
Abstract
Becoming a parent could be expected to affect personality development, but the existing results on parenthood-personality change connection are mixed. The present study investigated 2445 primi- and multiparous mothers’ facet- and domain-level changes in Neuroticism and Extraversion from early pregnancy to 6 months post-partum, using latent difference score models. The results showed that Excitability and the affective facets of Neuroticism decreased, and the Neuroticism facets Impulsivity and Self-Consciousness increased during the follow-up. Furthermore, mother-perceived child difficult temperament attenuated desirable personality change and amplified the increases in Impulsivity. The results suggested that considering facet-level changes in personality development across significant life events is informative, and that mother-perceived child temperament may represent an important moderator of short-term personality change across the transition to parenthood.
Becoming a parent can be considered as one of the most profoundly life-changing events. In line with this, the transition to parenthood has been suggested to have a considerable potential to affect personality development and change (e.g. Bleidorn, 2015; Hutteman et al., 2014). In particular, it could be expected that parenthood would predict personality development into a more mature and positive direction (e.g. Roberts & Wood, 2006). However, in spite of its theoretical plausibility, no clear support for the hypothesis that parenthood is related to mature changes in personality has emerged from the literature (e.g. Bleidorn et al., 2018). In fact, literature on personality and becoming a parent has yielded mixed and even contradictory results (e.g. Asselmann & Specht, 2020; Specht et al., 2011; van Scheppingen et al., 2016).
Several factors may contribute to the variability of the results on personality development related to the transition to parenthood (Bleidorn et al., 2018): length of the follow-up period, age of the child(ren) at the last measurement point, moderator variables (e.g. stressors, parents’ age, and socioeconomic situation), the complexity of parenthood in terms of new social roles (e.g. Specht et al., 2011), and the entanglement of selection, anticipation, and socialization effects of becoming a parent (e.g. Denissen et al., 2019; Luhmann et al., 2014), to name just a few. The present study aims to contribute to the parenthood and personality development literature by investigating short-term changes in the Five-Factor traits Extraversion and Neuroticism across the transition to parenthood among mothers. We investigate both trait- and facet-level change, thereby providing information about potential differences in change between different facets. Furthermore, we examine several moderators of change.
The current study focuses on two trait dimensions of the Five-Factor/Big Five model of personality: Extraversion and Neuroticism. These two traits were included into the present study due to the focus of the main study from where the data was obtained, the PREDO study, which main objective is to investigate the role of pre-eclampsia and prenatal stress on child’s psychological development. Thus, the choice of Extraversion and Neuroticism was not made with regards to the current research questions. Nevertheless, these two traits are highly relevant for parenthood experiences and for life–event-triggered personality development. First, parents’ neuroticism has been repeatedly connected to challenges in parenting, such as less warm and sensitive parenting (e.g. Clark et al., 2000; Metsäpelto & Pulkkinen, 2003; Prinzie et al., 2009). Furthermore, in personality development literature, decline in Neuroticism is typically considered to represent personality maturation, desirable change that could be expected to happen as a result of becoming a parent (e.g. Roberts & Wood, 2006).
Regarding Extraversion, some studies suggest a particularly complex pattern of development for this trait with regards to having a child (e.g. Galdiolo & Roskam, 2012, 2014; Jokela et al., 2009), and as a function of age (Roberts et al., 2006) therefore, investigating the development of Extraversion at the facet level and with potential moderators is informative. Finally, Extraversion and Neuroticism are related to general tendencies toward positive and negative affectivity, respectively (e.g. Watson & Clark, 1992). Given the emotional potential of pregnancy, childbirth and early post-partum time in human life, it could be expected that Extraversion and Neuroticism as affective traits would be sensitive to these experiences. Thus, although it would be optimal to investigate all five major personality traits in relation to having a child, Extraversion and Neuroticism provide excellent candidate traits for the present purposes.
Personality development across transition to parenthood
We consider three theoretical models of personality development in adulthood that are particularly relevant for the current research: the Five-Factor model (e.g. McCrae & Costa, 1989), according to which personality trait changes are due to intrinsic biological maturation, and should therefore be relatively universal and mostly determined by age, with little or no effects by life events. The Five-Factor model would thus predict no changes as a function of becoming a parent. The Social investment theory (SIT; Roberts & Wood, 2006) suggests that becoming a parent may cause personality changes via adopting and investing in a new social role—that of a parent—that requires maturity. Thus, according to SIT, becoming a parent should be related to shifts toward maturity in personality. The TESSERA model (Wrzus & Roberts, 2017) specifies the process through which short-term behavioral, social and emotional processes may eventually lead to long-term, enduring changes in personality. In particular, life situations, such as having a newborn to take care of, may serve as triggers to change. Such triggers are then viewed—implicitly or explicitly—through the lens of expectancies, momentary motivational constructs derived from the relevant role (in this case, being the mother of a baby). This leads to the person adjusting their personality state expressions (e.g. expressing higher level of warmth than was previously typical) to match the situation perception created by the trigger and expectation, if such adjustment is deemed necessary. Finally, reactions to the adjusted state expression from oneself and from others or from the environment in general (e.g., the baby seems happy) guide the person to either keep up with or re-adjust the modified state expressions. According to the TESSERA model, repeated trigger-expectancy-state expression-reaction sequences in which state expressions are adjusted from previous levels eventually lead to personality development (Wrzus & Roberts, 2017).
The TESSERA and the SIT models are broadly compatible, both predicting personality changes in relation to life events if the person invests into the new roles created by the event (SIT), or repeatedly goes through the TESSERA sequence and changes their personality state expressions accordingly, which eventually leads to changes in self-views. By contrast, the Five-Factor model would not predict changes solely as a result of becoming a parent. The body of literature on personality development across the transition to parenthood is substantial but, as noted above, the results are mixed and do not offer clear support to any of the existing models, as discussed next.
Regarding Extraversion, studies have found decreases (Asselmann & Specht, 2020), decreases for fathers only (Galdiolo & Roskam, 2012, 2014), more complex change pattern for fathers (Jokela et al., 2009), and no changes (e.g. Neyer & Asendorpf, 2001; Specht et al., 2011; van Scheppingen et al., 2016) after having a child. With regards to Emotional Stability, some studies have found decreases (Denissen et al., 2019; Jokela et al., 2009) and quite a few have found no changes (Asselmann & Specht, 2020; Neyer & Asendorpf, 2001; Specht et al., 2011; van Scheppingen et al., 2016). Several studies have found decreases in Conscientiousness (Denissen et al., 2019; Pusch et al., 2019; Specht et al., 2011), but some studies found no changes (Neyer & Asendorpf, 2001; van Scheppingen et al., 2016). Most studies have found no changes for Openness and Agreeableness, with the exception of Pusch et al. (2019) who, in their sample of young and teen parents, found decreases in Openness, and Asselmann and Specht (2020), who found increases in Agreeableness for mothers. These studies had heterogeneous follow-up periods (from 1 year post-partum up to 9 years), but no obvious patterns related to length of follow-up time.
In sum, few general conclusions can be derived from the existing body of research. One methodological reason for this may be the use of brief personality questionnaires in most previous studies (e.g. Asselmann & Specht, 2020; Specht et al., 2011; van Scheppingen et al., 2016). Brief questionnaires typically work well in measuring broad traits (e.g. Thalmayer et al., 2011), but it is difficult to investigate potential differences in changes of lower level aspects of traits without longer measures. However, studying the development of facets across life transitions separately may be useful, as different facets changing into different directions could be one reason for the variable results. Studies following facet-level change have shown that at least Extraversion (Bleidorn et al., 2009; Terracciano et al., 2005), Neuroticism (Terracciano et al., 2005), and Openness (Schwaba et al., 2019) may have distinct trajectories across time at the facet level. Furthermore, in the Roberts et al. (2006) meta-analysis on normative personality development, Extraversion was divided into two lower level components (social vitality and dominance) that showed different development across age. Thus, there is evidence that lower level trait constructs may have different change trajectories. Finally, recent research and theorizing suggests that facets (and even lower level aspects of traits) have distinct relations with several outcomes (Mõttus, 2016; Mõttus et al., 2015; Sutin et al., 2011), supporting the idea that considering facets separately is informative.
Moderators of change
One prominent explanation for the varying results regarding parenthood and personality development is that individual differences in change play a role (e.g. Van Scheppingen et al., 2018). That is, stressors, challenges, resources, and different life situations before and during pregnancy, and after childbirth may moderate parenthood-related changes in personality. Considered from the theoretical perspective of SIT, stressors and challenges may complicate the process of investing into the new social role of a parent and thus hinder mature personality change. Indeed, SIT specifically suggests that if the behavioral changes required by the age-graded or contextually required roles do not occur, the maturation process typically promoted by the new role may be hindered or stopped (e.g. Roberts et al., 2009; Roberts & Davis, 2016). For instance, work life entry is related to increases in conscientiousness-related traits (Asselmann & Specht, 2021; Leikas & Salmela-Aro, 2015), but individuals engaging in counterproductive work behaviors fail to show such mature development (Roberts et al., 2006).
Failing to adapt one’s behavior to the new role and/or engaging in behavior counterproductive to the role is referred to as “de-investing” to the new role in the SIT (Asselmann & Specht, 2021; Roberts et al., 2006; Roberts & Davis, 2016). This means that individuals faced with a new social role may not adjust their behavior according to the demands of this role, which stops the maturation process, or, possibly, leads to changes toward immaturity. On the other hand, resources such as high level of social support may promote the maturation process. In terms of the TESSERA model, high levels of stressors may complicate each step of the TESSERA process: New parents with high level of stressors may be too overwhelmed to notice the triggers, acknowledge the expectations, adjust their personality state expressions accordingly, or to reflect on their changed behavioral or emotional processes, making mature change less likely (Wrzus & Roberts, 2017).
Stressors such as financial and health difficulties predict more difficult early parenthood experiences (Liu & Tronick, 2013; Matvienko-Sikar et al., 2018; Stickel et al., 2021), and there is some evidence of stressors enhancing undesirable personality changes and/or weakening or blocking mature changes (Lüdtke et al., 2011; Roberts & Bogg, 2004). Furthermore, maternal stress as such has been linked to undesirable personality change. For instance, Hutteman et al. (2014, Study 1) found that women experiencing stress in early motherhood reported declines in Emotional Stability, Agreeableness, and Conscientiousness by the time the child was 1 to 3 years. Rantanen et al. (2015) found that parenting stress predicted higher Neuroticism and lower Extraversion later in life. In sum, it could be expected that pre-existing and pregnancy-related stressors affect maternal personality change during the transition to parenthood by promoting undesirable changes of hindering mature changes. Such processes would be broadly compatible with the SIT and TESSERA model. In the present study, we were able to include several potentially impactful stressors and resources, as discussed next.
Pregnancy in itself is a major physiological and psychological stressor to the woman and induces a cascade of hormonal, metabolic, emotional, social and behavioral changes that may vary across pregnancies. In addition to variations in normal pregnancies, variations in pregnancies complicated by common cardiometabolic pregnancy disorders add to this complexity. Early pregnancy obesity, gestational diabetes, gestational hypertension, and pre-eclampsia burden a large number of pregnancies, and are among the most common causes of preterm birth, low birth weight, macrosomia, stillbirth, and caesarian section delivery (e.g. Abalos et al., 2014; Flenady et al., 2011; Yu et al., 2013). As they threaten the health and wellbeing of the mother and the child, these are major stressors that take place within pregnancies. Hence, exposure to these conditions may moderate any potential personality change related to becoming a parent. In addition to pregnancy complications, complications related to labor may be stressful and even traumatizing (e.g. Andersen et al., 2012), and to have a considerable effect on mothers’ post-partum experiences. Furthermore, child prematurity is a clear maternal stressor and a risk factor for mothers’ post-partum anxiety and depression (e.g. Holditch-Davis et al., 2003; Singer et al., 1999).
Child characteristics may also play a role, as parents’ perceptions of infant temperament are related to parents’ experience of the early stages of parenthood (e.g. Solmeyer & Feinberg, 2011). Child temperament has been investigated as a moderator of change in two relevant studies, though neither of these studies measured Big Five traits. First, one study found that parent-perceived child temperament moderated parents’ personality change during child’s infancy (Sirignano & Lachman, 1985): parents who perceived their infant’s temperament as easy reported positive changes in their own level of personal control, whereas parents who perceived their infants’ temperament as difficult reported negative changes in their personal control. Second, parents of infants with a difficult temperament reported increased levels of depressive symptoms after childbirth as compared to parents of an infant with an “easy” temperament (Wilkie & Ames, 1986). However, no study that we are aware of has investigated the role of child temperament in change in parents’ Big Five personality traits or facets.
Conversely, high level of social support is linked to lower post-partum depressive and anxiety symptoms among mothers (Asselmann et al., 2020). Furthermore, mother’s satisfaction with her relationship with her spouse—typically the most important source of social support during pregnancy and post-partum—has been linked to better post-partum health and lower stress (Tissera et al., 2020). Given the close links between depressive and anxiety symptoms and corresponding facets of neuroticism, it seems plausible that level of available social support may moderate changes in these facets. Finally, maternal prenatal mental health status is among the most robust predictors of post-partum depression (Robertson et al., 2004; Smorti et al., 2019).
To sum up, the existing literature suggests that maternal prenatal stress, pre-existing stressors, physical complications during pregnancy and labor, and child’s difficult temperament could enhance undesirable personality change and weaken desirable change, whereas protective factors and resources such as social support could enhance desirable change and serve as a buffer against undesirable change. Findings along these lines would be informative for theoretical models of personality development such as SIT and TESSERA, as such findings would help understand contextual factors modifying the theoretically predicted maturation effects.
In the present study, we investigate the following potential stressors and resources as moderators of change: maternal pregnancy-related stress, physical pregnancy complications, complications related to labor, child prematurity, presence of a mother’s pre-pregnancy mental health diagnosis, relationship satisfaction, and mothers’ perceptions of child temperament. In addition, the possible moderating roles of maternal age, education level, and parity are investigated. We note at this point that our sample consists of both primiparous and multiparous mothers. As having one’s first child is conceivably a qualitatively different experience than having one’s second or subsequent child, we initially conducted the analyses separately for these two groups. However, the results were largely identical for primi- and multiparous mothers, and we decided to combine the groups to reduce the number of results presented. We use parity as a moderator variable instead, and the analyses conducted separately for each subgroup are presented in the online Appendix.
Personality development and life events: long- and short-term change
Research on life events and personality development has largely focused on long-term, enduring change. While it is imperative to explore and identify long-term changes in order to understand personality development across the life span, examining short-term changes that occur temporally close to the actual event may also reveal relevant aspects of the dynamics between personality and life events (e.g. Bleidorn et al., 2018; Nesselroade, 1991). First, one of the reasons to varying results regarding personality change and parenthood may be that the parenthood experience and the associated social roles change considerably from the birth of a child to several years post-partum (e.g. Asselmann & Specht, 2020). Thus, studying personality development at several different points during parenthood is needed in order to achieve a complete picture of personality and having children.
Second, as the TESSERA model suggest, long-term change may be based on short-term sequences of situational triggers and affective and behavioral reactions to such triggers (Wrzus & Roberts, 2017). When changes in environmental or personal factors occurs (e.g., a person becomes a parent), the sequences prevailing in one’s everyday life change too, and, when repeated over time and many occasions, the new sequences may eventually result in personality change (Wrzus & Roberts, 2017). This view highlights the need to investigate short-term changes in personality alongside with long-term change. Third, although personality trait changes that occur temporally close to the life event may be temporary (e.g. van Scheppingen et al., 2016), they inform us about immediate reactions to new life situations and may thus provide insight into the dynamics between personality and life transitions and into new parents’ immediate reactions to new social roles and situations (Asselmann & Specht, 2020). The present research provides such information by focusing on short-term personality changes from early pregnancy to 6 months post-partum.
Method
Participants and procedure
The participants of the present study came from the Prediction and Prevention of pre-eclampsia and Intrauterine Growth Restriction (PREDO) cohort that originally enrolled 4785 pregnant women between 2005 and 2009 through antenatal clinics in 10 hospitals in Southern and Eastern Finland. Detailed information about the sample and recruitment process have been published elsewhere (Girchenko et al., 2017; Reynolds et al., 2015), but two recruitment processes were used. First, women with a known pregnancy risk factor such as risk of pre-eclampsia were recruited (risk factor subsample), and second, women with no known risk factors were recruited (community-based subsample). The current sample includes women in the PREDO cohort’s both subsamples who gave birth to a live-born singleton child between 2006 and 2010 and provided personality data at two time points. Participants were not screened in any way, except for the physical health risk factors. The sample was a convenience sample and no sample size calculations pertaining to the present study were conducted prior to data collection.
The self-report measures used in the current study were mailed as paper versions to the women’s home addresses with a return envelope at the 12th pregnancy week and at 6 months post-partum. A total of 2500 women returned both questionnaires with completed personality measures. It was important that participants completed the questionnaires roughly at the designated times (Time 1 = 12th week of pregnancy and Time 2 = 6 months post-partum). Based on a visual investigation of the distributions of completion times, as well as on considerations of sufficient time gap between the measurements, and the possible changes in the family’s child care situation around 9 months post-partum (because of the Finnish parenting leave policy, almost all children stay at home with a parent at least until the age of 9 months, after which some children start day care) we decided on cutoff points at pregnancy week 24 for the T1 questionnaire, and child’s age of 10 months for the T2 questionnaire. Five women returned the T1 questionnaire later than at pregnancy week 24, and 50 women returned the T2 questionnaire when their child was over 10 months old. These 55 women were removed from the analyses, leaving us with a sample of 2445 participants.
The mean age of participants was 31.8 years (sd = 4.7 years). Regarding parity, 1030 were expecting their first child, 985 their second child, 323 their third child, 91 their fourth or further child, and parity information was missing for 16 participants. Regarding education level, 45 participants had primary, 887 secondary, 650 lower tertiary, and 863 upper tertiary education. Regarding relationship status, 45 participants reported being single, and 2272 reported being married or in a co-habiting relationship.
Measures
Extraversion and neuroticism
Extraversion and Neuroticism were measured with the corresponding subscales of the NEO-PI-R, a 240-item, valid and reliable questionnaire designed to measure the Five-Factor model personality traits (Costa & McCrae, 2008). Extraversion and Neuroticism were measured with 48 items each, and participants responded on a five-point scale from 0 (totally disagree) to 4 (totally agree). Each of the 6 facets of each trait was measured with 8 items. Example items for the facet scales are “I often feel tense and jittery” (N-Anxiety), “I often get angry at the way people treat me” (N-Hostility), “I am seldom sad or depressed” (N-Depression, reversed), “I often feel helpless and want someone else to solve my problems” (N-Vulnerability), “In dealing with other people, I always dread making a social blunder” (N-Self-Consciousness), “I have trouble resisting my cravings” (N-Impulsivity), “I really like most people I meet” (E-Warmth), “I like to have a lot of people around me” (E-Gregariousness), “I am dominant, forceful, and assertive” (E-Assertiveness), “I often crave excitement” (E-Excitement seeking), “My life is fast-paced” (E-Activity), and “Sometimes I bubble with happiness” (E-Positive Emotions).
The reliabilities (Cronbach’s alphas) for Neuroticism for T1/T2 were .93/.93 for the full scale, .79/.79 for Anxiety, .75/.74 for Hostility, .84/.84 for Depression, .78/.77 for Vulnerability, .74/.75 for Self-Consciousness, and .74/.76 for Impulsivity. Reliabilities for Extraversion for T1/T2 were .90/.90 for the full scale, .79/.78 for Warmth, .77/.77 for Gregariousness, .75/.75 for Assertiveness, .70/.70 for Excitement Seeking, .80/.78 for Activity, and .81/.80 for Positive Emotions. Correlations between raw trait and facet mean scores within and across measurement points are presented in Tables 2–5.
Pregnancy stress
Pregnancy-related stress was measured at T1 with a single visual analogue scale asking participants to indicate how much pregnancy-related stress they experienced at the moment by placing a mark on a 650 millimeter long line with anchors “no stress” and “very high stress” at left and right poles, respectively.
Relationship satisfaction
Relationship satisfaction was measured at T1 with the 7-item Dyadic Satisfaction subscale of the Dyadic Adjustment Scale (DAS, Spanier, 1976), responded on a 7-point scale from 1 (all the time) to 7 (never), complemented with the full DAS item 32 “Which of the following statements best describes how you feel about the future of your relationship,” with response options ranging from 1 (I want desperately for my relationship to succeed, and would go to almost any length to see that it does) to 6 (My relationship can never succeed, and there is no more that I can do to keep the relationship going). DAS items were reverse-coded so that higher values indicated higher relationship satisfaction, and the scale reliability (Cronbach’s alpha) was .83.
Child temperament
Participants reported on their child’s temperament traits using the Revised Infant Behavior Questionnaire (Gartstein & Rothbart, 2003) at T2. This instrument asks respondents to report on the relative frequency of specific infant reactions and behaviors during the past week (or 2 weeks for some items). These behavioral ratings are combined into 14 subscales (e.g. vocal reactivity, cuddliness, distress to limitations, soothability, and activity level), and these subscales further into three broader temperamental factors: Extraversion/Surgency (E/S), Negative Affectivity (NA), and Orienting/Regulation (O/R). These factors tap expressions of positive emotions and approach behavior (E/S), expressions of distress and negative emotions (NA), and self-regulation, including direction of attention and soothability (O/R). The scale reliabilities (Cronbach’s alphas) for E/S, NA, and O/R were .73, .72 and .63, respectively. Father-ratings of child temperament traits were also obtained at T2 using the same behavioral ratings. Father-ratings’ reliabilities were .77, .71, and .64 for E/S, NA, and O/R, respectively. Father-ratings correlated moderately with mother-ratings, r = .32 for E/S, r = .48 for NA, and r = .30 for O/R.
Maternal mental health
Information regarding maternal mental health was retrieved from the Finnish nationwide Care Register for Health Care with participants’ permission and permission from the register authorities. This register comprises International Classification of Diseases 8th, 9th, and 10th revision diagnostic codes and are available since 1969. We recorded whether participants had received any mental disorder diagnosis (any ICD-10 category F diagnosis) before the birth of the child born during our follow-up and formed a binary (yes/no) variable indicating that the participant had or did not have a mental disorder diagnosis before childbirth. In addition, participants who received a mental disorder diagnosis during the follow-up, that is, between T1 and child turning 10 months were marked as having a missing value on this variable. One-hundred ninety-nine (199) participants had a mental health diagnosis, 2075 participants did not, and the information was missing or participant received a mental health diagnosis between T1 and T2 for 171 participants.
Maternal physical health
As indicators of physical health during pregnancy, we considered the most common pregnancy-related physical complications: diabetes, gestational hypertension, and pre-eclampsia. With the permission of the participant and register authority, we retrieved diagnostic data from the Care Register for Health Care and Medical Birth Register, and coded whether women in our sample were normotensive or had gestational hypertension (ICD-10:O13), chronic hypertension (ICD-10: O10, I10) or pre-eclampsia (ICD-10: O11, O14, O15), and whether they had no diabetes or Type 1 (ICD-9:2500A-2509A; ICD-10:E10) or Type 2 (ICD-9:2500B-2509B; ICD-10:E11) diabetes diagnosed before current pregnancy, or gestational or other (ICD-10:O24) diabetes diagnosed in the current pregnancy (see Lahti-Pulkkinen et al., 2020, for more detailed information of the diagnostic data).
These diagnostic variables listed above were combined into a single binary variable representing no physical health disorders during current pregnancy (coded as 0) vs. having one or more physical disorders issue during current pregnancy (coded as 1). Out of the 2445 participants, 1728 had no diagnosis, and 506 had a diagnosis of hypertension, diabetes, and/or pre-eclampsia. In addition, 205 participants had been diagnosed with hypertension (ICD-9: 642, 401-405; ICD-10: I1, O10-O11, O13-O16) or diabetes (ICD-9:6480A, 6488A; ICD-10:O24) prior to, but not during the current pregnancy; these 205 participants were coded as missing for this variable. Physical health information could not be retrieved for 6 participants; these participants were also coded as missing.
Delivery mode
Delivery mode was retrieved from the Medical Birth Register with the permission of the participants and register authority. Delivery mode was binary coded as 0 (normal vaginal delivery) vs. 1 (breech, forceps, or vacuum vaginal delivery or elective, urgent or emergency c-section). Out of all participants, 1729 had a normal vaginal delivery and 696 participants had some delivery-related complication or an elective c-section. Delivery mode information could not be retrieved for 20 participants.
Child prematurity
Child prematurity status was retrieved from the Medical Birth Register with the permission of the participants and register authority. Children born at pregnancy week 36+6 or earlier were coded as born premature (coded as 1), and children born at 37+0 or later were coded as born full term (coded as 0). Eighty-four (84) children were born premature, 2344 were born full term, and prematurity information could not be retrieved for 17 participants.
Analytical strategy
As only two time points were available, Latent Difference Score Models (LDSM; e.g. McArdle & Hamagami, 2001) were used to investigate change. Models for facets were built by using 4 parcels with two items each as indicators (randomly paired), and models for traits were built using facets as indicators. Parcels were used to enhance reliability of indicators (e.g. Little et al., 2013). Corresponding parcels/facets were allowed to correlate over time. Mean-level change was measured via the magnitude and significance of the latent change scores (e.g. Kievit et al., 2018), and rank-order stability via correlations between latent T1 and T2 variables. Moderated change was investigated via latent moderated difference score models. A moderation effect was considered to be indicated by a significant regression path between the moderator and the change estimate. Full information maximum likelihood estimation was used in all analyses. Analyses were conducted in R (v. 4.0.2, R Core Team, 2020) using the lavaan package (v. 0.6-8; Rosseel, 2012).
Figure 1a depicts the model outline for the unconditional trait model and Figure 1b, the model outline for the moderated facet model. The figures were created with the semPlot package in R (Epskamp, 2022). For the R code for the LDSMs, see online Appendix at https://osf.io/q45f6/. Strict invariance models were used in the unconditional and moderated change analyses. Because a very large number of comparisons (170) were conducted on the same dataset, p-values were adjusted according to the Benjamini–Hochberg correction (Benjamini & Hochberg, 1995) using the p.adjust function in R. (a) Model outline for the unconditional trait model. The unconditional trait model with Neuroticism as an example. The indicators are facets. Anx = Anxiety, Hos = Hostility, Dep = Depression, SC = Self-Consciousness, Imp = Impulsivity, Vul = Vulnerability. Solid lines represent estimated paths/variances/covariances and dashed lines represent fixed paths/variances/covariances. (b) Model outline for the moderated facet model. par = parcel, d = latent change score, M = moderator. Solid lines represent estimated paths/variances/covariances. Dashed lines represent fixed paths/variances/covariances.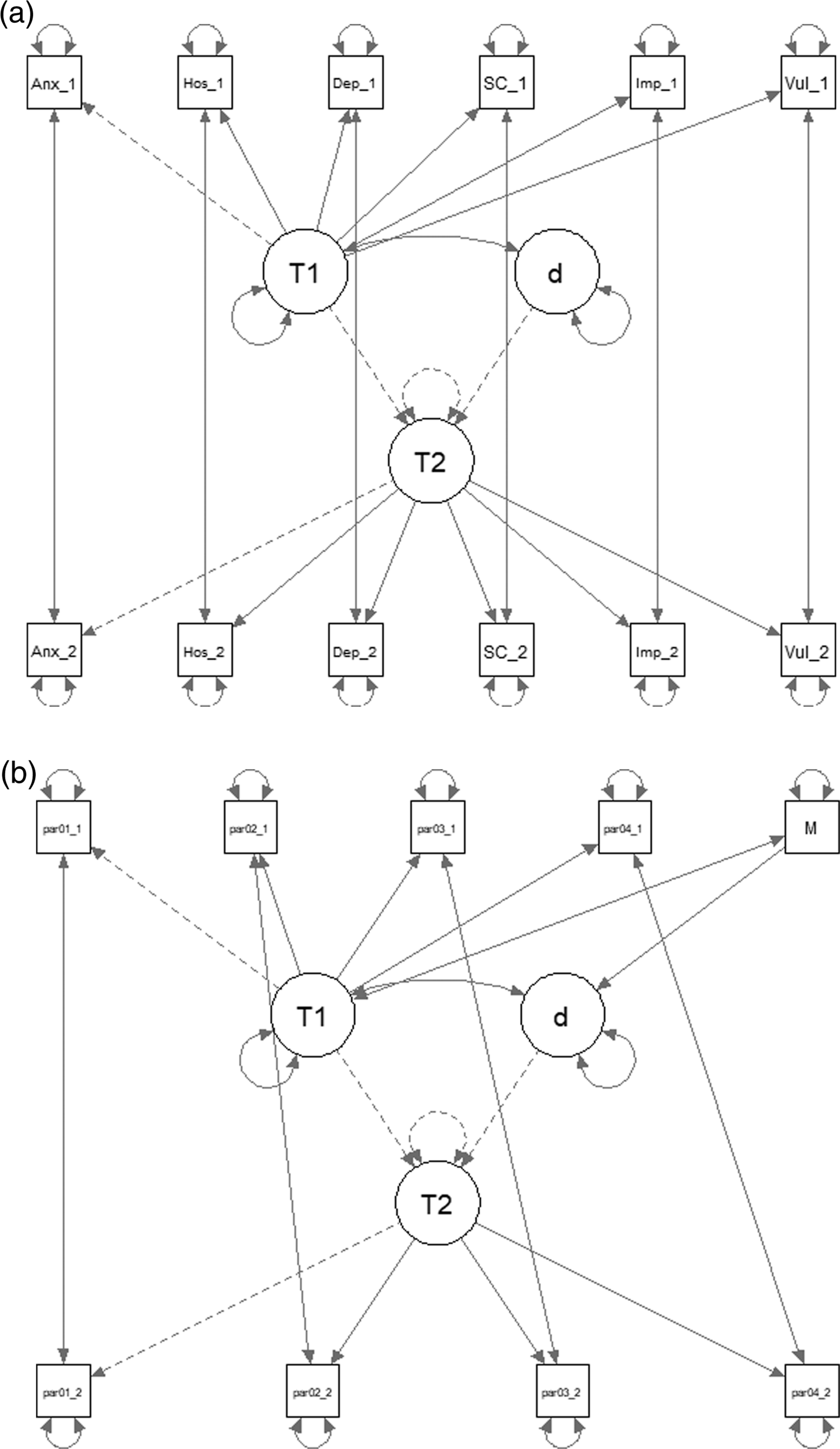
Measurement invariance (MI) testing was conducted by fitting a series of LDS models with the above presented model outlines and increasingly stringent constraints (e.g. Putnick & Bornstein, 2016). For model fit, we used criteria of CFI > = .95 and RMSEA < .09. For measurement invariance criteria, we used the guidelines of Rutkowski and Svetina (2014), according to which there should be a maximum change of −.02 in CFI and maximum change of +.03 in RMSEA for metric invariance, and a maximum change of −.01 for CFI and +.01 for RMSEA for scalar invariance. Further, Cheung and Rensvold (2002) suggest that is change in CFI between two models is < .01, the model with more constraints should be chosen.
Scalar invariance was found for all traits and facets except for Activity (for completeness, we present the unconditional results for Activity in Table 3 but refrain from interpreting them, and Activity is omitted from moderation analyses). The MI results are presented in detail in the online Appendix (https://osf.io/q45f6/). Because CFI changes from scalar to strict invariance models were smaller than (or in case of Warmth, equal to) .01, we used the strict invariance models in our main analyses (Cheung & Rensvold, 2002).
Because of the main aim of the study was to predict and prevent pre-eclampsia and IUGR, power calculations pertaining to current analyses were not conducted before data collection. For the same reasons, the present research was fully exploratory and no parts of it were pre-registered.
Results
Means, standard deviations, and reliabilities of the continuous variables studied.
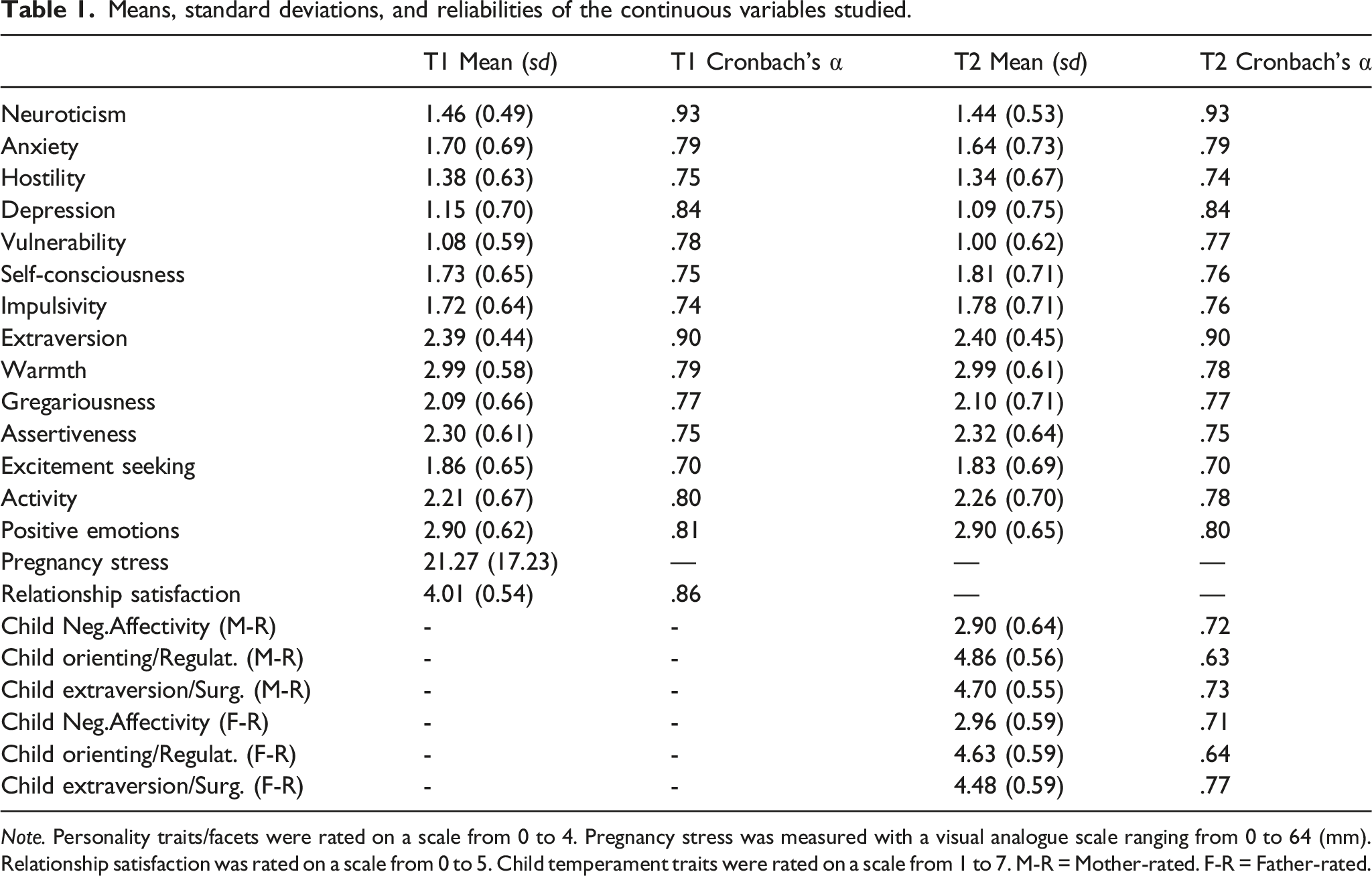
Note. Personality traits/facets were rated on a scale from 0 to 4. Pregnancy stress was measured with a visual analogue scale ranging from 0 to 64 (mm). Relationship satisfaction was rated on a scale from 0 to 5. Child temperament traits were rated on a scale from 1 to 7. M-R = Mother-rated. F-R = Father-rated.
Correlations between neuroticism facets across time points.
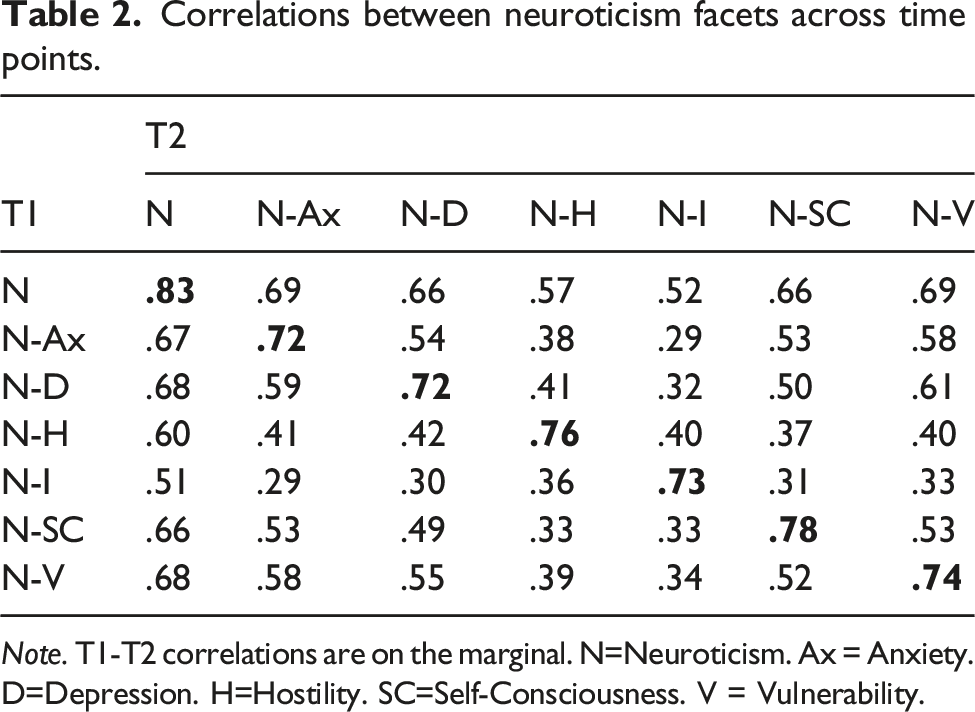
Note. T1-T2 correlations are on the marginal. N=Neuroticism. Ax = Anxiety. D=Depression. H=Hostility. SC=Self-Consciousness. V = Vulnerability.
Correlations between neuroticism facets within time points.
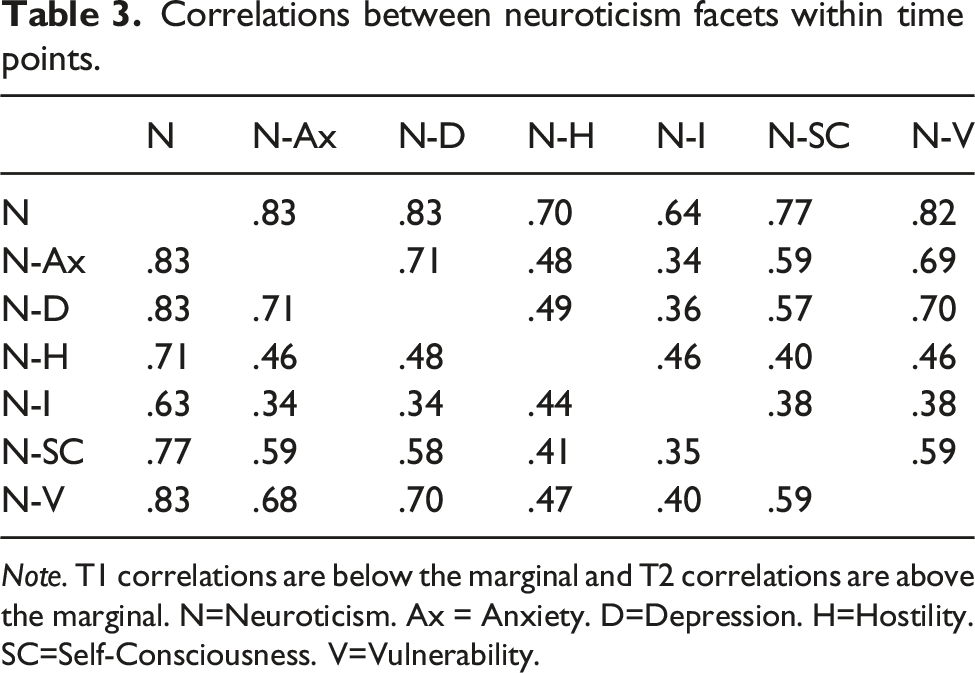
Note. T1 correlations are below the marginal and T2 correlations are above the marginal. N=Neuroticism. Ax = Anxiety. D=Depression. H=Hostility. SC=Self-Consciousness. V=Vulnerability.
Correlations between extraversion facets across time points.
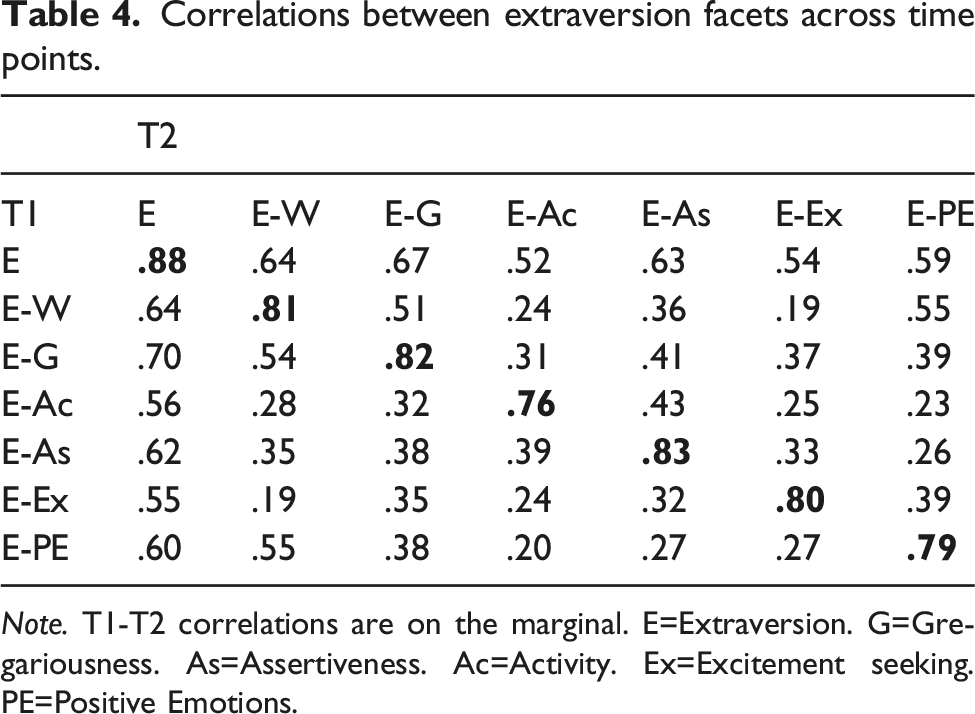
Note. T1-T2 correlations are on the marginal. E=Extraversion. G=Gregariousness. As=Assertiveness. Ac=Activity. Ex=Excitement seeking. PE=Positive Emotions.
Correlations between extraversion facets within time points.
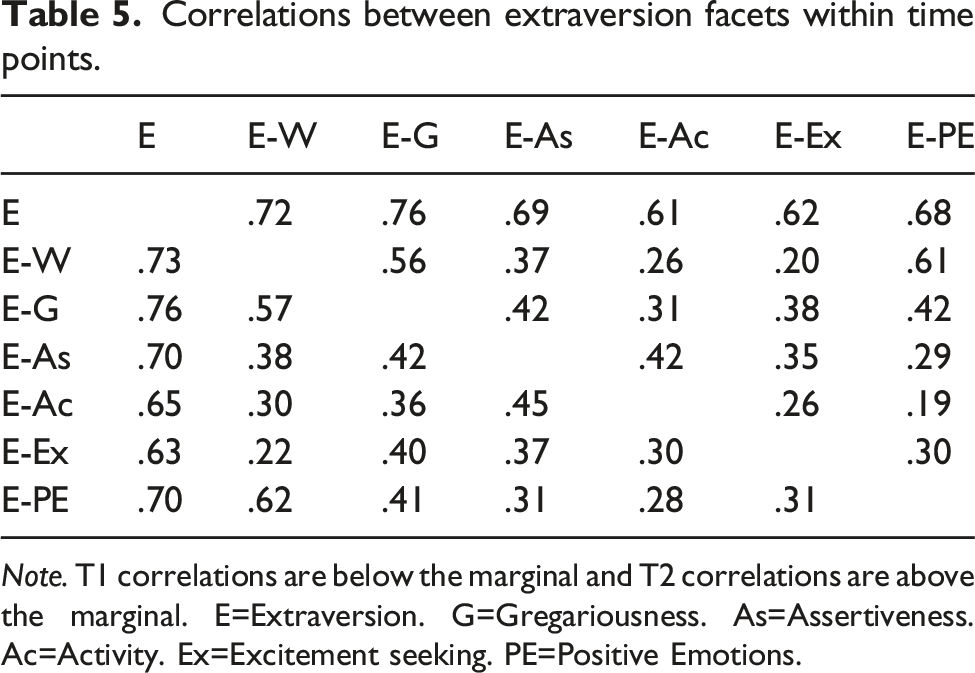
Note. T1 correlations are below the marginal and T2 correlations are above the marginal. E=Extraversion. G=Gregariousness. As=Assertiveness. Ac=Activity. Ex=Excitement seeking. PE=Positive Emotions.
Mean-level change and rank-order stability
Results of unconditional latent difference score models.
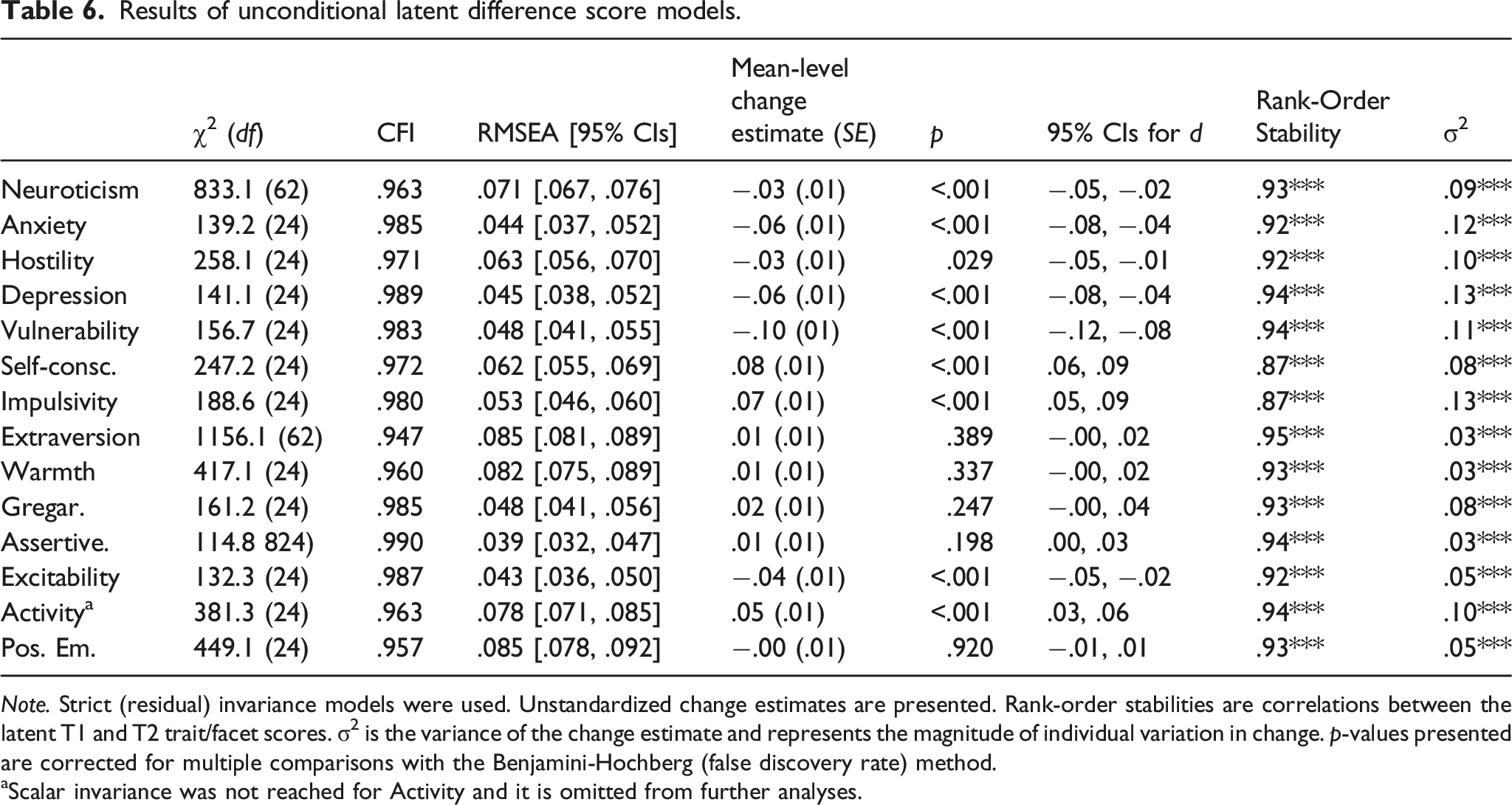
Note. Strict (residual) invariance models were used. Unstandardized change estimates are presented. Rank-order stabilities are correlations between the latent T1 and T2 trait/facet scores. σ2 is the variance of the change estimate and represents the magnitude of individual variation in change. p-values presented are corrected for multiple comparisons with the Benjamini-Hochberg (false discovery rate) method.
aScalar invariance was not reached for Activity and it is omitted from further analyses.
Moderated change
Results of latent moderated difference score models: Demographic variables as moderators.
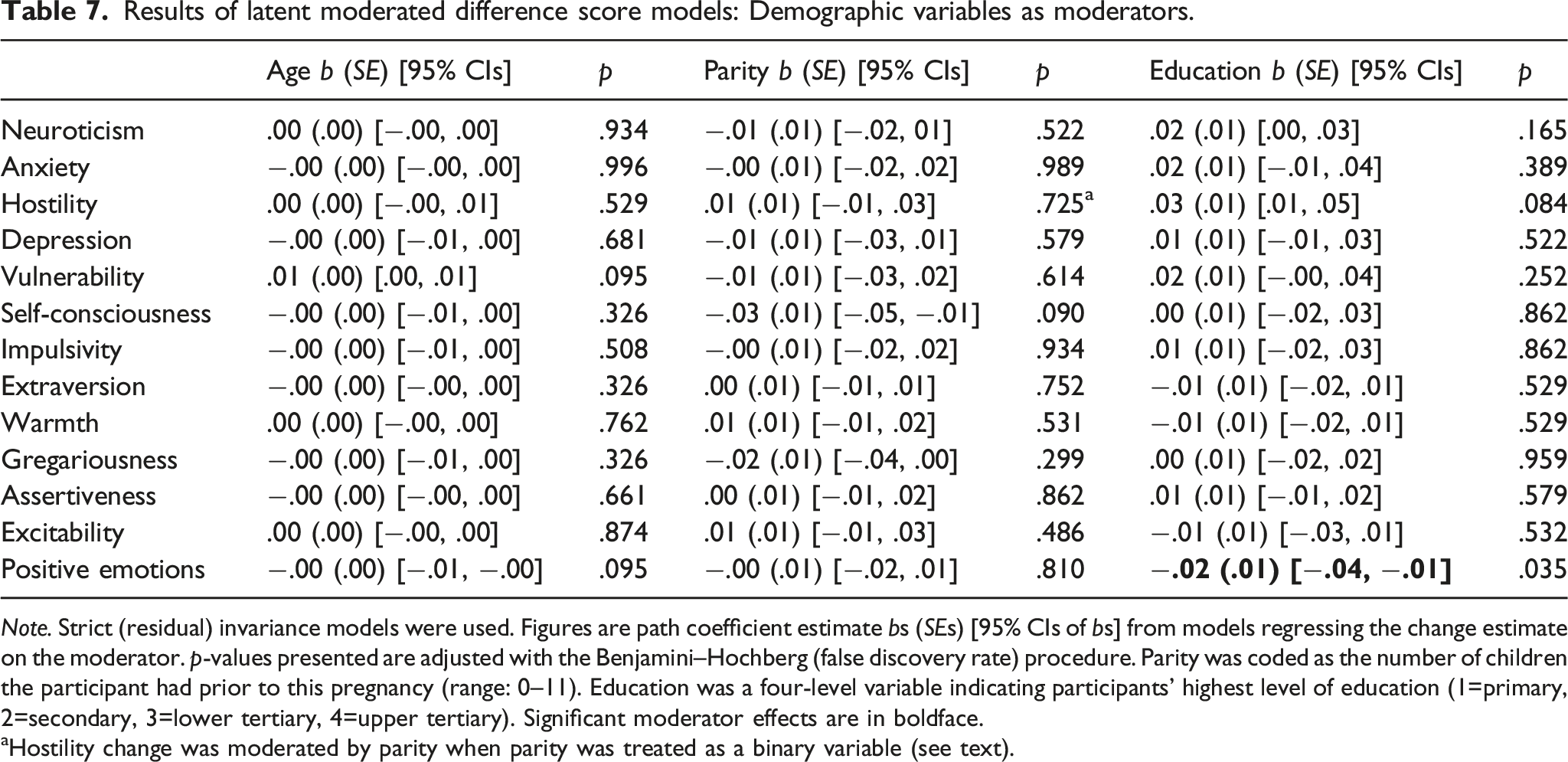
Note. Strict (residual) invariance models were used. Figures are path coefficient estimate bs (SEs) [95% CIs of bs] from models regressing the change estimate on the moderator. p-values presented are adjusted with the Benjamini–Hochberg (false discovery rate) procedure. Parity was coded as the number of children the participant had prior to this pregnancy (range: 0–11). Education was a four-level variable indicating participants’ highest level of education (1=primary, 2=secondary, 3=lower tertiary, 4=upper tertiary). Significant moderator effects are in boldface.
aHostility change was moderated by parity when parity was treated as a binary variable (see text).
Results of latent moderated difference score analyses: Health complications as moderators.
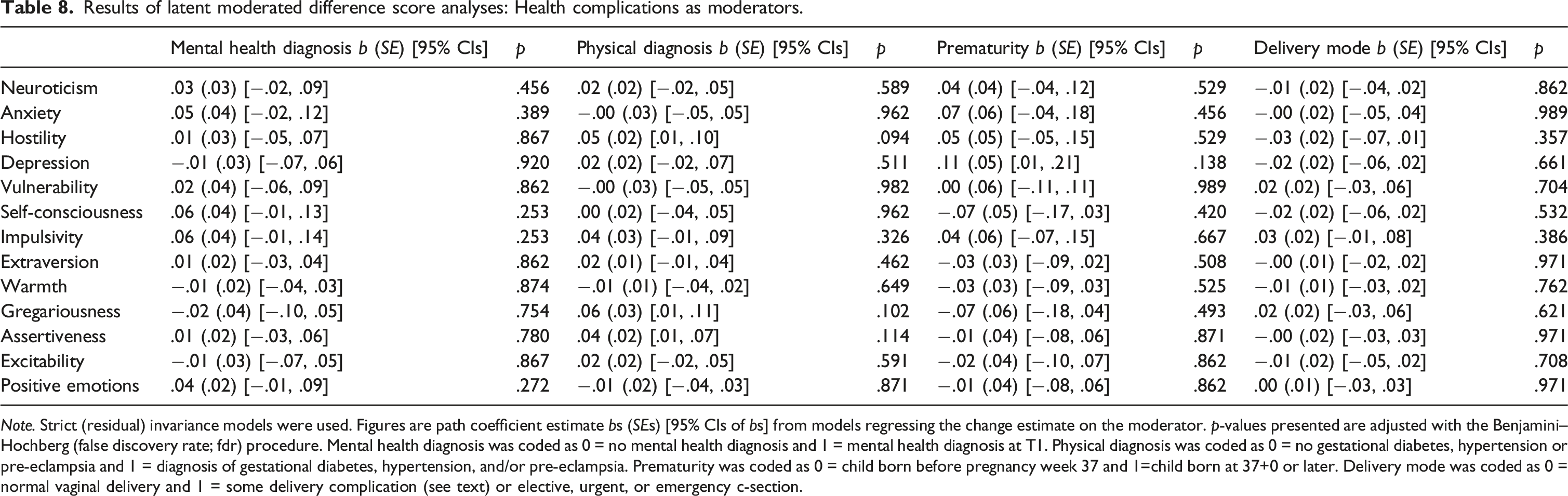
Note. Strict (residual) invariance models were used. Figures are path coefficient estimate bs (SEs) [95% CIs of bs] from models regressing the change estimate on the moderator. p-values presented are adjusted with the Benjamini–Hochberg (false discovery rate; fdr) procedure. Mental health diagnosis was coded as 0 = no mental health diagnosis and 1 = mental health diagnosis at T1. Physical diagnosis was coded as 0 = no gestational diabetes, hypertension or pre-eclampsia and 1 = diagnosis of gestational diabetes, hypertension, and/or pre-eclampsia. Prematurity was coded as 0 = child born before pregnancy week 37 and 1=child born at 37+0 or later. Delivery mode was coded as 0 = normal vaginal delivery and 1 = some delivery complication (see text) or elective, urgent, or emergency c-section.
Results of latent moderated difference score analyses: Relationship satisfaction, mother-rated child temperament, and pregnancy stress as moderators.
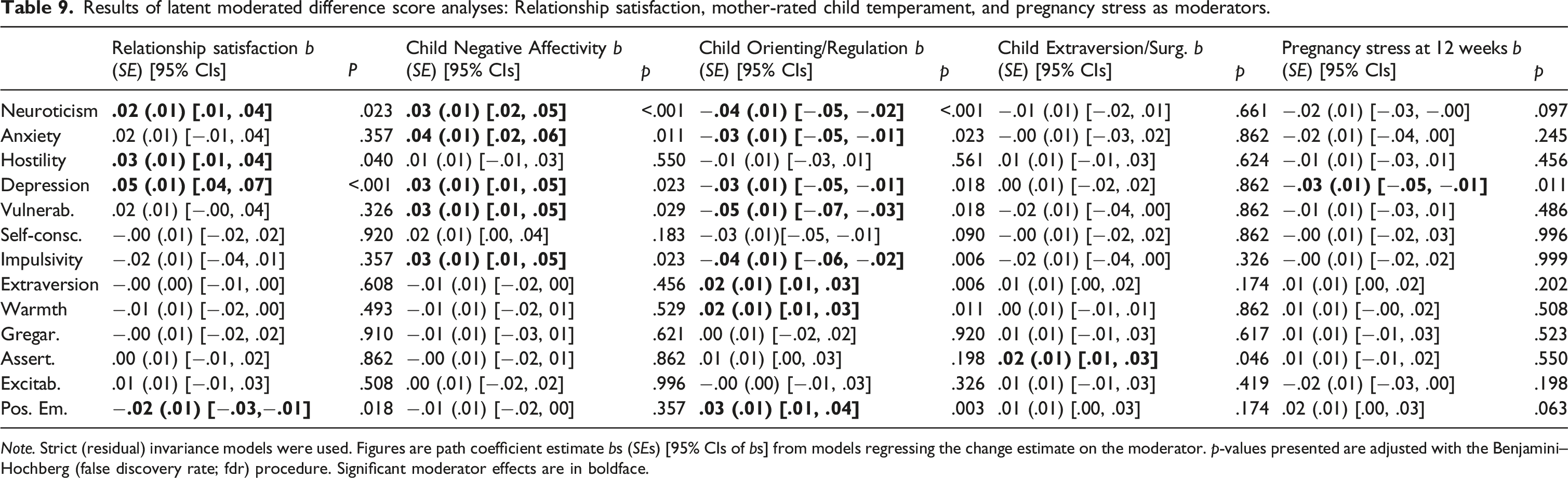
Note. Strict (residual) invariance models were used. Figures are path coefficient estimate bs (SEs) [95% CIs of bs] from models regressing the change estimate on the moderator. p-values presented are adjusted with the Benjamini–Hochberg (false discovery rate; fdr) procedure. Significant moderator effects are in boldface.
Results of latent moderated difference score analyses: Father-rated child temperament traits as moderators.
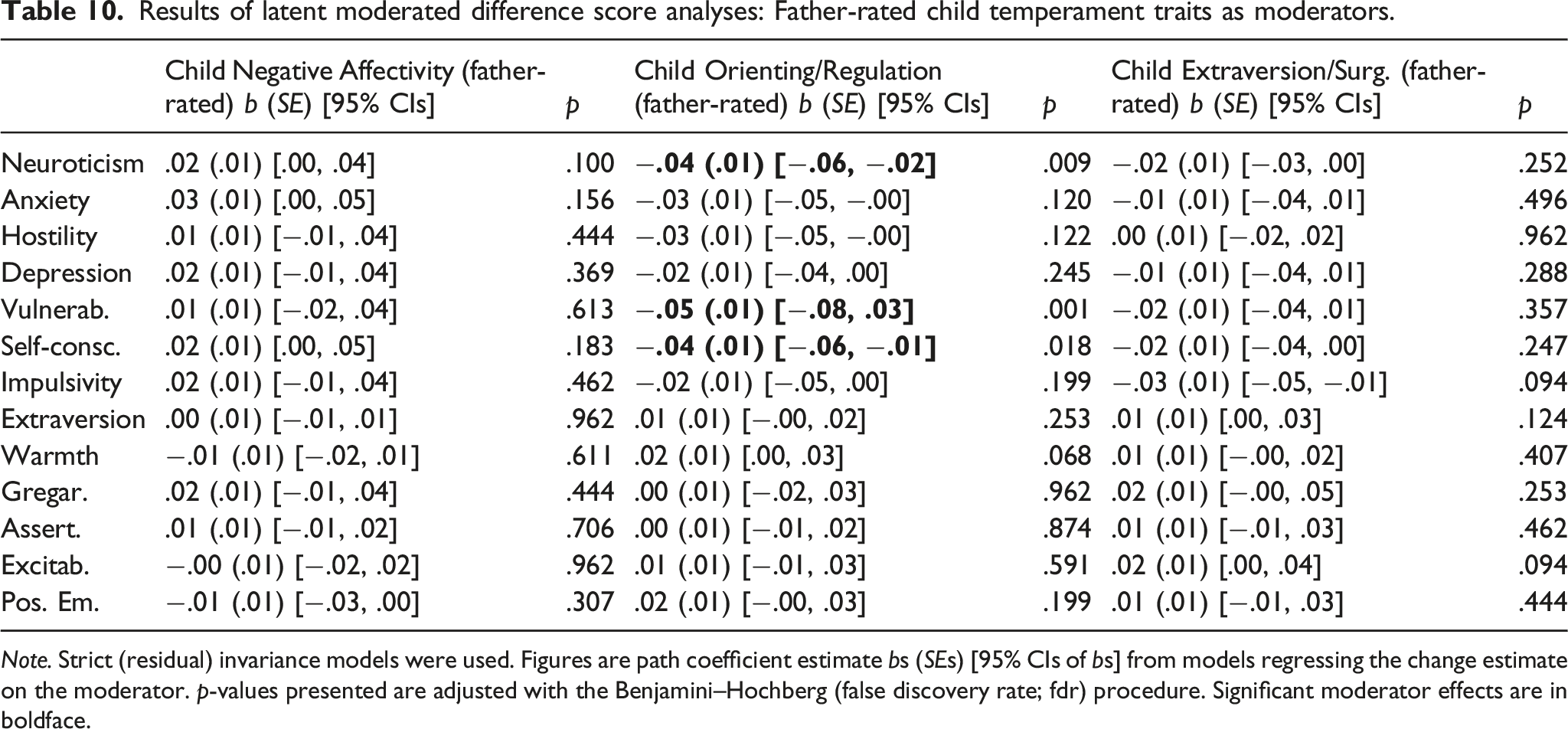
Note. Strict (residual) invariance models were used. Figures are path coefficient estimate bs (SEs) [95% CIs of bs] from models regressing the change estimate on the moderator. p-values presented are adjusted with the Benjamini–Hochberg (false discovery rate; fdr) procedure. Significant moderator effects are in boldface.
Mothers’ education moderated change in Extraversion facet Positive Emotions. Pregnancy stress moderated change in Neuroticism facet Depression. Relationship satisfaction moderated change in Neuroticism facets Hostility and Depression, in trait Neuroticism, and in Extraversion facet Positive Emotions. Mother-rated child NA moderated change in Neuroticism facets Anxiety, Depression, Vulnerability, and Impulsivity, and in trait Neuroticism. Mother-rated child O/R moderated change in Neuroticism facets Anxiety, Vulnerability, and Impulsivity, as well as in trait Neuroticism, and in Extraversion facets Warmth, Positive Emotions, and in trait Extraversion. Mother-rated E/S moderated change in Assertiveness. Father-rated O/R moderated change in mothers’ Vulnerability, Self-Consciousness, and trait Neuroticism.
We first go through the moderating effects for facets and traits with only one significant moderator. We investigated these moderation effects more closely by running unconditional change score models separately for participants scoring low and high on the moderator using median split. For Hostility and relationship satisfaction, neither participants with low nor participants with high T1 relationship satisfaction showed significant change in Hostility (d = −.03, SE = .01, p = .015 for low relationship satisfaction group, and d = −.02, SE = .02, p = .838 for high relationship satisfaction group). Participants who rated their child as low in O/R did not change in Warmth (d = −.01, SE = .01, p = .559), whereas participants rating their child as high in O/R increased in Warmth (d = .03, SE = .01, p = .001); see Figure 3a. Note that participants rating their child as higher in O/R at T2 had higher Warmth at T1, and they further increased in Warmth, whereas participants rating their child as lower in O/R at T2 had lower Warmth at T1 and they remained at this level.
Assertiveness change scores for participants who rated their child as low in E/S (d = .00, SE = .01, p = .929) and change scores of participants rating their child as high in E/S (d = .02, SE = .01, p = .040) did not reach significance at the p < .01 level. Participants rating their child as low in O/R did not change in trait Extraversion (d = −.01, SE = .01, p = .323), whereas participants rating their child as high in O/R increased in trait Extraversion (d = .02, SE = .01, p = .004); note that participants rating their child as high in O/R had higher trait Extraversion at T1 and further increased in trait Extraversion and participants rating their child as low in O/R had lower initial trait Extraversion and they remained at this lower level (Figure 3d). Finally, regarding Self-Consciousness, mothers whose children were rated as low in O/R by fathers increased in Self-Consciousness more (d = .11, SE = .02, p < .001) than participants whose children were rated as high in O/R by fathers (d = .05, SE = .02, p = .002); the latter group of mothers had higher Self-Consciousness at T1 and they increased more strongly in Self-Consciousness than the former group, though both groups increased (see supplementary Figure 12).
As explained above, some facets and traits had more than one significant moderator. For these facets and traits, we ran new models which included all significant moderators, to see which moderators would remain significant after controlling for others. Child temperament traits, pregnancy stress, and relationship satisfaction were allowed to correlate in the multiple moderation models (we also ran these models with moderators set as uncorrelated and the results were unchanged in terms of significance levels and estimate sizes). We used p < .01 for cutoff for significance for these additional analyses (but note that the p-values of the multiple moderated models were not formally adjusted). We then again ran the unconditional LDS models separately for participants below vs. above median on the moderator for those moderator effects that remained significant in these multiple moderator models.
For Anxiety, mother-rated NA remained a significant moderator (b = .03, SE = .01, p = .009), whereas O/R did not (b = −.02, SE = .01, p = .041). Anxiety decreased among participants who rated their child as low in NA (d = −.07, SE = .02, p < .001; these participants were initially lower in Anxiety and then decreased), but those who rated their child as high in NA did not change (d = −.03, SE = .02, p = .062; see Figure 2a; these participants remained in their initially higher level of Anxiety). Selected moderator effects for Neuroticism facets.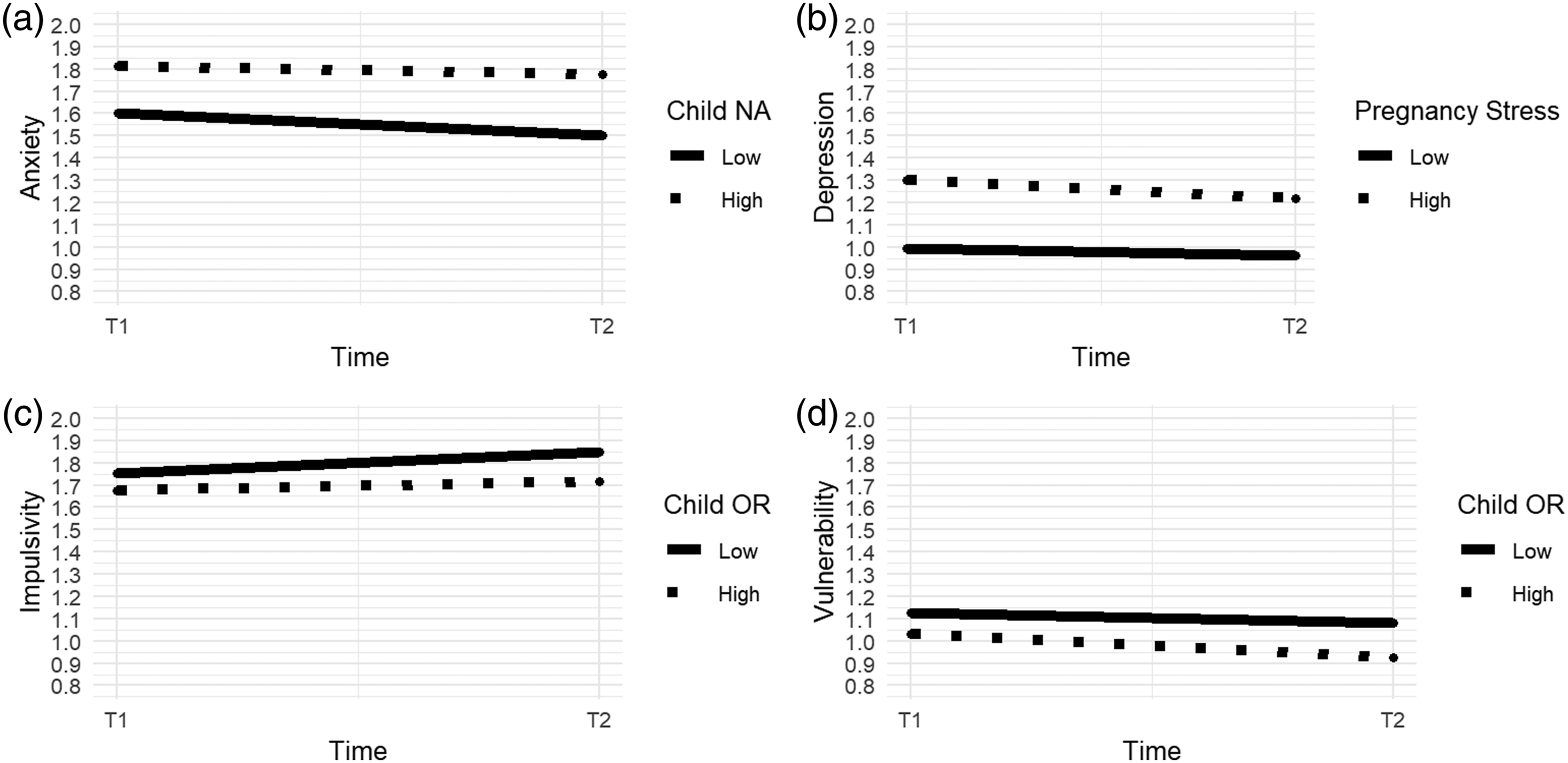
For Depression, the moderating effect of pregnancy stress (b = −.03, SE = .01, p < .001) remained significant after controlling for other moderators. The moderating effects of relationship satisfaction (b = .01, SE = .01, p = .132), mother-rated O/R (b = −.02, SE = .01, p = .017), and mother-rated NA (b = .03, SE = .01, p = .011) were no longer significant. The unconditional models ran separately for participants who were below and above median in pregnancy-related stress at T1 showed that both groups decreased in Depression, but, surprisingly, high-stress participants decreased more (d = −.08, SE = .01, p < .001) than low-stress participants (d = −.04, SE = .01, p = .007; Figure 2b). Note that low-stress participants had very low T1 level of Depression, and they remained at this low level, whereas high-stress participants had higher T1 Depression levels, which then decreased (Figure 2b).
For Impulsivity, mother-rated child O/R remained a significant moderator (b = −.03, SE = .01, p = .005), whereas mother-rated child NA did not (b = .02, SE = .01, p = .055), see Figure 2c. Participants who rated their child as low in O/R increased in Impulsivity more (d = .10, SE = .02, p < .001) than participants who rated their child as high in O/R (d = .05, SE = .02, p = .001). T1 levels of Impulsivity were similar across these groups (Figure 2c).
For Vulnerability, mother-rated O/R remained a significant moderator (b = −.03, SE = .01, p = .001), and father-rated OR also remained a significant moderator (b = −.04, SE = .01, p = .009). The effect of mother-rated NA was no longer significant (b = .02, SE = .01, p = .068). All participants decreased in Vulnerability, but mothers who rated their child as high in O/R decreased more strongly (d = −.14, SE = .02, p < .001) than participants who rated their child as low in O/R (d = −.06, SE = .02, p < .001; Figure 2d); the T1 Vulnerability levels were slightly lower for participants rating their child as higher in O/R at T2. The effect of father-rated O/R was virtually identical to that of mother-rated O/R (d = −.16, SE = .02, p <.001 for high O/R group and d = −.06, SE = .02, p = .002 for the low-O/R group).
For trait Neuroticism, mother-rated NA (b = .02, SE = .01, p = .003) and O/R (b = −.03, SE = .01, p < .001) remained significant moderators, whereas relationship satisfaction (b = .01, SE = .00, p = .180) and father-rated O/R (b = −.03, SE = .01, p = .011) did not. Mothers rating their child as low in NA decreased in Neuroticism (d = −.05, SE = .01, p < .001), whereas those rating their child as high in NA did not (d = −.01, SE = .01, p = .411); mothers rating their child as high in NA had higher T1 Neuroticism level than mothers rating their child as low in NA, and the former group remained at this higher level of Neuroticism (see supplementary Figure 4 in the online Appendix.). Similarly, mothers rating their child as low in O/R did not change in Neuroticism (d = −.00, SE = .01, p = .834), whereas mothers rating their child as high in O/R decreased in Neuroticism (d = −.06, SE = .01, p < .001). Again, mothers rating their child as low in O/R had higher Neuroticism at T1 and they remained at this higher level (see supplementary Figure 5).
For Positive Emotions, relationship satisfaction (b = −.01, SE = .00, p = .005) and Child O/R (b = .03, SE = .01, p < .001) remained significant moderators in the multiple moderator models, but the effect of education was rendered non-significant (b = −.02, SE = .01, p = .012). Separate change score models showed that mothers rating their child as low in O/R decreased in Positive Emotions (d = −.03, SE = .01, p = .003), whereas mothers who rated their child as high in O/R did not change (d = .04, SE = .01, p = .039). As shown in Figure 3b, participants rating their child as higher in O/R at T2 had higher level of Positive Emotions at T1, and they increased in Positive Emotions, whereas participants rating their child as lower in O/R at T2 remained at their lower level of Positive Emotions. Finally, the change scores of participants with low vs. high in T1 relationship satisfaction did not reach significance for either group (low-RS participants d = .02, SE = .01, p = .064; high-RS participants d = −.02, SE = .01, p = .055). Selected moderation effects for Extraversion and its facets.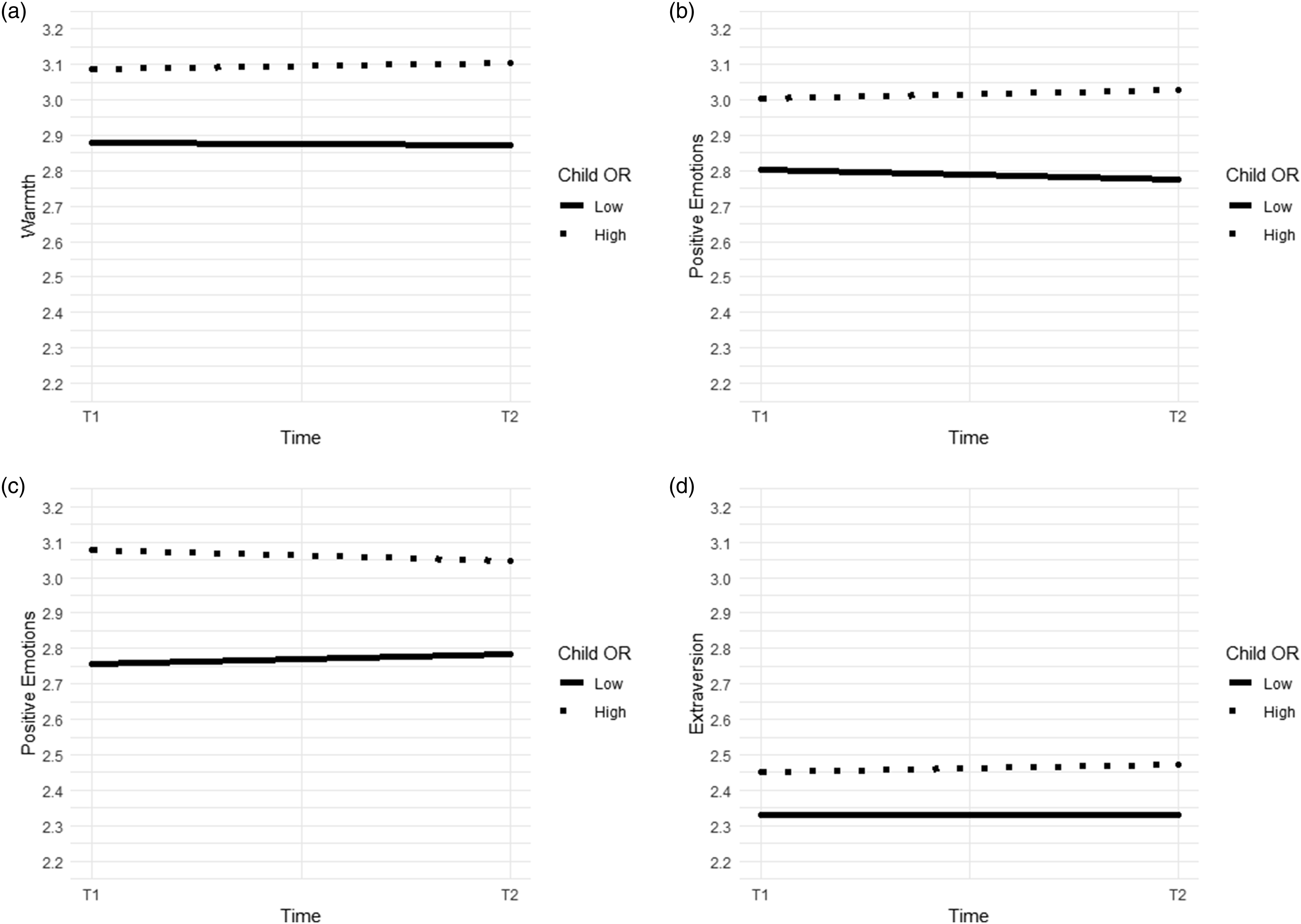
Figure 2 depicts a selection of moderation effects for Neuroticism facets, and Figure 3 depicts a selection of moderation effects for Extraversion facets (the moderator was split at the median, and changes for participants low vs. high on the moderator were plotted as separate lines from raw data). Moderation effects not depicted in Figures 2 and 3 are presented in the online Appendix (https://osf.io/q45f6/), Figures S1–S6. Figures were created with the ggplot2 package in R.
For completeness, we ran additional moderation analyses for the parity and education variables, because they were treated as continuous in the above presented analyses, and binary comparisons may be more appropriate for these variables. First, we ran additional analyses using a binary parity variable with primiparity (mothers expecting their first child) coded as 0 and multiparity (mothers expecting their second or subsequent child) coded as 1, again using the p < .01 as the approximate cutoff point for significance. In these analyses, parity significantly moderated change in Hostility (b = .06 SE = .02, p = .002): primiparous mothers decreased in Hostility (d = −.06 [−.08, −.03], SE = .01, p < .00001), but multiparous mothers did not change (d = −.00 [−.03, .02], SE = .01, p = .929); this effect is plotted in the supplementary Figure S7 (https://osf.io/q45f6/).
Second, we ran the moderation models for education using dummy coded education variables comparing each education level in turn against the other three levels combined. No significant moderation effects by education (at p < .01) emerged from these analyses; however, some contrasts for Depression, Hostility, Positive Emotions, and Excitability were close to significance (ps < .02). For interest, changes in these facets as a function of education level are plotted in supplementary Figures S8-S11 in the online Appendix (https://osf.io/q45f6/).
Discussion
To sum up the results, (1) affective facets of Neuroticism decreased from pregnancy to post-partum, whereas Neuroticism facets related to self-regulation and self-consciousness increased, (2) few changes in Extraversion were found, (3) mother-perceived difficult child temperament was related to the attenuation of desirable personality change (e.g. Anxiety decreased only among mothers rating their child as low in Negative Affectivity) and to enhanced undesirable change (e.g. mothers who rated their child as low in Orienting/Regulation increased in Impulsivity more than mothers rating their child as high on this trait), and (4) objective stressors (e.g. pregnancy-related or birth complications) had virtually no moderating effects on personality change. In what follows, we first discuss the general change results and then, the moderation results.
Personality change from pregnancy to post-partum
Neuroticism facets Anxiety, Hostility, Depression, and Vulnerability decreased from pregnancy to post-partum, whereas Impulsivity and Self-Consciousness increased. What could explain this pattern? These results are partly in line and partly contrary to the theoretical predictions of both the Five-Factor model – which would predict no changes – and SIT (Roberts & Wood, 2006) – which would predict overall decreases in Neuroticism. However, given that most results up until now have shown either no changes (e.g. Asselmann & Specht, 2020; Specht et al., 2011) of increases in Neuroticism (e.g. Jokela et al., 2009) after having a child, it seems clear that parenthood-related personality development is more complex. The present study brought a relatively novel aspect into this discussion—personality facets changing into different directions after having a child. This cannot be explained by mothers investing vs. de-investing into the maternal role, which would mean that mothers changing their behavior according to the demands of the maternal role would change toward maturity, and mothers not changing their behavior according to the maternal role would not change or change toward immaturity. As both mature and immature changes within the same trait were observed, investment vs. de-investment explanation does not seem likely.
Given that the current research was exploratory, all explanations at this point are somewhat speculative. However, the observed change pattern can be understood within the perspective of the TESSERA framework (Wrzus & Roberts, 2017). Notably, all Neuroticism facets that decreased were affective—tendencies to worry and feel vulnerable, sad, and angry went down, whereas the more directly behavioral facet of Impulsivity and the facet of Self-Consciousness, which taps more complex social emotions such as embarrassment and shame, went up. Having a newborn may trigger feelings of happiness and contentment, which are likely to diminish negative feelings. According to the TESSERA model, such repeated emotional instances—that are also in line with the new social role—may eventually lead to changed affect-related self-views, which are then evident in self-ratings of the affective facets. By contrast, taking care of a baby full time may put participants to new types of situations in which it is difficult to maintain self-control, for instance because of lack of sleep or increased daily duties, and such a development may have led to increases in Impulsivity. Furthermore, having a baby or a baby and an older child or children may also increase the likelihood of getting into complex situations that may have the potential to evoke feelings of embarrassment or guilt, such as being at a grocery store with a crying infant, or forgetting an appointment due to fatigue or mental overload. Again, the TESSERA model would suggest that repeated occurrences during which a new mother sees herself as behaving in an impulsive way, or feeling self-conscious, may eventually lead to changed self-views (Wrzus & Roberts, 2017).
More generally, it seems possible that during the first year of motherhood (whether with one’s first or subsequent child) the positive aspects of parenting a newborn diminish the tendency to feel negative emotions. For instance, parenthood has been connected to the experience of having a meaningful life (Umberson & Gove, 1989) which may counteract feelings of anxiety, sadness, and vulnerability. Future studies following facet-level change in Neuroticism for longer time periods will be able to show whether the changes observed here are enduring.
Out of Extraversion facets, only Excitability showed significant change—it decreased. This result is in line with several previous studies showing declines in Extraversion after having a child (Asselmann & Specht, 2020; Galdiolo & Roskam, 2012, 2014; van Scheppingen et al., 2016). The present results suggest that these declines may be particularly due to declines in Excitability. This may be due to Excitability measuring tendencies to do things for fun and excitement, and to experience thrill. It seems plausible that mothers of newborns feel that such tendencies are diminished during the post-partum time, as taking care of a newborn typically requires a lot of effort and presence of mind, and leaves little room for wishing extra stimulation. In general, the results suggested that Extraversion remains mostly unchanged from pregnancy to 6 months post-partum, except for some facets in some subgroups, as discussed next.
One additional issue warrants mention—while Impulsivity is considered to be a facet of Neuroticism under the Five-Factor model (McCrae & Costa, 1989), it is both substantially and conceptually also related to the trait Conscientiousness (e.g. Whiteside & Lynam, 2001). Thus, the increases in Impulsivity observed here are in line with the Conscientiousness declines observed in previous studies (Denissen et al., 2019; Pusch et al., 2019; Specht et al., 2011), as well as recent results showing self-control difficulties among new mothers (Van Scheppingen et al., 2018).
Moderated change
Mother-rated child temperament, especially the temperament trait Orienting/Regulation, moderated change in several facets and in both traits. In essence, mothers who perceived that their child had a more difficult temperament (here, low Orienting/Regulation and/or high Negative Affectivity) showed weaker desirable changes and stronger undesirable changes in their personality than mother rating their child as easy. For instance, mothers rating their child’s temperament as easy declined in Anxiety and Vulnerability, and increased in Warmth, suggesting that child’s easy temperament enhanced mature changes in self-views (see Figure 2).
Children with high Orienting/Regulation are easy to sooth and show high self-regulatory capacity, and children with low Negative Affectivity exhibit low levels of negative affect and distress (Gartstein & Rothbart, 2003). Thus, on average, the everyday lives of mothers with children with high Orienting/Regulation and/or low Negative Affectivity are likely to include less stressful and more rewarding situations, more positive affect, and perhaps more experiences of successful parenting. Thus, it is plausible that these mothers experience early parenting more positively than mothers with infants with more difficult temperament. In sum, the present results suggest that such differences in everyday life experiences during early parenthood are reflected in mothers’ short-term personality development.
The above described results are not surprising, as previous research has robustly shown that mother-perceived difficult child temperament is related to more difficult early motherhood experiences (e.g. Denis et al., 2012; McGrath et al., 2008; Porter & Hsu, 2003). Furthermore, stressors and negative life events and situations have been shown to decrease desirable change and enhance undesirable change in personality (Hicks et al., 2012; Leikas & Salmela-Aro, 2015; Lüdtke et al., 2011; Roberts & Bogg, 2004). However, the present results are among the first to provide a detailed account of how perceptions of child temperament may relate to facet-level personality development across the transition to parenthood.
Mother-ratings of child temperament may have been affected by mothers’ tendencies to perceive their child in a certain way. That is, it is unclear whether children’s actual behavioral differences or mothers’ perception tendencies were related to the mothers’ personality changes. Mothers with high anxiety (e.g. Britton, 2011), or depressive symptoms (e.g. Britton, 2011; McGrath et al., 2008) tend to rate their child’s temperament as more difficult. Similarly in the present study, mothers rating their child as low in Orienting/Regulation or high in Negative Affectivity at T2 had higher levels of Anxiety (Figure 2b), and lower levels of Warmth and Positive Emotions (Figures 3a and b) at T1. Thus, differences in mother-rated children’s temperament observed here may reflect actual differences in children of mothers with higher vs. lower level of those facets, a tendency of mothers with high Anxiety and/or low Positive Emotions or Warmth to perceive their children as more difficult, or both.
As fathers also rated children’s temperament, we were able to overcome the above described entanglement to some extent. Father-ratings of children’s temperament correlated only moderately with mother-ratings. However, father-rated child temperament traits had very similar moderating effects on mothers’ personality changes as mother-rated child temperament on Vulnerability and Self-Consciousness change, suggesting that at least for these facets, actual child temperament may have been the moderator of change. Furthermore, we note that a substantial body of evidence shows that high-Neuroticism individuals report more stress—especially interpersonal stress—in their daily lives (e.g. Bolger & Schilling, 1991; Borghuis et al., 2020; Gunthert et al., 1999). High-Neuroticism individuals also tend to react more intensely to stressors than low-Neuroticism individuals (e.g. Bolger & Schilling, 1991; Gunthert et al., 1999). Thus, a socio-emotional dynamic in which participants with high Neuroticism react to child’s difficult behaviors with more distress than low-Neuroticism participants, and such reactions, in turn, lead to less desirable maternal personality development, seems plausible.
Maternal pregnancy-related stress at T1 moderated change in Depression in an unexpected way: participants reporting higher T1 pregnancy-related stress decreased more in Depression than participants reporting low T1 pregnancy stress. However, as is evident from Figure 2b, these results were likely due to low-stress participants having very low initial levels of Depression. Thus, while a decline in Depression from pregnancy to post-partum seems to have been the typical development in the current sample, low-stress participants simply did not have as much room to decline in Depression as high-stress participants had.
Objectively measured stressors such as a pre-existing mental health diagnosis, physical pregnancy complications, a complicated labor, or premature birth, all derived from medical registers, had no moderating effects on personality change in the present study. This suggests that at least in the present sample, parenthood-personality change link was less affected by health-related objective hardships, and more by mothers’ subjective experiences and by (mothers’ perceptions of) child temperament. The only exception was Hostility, which was moderated by parity status (when parity status was considered as binary): primiparous mothers decreased in Hostility, but multiparous mothers did not. It seems plausible that this pattern is related to the differences between having one newborn and a newborn and older child(ren); the latter situation typically involves more daily emotional and physical labor. Higher everyday life workload of multiparous mothers may have hindered the decline in Hostility that described the personality development of primiparous mothers.
The moderated change results are broadly in line with previous studies showing that parenting challenges and stressors are related to undesirable personality changes (Hutteman et al., 2014; Sirigano & Lachlan, 1985), as well as in line with SIT and TESSERA models: stressors may hinder mature, desirable change, whereas lack of stressors promotes such change. In sum, it seems possible that the inconsistency in the results of parenting and personality change research could be partly explained by moderating factors attenuating or amplifying change in some subgroups (see also Denissen et al., 2019), at least when considering changes in the earliest stages of parenthood. However, it should be noted that the moderator effects we detected were very small. Thus, while these effects were significant and theoretically reasonable, it seems unlikely that the moderators considered here would strongly influence parenthood-related personality development.
Limitations
The most important limitation of the present study was the lack of a control group of non-parents. We cannot conclude that the changes observed are due to having a child; it is possible that they were normative age-related changes that coincide with the age range that our participants represent (Roberts et al., 2006). However, given that the follow-up period was about 1 year, it seems unlikely that significant changes would have happened solely due to aging. Furthermore, Neuroticism typically decreases with age, and we found both increases and decreases at the facet level of Neuroticism.
Another important limitation was, however, the brief follow-up period. The T2 measurements were obtained when participants’ children were around 6 months old. This is a very short time both in the context of parenthood and personality development. In addition, parenting an infant is different from parenting an older child. It should also be noted that some previous studies following new parents longer have found no personality changes among parents (Neyer & Asendorpf, 2001; van Scheppingen et al., 2016). A particularly relevant longitudinal study on self-esteem, a construct that is conceptually and empirically related to Neuroticism, found increases in self-esteem in a follow-up from pregnancy to 6 months post-partum, but a weak, linear decrease in self-esteem from 6 months to 2.5 years post-partum (van Scheppingen et al., 2016). Thus, it is possible that the overall positive changes observed here—that is, decreases in the affective facets of Neuroticism—will be reversed later. Our results should be taken as describing short-term childbirth-related changes specific to the period from pregnancy to the newborn phase.
Having only two measurement points was another methodological limitation. With only two time points, we could not model slope as a latent variable, nor investigate non-linear change. Furthermore, an obvious limitation was that the sample was all-female. This is especially unfortunate given that the experience of having a child as well as early parenting is very different to new mothers vs. fathers. Finally, measuring only Neuroticism and Extraversion, and not the other three Big Five traits is also a limitation. It would be desirable to investigate longitudinal facet-level changes in other traits, both in general and in relation to life events.
Finally, we acknowledge that the moderation effects were very small, and, as power analysis was not conducted prior to data collection, it is possible that our sample was underpowered for detecting of such effects. Therefore, interpretation of the moderation results should be very tentative.
Conclusion
The present research provided novel information on facet-level changes in mothers’ Neuroticism and Extraversion after having a child. The results showed that factor-level personality change, or the lack thereof, may mask heterogeneity in facet-level change. Furthermore, mothers’ perceptions of their child as having a difficult temperament attenuated desirable change in several facets, and amplified undesirable change in Impulsivity. Overall, the results point to the importance of investigating facet-level change in personality across life transitions, suggest that mother-perceived child temperament is an important factor in maternal postpartum experiences, and support the view that individual differences play a role in understanding the dynamics between life events and personality development.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Academy of Finland, Grant numbers 266076 and 309537; Academy of Finland: University of Helsinki Funds; European Union’s Horizon 2020 Award SC1-2016-RTD-733280 for Research on European Children and Adults Born Preterm (RECAP); European Commission Dynamics of Inequality Across the Life-course: structures and processes (DIAL) No 724363 for PremLife.
Data accessibility statement
The data is not open access because (a) it contains participants’ sensitive medical information and (b) in the original informed consent, participants were assured that the data they provided would only be available to the researchers in the PREDO project, and (c) given the dearth of information in this dataset, as well as the public information regarding its collection, it would not be impossible to identify a participant, were the data to be made open access. Analysis scripts, supplementary Tables and Figures, and details of measurement invariance calculations are available in the online Appendix at ![]() .
.