
Abstract

Keywords
Background
Leading health agencies in the United States recognize breastfeeding as a public health priority (American Academy of Pediatrics, 2012; American Public Health Association, 2013; Centers for Disease Control and Prevention, 2013; U.S. Department of Health and Human Services, 2011). Through Healthy People 2020, U.S. national objectives have been set to increase the proportion of infants who are breastfed (U.S. Department of Health and Human Services, 2012). There has been a steady upward trend in the percentage of breastfed infants. The latest National Immunization Survey data from infants born in 2014 show that most of the U.S. national breastfeeding goals have been met when data for all survey participants was aggregated (Centers for Disease Control and Prevention, 2017).
Unfortunately, this achievement is not equitably shared across all subsets of the population. Non-Hispanic black (black) infants born in 2014 have not met any of the U.S. national breastfeeding goals, while non-Hispanic white (white) infants met or exceeded all of them (Centers for Disease Control and Prevention, 2017). On average, there is a 17 percentage point gap in breastfeeding initiation between black and white infants born between 2009 and 2014 (Centers for Disease Control and Prevention, 2017). Furthermore, a recent study revealed a widening black-white gap in breastfeeding rates at 6 and 12 months (Anstey et al., 2017). The percentage difference in rates for exclusive breastfeeding through 6 months between black and white infants increased from 7.8 percentage points for children born from 2003 to 2006 to 8.5 percentage points for children born from 2010 to 2013 (Anstey et al., 2017). During the same period, the 12-month breastfeeding duration rates difference gap increased from 9.7 to 13.7 percentage points (Anstey et al., 2017).
In an effort to address these disparities through community-driven solutions, in 2014, the Centers for Disease Control and Prevention (CDC), Division of Nutrition, Physical Activity and Obesity, engaged in a cooperative agreement with the National Association of County and City Health Officials (NACCHO) to implement the Reducing Disparities in Breastfeeding Through Peer and Professional Support (Breastfeeding) Project. The purpose of the project was to increase community-level implementation of evidence-based and innovative breastfeeding programs, practices, and services in predominantly African American communities.
Between January 2015 and June 2016, NACCHO awarded $2.9 million to fund 72 demonstration projects by 69 community agencies, with overarching requirements to (a) provide direct peer or professional lactation support services and (b) develop and maintain public health partnerships to build community support for breastfeeding. Grantees had autonomy in designing interventions and identifying the key partnerships to best serve their communities. Most of the grantees went further and worked to identify and remove structural breastfeeding barriers while building access to sustainable, multilevel, culturally attuned lactation support services within communities. On the basis of key lessons learned from this project, in this report we share practice-oriented strategies for agencies seeking to implement community-level breastfeeding interventions through a public health policy, systems, and environmental (PSE) change approach.
Breastfeeding Support and the PSE Change Approach
Factors known to influence maternal breastfeeding behavior include lack of breastfeeding knowledge, poor maternal self-efficacy or concerns about supply, unsupportive cultural and social norms, limited access to high-quality lactation support, and nonsupportive workplace and childcare environments (Dunn, Kalich, Fedrizzi, & Phillips, 2015; Jones, Power, Queenan, & Schulkin, 2015; U.S. Department of Health and Human Services, 2011). Furthermore, there are structural barriers to breastfeeding that exist largely outside of the mothers’ sphere of power (Lutter & Morrow, 2013). Black and low-income mothers are disproportionately affected by these unjust barriers, (e.g., unsupportive policies and systems), which affect their ability to breastfeed (Jones et al., 2015). Black women are more likely to return to work earlier (DeVane-Johnson, Woods-Giscombé, Thoyre, Fogel, & Williams, 2017; Johnson, Kirk, Rosenblum, & Muzik, 2015; Spencer & Grassley, 2013), work in environments not conducive to supporting breastfeeding mothers (Johnson et al., 2015), experience inadequate breastfeeding support from health care providers (DeVane-Johnson et al., 2017; Johnson, Kirk, Rooks, & Muzik, 2016; Spencer & Grassley, 2013; Wheeler & Bryant, 2017), and deliver at birthing facilities that do not implement evidence-based maternity care practice that support breastfeeding (Anstey et al., 2017).
Local health departments and community-based organizations are uniquely positioned to lead breastfeeding promotion and support efforts in the community. These agencies must strive to provide breastfeeding services that are consistent, frequent, predictable, and not reactively where women are expected to initiate contact (Renfrew, McCormick, Wade, Quinn, & Dowswell, 2012). Moreover, interventions to increase black breastfeeding rates and ameliorate disparities must be multilevel, touching on the many systems and social structures that shape maternal capacity to breastfeed (Chapman and Perez-Escamilla, 2012; Johnson et al., 2015). Traditional public health programs, or downstream implementations, that focus solely on individual behavior change (e.g., increasing maternal knowledge and self-efficacy) do not achieve long-term systemic influences on health (Crosby, Salazar, & DiClemente, 2013; Frieden, 2010).
The PSE change approach to public health interventions uses the socioecological model to identify systems-level factors that affect individual and community health (Comprehensive Cancer Control National Partnership, 2015; Honeycutt et al., 2015). Implementing PSE changes provides an opportunity to create sustainable organizational and community shifts and to enables long-term improvements in population health (Table 1). The PSE change approach seeks to address upstream structural or systemic barriers that lead to poor health outcomes and inequities (Honeycutt et al., 2015). PSE shifts help deconstruct barriers and build environments where the healthy choice (e.g., breastfeeding) can be the easy default option (Comprehensive Cancer Control National Partnership, 2015; Cook County Public Health Department, n.d.; Frieden, 2010; National Association of County and City Health Officials, 2017). The PSE change approach focuses on systemic solutions to community issues rather than individual behavior (Table 2). It is an upstream implementation approach, which are often proactive and sustainable beyond the funding period.
Definition and Examples of Policy, Systems, and Environmental Change With Breastfeeding-Related Examples.
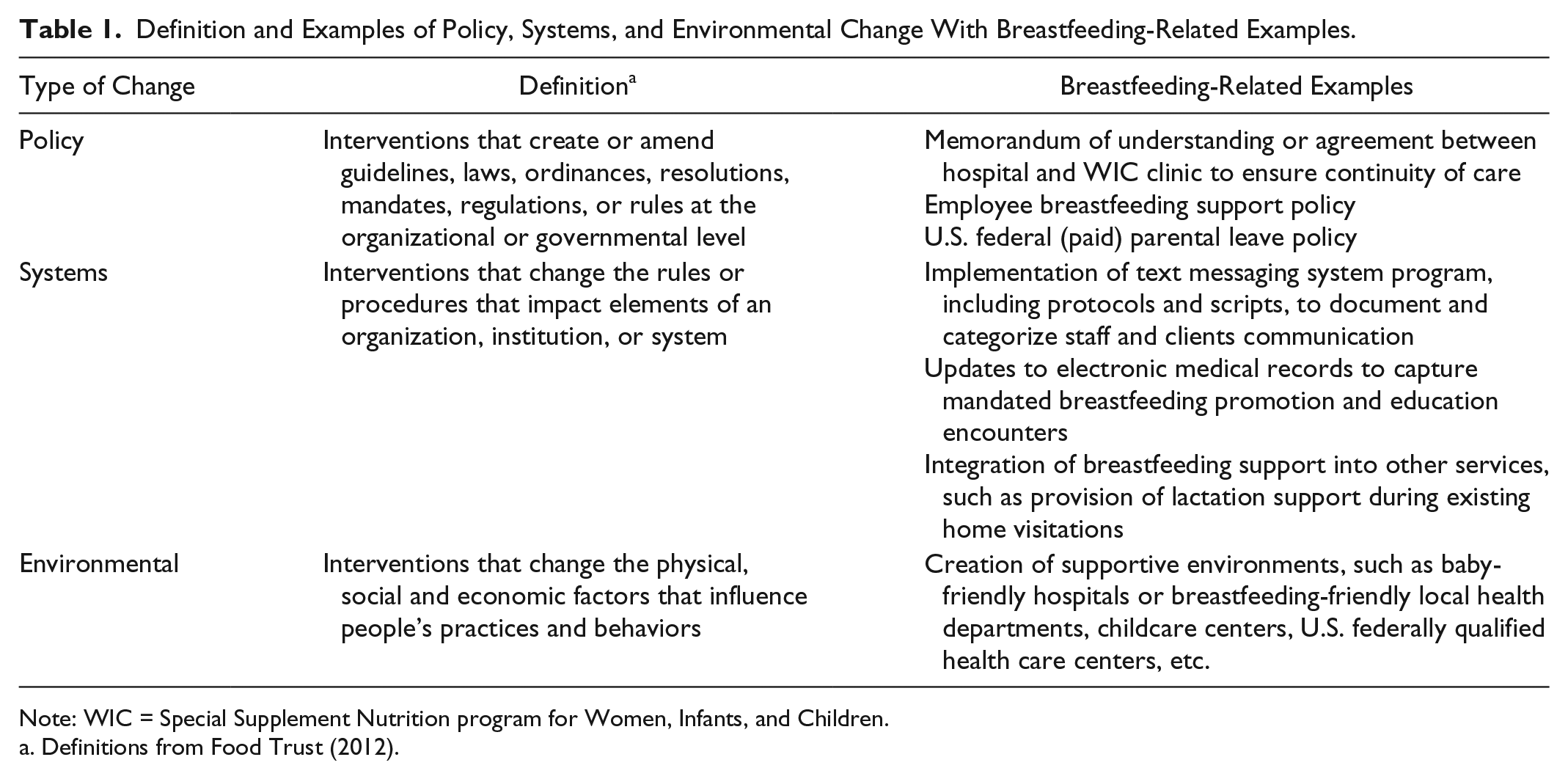
Note: WIC = Special Supplement Nutrition program for Women, Infants, and Children.
Definitions from Food Trust (2012).
Program Implementation Versus PSE Change Implementation.
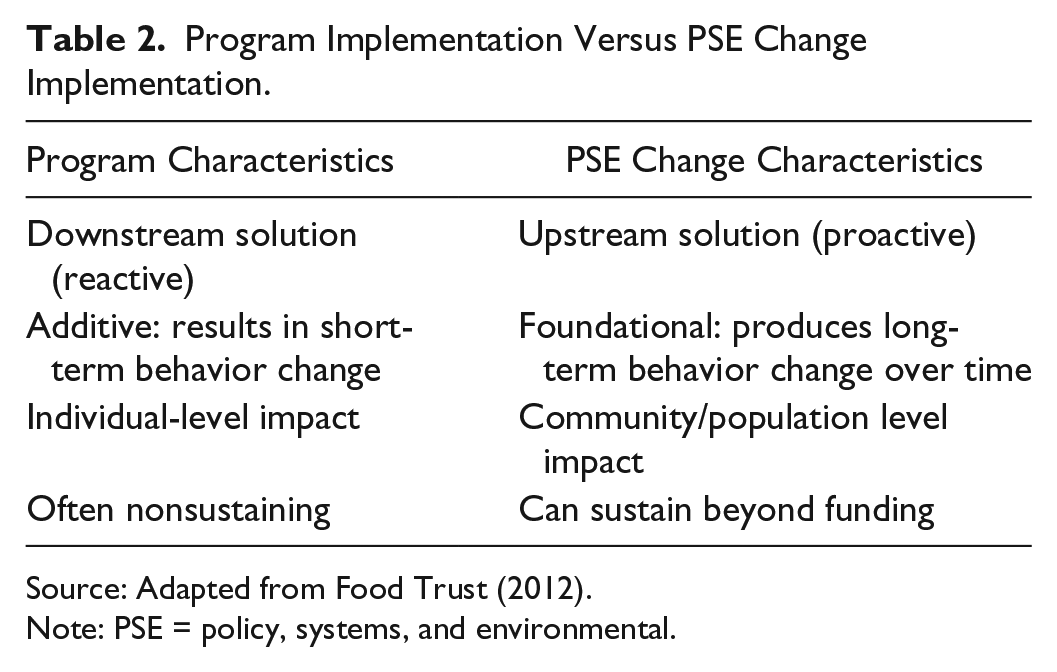
Source: Adapted from Food Trust (2012).
Note: PSE = policy, systems, and environmental.
Originating from CDC and Institute of Medicine (2003) efforts, the PSE change approach is widely used in community health programming (Comprehensive Cancer Control National Partnership, 2015). Within the breastfeeding support context, there are also well-known programs that implemented the PSE change approach. For example, the Baby-Friendly Hospital Initiative (World Health Organization & UNICEF, 2009) is an effective PSE change intervention that sets requirements for hospitals and birth centers to adopt a comprehensive set of policies and systems on the basis of evidence-based maternity care practices to improve the environment where breastfeeding initiation takes place (Baby-Friendly USA, 2012; Lutter & Morrow, 2013; Pérez-Escamilla, Curry, Minhas, Taylor, & Bradley, 2012; Spaeth, Zemp, Merten, & Dratva, 2018).
For community-level breastfeeding programs, the use of the PSE change approach seeks to change the context to enable breastfeeding at recommended levels to be the default, easy option for families. Changing the community context includes increasing access to breastfeeding care by establishing supportive policies, systems, and environments within the community (Pérez-Escamilla et al., 2012). NACCHO grantees implemented several PSE changes, including the development of culturally tailored curricula and community resource guides, implementation of social marketing campaigns to promote normalization of breastfeeding, establishment of referral systems to institutionalize care transitions for mother-infant dyads, and use of technology (e.g., social media interaction groups, online portals, semiautomated texting programs, and telehealth applications).
Recommendations
Twenty-seven grantees reported inclusion of PSE change strategies in their projects. However, qualitative analysis of final reports and call notes from quarterly meetings revealed that additional grantees implemented or were on the pathway to creating PSE shifts through their project. This discrepancy in reporting indicates a gap in public health breastfeeding knowledge and the need for training and technical assistance on the use of the PSE change framework for agencies implementing community-level breastfeeding programs.
NACCHO identified four key drivers for the PSE change approach implementation. These critical facilitators were (a) building a community-specific understanding of breastfeeding barriers, (b) assessing organizational opportunities and capacities to improve breastfeeding support services, (c) leveraging internal resources (e.g., grant funds, staff, and systems), and (d) leveraging external partner resources (e.g., shared space, community connections, client access) to effect change in the policies, systems, and environments that serve families and communities. On the basis of lessons learned from grantees and these identified driving forces, NACCHO recommends the following for local agencies aiming to implement community-level breastfeeding support programs.
Assess Community-Specific Needs and Breastfeeding Barriers
Although researchers have identified a set of common structural barriers to breastfeeding that disproportionately affect low-income mothers of color, the specific PSE changes necessary to sustainably support breastfeeding at the community level depend on the unique assets and needs of the servicing community (McKenzie, Neiger, & Thackeray, 2013). Forty-one grantees conducted a pre-implementation community needs assessment or environmental scan (see Table 3 for examples). Some assessments were an informal polling of community mothers, and others were formalized evaluations, typically embedded in a local health department, health care system, or health coalition’s existing community health assessment plan.
Community Needs Assessment.
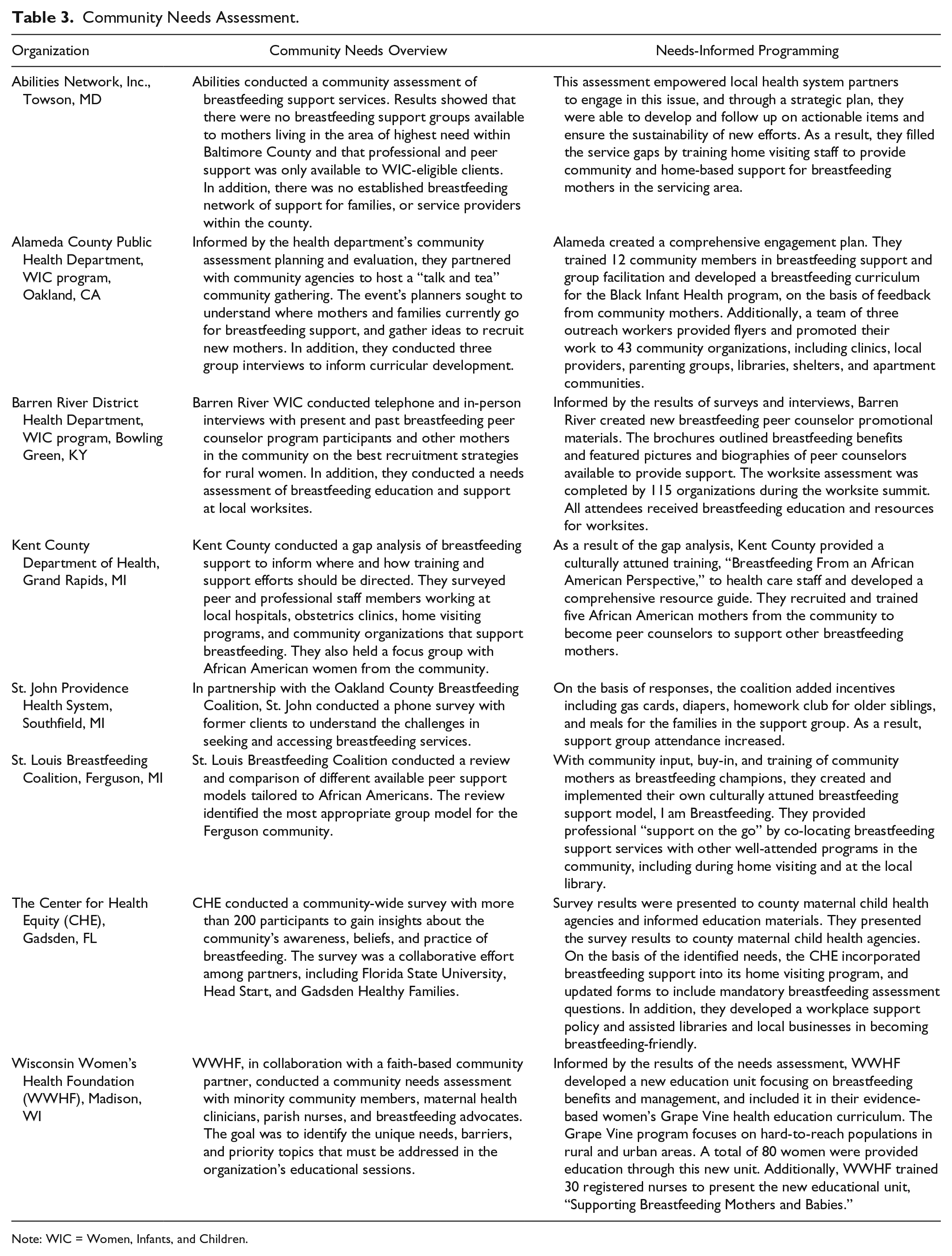
Note: WIC = Women, Infants, and Children.
A key lesson learned during the project was that service availability is not synonymous with service accessibility. Some factors (e.g., timing and location of services, transportation, childcare, and cultural appropriateness of educational materials and providers) can make existing lactation support services largely inaccessible to women in the community.
Grantees who were empowered with this knowledge from a community needs assessment were able to modify their implementation to better support families by addressing identified needs. One of the most poignant lessons learned by all grantees was eloquently stated in a grantee’s final report: “If we are truly supporting moms, we must listen to their needs, meet their expectations and remove barriers to their participation.”
Identify Organizational Levers for Change
Organizations seeking to implement community-level breastfeeding support interventions should conduct a comprehensive analysis of internal operations to determine the organizational limitations to continuously support breastfeeding, by making it easier for mothers to sustain breastfeeding and identify potential organizational contributions to community breastfeeding barriers. The grantees presented in Table 4 conducted self-assessments and identified strategic opportunities to improve the nature and quality of their breastfeeding services to their communities by implementing PSE changes within their organizations.
Assessment of Organizations’ Limitations to Sustainably Support Breastfeeding.
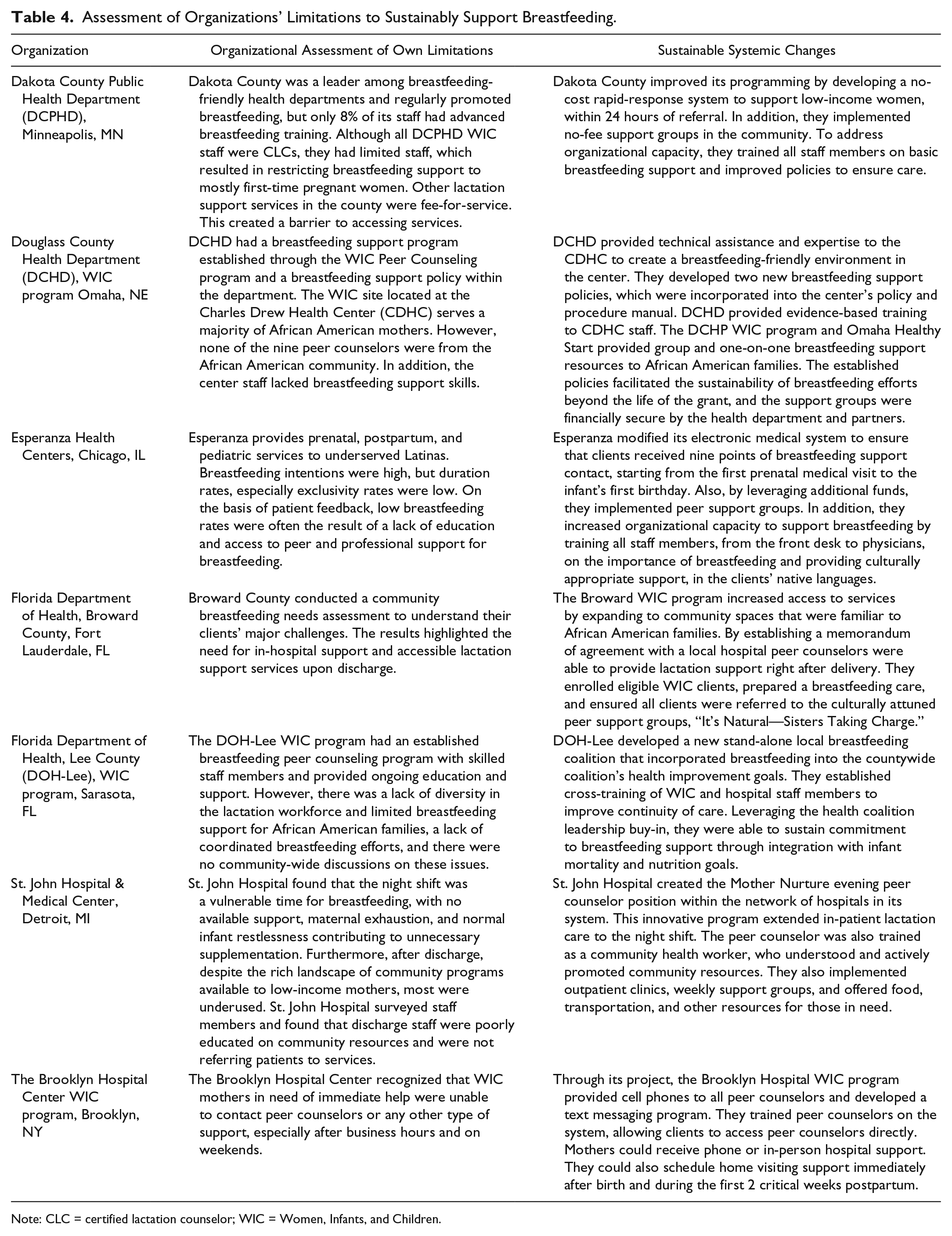
Note: CLC = certified lactation counselor; WIC = Women, Infants, and Children.
Identified organizational limitations included having poorly trained staff members who are not knowledgeable about breastfeeding; not providing a welcoming space for mothers to breastfeed within the agency; offering support services that families are not able to access because of timing, location, and are not welcoming of family members and older siblings; and providing inconsistent, conflicting messaging within the organization staff.
Leveraging Internal and External Resources
In the face of limited resources, it is challenging to make a lasting and sustained impact on many public health efforts, including breastfeeding (Centers for Disease Control and Prevention, 2012). Strategically leveraging internal and external resources through integration and co-location of services may extend the lactation support safety net available to families and is part of a PSE change solution.
Grantees that used NACCHO funds to complement or expand preexisting projects, instead of investing in a downstream lactation support interventions (limited to the provision of direct services only) were more effective in supporting a larger number of families during and beyond the funding period. Grantees leveraged resources not only to sustain programs but also to benefit partners and the broader community. Some outcomes of leveraging were expanding program or organizational capacity to serve more families, supporting program activities sustainability, increasing the use of current and new programs and services, meeting identified needs of the community, providing and identifying unused or underused resources, and avoiding duplication of services.
Some grantees formally incorporated breastfeeding intervention activities into their organizational strategic plans. As a result, they were able to make essential lactation services available to a vast number of women and families by integrating those services into existing programs (Table 5). Across all projects, organizations invested grant dollars to increase the capacity of staff members, contractors, community volunteers, and staff members from partner organizations to provide lactation support services in the community. A nondistinct count of 654 people received lactation-related training through NACCHO grant funds. Among this group, some people received multiple types of training (e.g., as a peer counselor and subsequent training to become a certified lactation counselor (CLC). Fifty-one International Board Certified Lactation Consultants (IBCLCs) received advanced lactation training. Sixty-nine individuals received required training to qualify for the IBCLC examination. Two hundred seventy-nine people received training to qualify for the CLC or equivalent certification exam, and 255 people were training as peer counselors.
Leveraging Internal Resources.
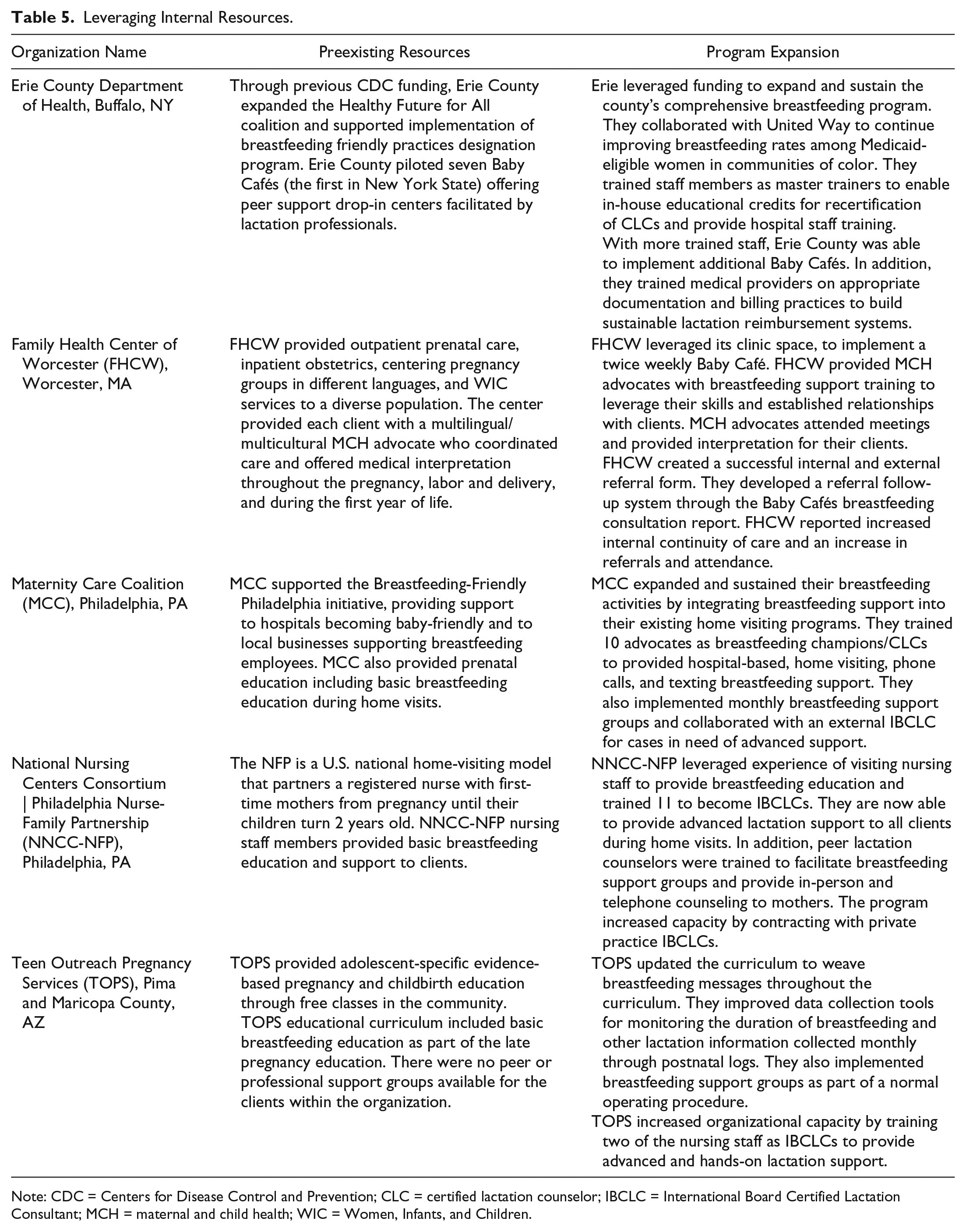
Note: CDC = Centers for Disease Control and Prevention; CLC = certified lactation counselor; IBCLC = International Board Certified Lactation Consultant; MCH = maternal and child health; WIC = Women, Infants, and Children.
Grantee partnerships with other community organizations enabled the leveraging of multiorganizational resources, skills, and policies and systems to expand service capacity, improve coordination of referrals, and integrate breastfeeding support into other public health and social services programs. Collaboration with agencies that also provide health services to the community allows leveraging of space, staff, and programming. In addition, partnerships with nontraditional and nonhealth agencies (e.g., faith-based organizations, social service agencies, housing agencies, and transportation offices) created the space to broaden the reach of both organizations.
Breastfeeding services should be incorporated into or co-located with and be provided around the same time as existing well-attended programs, rather than being stand-alone programs (Lilleston, Nhim, & Rutledge, 2015). Programs prime for integration are services that already have mandatory attendance or participation (e.g., maternal and infant home visitation programs and prenatal care program such as Centering Pregnancy). This strategy of providing a one-stop shop for program participants enables families to overcome barriers of lack of transportation and time. Grantees were innovative in their approach to service integration and co-location. Table 6 shows selected grantees examples leveraging partnerships.
Leveraging External Partnerships.
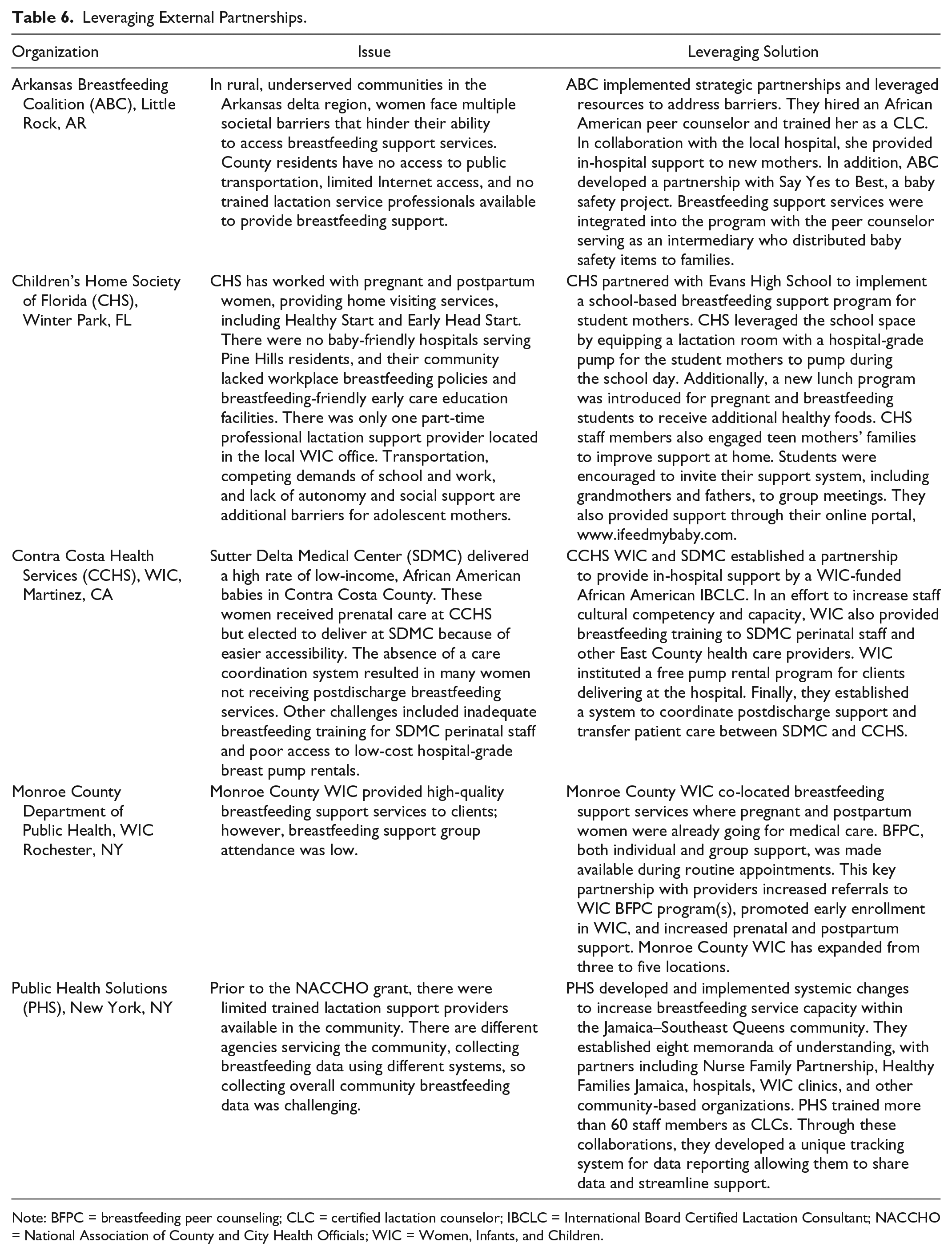
Note: BFPC = breastfeeding peer counseling; CLC = certified lactation counselor; IBCLC = International Board Certified Lactation Consultant; NACCHO = National Association of County and City Health Officials; WIC = Women, Infants, and Children.
Conclusions
Community agencies seeking to provide breastfeeding promotion, education, and support services in black and low-income communities in an effort to ameliorate breastfeeding disparities must operate with the understanding that suboptimal breastfeeding rates among these populations are influenced largely by social and systemic barriers that exist outside the parents’ sphere of power (Lutter & Morrow, 2013; Temple, 2017). Programs focusing solely on individual behavior change miss the opportunity to identify and creatively address the underlying needs of the families within their communities (Honeycutt et al., 2015).
To implement PSE changes, organizations must understand and address the needs of the community and strategically plan to sustain activities initiated with time-limited grants by incorporating breastfeeding services into the agency’s larger programming and by building solid community partnerships (Centers for Disease Control and Prevention, 2012). Partnerships are critical for PSE change implementation and can strengthen collective capacity to address structural barriers that contribute to inequitable breastfeeding rates that local agencies cannot overcome alone.
Footnotes
Acknowledgements
We thank Debra Dekker, PhD, for analyzing and providing grantee’s data throughout the project. We thank Margaret Carr for supporting the project and this article development in any way needed. Finally, we thank all 69 grantee organizations who worked hard with limited funds and provided great qualitative data through reports, calls, and presentations.
Authors’ Note
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the CDC. The authors prepared this article within the scope of their employment with NACCHO.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Reducing Breastfeeding Disparities Through Peer and Professional Support is funded by the CDC, Division of Nutrition, Physical Activity and Obesity.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: U.S. Department of Health and Human Services, CDC, Grant 6 NU38OT000172-05-02.