in proactive care model.
Feeding Outcomes, Entire Neonatal Intensive Care Unit Stay (N = 981).
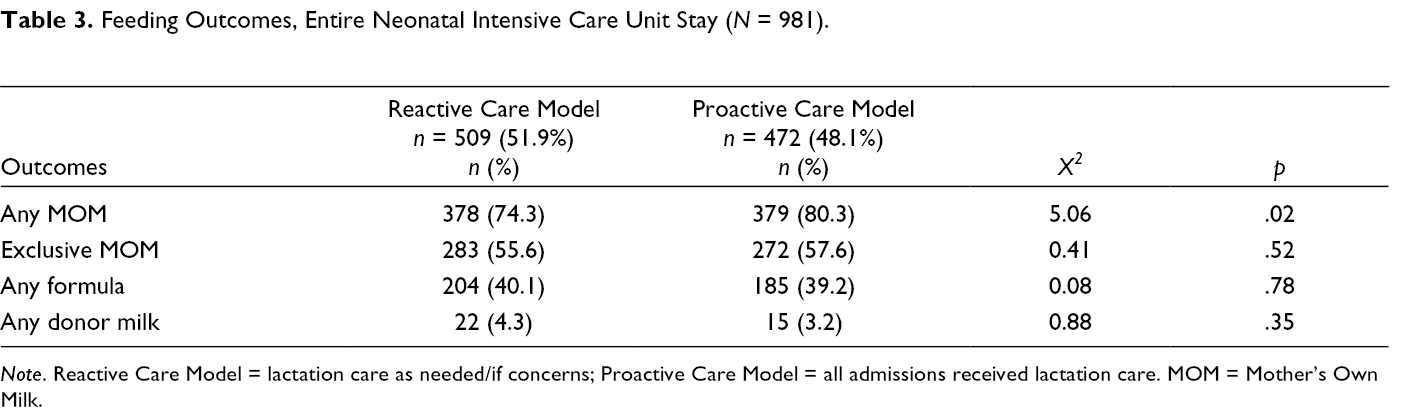
Note. Reactive Care Model = lactation care as needed/if concerns; Proactive Care Model = all admissions received lactation care. MOM = Mother’s Own Milk.
Neonatal Intensive Care Unit Mother’s Own Milk Storage.
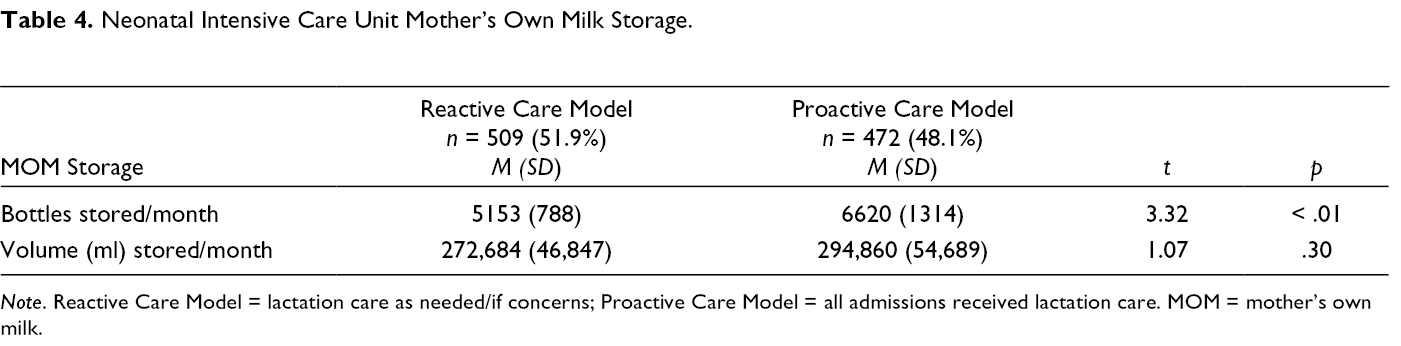
Note. Reactive Care Model = lactation care as needed/if concerns; Proactive Care Model = all admissions received lactation care. MOM = mother’s own milk.
Discussion
A change to a proactive lactation care model with additional staffing in a referral NICU was associated with increases in the proportion of infants receiving MOM during the NICU stay, as well as large increases in the number of MOM bottles received by the milk room. The median age of admission was 0.8 days in both the reactive and proactive care model time periods, so most infants were admitted very early in the 1st week of life, when lactation is modifiable.
Although we did not see statistically significant increases in exclusive MOM provision throughout the NICU stay, given the increases in milk room MOM bottles, it is possible that infants received proportionally more MOM. It is known that a higher dose of MOM received during the NICU stay is associated with improved short- and long-term outcomes (Johnson et al., 2019; Patel et al., 2017; Patra et al., 2017), so access to granular feeding data should be a focus of future studies.
With an increase in bottle number with a non-statistically significant (but clinically significant) increase of 12,000 ml/month in stored milk volume, we postulate that some of the bottles in the Proactive Care Model time period were small volume bottles used for early feeds. Concern about MOM supply in the early postpartum period has been a barrier to sustained lactation and a source of maternal stress, making the large increase in stored MOM bottles a potentially important finding (Meier et al., 2017; Mercado et al., 2019b).
Although interventions involving NICU lactation support have not universally been associated with improved MOM outcomes, our findings of increased MOM are consistent with the studies of the few researchers addressing IBCLCs in NICUs. However, unlike our study, the studies of these researchers were specific to either very low birthweight infants and/or took place in NICUs with an exclusively or largely inborn population (Mercado et al., 2019b). In addition, our approach of a proactive versus reactive model of lactation care has not been well described in the literature, in which researchers have addressed either no versus any lactation support, increasing hours of lactation support, or other methods. Nearly 20 years ago, Gonzalez et al. (2003), in one of the few studies specific to a children’s hospital referral NICU, reported that the proportion of infants ever fed MOM increased from 31% to 47% after IBCLCs were brought into the NICU; any MOM at discharge also increased. Increases in MOM provision were highest in those admitted immediately after birth, in keeping with the importance of very early pumping. In this older study, similar to our study, all participants ideally were seen within 24 hr of admission by an IBCLC for proactive support. However this comparison was to a previous era without any IBCLC availability, which would be less common in modern North American children’s hospitals (Gonzalez et al., 2003; Nottingham, 2018). In a mixed inborn/referral NICU, Dweck et al. (2008) reported that only outborn infants showed increased in-NICU and discharge MOM provision after an IBCLC was hired to see all patients upon admission, but infants with surgical conditions and anomalies, which are typically the population sent to a referral NICU, were excluded. Leeman et al. (2019) recently published a quality improvement intervention very similar to ours that took place at a referral children’s hospital NICU in which a part-time dedicated IBCLC was hired to supplement hospital-wide lactation service to increase availability of lactation care in the NICU. With proactive approaches like an automatic order for am IBCLC consult for infants admitted at < 48 hr of age, percentage of infants fed MOM on Day 7 of age increased from 76% to 90%; MOM provision throughout hospitalization or at discharge was not reported.
Our study, in keeping with findings by Leeman et al. (2019) and Dweck et al. (2008), sheds light on the challenges of relying on the infant’s healthcare team to determine which mothers are high-risk and/or need a lactation consultation. These results highlight that all mothers of infants admitted to a referral NICU should be considered high-risk for lactation challenges, in keeping with their pump dependency and maternal–infant separation (Meier et al., 2016).
Although increases in MOM provision were seen in association with our Proactive Care Model, challenges remain. Although the goal is to see all admissions within 24 hr, with staffing for 6 days a week coverage, families of infants admitted on a weekend day without coverage do not meet this goal. In addition, as a referral NICU with a large geographic catchment, mothers are not usually present on infant admission early in life, as many are still inpatients in community obstetric wards. Therefore, an in-person consult within 24 hr was not always possible, leaving IBCLCs to consult via phone or indirectly via the partner. This timing challenge for a referral NICU was also reported by Leeman et al. (2019), who reported the time to first IBCLC visit, even with an automatic consult similar to our model, decreased from 5 days to 3.3 days, an improvement; however, still missing the critical first few days of life. These barriers were partially addressed in our NICU with formal education sessions for bedside nurses, encouraging nurses upon first family phone contact to discuss early pumping prior to visitation, as well as to determine visitation timing for an in-person IBCLC consult. In addition, the NICU transport team, who transports the majority of admissions into the NICU, received education on the importance of early pumping, providing brochures (see Supplemental Material) and education to families at the referring community hospital prior to IBCLC contact, and was encouraged to bring mother’s expressed colostrum from the referring hospital to our NICU.
Overall, the addition of a NICU-specific full-time IBCLC to facilitate a Proactive Care Model was associated with improvements in MOM feeding in our children’s hospital referral NICU. This continues to be an important focus for future research and potential practice change given that less than 50% of NICUs currently employ a dedicated IBCLC (Hallowell et al., 2014). In light of the increasing financial challenges in today’s healthcare environment, given cost savings with increased MOM provision in the NICU, the cost-benefit of this staffing addition deserves further study (Johnson et al., 2014, Johnson et al., 2015; Patel et al., 2013).
Limitations
As a referral NICU, all infants were transported from other hospitals, which varied from Level I community hospitals to Level III perinatal center NICUs. Therefore, the lactation support (if any) and resources that families may have had access to prior to admission to our NICU, including early use of hospital grade pumps, varied widely. Although we limited our analysis of feeding data throughout admission to infants admitted in the 1st week of life, it has been shown that very early pumping, potentially even in the 1st hour of life, can affect long-term MOM volumes (Parker et al., 2015, Parker et al., 2020; Spatz et al., 2015). As we did not have access to families prenatally or in the immediate postpartum period, we could not influence these very early behaviors. An additional limitation is that we did not have access to proportions of each type of feed (other than exclusive MOM). Therefore, if an infant received even a single donor milk or formula feed, as is often done early in life if there is a delay in MOM coming in, it would be designated as non-exclusive MOM in our data, even if 99.9% of feeds were otherwise exclusive MOM.
There are also limitations with using milk room data, in that our milk room volumes and bottle numbers do not include fresh unfortified milk that was fed the same day as it was pumped, which is only done if there is no frozen milk in storage. The milk preparation and storage room was not involved (and therefore these volumes and bottles were not recorded other than in the infant feeding records) if the infant was not receiving fortified feeds and the mother did not have any excess milk to store. Finally, as with any retrospective study, it is possible that findings occurred by chance or were related to other initiatives. No other quality improvement initiatives focusing on MOM took place during the study period, which occurred in a relatively short time frame. However, since the initiative included increasing IBCLC hours and a universal consultation model as well as improving nursing education, we are unable to determine which part(s) of the model may have facilitated improved outcomes.
Conclusion
In this retrospective study at a tertiary referral NICU, a proactive lactation approach facilitated by increased IBCLC staffing and automatic consultations for all patients was associated with significant increases in infants receiving any MOM during the NICU stay and in the number of stored MOM bottles. Our study adds to the very limited literature for lactation care for the unique population of infants served by referral NICUs. This suggests using proactive lactation resources may improve MOM outcomes for a high-risk population.
Supplemental Material
Supplementary Material 1 - Supplemental material for Proactive Lactation Care is Associated With Improved Outcomes in a Referral NICU
Supplemental material, Supplementary Material 1, for Proactive Lactation Care is Associated With Improved Outcomes in a Referral NICU by Rebecca Hoban, Laura McLean, Samantha Sullivan and Caroline Currie in Journal of Human Lactation
Supplemental Material
Supplementary Material 2 - Supplemental material for Proactive Lactation Care is Associated With Improved Outcomes in a Referral NICU
Supplemental material, Supplementary Material 2, for Proactive Lactation Care is Associated With Improved Outcomes in a Referral NICU by Rebecca Hoban, Laura McLean, Samantha Sullivan and Caroline Currie in Journal of Human Lactation
Footnotes
Author note
All authors made substantial contributions to the study design, analysis, interpretation of data, and drafting and revising the article. All approve the final version.
Ethics approval
Written consent was waived by Hospital for Sick Children’s Research Ethics Board for retrospective use of de-identified data.
Editor’s note
JHL has a policy of not publishing references from predatory publishers. The references in the Reference List with * were published in journals whose publishers have been criticized by some academics for low standards of peer review as well as some allegations of academic misconduct. Others have felt these publishers have done their due diligence. Due to the importance of the topic covered in this review, we left the inclusion of these articles to the authors’ discretion. The authors have reviewed all references and take responsibility for their quality.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Of note, the authors L. M., S. S., and C. C. were involved clinically in the study, as they are part of the hospital and NICU IBCLC team described in the manuscript, but they have no specific conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.