
Abstract
Researchers and practitioners have long been interested in the relations of basic personality domains with health. Whereas previous meta-analyses have focused on the Big Five traits, we provide the first meta-analysis of the relations between the HEXACO domains, as assessed by HEXACO Personality Inventories, and various health outcomes (k = 276, N = 92,319). In general, relations of the HEXACO domains were strongest with mental health, followed by health behavior, whereas relations with physical health outcomes were weak and largely non-significant. All HEXACO domains were significantly linked to mental health and health behavior outcomes. Extraversion exhibited the strongest correlation with mental health (
Introduction
Being healthy is typically regarded as an important goal of human life. Correspondingly, researchers have long been searching for the predictors of health across various categories, including mental health, health behavior, and physical health, and several important correlates of health have been identified. These include environmental factors, such as climate change (Watts et al., 2015), discrimination (Pascoe & Richman, 2009), and social inequality (Kondo et al., 2009)—which all affect health negatively—as well as individual difference variables, such as cognitive abilities (Gottfredson & Deary, 2004), socioeconomic status (Adler & Ostrove, 1999), and personality traits (Friedman & Kern, 2014). Especially the idea that personality traits are related to health has been of interest to researchers and practitioners for a long time (Dammeyer & Zettler, 2018): Greek and Roman philosophers, such as Hippocrates or Galen, already investigated individual differences in the proclivity to be healthy. In recent decades, more rigorous research has emerged across disciplines, including medicine as well as clinical and health psychology (Chapman et al., 2011; Costa & McCrae, 1986; Ferguson, 2013).
Most recent research on the relations of personality traits with health has focused on the Big Five domains: Openness to Experience/Intellect, Conscientiousness, Extraversion, Agreeableness, and Neuroticism (vs. Emotional stability). Findings from several meta-analyses indicate that these domains explain considerable variance in various health outcomes (e.g., Malouff et al., 2006; Ohi et al., 2016; Wilson & Dishman, 2015). For instance, meta-analyses found significant relations between Conscientiousness and subjective and psychological well-being (mean r = .36; Anglim et al., 2020), between Extraversion and schizophrenia (Hedges' g = −.79 comparing patients with healthy individuals; Ohi et al., 2016), and between Neuroticism and depressive symptoms (r = .39; Hakulinen et al., 2015).
Definitions of the HEXACO Domains.
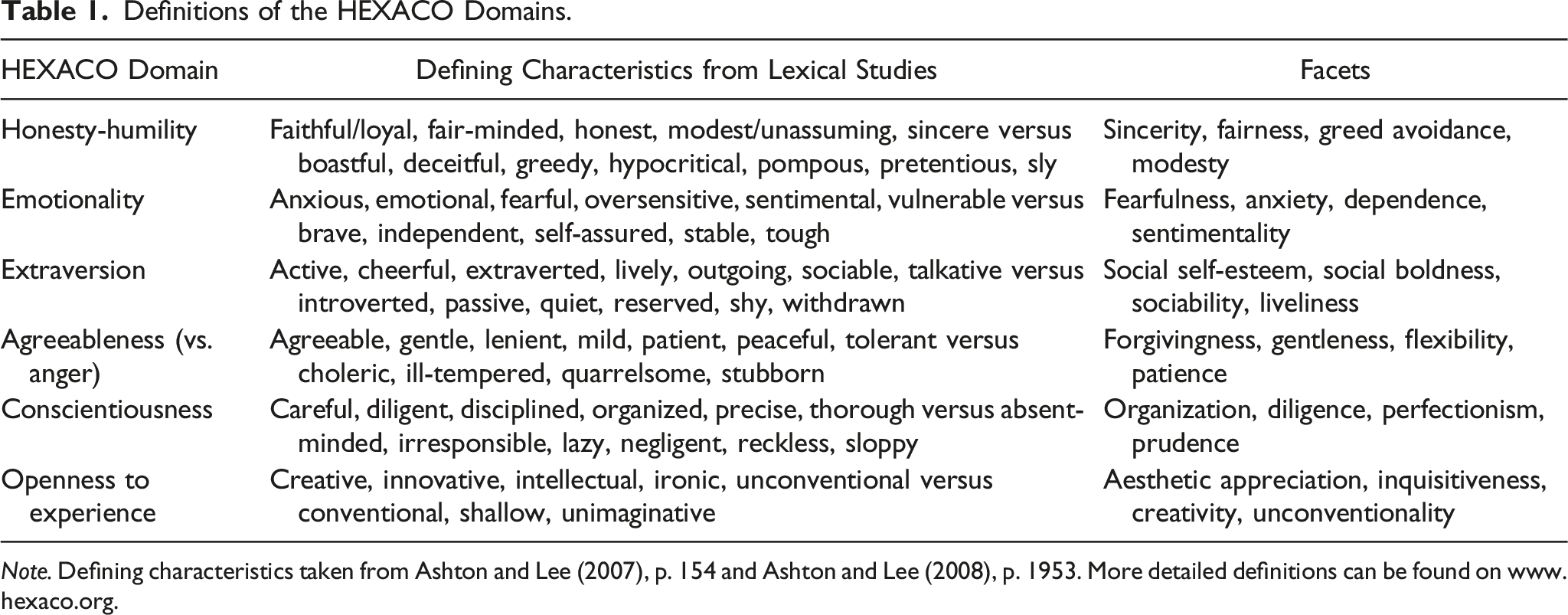
Note. Defining characteristics taken from Ashton and Lee (2007), p. 154 and Ashton and Lee (2008), p. 1953. More detailed definitions can be found on www.hexaco.org.
Importantly, notable differences between the Big Five and the HEXACO model exist in how they organize the personality space (Thielmann et al., 2022). By implication, the consideration of the HEXACO model might also be worthwhile in relation to health outcomes. Specifically, Honesty-Humility, the domain reflecting the most prominent difference between the HEXACO and other personality models, exhibits a positive meta-analytic correlation with subjective and psychological well-being (Anglim et al., 2020), and initial evidence has also linked Honesty-Humility to other health outcomes, such as emotional exhaustion (Yang et al., 2019) or alcohol consumption and smoking (Wetzel & Frick, 2020). There is also initial evidence for an association of the HEXACO domain Emotionality—the counterpart of Big Five Neuroticism, which, however, involves noteworthy conceptual differences—with health outcomes, such as mindfulness (Holden et al., 2020) and schizotypy (Janošević & Petrović, 2019). Other differences between the Big Five and the HEXACO model, such as those in the personality variance captured by Agreeableness (vs. Anger), might also affect relations with health. Prior research relating personality traits to health criteria solely based on the Big Five model might thus prevent a more comprehensive understanding of how basic personality in general relates to health outcomes. To address this issue, we meta-analytically examine for the first time the relations of the HEXACO domains with various indicators of health and compare effect sizes to those for the Big Five domains.
Specifically, we provide a meta-analysis of the relations of the HEXACO domains with mental health, health behavior, and physical health, as well as with more specific health criteria within these categories (e.g., life satisfaction, physical strength, and substance use). In addition, we compare the criterion-related validity of the HEXACO domains for specific health outcomes with the validity of the Big Five domains and examine if Honesty-Humility explains incremental variance over and above the Big Five in these outcomes. Our findings thereby foster a deeper understanding of how basic personality domains relate to various health outcomes, which has important implications for research. First, our findings can illuminate the various trait-based pathways to health. Second, our findings extend the nomological net of the HEXACO domains by examining their relations with various health outcomes, which have not been systematically examined before. Comparing results to those found for the Big Five further clarifies how structural differences between the two personality models affect outcome relations in the context of health.
Health
The World Health Organization (1946, p. 1) defines health as “a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity.” This implies that not just diagnosed physical diseases, such as cancer or diabetes, but also broader conceptualizations including mental health or health behaviors are indicative of overall health. Following Strickhouser et al. (2017), who conducted a second-order meta-analysis of the relations between the Big Five domains and health, we distinguish between three health categories: mental health, health behavior, and physical health. Strickhouser et al. (2017) defined mental health as “outcomes that reflect cognitive, emotional, or social well-being, such as depression, happiness, and diagnosed psychopathologies”; health behaviors as “outcomes that reflect engagement in health promoting or deteriorating activities, such as exercise, risky sex, and substance use” 1 ; and physical health as “outcomes that reflect the fitness of the body, including measures of one’s physical condition, diagnosed physical diseases (e.g., cancer), and ultimately mortality” (all p. 3).
Health criteria included in any of the three categories have important large-scale implications for social cohesion and societal functioning: For example, being healthy facilitates actively participating in society, and it takes pressure from the health care system. The prediction and promotion of health is therefore an important aim of many societies, governments, and organizations. One cornerstone to develop and implement health-promoting interventions is to know which individual differences variables are associated with being healthy.
Personality
Personality traits denote relatively stable tendencies to think, feel, and act. One common approach to structure personality traits is to categorize a large number of attributes on which individuals differ (taken from the lexicon) into a limited set of latent constructs. This so-called lexical approach to personality assumes that human personality is encoded in spoken languages. Using this approach provides a clear framework for the study of relatively enduring individual differences. For a long time, the Big Five model (or Five-Factor Model [FFM]; Goldberg, 1990; McCrae & Costa, 1992) has been the most commonly used, broad personality taxonomy. More recent evidence has shown, however, that six domains can be replicated across lexical studies in various languages, resulting in the HEXACO model which captures more personality variance than the Big Five (Ashton & Lee, 2019, 2020; Thielmann et al., 2022). Although the Big Five and the HEXACO model share several similarities, crucial differences exist. Most notably, the HEXACO model includes a sixth domain termed Honesty-Humility. This domain describes the tendency to be fair, genuine, and modest versus greedy, pretentious, and sly. Whereas Honesty-Humility is considerably correlated with Big Five Agreeableness (
The HEXACO domains Emotionality and Agreeableness versus Anger (in the following simply: Agreeableness) also differ substantially from their Big Five counterparts Neuroticism and Agreeableness, respectively. That is, the specific lower-order facets of these two domains are differently distributed across domains to facilitate the interpretability of the two factors. Emotionality describes the tendency to be fearful and anxious, but also to feel a close connection with others and to be dependent on them. Compared to Big Five Neuroticism, Emotionality thus lacks variance associated with irritability and anger, which is instead captured by (low) HEXACO Agreeableness. HEXACO Agreeableness describes the tendency to be forgiving, gentle, and patient with others, and to be willing to compromise with them. Compared to Big Five Agreeableness, it lacks variance associated with sentimentality, which is instead captured by HEXACO Emotionality. Big Five but not HEXACO Agreeableness also captures content related to compassion and empathy, which is captured by Emotionality in the HEXACO model.
Extraversion, Conscientiousness, and Openness to Experience are almost identical across models (for meta-analytic estimates, see Thielmann et al., 2022).
Big Five and Health
Various meta-analyses have reviewed the relations of the Big Five domains with several indicators of health (e.g., Connor-Smith & Flachsbart, 2007; Luo et al., 2022; Ohi et al., 2016; Samuel & Widiger, 2008; Saulsman & Page, 2004; Wilson & Dishman, 2015). Strickhouser et al. (2017) summarized (some of) these meta-analyses in a second-order meta-analysis, showing that Neuroticism (average r = −.20, range −.48 to .10), Conscientiousness (average r = .19, range −.13 to .53), and Agreeableness (average r = .17, range −.03 to .47) were, on average, the strongest predictors of overall health. Correlations of Extraversion (average r = .08, range −.19 to .40) and Openness to Experience (average r = .05, range −.15 to .45) with overall health were substantially weaker. Regarding the three health categories, correlations were generally stronger for mental health (average r = |.06| to |.27| across Big Five domains) compared to health behaviors (average r = |.00| to |.12|) and physical health (average r = |.00| to |.03|).
Crucially, the average correlations between the Big Five traits and health varied considerably across the criteria included in Strickhouser et al.’s (2017) meta-analysis. For example, although Openness/Intellect did not show a strong average correlation with overall health, criterion-specific correlations varied from r = .03 (physical activity) to r = .45 (resilience). The same held for the other Big Five domains, even when comparing criteria within the specific health categories. For example, although Neuroticism exhibited the strongest average correlation with mental health (r = −.27), the correlations differed for the specific mental health outcomes, ranging between r = −.48 (life satisfaction) to r = .10 (psychopathy). Despite these differences between criteria, we base our hypotheses, as described next, on the average correlations with the three health categories (i.e., mental health, health behavior, and physical health). Importantly, though, the high variability in correlations between specific health outcomes indicates that much is to be gained from such a finer-grained analysis—something that we offer in the current meta-analysis as well.
HEXACO and Health
Because personality traits are psychological variables, which likely exhibit stronger relations with outcomes on the same construct level, we generally expect that personality-health relations are strongest for mental health, somewhat weaker for health behaviors, and weakest for physical health. Indeed, this is also what Strickhouser et al. (2017) found (see also, Luo et al., 2022).
Although HEXACO Emotionality differs to some extent from Big Five Neuroticism, the two domains still correlate substantially with each other (
Recent meta-analytic evidence (Anglim et al., 2020; Zettler et al., 2020) also indicates that HEXACO Agreeableness correlates positively with indicators of subjective and psychological well-being and negatively with anxiety, stress, and risk-taking, but relations with other health outcomes have not yet been meta-analytically examined. Primary studies do, however, indicate that agreeable individuals are less likely to engage in risky health behaviors, such as sexting (Morelli et al., 2020) or problematic gambling (McGrath et al., 2018). Based on these findings, we expected a positive correlation of HEXACO Agreeableness with mental health and health behavior. We had no a priori expectations for the relations of HEXACO Agreeableness with physical health.
For Big Five Agreeableness, which exhibits substantial overlap with HEXACO Agreeableness (
Method
Literature Search
The goal of our literature search was to include as many studies as possible assessing at least one of the HEXACO domains and a relevant health outcome. As a starting point, we relied on the results of the literature search by Zettler et al. (2020), who conducted a large-scale meta-analysis of the nomological net of the HEXACO model to examine whether each HEXACO domain maps onto a theoretically relevant outcome domain. These authors coded all studies assessing at least one of the HEXACO domains irrespective of the examined outcome but did not systematically examine relations with health outcomes in their meta-analysis. Zettler et al. (2020) conducted their literature search in September and October 2017 and searched for all studies—described in English-written published articles, conference proceedings, and dissertations or theses—assessing HEXACO domains. We updated their literature search on July 1, 2020, following the same procedures to include all relevant articles and to guarantee consistency in the search process. For all search results detailed below, we therefore focused on documents published in or after 2017.
Using the search terms “HEXACO OR ‘Big Six’ OR ‘Honesty-humility’”, we searched EBSCOhost/PsycINFO (397 hits; in the keywords) and Scopus (264 hits; in the title, abstract, and keywords). We also conducted three independent searches on Google Scholar: One searching for “HEXACO personality” (3760 hits), one for “Honesty-humility” (2980 hits), and one for “Big Six” (1390 hits). For these three searches, we extracted the first 1000 search results. 2
These search strategies resulted in 2326 combined results after removing duplicates. Of these, 48 documents were already coded by Zettler et al. (2020). Of the remaining results, 502 documents were deemed potentially relevant for the current meta-analysis based on an examination of the title, abstract, and keywords by the first author. The full-texts of these 502 documents were then examined with regard to the inclusion criteria outlined below. Whenever we did not have access to the full-text, we contacted the corresponding (or first) author and asked for the document or for the relevant statistical information (24 documents remained inaccessible). We also posted calls for unpublished data in January 2021 via the email lists of different personality associations (i.e., Association for Research in Personality, European Association of Personality Psychology, and German Association of Psychology). Figure 1 includes a PRISMA flowchart summarizing the literature search. Flowchart depicting the literature search process.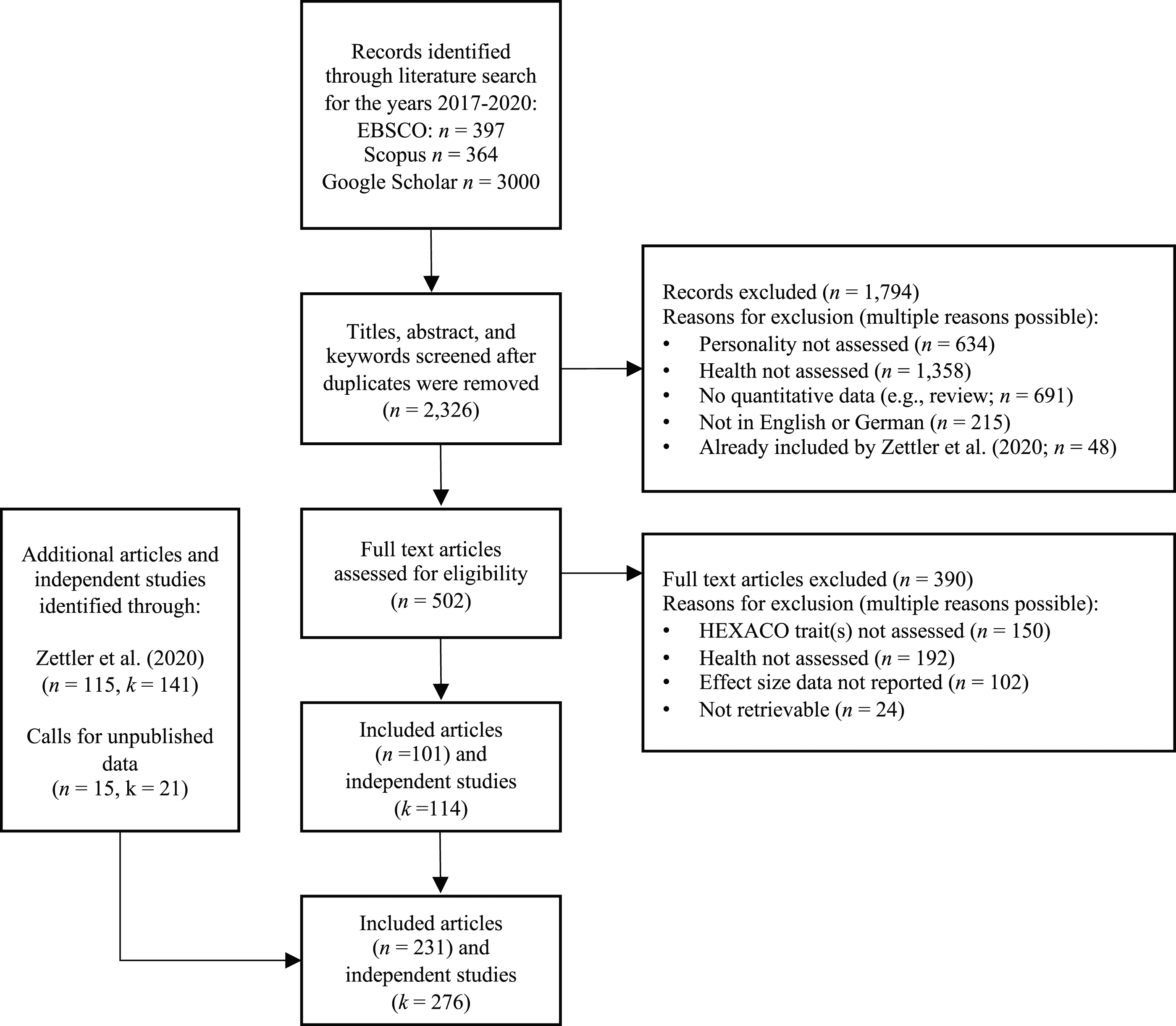
Inclusion Criteria
To be included in the current meta-analysis, studies had to: 1. Measure at least one of the HEXACO domains with a version of the HEXACO-PI-R.
3
2. Measure at least one health outcome that a) is either beneficial or detrimental for overall health (i.e., has valence) and b) contributes to overall health in a linear manner. For example, we excluded physical measures, such as the 2D:4D ratio or genetic information, for which it is unclear whether and how they contribute to overall health, or outcomes such as perfectionism, which is beneficial for health at moderate levels but can be detrimental for health at high levels (Molnar et al., 2012). 3. Report the correlation coefficient r and the sample size N for the relation of interest, or statistics that allow for the calculation of r (e.g., standardized regression coefficients, Cohen’s d). 4. Report results in English, German, or Dutch.
Overview of the Meta-Analytic Dataset.
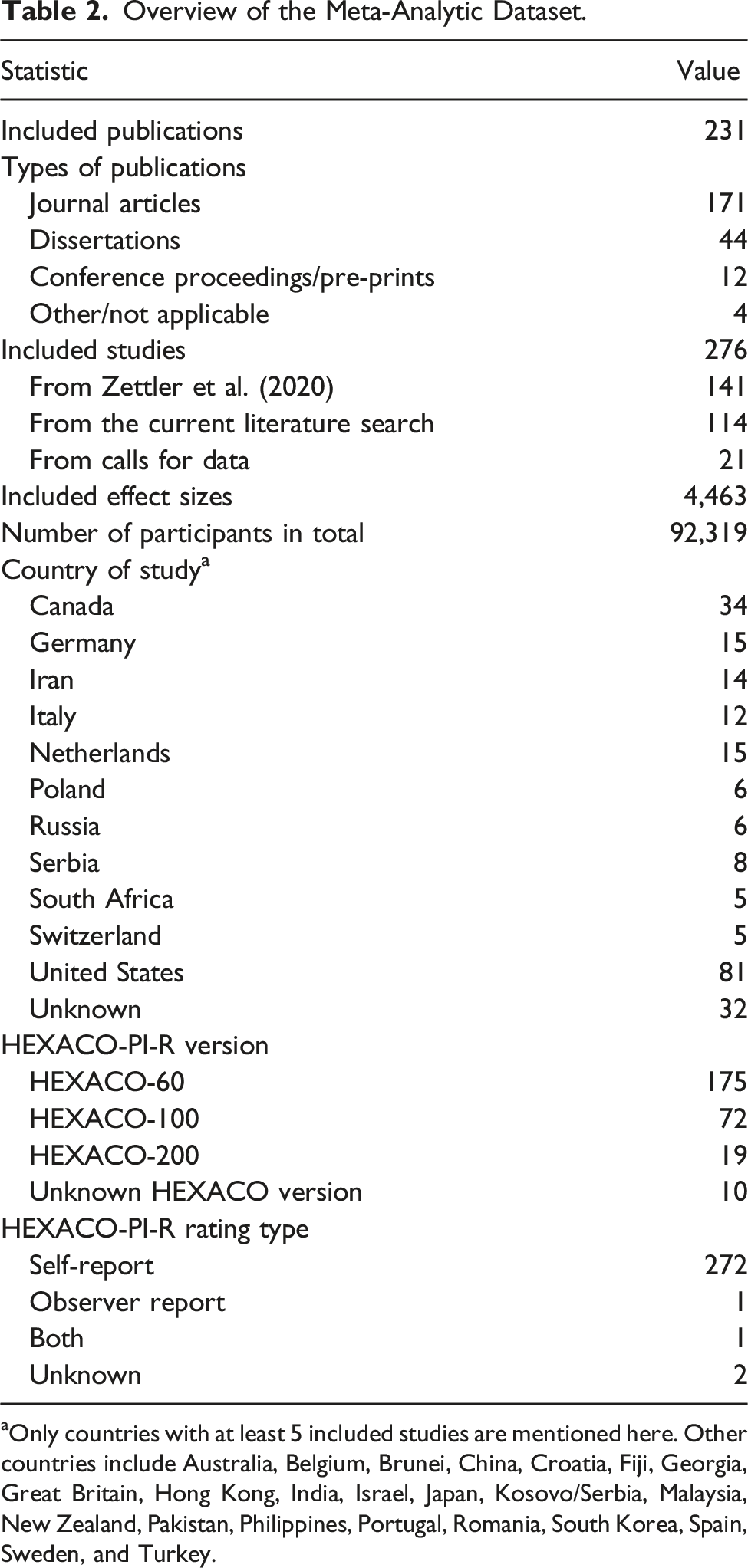
aOnly countries with at least 5 included studies are mentioned here. Other countries include Australia, Belgium, Brunei, China, Croatia, Fiji, Georgia, Great Britain, Hong Kong, India, Israel, Japan, Kosovo/Serbia, Malaysia, New Zealand, Pakistan, Philippines, Portugal, Romania, South Korea, Spain, Sweden, and Turkey.
Coding of Study Variables
The second and third author coded all data extracted from Zettler et al. (2020). Their coding scheme and all coded data is available via this link. It should be noted that the current meta-analysis includes some effect sizes that were already analyzed by Zettler et al. (e.g., life satisfaction and exercising), but mostly includes effect sizes that have not been analyzed yet, although they were initially coded (e.g., alcohol consumption). The first author of the current manuscript coded all documents included from the current literature search (55.1% of all included effect sizes), and checked approximately half of the codings included from Zettler et al. (2020). Inconsistencies were resolved through discussions among the authors.
To assign criteria to a health category (i.e., mental health, health behavior, or physical health), the first author provided an initial categorization of all included outcomes and discussed it with the second author until agreement was reached. When in doubt, we revisited the operationalization and measurement of the outcome in the included study. The third author then checked these categorizations until agreement was reached among all three authors. 5 A few criteria (e.g., perceived health and health-related quality of life) could not be classified into one of the categories because they tapped into multiple categories. For example, when participants were asked to rate their overall health, it is not clear whether they considered their mental or physical health, or both. We assigned these criteria to an additional category labeled “various.”
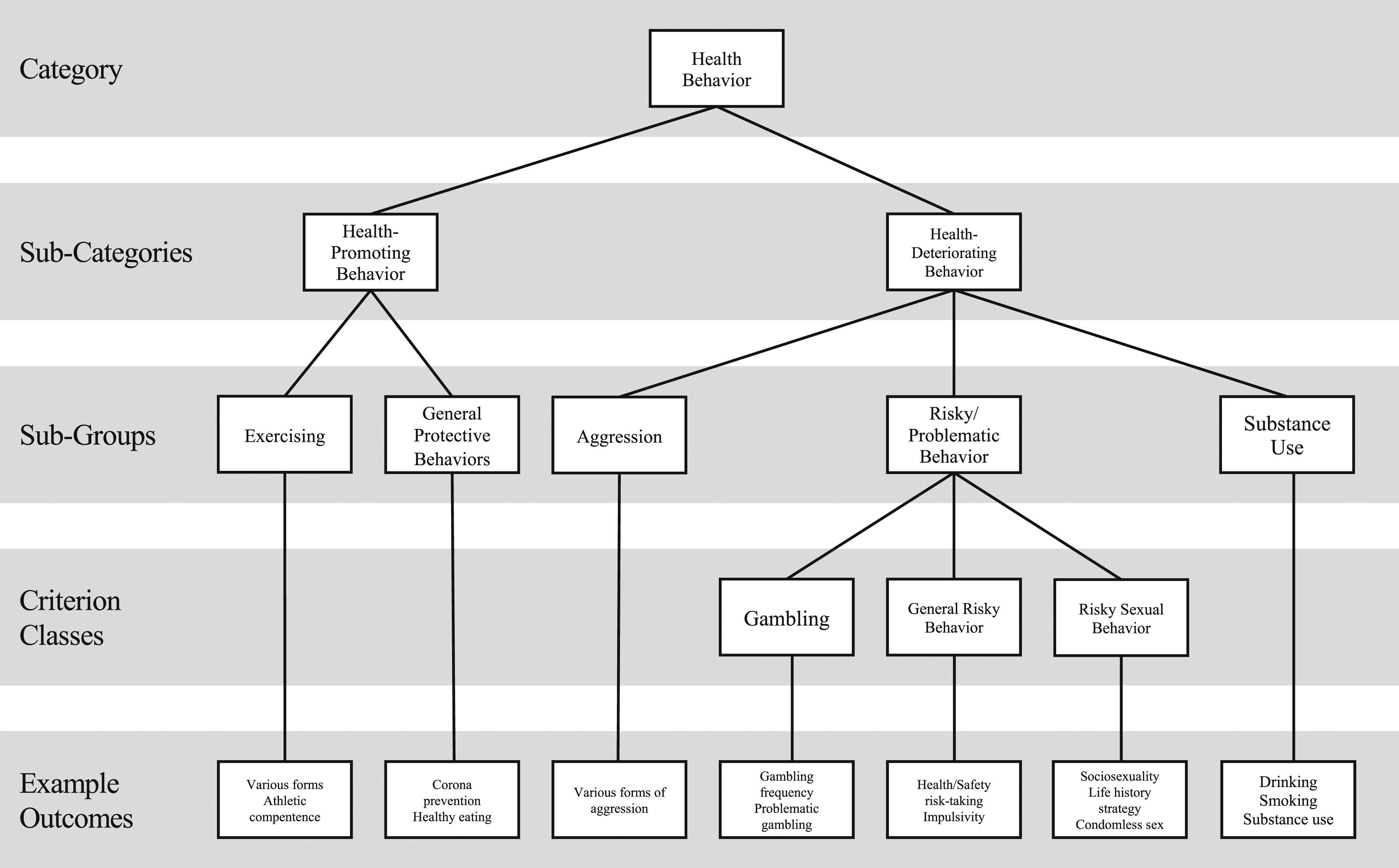
We also created sub-categories, sub-groups, and criterion classes for the three overarching health categories to yield meaningful analyses across criteria. To create and further categorize criteria, we followed a similar procedure as described above for assigning criteria to one of the three main categories: The first author formed initial sub-categories, sub-groups, and criterion classes after consulting relevant prior meta-analysis (e.g., Davis et al., 2015; Emmer et al., 2020; White et al., 2017) and based on data availability to allow meaningful analyses, which were then discussed with the second and third author until agreement was reached. Figures 2 (mental health) and 3 (health behavior) depict an overview of all categories, sub-categories, sub-groups, criterion classes, and example outcomes. We did not include a figure for physical health because we only meta-analyzed one sub-category (i.e., physical fitness) for this category. Category overview for mental health. Note. Example outcomes include the most commonly studied outcomes. Category overview for health behavior. Note. Example outcomes include the most commonly studied outcomes.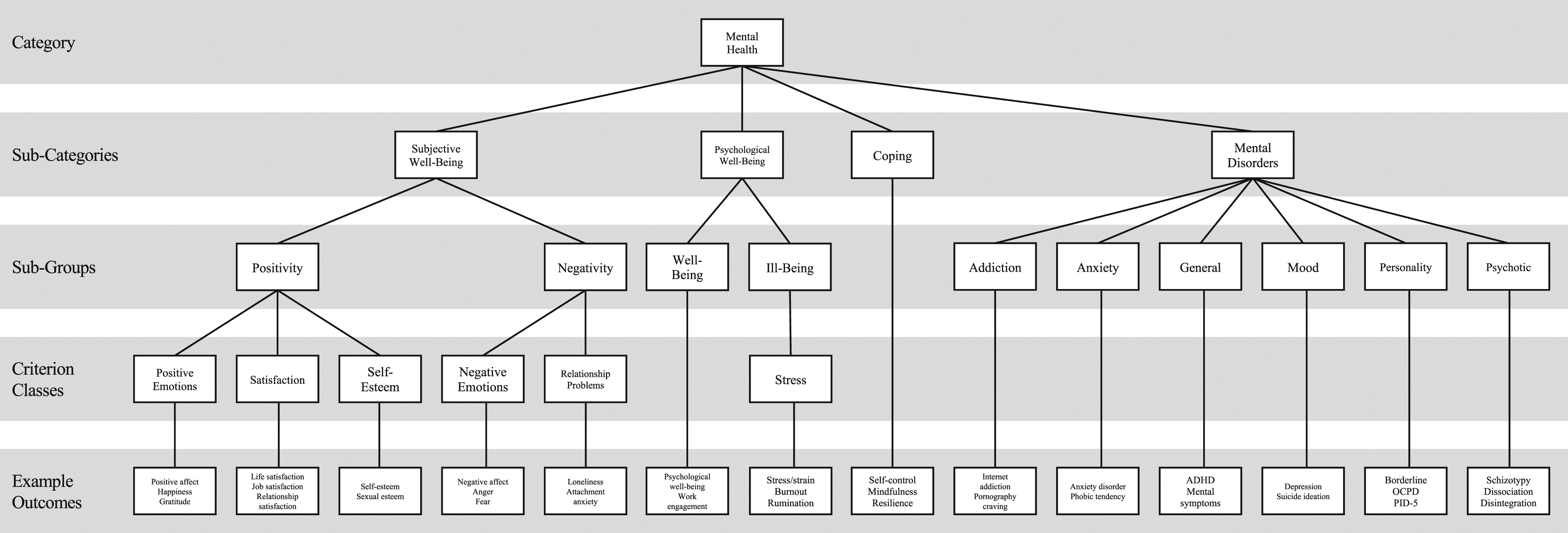
Analytic Procedures
All analyses are based on Pearson’s product-moment correlation coefficient r. If a study reported other effect sizes (e.g., standardized regression coefficients, Cohen’s d), we transformed those to r using appropriate formulas (Borenstein et al., 2009). We analyzed the data in a random-effects model weighted by sample size according to the Hunter and Schmidt (2004) meta-analytic approach as implemented in the R package metafor (Viechtbauer, 2010). We corrected effect size estimates for unreliability in both the predictor and the criterion using local internal consistency estimates (i.e., Cronbach’s alpha values from the included studies). When the internal consistency estimate of a measure was not reported in a document, we conservatively assumed perfect reliability (i.e., α = 1). When a range of alphas was reported, we conservatively coded the highest value. 6
To guarantee the independence of effect sizes, we aggregated effect sizes to the higher-order health category if a study contributed multiple effect sizes based on the same sample, accounting for the intercorrelation of the criteria (Hunter & Schmidt, 2004). If the intercorrelation was not available, we assumed perfect redundancy (r = 1). We corrected aggregate effect sizes with the average internal consistency estimate across aggregated criteria. When a study reported effect sizes for both self- and other-ratings of a given variable (e.g., Ashton et al., 2008), we also aggregated these effect sizes following the same procedure.
We report the number of included independent samples (k), the associated sample size (N), the corrected meta-analytic effect size estimate (
Studies with statistically significant results are more likely to be published (Borenstein et al., 2009), which can inflate meta-analytic effect size estimates. Thus, we intended to include as much data as possible from unpublished sources. However, publication bias might nevertheless be present in our data. To detect publication bias, we conducted Egger et al.'s (1997) regression intercept test. Significant results indicate publication bias.
Results
In total, we included 205 different health outcomes (133 mental health, 64 health behavior, and 8 physical health outcomes). We meta-analyzed relations of all HEXACO domains with (i) mental health, health behavior, and physical health; (ii) seven health sub-categories (four mental health, two health behavior, and one physical health); (iii) sixteen sub-groups (ten mental health, five health behavior, and one physical health); and (iv) nine criterion classes (six mental health and three health behavior). At the level of individual health outcomes, we further provide meta-analytic effect size estimates for at least one of the HEXACO domains with 59 outcomes (39 mental health, 18 health behavior, and 2 physical health outcomes). Overall, the meta-analytic correlations are based on data from 231 documents including 276 independent studies, 4462 effect sizes, and 92,319 participants (see Table 2 for details). The majority of included documents were journal articles (k = 171), but we also included dissertations (k = 44) and conference proceedings or pre-prints/unpublished data (k = 12). Studies came from 34 different countries with most of them being conducted in the United States (k = 81) or Canada (k = 34). The vast majority of included studies relied on self-reports rather than observer reports to assess the HEXACO domains (272 out of 276) and used the 60-item HEXACO measure (k = 175), followed by the 100-item (k = 72) and the 200-item HEXACO-PI-R (k = 19).
Relations of the HEXACO Domains with Health Categories
Meta-Analytic Results for the Relations of the HEXACO Domains with Mental, Behavioral, and Physical Health.
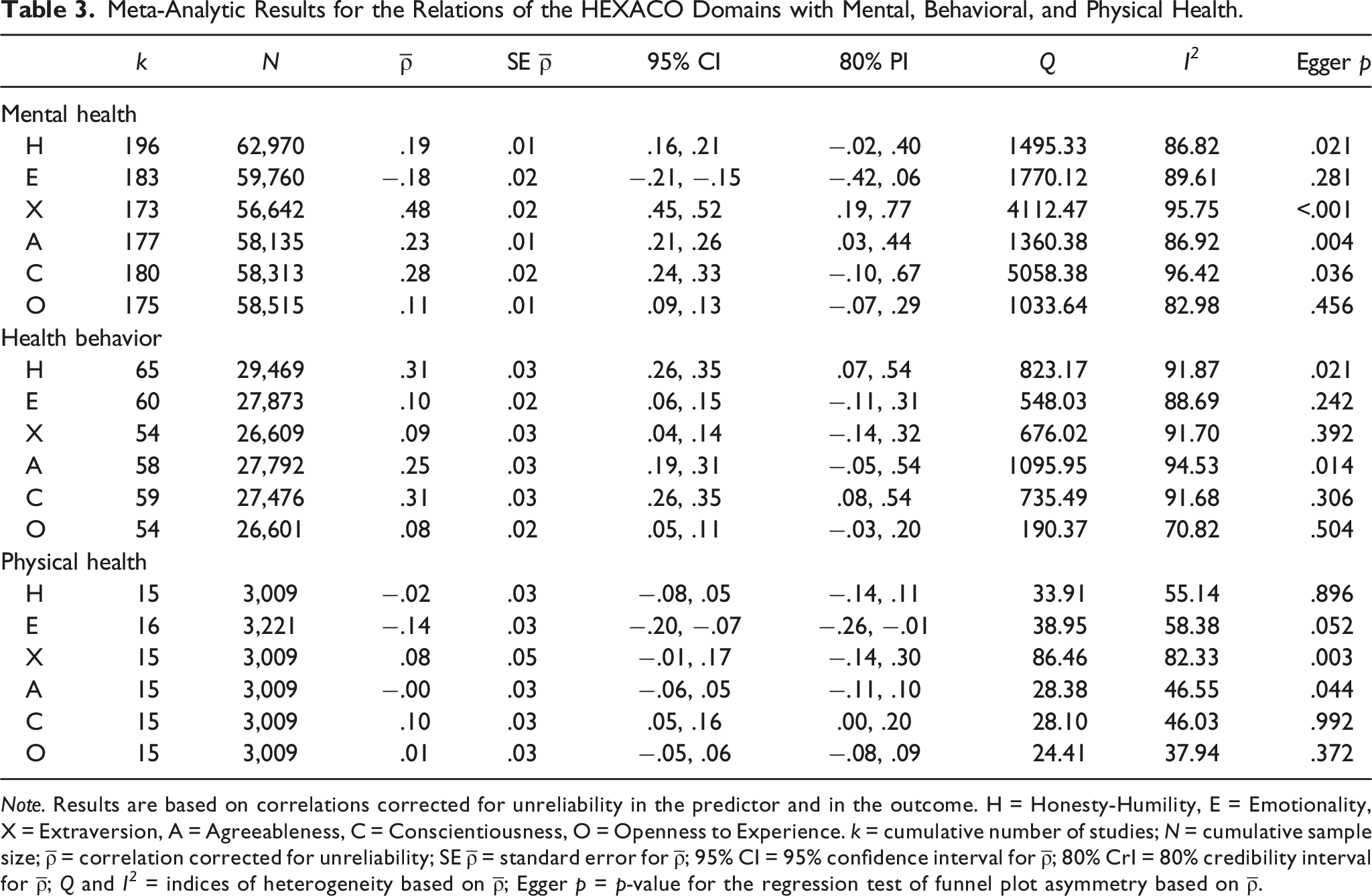
Note. Results are based on correlations corrected for unreliability in the predictor and in the outcome. H = Honesty-Humility, E = Emotionality, X = Extraversion, A = Agreeableness, C = Conscientiousness, O = Openness to Experience. k = cumulative number of studies; N = cumulative sample size;
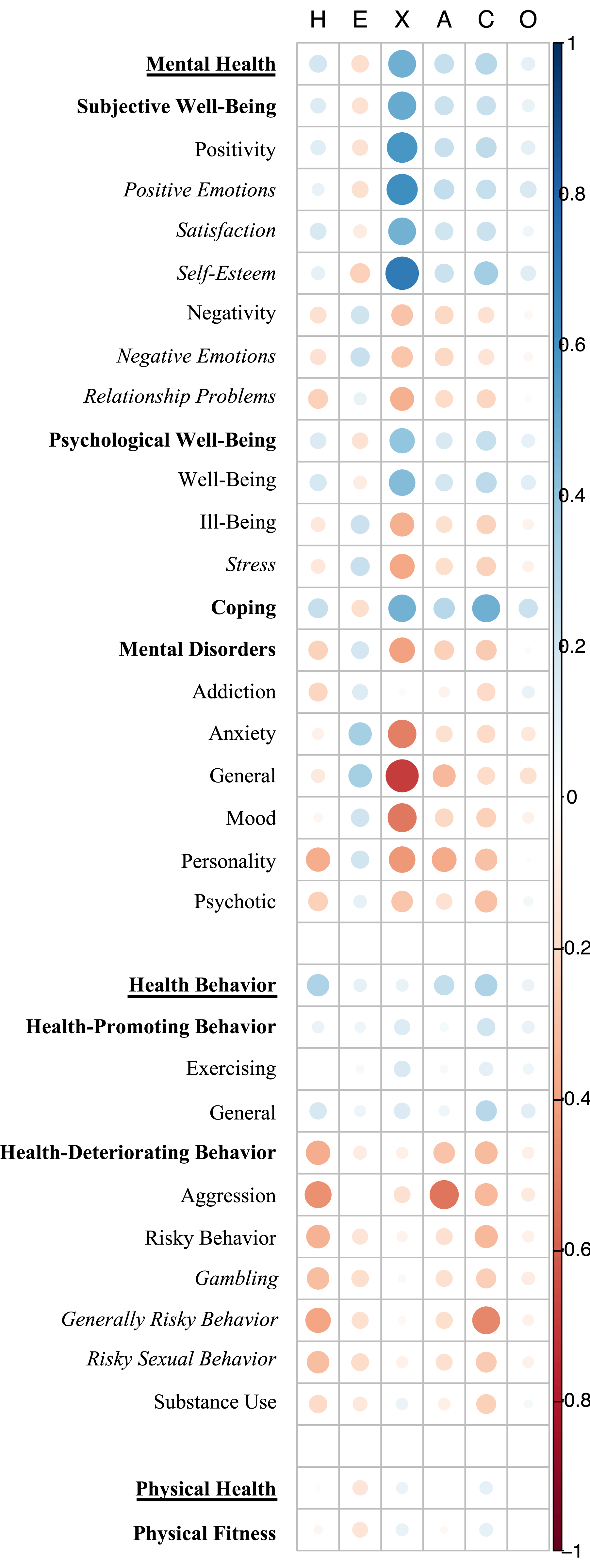
Graphical overview of the correlations of all HEXACO traits with the health categories, sub-categories, sub-groups, and criterion classes. Note. Categories are printed in
Correlations of the HEXACO domains with health behaviors were generally weaker. Honesty-Humility (
Surprisingly, for physical health, only Emotionality (
Several notes of caution need to be mentioned when interpreting these results. First, correlations with physical health are all based on a relatively small number of studies (15 ≤ k ≤ 16). Second, not all meta-analytic correlations exhibited validity generalization (i.e., 80% prediction intervals that exclude zero), demonstrating that there was high variability in the effect size distributions. Specifically, for mental health, only the correlations for Extraversion and Agreeableness exhibited validity generalization (i.e., 80% prediction intervals that excluded zero); for health behaviors, only the correlations of Honesty-Humility and Conscientiousness; and for physical health, only the correlations of Emotionality and Conscientiousness. Correspondingly, the Q and I
2
values of all analyses were high, indicating that moderators might be at play and that some of the correlations might even be reversed under certain circumstances. This likely happened because the specific health outcomes that we subsumed in the three overarching health categories showed differential relations with the same HEXACO domain. For example, Honesty-Humility correlated only weakly with the mental health outcome happiness (
Relations with Mental Health Outcomes
Extraversion exhibited consistently strong relations with the four mental health sub-categories subjective well-being (
Correlations of the HEXACO domains with the subjective well-being sub-groups positivity and negativity (see Supplementary Table 3) were, as expected, in opposite directions and generally of similar magnitude, with one notable exception: Extraversion correlated more strongly with positivity (
Correlations of the HEXACO domains with the psychological well-being sub-groups well-being and ill-being were also in opposite directions and of similar magnitude, although the difference in correlations for Extraversion was less notable (
There were no further sub-groups for the coping sub-category, but we separately examined six different mental disorder sub-groups (i.e., addiction, anxiety, general, mood, personality, and psychotic disorders; see Supplementary Table 3). Honesty-Humility exhibited the strongest negative correlations with personality disorders (
Relations with Health Behavior Outcomes
For health behavior, we created the two sub-categories health-promoting behavior and health-deteriorating behavior. Correlations of the HEXACO domains were generally stronger for health-deteriorating than for health-promoting behavior. All HEXACO domains correlated negatively with health-deteriorating behavior, with Honesty-Humility (
We created three sub-groups (i.e., aggression, risky/problematic behavior, and substance use) for the health-deteriorating sub-category. Honesty-Humility (−.20 ≤
The health-promoting sub-category was further divided into two sub-groups (i.e., exercising and general protective behaviors). Results were highly similar to those for the broader health-promoting sub-category: Conscientiousness (
Finally, we examined three further criterion classes for risky/problematic behavior: Gambling, general risky behavior, and sexually risky behavior. We generally observed relatively little variance in the effect size distribution across these three criterion classes. Honesty-Humility (−.31 ≤
Relations with Physical Health Outcomes
For physical health, we only created one sub-category which is called physical fitness and which included variables such as physical health and physical strength. Only the meta-analytic correlations of Emotionality (
Explained Variance in Health
Explained Variance by the HEXACO Traits in Health Categories, Sub-Categories, and Criterion Classes.
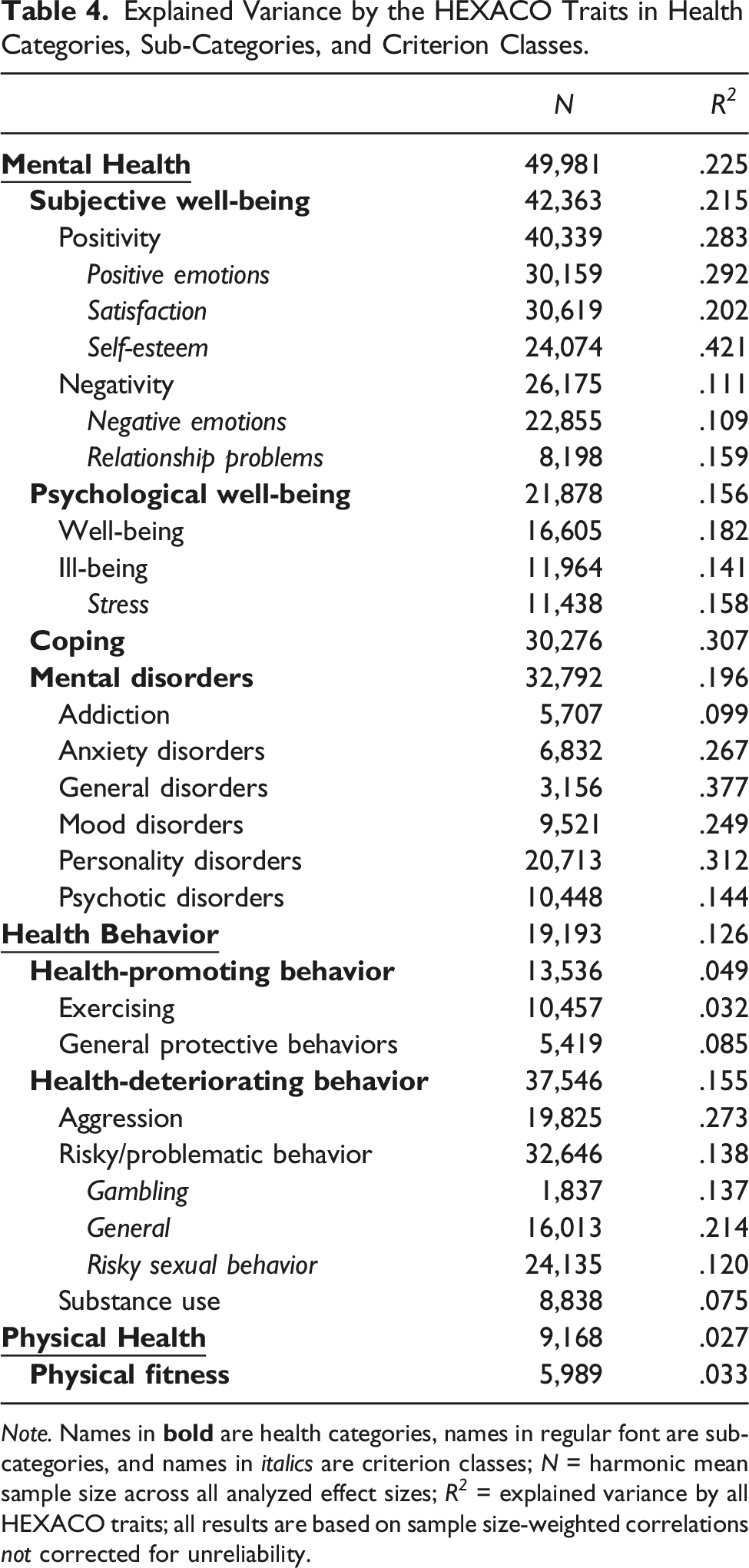
Note. Names in
Explained Variance in Specific Health Outcomes.
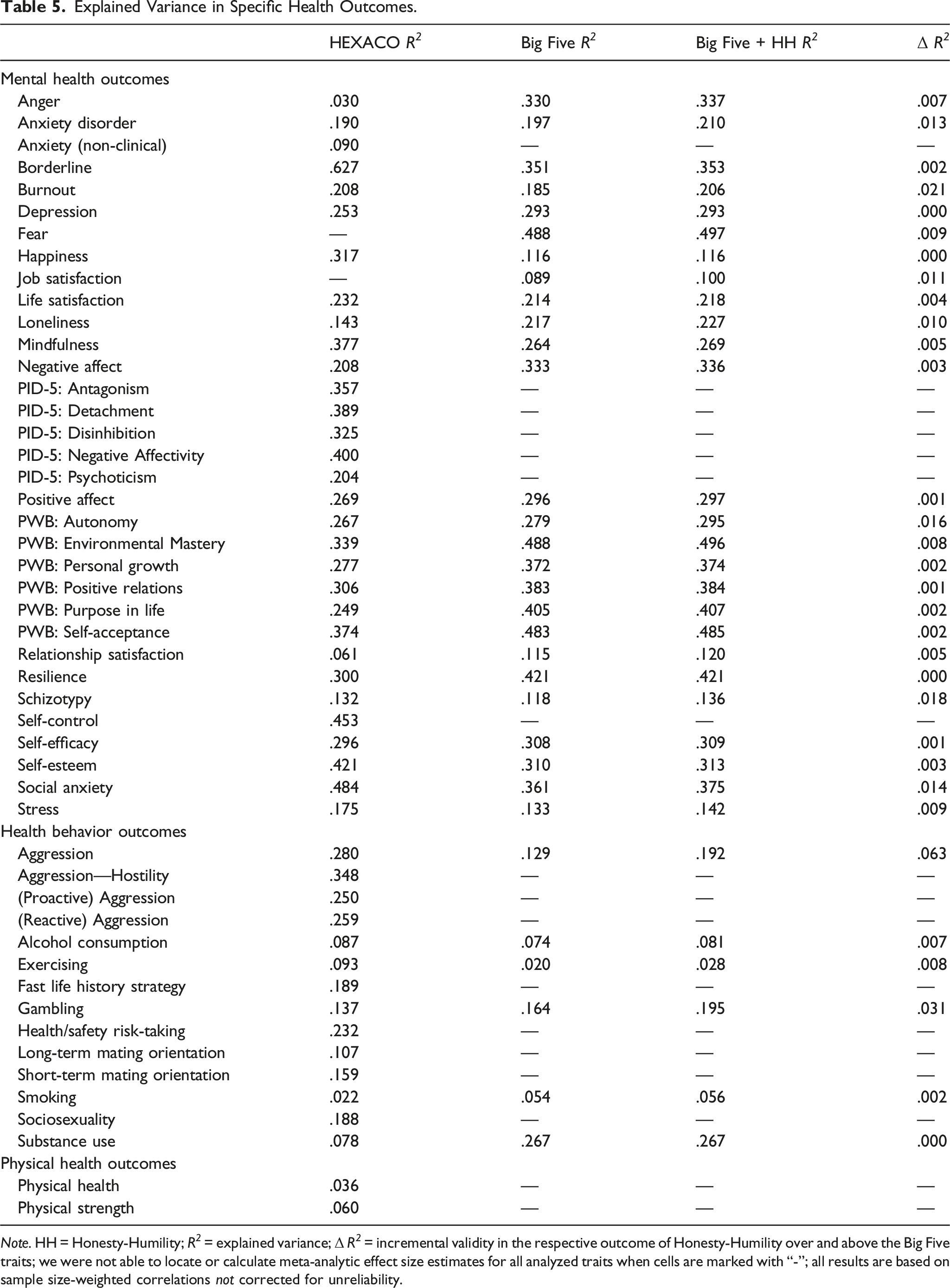
Note. HH = Honesty-Humility; R 2 = explained variance; Δ R 2 = incremental validity in the respective outcome of Honesty-Humility over and above the Big Five traits; we were not able to locate or calculate meta-analytic effect size estimates for all analyzed traits when cells are marked with “-”; all results are based on sample size-weighted correlations not corrected for unreliability.
The HEXACO domains explained more variance than the Big Five traits in borderline personality disorder (R 2 = .627 vs. R 2 = .351), happiness (R 2 = .317 vs. R 2 = .116), mindfulness (R 2 = .377 vs. R 2 = .264), self-esteem (R 2 = .421 vs. R 2 = .310), and social anxiety (R 2 = .484 vs. R 2 = .361). The Big Five domains explained more variance compared to the HEXACO domains in anger (R 2 = .030 vs. R 2 = .330), loneliness (R 2 = .143 vs. R 2 = .217), negative affect (R 2 = .208 vs. R 2 = .333), psychological well-being—environmental mastery (R 2 = .339 vs. R 2 = .448)/personal growth (R 2 = .277 vs. R 2 = .372)/positive relations (R 2 = .306 vs. R 2 = .383)/purpose in life (R 2 = .249 vs. R 2 = .405)/self-acceptance (R 2 = .374 vs. R 2 = .483), relationship satisfaction (R 2 = .061 vs. R 2 = .115), and resilience (R 2 = .300 vs. R 2 = .421). The domains from both models explained similar amounts of variance for the following mental health outcomes: anxiety disorders, burnout, depression, life satisfaction, positive affect, psychological well-being—autonomy, schizotypy, self-efficacy, and stress.
Honesty-Humility showed only weak incremental validity over the Big Five for specific mental health outcomes, ranging from 0.0% to 2.1%. Specifically, incremental variance was equal to or larger than 1% for burnout (2.1%), schizotypy (1.8%), psychological well-being—autonomy (1.6%), social anxiety (1.4%), anxiety disorders (1.3%), job satisfaction (1.1%), and loneliness (1.0%).
For specific health behaviors, the HEXACO domains explained more variance than the Big Five domains in aggression (R 2 = .280 vs. R 2 = .129) and exercising (R 2 = .093 vs. R 2 = .020), and less variance in substance use (R 2 = .078 vs. R 2 = .267). The HEXACO and Big Five domains explained similar amounts of variance in alcohol consumption, gambling, and smoking. Honesty-Humility had relatively high incremental validity over the Big Five domains for aggression (6.3%) and gambling (3.1%), only little incremental validity for exercising (0.8%), alcohol consumption (0.7%), and smoking (0.2%), and none for substance use.
We did not locate any Big Five meta-analyses for the two specific physical health outcomes that we included and so could not compare the corresponding amounts of variance explained.
Discussion
For decades, researchers have investigated which personality characteristics are associated with health. To summarize and extend prior research on this topic, we conducted a comprehensive meta-analysis of the health-related nomological net of the HEXACO personality domains, focusing specifically on criteria related to mental health, health behavior, and physical health. We also compared results for the HEXACO domains with those for the Big Five domains as observed in previous meta-analyses. By doing so, we add evidence on how basic personality domains relate to a broad array of health indicators, overcoming the predominant focus on the Big Five domains in past health research.
Based on data from 276 studies, we found that the HEXACO domains relate most strongly to mental health outcomes, such as borderline personality disorder or self-esteem, followed by health behavior outcomes, such as aggression or risk-taking. Relations with physical health outcomes (e.g., physical strength) were generally weak, but significant for Emotionality (negatively) and Conscientiousness (positively). Many findings for the HEXACO domains converged with those for the Big Five domains, but important differences also occurred, especially for those HEXACO domains that conceptually differ from the Big Five domains. Specifically, Honesty-Humility showed meaningful relations with many indicators of mental health and health behavior. However, it explained relatively little incremental variance over the Big Five domains in mental health outcomes, whereas it had noteworthy incremental validity for some indicators of health behavior (e.g., aggression and gambling). Both models had incremental validity over the other for certain health outcomes, which was, however, more often the case for the Big Five domains. By implication, the choice of which model to use when predicting health could be outcome-dependent.
How Well Do the HEXACO Domains Predict Health?
The current meta-analysis contributes to the literature in several ways. First, on the most general level, our findings add to the growing literature demonstrating that personality traits are related to health (Strickhouser et al., 2017). Referring to the HEXACO model in particular, our results show that consideration of the HEXACO domains can be useful when examining personality correlates of specific health outcomes. Specifically, relations of all HEXACO domains with mental health and health behavior were significant (and some even exhibited validity generalization), and Emotionality and Conscientiousness were even associated with physical health.
Second, and related to that, we found the HEXACO domains to predict mental health (R 2 = .225) moderately, whereas the amount of explained variance in health behavior (R 2 = .126) and especially in physical health (R 2 = .027) was lower. These findings align well with findings for the Big Five domains (Luo et al., 2022; Strickhouser et al., 2017), and therefore seem to be largely independent of the utilized personality framework. One interpretation of these findings is that personality domains affect the appraisal of events (Lazarus, 1999), which likely matters more for mental health than for health behavior and physical health. This is in line with the idea that the relatively high conceptual correspondence between personality traits as psychological constructs and mental health can likely explain why personality traits relate more strongly to psychological health-related processes than to actual health-related behaviors or physical health outcomes. Further evidence for this idea comes from some of the outcome-specific findings in the current meta-analysis. For example, Extraversion—an indicator of being enthusiastic and gregarious—correlated more strongly with outcomes of the same valence as combined in the positivity sub-category than with outcomes of opposite valence as combined in the negativity sub-category. Similarly, Emotionality correlated more strongly with negative than with positive affect.
Importantly, a more critical interpretation suggests that the large amount of variance explained in mental health can be attributed to conceptual overlap, which might explain the strong relation between personality and mental health. One reason for this conceptual overlap is common method variance (Podsakoff et al., 2012) as both personality domains and mental health outcomes are usually assessed via self-reports. Another reason is item overlap between personality and (mental) health measures. For example, some items assessing Extraversion (e.g., “On most days, I feel cheerful and optimistic”) closely resemble items assessing mental health outcomes, such as life satisfaction (e.g., “I am satisfied with my life”) or positive affect (e.g., being “excited” or “enthusiastic”). Further, some HEXACO facets, such as the anxiety facet of Emotionality or the social self-esteem facet of Extraversion, overlap strongly with some of the included outcomes (e.g., anxiety disorder and self-esteem). To reduce the influence of common method variance and item overlap, future research should rely on other-reports of personality or use more objective assessments of health, such as observations or biomarkers (Pratt & Hall, 2018).
Nevertheless, it is unlikely that the difference in the amount of explained variance between mental health and health behavior/physical health can be fully attributed to common method variance or item overlap. After all, even seemingly small effect sizes for physical health can have non-trivial, practical relevance for important outcomes such as the onset of diseases or mortality (Graham et al., 2017; Turiano et al., 2015). In addition, (small) effects can be amplified or counteracted by different mechanisms (Anvari et al., 2022). For example, professional medical help or social support can likely buffer the negative relations of Emotionality with mental and physical health, whereas interventions specifically designed for individuals with certain personality traits might promote health behaviors among those individuals (Chapman et al., 2014; Conrod, 2016).
Which HEXACO Domains Are the Best Predictors of Health?
Taken together, Conscientiousness was the only HEXACO domain that significantly predicted all three health categories, and it also significantly predicted most of the specific mental health (32 out of 37), health behavior (12 out of 14), and physical health outcomes (1 out of 2). Conscientiousness can therefore be considered one of the most important personality characteristics when it comes to a healthy life, which aligns well with findings highlighting the relevance of Conscientiousness in a wide variety of other important domains of life, such as at school or university (Poropat, 2009), at work (Wilmot & Ones, 2019), or in interpersonal relationships (Malouff et al., 2010). Zooming in on specific mental health outcomes, it becomes apparent that Conscientiousness correlates to a similar extent with most mental health outcomes, the only exception being a somewhat stronger positive correlation with coping. This finding corresponds with Big Five meta-analyses that generally found similar relations of Conscientiousness with most mental health outcomes (e.g., Buecker et al., 2020; Giluk, 2009; Kotov et al., 2010), but slightly stronger correlations with coping-related outcomes, such as resilience or self-efficacy (Barańczuk, 2021; Oshio et al., 2018). HEXACO Conscientiousness also correlated similarly with most health behaviors, which largely converges with past meta-analytic findings for Big Five Conscientiousness (e.g., Dudfield et al., 2022; Jones et al., 2011).
Extraversion emerged as the overall strongest predictor of mental health, but it predicted health behavior only weakly and failed to predict physical health. The particularly strong relation with mental health is one of the most notable findings of the current meta-analysis. Arguably, one reason for this finding is that we defined mental health very broadly, including several outcomes that are conceptually strongly related to Extraversion (e.g., positive affect and optimism). Then again, Extraversion exhibited similar correlations with almost all mental health outcomes, including more distant outcomes, such as borderline disorder, mindfulness, or self-efficacy.
7
This general pattern has likewise been observed for Big Five Extraversion, although corresponding meta-analytic correlations (e.g., Alarcon et al., 2009; Barańczuk, 2021; Giluk, 2009) are generally weaker than those for HEXACO Extraversion observed here. Interestingly, HEXACO Extraversion also had incremental validity over and above the Big Five domains for several specific (mental) health outcomes (see Table 15 in the supplementary materials). This is surprising given that HEXACO and Big Five Extraversion strongly converge on the domain level (Thielmann et al., 2022), but converges with findings by Anglim et al. (2020) who also found stronger relations for HEXACO Extraversion, compared to its Big Five counterpart, with subjective and psychological well-being. One explanation can be based on findings by Watson and Clark (2020), who showed that the social self-esteem facet of HEXACO Extraversion correlates particularly strongly with the depression facet of Neuroticism in some Big Five models, suggesting potential differences between Big Five and HEXACO Extraversion. This facet can be an important predictor of various mental health outcomes. It is therefore also not surprising that HEXACO Extraversion exhibits relatively strong correlations with mental health outcomes such as anxiety disorders (
The relatively weak correlation of Extraversion with health behavior can be explained by the fact that Extraversion correlated positively with both health-deteriorating (e.g., alcohol consumption and substance use) and health-promoting behaviors (e.g., exercising), likely because extraverted individuals are more inclined to engage in social activities which can take a healthy (e.g., exercising together) or an unhealthy form (e.g., drinking together). These behaviors might cancel each other out, resulting in an overall weaker relation with health behavior. Assuming that health behaviors drive physical health, these cancellation effects with specific health behaviors might also explain the non-significant relation of Extraversion with physical health.
Honesty-Humility predicted mental health and health behavior significantly, but failed to predict physical health. Relations of Honesty-Humility with specific mental health categories and outcomes were relatively weak and similar in magnitude. Interestingly, Honesty-Humility did not correlate significantly with mood disorders, but showed a relatively strong correlation with personality disorders. This finding aligns with research highlighting the role of personality disorders in predicting higher levels of dishonest and criminal behavior (R. C. Howard et al., 2008; Menon & Sharland, 2011) and lower levels of prosocial behavior (Thielmann et al., 2014), of which Honesty-Humility is among the strongest trait-based predictors (Pletzer et al., 2019; Thielmann et al., 2020). This might occur because both overlap substantially with aversive (dark) personality traits (Hodson et al., 2018; M. C. Howard & Van Zandt, 2020; Moshagen et al., 2018; Scholz et al., 2022). In turn, the relation of Honesty-Humility with health behavior was stronger than the one with mental health. This can be explained based on the nature of some of the included behavioral outcomes, such as aggression, gambling, or sexual risk-taking, which all contain a negative moral connotation and sometimes even involve deviant and/or norm-violating behavior. Honesty-Humility is a particularly strong predictor of such deviating behaviors (Pletzer et al., 2019; Zettler et al., 2020). Other health behavior outcomes that might have less of a moral connotation, such as eating healthy or regular visits to a physician, were not represented well in the current meta-analysis, and most of the included mental health outcomes also do not have a strong negative moral connotation. These differences in criteria might explain why Honesty-Humility correlated more strongly with health behavior than with mental health, and it might also explain the non-significant relation of Honesty-Humility with physical health.
Relations of Emotionality with the three health categories even differed in direction: Emotionality correlated negatively with mental and physical health, but positively with health behavior. The negative relation with mental health is in line with the central role of negative emotions, such as fearfulness and anxiety, for both high levels of Emotionality and mental health. These findings also generally align with prior results for Big Five Neuroticism (Strickhouser et al., 2017), suggesting that it is the shared personality variance of these two domains (e.g., anxiety and fearfulness) that can explain relations with mental health. The positive relation of Emotionality with health behavior, in turn, was largely driven by a negative relation with risky, health-deteriorating behaviors. For example, individuals scoring high on Emotionality were less likely to consume alcohol, gamble, or engage in risky, short-term sexual practices. Thus, the over-representation of risky behaviors in the studies included in our meta-analysis might explain why Emotionality correlated positively with health behavior. Of note, Big Five Neuroticism has been shown to correlate positively (rather than negatively) with risky health behaviors, such as gambling and substance use (Dudfield et al., 2022; Kotov et al., 2010). This can arguably be attributed to Neuroticism capturing anger- and sadness-related personality variance that is not captured by Emotionality in the HEXACO framework. Past research shows that both sadness/depression and anger exhibit high levels of comorbidity with problematic gambling and substance use (Boden & Fergusson, 2011; Korman et al., 2008; Quigley et al., 2015), which may explain why Emotionality and Neuroticism correlate in opposite directions with health behavior. It should also be mentioned that Emotionality was the only other domain, next to Conscientiousness, that was significantly associated with physical health (negatively). Apparently, the health behaviors under investigation in the current meta-analysis do not translate into benefits for physical health, again indicating that either the included physical health measures were insufficient to capture the true extent of participants’ physical health or that the included health behavior measures were biased towards those that are strongly predicted by Emotionality.
Agreeableness correlated similarly with mental health and health behavior (yielding small to medium-sized effects), but not significantly with physical health. This domain generally exhibited relatively similar, moderate correlations with most of the specific mental health outcomes included in our meta-analysis, which converges with findings for Big Five Agreeableness (Strickhouser et al., 2017). Correlations with specific health behavior outcomes, by contrast, varied more: Agreeableness was particularly predictive of health-deteriorating behavior, a relation that was especially driven by the strong negative correlation with aggression-related behaviors, but less predictive of health-promoting behaviors, such as exercising and general protective behaviors. These relations of different magnitude mask or cancel each other out when being combined to overall health behavior. Again, these findings resemble those for Big Five Agreeableness, which has been shown to correlate negatively with health-deteriorating behaviors such as aggression (Jones et al., 2011) and substance use (Kotov et al., 2010), but less so with health-promoting behaviors such as exercising (Wilson & Dishman, 2015) or walking speed (Stephan et al., 2018). 8 Together, these findings demonstrate that it is most likely the shared variance among Big Five and HEXACO Agreeableness (i.e., forgivingness and gentleness) that can explain relations with mental health and health behavior. Finally, HEXACO Agreeableness seems to be unrelated to physical health, but this finding is limited to the physical health outcomes included in the current meta-analysis, and relations with other markers of physical health should be examined in the future. For example, past research has found that Big Five Agreeableness predicts adherence to medication (Axelsson et al., 2011), which likely has direct consequences for physical health.
Openness to Experience was the weakest predictor of health. It only exhibited weak correlations with mental health and health behavior, and it did not significantly correlate with physical health. Apparently, being creative, open-minded, and unconventional is not particularly relevant for being healthy. Zooming in on the different mental health categories and outcomes, it is apparent that only two exceptions to this general pattern of findings occurred: Openness to Experience was more strongly related to coping outcomes, such as resilience and self-control, and to psychological well-being. Both findings mirror previous evidence for Big Five and HEXACO Openness to Experience (Anglim et al., 2020; Oshio et al., 2018). Relations of Openness to Experience with health behavior all hovered around zero, which is also in line with prior evidence for the Big Five (e.g., Lui et al., 2022; Wilson & Dishman, 2015). The same holds for relations with physical health outcomes (Strickhouser et al., 2017).
Should One Use the HEXACO or the Big Five in Health Research?
When comparing the criterion-related validity of the HEXACO domains with that of the Big Five domains for specific health outcomes, the question whether to prefer the HEXACO or Big Five domains for the prediction of health cannot be clearly answered. For some mental health outcomes—borderline personality disorder, happiness, mindfulness, stress, and self-esteem—the HEXACO domains outperformed the Big Five domains in predictive power. For other mental health outcomes, such as anger, negative affect, and resilience, the Big Five domains outperformed the HEXACO domains in predictive power. And for yet other mental health outcomes, such as anxiety disorder, burnout, and schizotypy, both personality models explained similar amounts of variance. A similar pattern was apparent for health behaviors: For some criteria, the HEXACO domains were more predictive (e.g., aggression and exercising), for other criteria, the Big Five domains were more predictive (e.g., substance use), and for even others, both models performed equally well (e.g., alcohol consumption, gambling, and smoking). 9 These results can thus guide researchers and practitioners when deciding which personality model to rely on in their work. If the aim is to predict outcomes particularly well, the choice should be outcome-dependent as each model exhibited superior criterion-related validity for some outcomes. However, the Big Five model more often showed higher criterion-related validity for specific health outcomes than the HEXACO model. One possible reason for this is that the HEXACO model may not capture personality variance associated with sadness/depressiveness, which seems relevant for many health outcomes, as well as the Big Five model. Another possibility is that item overlap, as discussed above, is more pronounced for the Big Five than for the HEXACO model. For example, items used to capture the sadness/depressiveness content of Big Five Neuroticism (e.g., “often feels sad” from the BFI-2; Soto & John, 2017) may strongly overlap with items commonly used to assess mental health outcomes such as burnout or depression.
We also examined whether Honesty-Humility has incremental validity for health over the Big Five domains. Past research has shown that Honesty-Humility has incremental validity for certain outcomes, such as counterproductive work behavior, but not for others, such as task performance (Y. Lee et al., 2019). This is also mirrored in the current results: Honesty-Humility had incremental validity for a few health behavior outcomes, but not for many mental or physical health outcomes. Among the 25 specific mental health outcomes for which the incremental validity of Honesty-Humility could be examined, Honesty-Humility never explained more than 1.8% of additional variance over the Big Five. By contrast, Honesty-Humility explained 6.3% of incremental variance over the Big Five in aggression and 3.1% of incremental variance in gambling, which are both health behaviors. For other health behaviors (e.g., alcohol consumption, exercising, and smoking), Honesty-Humility explained only little to no incremental variance. These findings suggest that the usefulness of Honesty-Humility in the health arena is largely confined to health-deteriorating behaviors. It is also worth noting that HEXACO Extraversion had incremental validity over and above the Big Five for many specific mental health (e.g., depression, mindfulness, and self-esteem) and health behavior outcomes (e.g., exercising and substance use), which might be due to facet-level differences between HEXACO and Big Five Extraversion (see above; Watson & Clark, 2020). Emotionality, Agreeableness, and Conscientiousness also explained incremental variance over and above the Big Five in some specific health outcomes (see Table 15 in the supplementary materials), suggesting that the differential partitioning of personality trait variance across the HEXACO and Big Five model affects relations with health. Researchers and practitioners can use these findings to optimize prediction of specific health outcomes.
Limitations and Directions for Future Research
The current findings should be viewed in light of the following limitations. First, we included an unequal number of effect sizes for specific health outcomes in the overall mental health, health behavior, and physical health analyses. For example, we included many studies assessing life satisfaction (k = 38–40) and negative affect (k = 20–25), but relatively fewer studies assessing anxiety disorders (k = 3–4) or burnout (k = 3–7). Thus, when combining these effect sizes to higher-order categories (e.g., mental health), relations for life satisfaction and negative affect influence the overall mental health effect sizes more strongly than relations for anxiety disorders or burnout. As a consequence, effect sizes in higher-order categories are biased towards outcomes that are better represented in the current data.
Second, we generally excluded outcomes that do not have a linear relation with health (e.g., perfectionism). That being said, one could argue that some of the outcomes that we included also exhibit a non-linear relation with overall health, although only at extreme levels. For example, although exercising behavior is generally beneficial for overall health, too much of it can result in injuries, thereby (temporarily) harming overall health. Similar arguments can be made for weight: Being overweight is certainly detrimental for overall health, but too little weight can be equally detrimental. Arguably, however, the included outcomes are, for most individuals, linearly related to health. Nonetheless, future research may benefit from a more nuanced examination that takes the non-linearity of certain personality-health relations into account.
Third, the majority of included studies are characterized by an over-reliance on self-reports to assess both the HEXACO domains and health. For example, there were no studies that actually assessed longevity or mortality, which are generally assumed to be the best markers of health (Friedman & Kern, 2014). Similarly, very few studies assessed diagnosed physical diseases. These limitations emphasize the fact that more research is needed that links the HEXACO domains—or personality traits more generally—to objective health measures. Moreover, future research may also examine whether the current findings can be corroborated with other HEXACO measures, such as the Brief HEXACO Inventory (De Vries, 2013) or the Honesty-Humility scale of the (Mini-)IPIP6 (Milojev et al., 2013).
Fourth, we initially intended to compare the criterion-related validity of the Big Five domains with that of the HEXACO domains for the categories mental health, health behavior, and physical health using the results from Strickhouser et al. (2017). However, we refrained from conducting these analyses because Strickhouser et al. (2017) included certain outcomes that could not be included in our meta-analysis due to insufficient data (e.g., accidents, all-cause mortality), and we, in turn, included outcomes that were not included in their meta-analysis (e.g., burnout, gambling, and psychological well-being). In addition, Strickhouser et al. (2017) report average correlations whereas we report sample size-weighted meta-analytic correlations, highlighting important differences in the chosen analytic approach. These differences would essentially render comparisons on the category-level invalid.
Finally, a methodological limitation arises from the fact that we corrected effect sizes using Cronbach’s alpha, which constitutes a lower-bound estimate of reliability (Sijtsma, 2009). Effect sizes corrected for unreliability using Cronbach’s alpha might therefore overestimate true effects. We nevertheless relied on this practice because Cronbach’s alpha is commonly reported (as opposed to, for example, test-retest reliabilities) and also consistently used to correct for unreliability in other meta-analyses. Of note, the main conclusions of the current meta-analysis are the same when correcting effect sizes based on test-retest reliabilities of the HEXACO domains as reported by Henry et al. (2022) (detailed results can be found in the supplementary materials). Whenever possible, however, future meta-analyses should correct effect sizes using test-retest reliabilities. This is especially important for shorter measures, such as those for personality facets, that are usually characterized by lower Cronbach’s alpha values.
Besides that, other issues are worthy of investigation in the future. First, given that the vast majority of included studies relied on cross-sectional study designs, it is difficult, if not impossible, to distinguish between personality traits as risk or beneficial factors for health or as derivations or even as consequences of health. One might argue that personality is generally considered to be exogenous, and several causal links between personality traits and health have indeed been suggested and tested (Ferguson, 2013; Kern & Friedman, 2011). For example, personality might affect the situations and environments individuals enter or the relationships they maintain, which can ultimately affect overall health. However, major life events, such as the experience of an injury or the onset of a life-threatening disease, may indeed change personality traits (Bleidorn et al., 2018; Haehner et al., 2021), offering an alternative interpretation of our findings. Personality traits might also shape the appraisal of and reaction to major life events (Connor-Smith & Flachsbart, 2007), which could then impact overall health. Moreover, it is conceivable that our findings may be confounded by age and sex/gender: Age-related development of and sex/gender differences in HEXACO domains are well-documented (Ashton & Lee, 2016; K. Lee & Ashton, 2020; Moshagen et al., 2019; Pletzer, 2021), and both age and sex/gender relate to overall health (Afifi, 2007; Gordon et al., 2017; World Health Organization, 2015). However, previous meta-analyses (e.g., Buecker et al., 2020; Chew, 2022; Marengo et al., 2020) have generally found inconsistent evidence for the moderating roles of age and sex/gender on personality-health relations. In addition, correlations of age and sex/gender with personality traits are generally smaller in magnitude than personality-health correlations, suggesting that age and gender cannot fully explain the personality-health relations. Yet, more research adopting a lifespan perspective is needed to disentangle the complex interplay between personality traits and health, and how this might be affected by age and sex/gender.
Second, the current meta-analysis focused exclusively on individual health outcomes, while health can also be considered a social or societal phenomenon. Future research should examine how personality traits of (groups of) individuals can affect group-level or societal health outcomes, such as adherence to health-protecting measures that prevent the spread of diseases (e.g., wearing facemasks during the COVID-19 pandemic; e.g., Zettler et al., 2022). Third, although substantial theoretical and empirical work has investigated the different pathways that can explain the relations of personality with different health outcomes (Ferguson, 2013; Friedman & Kern, 2014), this has not been examined for the HEXACO domains. Here, it might be especially worthy to investigate how and why Honesty-Humility shapes health-related processes, and to examine the (reciprocal) relations between personality, mental health, health behavior, and physical health. At last, it is important to examine cancellation and masking effects (Pletzer et al., 2020, 2021), which occur if different facets of one domain exhibit differential, opposing relations with an outcome. For instance, we found that Emotionality correlates negatively with mental health but positively with health behavior, which is indicative of a cancellation effect if we were to aggregate effect sizes to overall health. Similar findings may emerge when examining facet-level relations with other health outcomes (Anglim et al., 2020). For example, it is conceivable that the fearfulness and anxiety facets of Emotionality are particularly predictive of anxiety or mood disorders, whereas the dependence facet may be less predictive thereof. Such effects should be investigated in future research.
Conclusion
Personality relates to health. The HEXACO domains generally related most strongly to mental health outcomes but also exhibited many significant relations with health behavior outcomes. Relations with physical health were either weak or non-significant. Honesty-Humility explained relatively little incremental variance over and above the Big Five domains in mental and physical health outcomes, but showed substantial incremental validity for certain health behaviors. No clear pattern emerged as to whether the Big Five or HEXACO domains were better predictors of specific health outcomes.
Supplemental Material
Supplemental Material - Who is healthier? A meta-analysis of the relations between the HEXACO personality domains and health outcomes
Supplemental Material for Who is healthier? A meta-analysis of the relations between the HEXACO personality domains and health outcomes by Jan Luca Pletzer, Isabel Thielmann, and Ingo Zettler in European Journal of Personality
Supplemental Material
Supplemental Material - Who is healthier? A meta-analysis of the relations between the HEXACO personality domains and health outcomes
Supplemental Material for Who is healthier? A meta-analysis of the relations between the HEXACO personality domains and health outcomes by Jan Luca Pletzer, Isabel Thielmann, and Ingo Zettler in European Journal of Personality
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Accessibility Statement
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.