
Abstract
Objective
This review summarized the literature on employer-sponsored workplace wellness programs (WWP) to reduce cardiovascular disease (CVD) risk factors in employees at-risk for CVD.
Data Source
Using keywords related to WWP and CVD, a comprehensive search was conducted for articles published between 2000-2024 in PubMed, CINAHL, PsycINFO, ABI/INFORM, and Web of Science.
Study Inclusion and Exclusion Criteria
Original, peer-reviewed quantitative research articles comparing employer-sponsored WWP to a control or comparison group to reduce CVD risk factors in civilian adults that were at-risk for CVD were included.
Data Extraction
Summary tables included program/intervention, occupation/industry category, employer size, participant sample size, participant characteristics, outcomes, and other key information.
Data Synthesis
Intervention results and overall quality of the articles were evaluated to determine the state of the literature and whether WWP yielded statistically significant improvements in CVD-related outcomes.
Results
Eighteen articles met eligibility (including 7 randomized controlled trials). Systolic and diastolic blood pressure were the most commonly studied outcomes. Most studies reported non-statistically significant results, but nearly half found significant improvements in systolic blood pressure.
Conclusion
This systematic review found mixed evidence on the effectiveness of WWP to improve CVD risk factors. By focusing on at-risk employees and objectively measured biometrics, this review provides a more targeted synthesis of the evidence. Future studies should consider longer interventions and a randomized approach to augment the rigor and interpretability of intervention findings.
Keywords
Objective
Cardiovascular diseases (CVD) have remained one of the major causes of death in the United States since 1920 1 and are the leading cause of death and disability among workers.2,3 CVD encompass a range of heart and blood vessel diseases including hypertension, coronary heart disease, congestive heart failure, stroke, and atrial fibrillation, among others. 1 The American Heart Association estimates that 49% of the U.S. population had some form of CVD between 2017-2020. 4
While health behaviors (e.g., tobacco use, diet, exercise) are often addressed by community-based efforts to reduce CVD, the role of the workplace may be overlooked. 2 Characteristics of the workplace may both drive CVD and present a unique opportunity to deliver services and support. Work is linked to about 10-20% of all CVD deaths in middle-age populations.5,6 Various factors specific to employment (e.g., shift work, work-life balance, sedentary labor, heavy physical exertion, environmental hazards) pose concerns for the onset and worsening of CVD.2,5,7,8 For example, a systematic review found that work-related stress was significantly associated with CVD and CVD-related mortality in 13 out of 20 prospective cohort studies and randomized controlled trials (RCTs). 8
Furthermore, there are considerable indirect costs of CVD that stem from lost productivity, absenteeism, and presenteeism (i.e., when employees are present but working at reduced capacity due to illness) in the workplace that have economic consequences both for employers and employees.1,9,10 The American Heart Association estimates that the indirect costs from CVD reached $184.6 billion between 2020-2021. Data from the 2019 Panel Study of Income Dynamics estimated that employees with heart disease received on average $13,463 less in annual income compared to those without heart disease, and employees with stroke received about $18,716 less. 11 These figures amounted to approximately $203.3 billion lost in total labor income for heart disease and $63.6 billion for stroke, far greater than labor income losses associated with premature mortality. 11 Likewise, a 2012 study found that each short-term disability claim filed because of a heart attack or chest pain resulted in $8,000 in lost productivity, with long-term claims generating over $52,000 in lost revenue to employers.1,12
On the other hand, employers are in a unique position to promote cardiovascular health and reduce CVD through workplace wellness programs (WWP). 13 Employers may invest in WWP to increase employee satisfaction and retention and diminish revenue losses associated with disease-driven reductions in work productivity. Additionally, working-age adults spend more than half of their waking lives engaging in work and related activities. 14 The sheer contact that employees have with their workplace suggests that WWP may be an opportunity for employees to enhance their cardiovascular health. 15 Additionally, the goal-oriented, congregate nature of workplace settings may exemplify the core mechanisms of effective group-based interventions (e.g., peer support, team cohesion, group coherence, accountability, shared experiences) that promote healthy behaviors and program participation.16,17 Finally, as the number of employers offering WWP increases, 18 there is more availability of the infrastructure and resources needed for employers to adopt and expand these health interventions.5,19,20 For example, the National Institute for Occupational Safety and Health (NIOSH) has disseminated a Total Worker Health framework that guides employers in health promotion efforts.21,22 Increasing the proportion of worksites that offer a WWP is also one of the Healthy People 2030 objectives. 23
Despite the opportunity for employers to advance cardiovascular health, past research has not systematically examined the characteristics or effectiveness of WWP to promote cardiovascular health in the U.S., particularly among at-risk populations who may benefit from WWP the most. 24 Prior reviews have often included non-U.S. populations, broad workforce samples, wide-ranging physical health outcomes, and often self-reported outcomes. 25 However, several relevant systematic reviews have considered CVD risk factors.
A systematic review that focused on male-dominated industries found little evidence of intervention effectiveness on systolic or diastolic blood pressure. 25 A 2010 review found no evidence for a positive effect of workplace lifestyle interventions on blood pressure, serum lipid profile, blood glucose, or triglycerides. 26 On the other hand, a 2021 meta-analysis investigating interventions to improve diet and cardiometabolic risk factors found positive effects on LDL and HDL cholesterol, triglycerides, diastolic blood pressure, and fasting glucose; though the study only included multicomponent interventions targeting the overall workforce rather than at-risk populations or specific cardiometabolic diseases. 27 An umbrella review examining the effects of workplace interventions on type 2 diabetes, CVD, mental health, and musculoskeletal disorders identified 5 reviews that included measures of cardiovascular health, 28 but focused on non-U.S. populations, were limited to specific sectors (e.g., industrial workers), examined a broad variety of health outcomes, or had limited evidence for biometric measures of hypertension, diabetes, and high cholesterol.22,26,29-31 Another umbrella review examined workplace interventions for musculoskeletal disorders, psychological and behavioral disorders, and older employees, but did not focus on CVD. 32
In contrast, this review specifically focuses on U.S.-based WWP targeting employees with elevated cardiovascular risk factors, restricts inclusion to studies with pre/post comparative designs (excluding descriptive or educational-only programs), and emphasizes objectively measured biometric outcomes (e.g., blood pressure, HbA1c, cholesterol, glucose). By narrowing our focus to at-risk populations and objectively measured outcomes, this study provides a more rigorous and clinically relevant synthesis of the evidence base and identifies methodological weaknesses that future workplace cardiovascular health research must address. As such, this systematic review aimed to collate and elucidate the research literature on employer-sponsored WWP for employees at risk of CVD in the U.S.
Methods
This study examined health outcomes resulting from employer-sponsored WWP that targeted cardiovascular health for at-risk employees. We registered the systematic review in the International Prospective Register of Systematic Reviews (PROSPERO; ID #1338287). We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) approach to document the identification of eligible articles (Figure 1).33,34 We used the Rayyan
35
systematic review software for article screening, Zotero
36
reference management software for article storage and organization, and Microsoft Excel for manual data extraction.
Data Sources
A health sciences librarian conducted literature searches in PubMed using both a keyword search (Supplemental Table 1) and a Medical Subject Headings (MeSH) search (Supplemental Table 2). Keyword searches were also performed in CINAHL, PsycINFO, ABI/INFORM, and Web of Science. A search algorithm was used to query for peer-reviewed, English-language articles published between January 2000 – June 2024 using keywords related to (1) the workplace, (2) health or wellness, (3) programs or interventions, and (4) cardiovascular or metabolic disease. Titles and abstracts were exported to the Zotero 36 reference management software where duplicates were removed and initial eligibility was assessed. Articles that specifically measured CVD biometrics were then identified using an in-depth eligibility screening protocol.
Inclusion and Exclusion Criteria
Inclusion criteria included (1) original, peer-reviewed research articles that (2) addressed programs or interventions related to health promotion, safety, maintenance, screening, or treatment of cardiovascular or metabolic disease (hypertension, hyperlipidemia, hypercholesterolemia, atherosclerosis, atrial fibrillation, heart failure, acute myocardial infarction, stroke, or diabetes). 37 Articles had to (3) evaluate an employer or worksite-based program or otherwise target employees of a specified entity, (4) be available in English and describe programs or interventions that were conducted in the U.S., (5) include adult employees (ages 18 or older), and (6) focus on civilian populations. Additionally, articles had to (7) present original research involving primary data collection that (8) reported quantitative findings, and further, (9) compare findings from an intervention group to a control or comparison group and (10) describe research that targeted workers who were identified as “at-risk” for adverse health outcomes. (11) In the event that more than one article described similar findings from the same study, only the article presenting the most up-to-date or comprehensive study results was included. A detailed list of inclusion and exclusion criteria can be found in Supplemental Table 3.
Eligibility Screening
For the first screen, articles were sorted alphabetically by author name and evenly split for review by a health sciences librarian and a health services researcher. Titles/abstracts that clearly did not meet inclusion criteria were flagged for exclusion. Titles/abstracts were then reassigned to the opposite reviewer for further review. Articles that were flagged for exclusion by both reviewers were removed.
Next, articles were imported into the Rayyan 35 systematic review software for a second screen that provided an in-depth examination of the remaining titles/abstracts. Both reviewers screened the titles/abstracts to exclude any articles describing workplace interventions that did not address cardiovascular or metabolic disease. Discrepancies were discussed and were resolved between reviewers when possible, while any conflicts or ambiguous titles/abstracts were retained.
Finally, a third screen was conducted using the full texts of the remaining articles. To begin, a subset of ten articles were screened by both reviewers to improve inter-rater reliability. Disagreements were resolved through group-based discussion with the entire study team; clarifying notes were added to the inclusion/exclusion criteria before proceeding with the remainder of the full-text review. Potentially eligible articles were tagged with the specific chronic condition(s) that were targeted, and ineligible articles were tagged with the primary reason for exclusion. Articles that generated conflicting decisions by the two reviewers were flagged for adjudication by one of the two project leads (a medical psychologist and a mixed methods researcher), whose decision was then brought to the larger study team meeting for discussion and a final verdict. The rationale for the final inclusion or exclusion decision was also documented. The reference sections of the remaining eligible articles were scanned for additional articles that were unidentified by the initial literature search. Throughout the review process, the study team met weekly to discuss questions, address inconsistencies, highlight emerging themes, and further refine the details of inclusion/exclusion criteria when additional specificity was needed.
Data Extraction
Data from the final sample of articles was extracted into an Excel spreadsheet by the health sciences librarian and two health services researchers. Elements for data extraction were chosen a priori and grounded in a core set of recommended health metrics for the evaluation of employee health management programs, developed by the Health Enhancement Research Organization (HERO) and Population Health Alliance. 20 The following data elements were extracted when available: author name; publication year; article title; number of worksites included in the program/intervention; free-text descriptions of the worksite/occupation type; employer size (under vs over 5000 employees, based on prior classifications used in national datasets and large-employer surveys38,39); participant sample size (exact number, when reported); free-text descriptions of sociodemographic and clinical characteristics of participants at baseline (when reported); free-text descriptions of the program/intervention; free-text descriptions of the interventions’ goal or target condition; conditions targeted by the intervention (hypertension, cholesterol, diabetes, or other cardiovascular condition, reflecting selected HERO metrics guidelines 20 ); years during which the intervention was administered; duration of the intervention in weeks/months/years; delivery mechanism(s) by which the intervention was administered (in-person, online, and/or telephonic, per the HERO metrics guidelines 20 ); whether monetary incentives were provided (e.g., cash, gift cards, cost-sharing incentives (coded as yes/no)); whether the study was grounded in theory or a conceptual framework (yes/no); whether an RCT design was used (yes/no); whether pre-/post-measures were reported (yes/no); and free-text descriptions of the authors’ key findings and recommendations. All extracted data was cross-checked for accuracy by three team members.
Additionally, we conducted a quality assessment of the articles using criteria established by the National Heart, Lung and Blood Institute (NHLBI) for before-after (pre-post) studies with no control group and case-control studies (NHLBI, 2021). 40 These quality assessment tools are frequently used for systematic reviews to assist reviewers in examining concepts key to a study’s internal validity.
Data Synthesis
Study Characteristics (N = 18)
Abbreviations: NR: Not reported; Y: Yes; N: No; RCT: Randomized controlled trial; SBP: Systolic blood pressure; DBP: Diastolic blood pressure; HbA1c: Hemoglobin A1C; HDL: High-density lipoprotein; LDL: Low-density lipoprotein.
*The underlying NIH Diabetes Prevention Program model is based on social cognitive theory.
Intervention Outcomes
Notes. Results reflect between-group differences between intervention and comparison/control groups. Significant differences are noted in bold.
(+) Significant improvement
(-) Significant worsening
(NS) Non-significant results.
Abbreviations. SBP: Systolic blood pressure; DBP: Diastolic blood pressure; HbA1c: Hemoglobin A1C; HDL: High-density lipoprotein; LDL: Low-density lipoprotein.
Summarized Intervention Outcomes
Notes. If results were reported for multiple follow-up time points (e.g., Faghri and Li, 2014 and Weinhold et al, 2015), only results for the follow-up point closest to the intervention is reported. However, this distinction only affected our reporting of HDL cholesterol and glucose by Weinhold (2015), who observed non-significant effects for HDL cholesterol and significant improvements for glucode at the 4-month follow-up (reflected in this table), but then saw significant improvements in HDL cholesterol and non-significant effects for glucose by the 7-month follow-up (not reflected in this table). For Cohen, only the pooled estimates from the combined sample of pre-diabetics and diabetics) were reported. Pooled estimates were also used for Misra-Hebert (2016). Results from the three intervention arms reported in the single article by Cheon et al (2020) are each included here and thus treated as three separate study populations.
Abbreviations. HDL: High-density lipoprotein; LDL: Low-density lipoprotein.
Quality of the Articles and Their Interventions
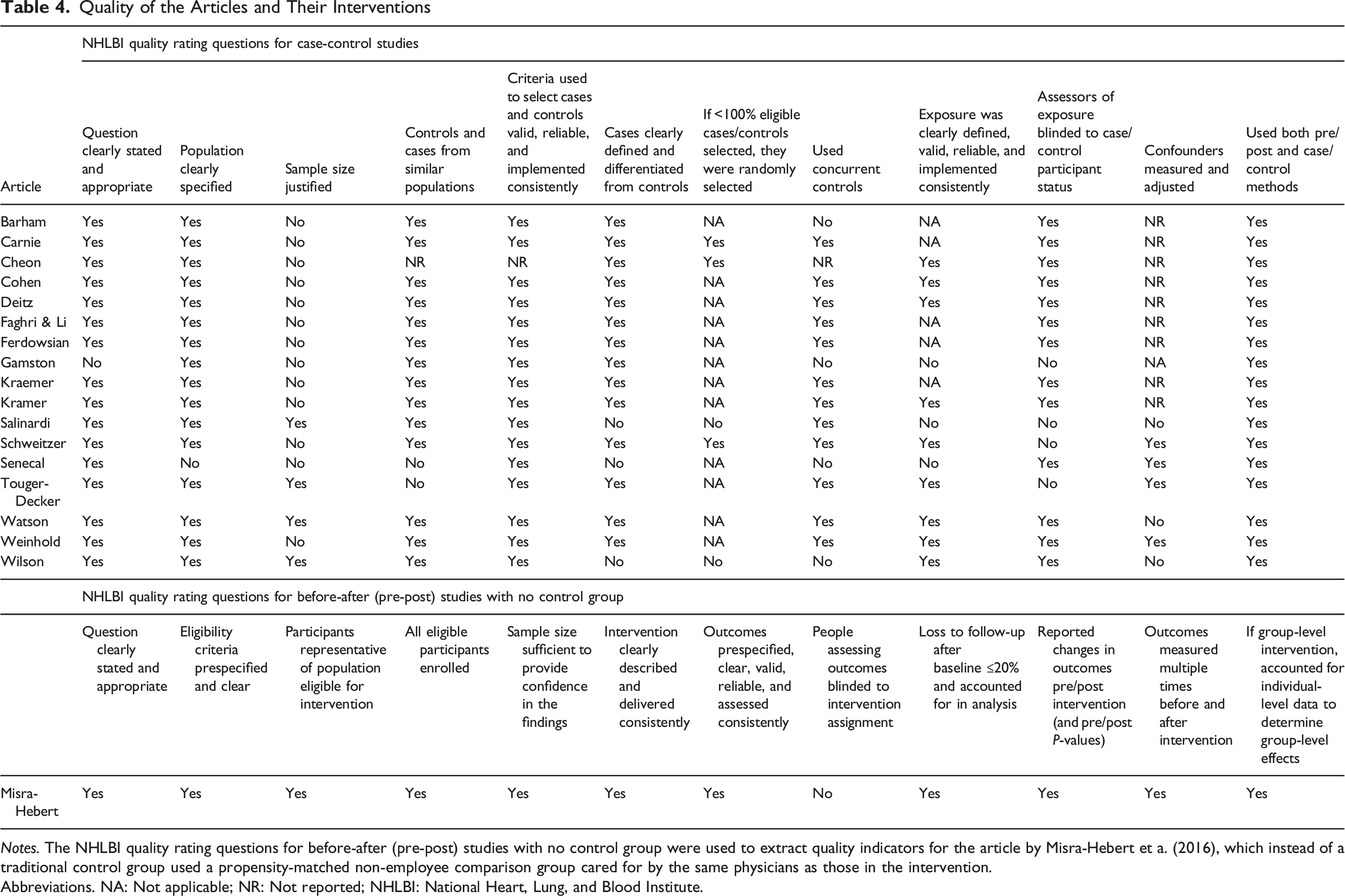
Notes. The NHLBI quality rating questions for before-after (pre-post) studies with no control group were used to extract quality indicators for the article by Misra-Hebert et a. (2016), which instead of a traditional control group used a propensity-matched non-employee comparison group cared for by the same physicians as those in the intervention.
Abbreviations. NA: Not applicable; NR: Not reported; NHLBI: National Heart, Lung, and Blood Institute.
Results
Sample
Our keyword and MeSH searches (Supplemental Tables 1 and 2) yielded a total of 2513 records (Figure 1). Of these, 862 were identified as duplicates. Among the remaining 1651 unique articles, 1227 were determined as irrelevant and thus excluded during the initial title/abstract screen. After a second screening of the remaining potentially relevant titles/abstracts, an additional 330 articles were excluded. This left 94 articles for a full-text review, including a review of their reference sections. Of those, 14 articles met eligibility criteria whereas 80 were excluded because they did not meet inclusion criteria. The most common reason for exclusion was that the study did not include or compare results from an intervention group to a control/comparison group. We also conducted a reference review of the 94 articles that were eligible for a full-text review. The reference review identified four additional articles that met inclusion criteria. Our final analytic sample included 18 articles.41-58 A PRISMA flowchart detailing the progression of article identification, screening, and inclusion is depicted in Figure 1.33,34
Study Characteristics
The design and study characteristics of each intervention are characterized in Table 1. The final sample of eligible articles were published between 2010 47 to 2023. 53 Most studies included multiple worksites, and occasionally multiple employers, across a diverse sample of occupations and industries including health care delivery organizations, universities, government agencies, insurance providers, IT/computer companies, pharmaceutical and medical suppliers, consumer goods businesses, office worksites, and retail. The number of worksites per intervention ranged from 1-7 among the 13 articles that quantified this information.41,42,45-50,52,54-57 Participant sample sizes ranged from 4141 to 24,117 43 ; the average sample size was 1645 and the median was 104 participants. Examples of populations characterized as “at-risk” for negative health outcomes included individuals with prediabetes or type 2 diabetes, who were overweight (BMI ≥25), had hypertension, out-of-range biometric values of systolic BP or diastolic BP, high cholesterol, metabolic syndrome, or other known risk factors for CVD. Participant demographics and their clinical metrics at baseline are also summarized in Table 1.
Across studies, the interventions were administered between 2006 55 to 2019, 48 though the intervention period was not specified in 6 articles.42,45-47,49,53 The duration of the interventions varied from 2-24 weeks in a few studies to 1-2 years in others. The articles captured a range of health interventions across 18 states that included intensive lifestyle interventions, nutrition interventions, diabetes prevention programs, and digital health interventions, among others. All except one of the interventions included an in-person component (17/18).41-55,57,58 Eight studies included web-based components42,45,48,52,54-56,58 and three included telephonic components.47,50,56 Monetary incentives were provided in 11 studies.42,43,45-51,54,56 There were 9 study designs that were theory-driven41-43,46,48,50,52,57,58 and 7 RCTs.42,45,46,49,52,53,56 All studies conducted traditional pre/post analyses among the intervention group with the exception of Cohen et al, 44 who used propensity scores to match clinic users in 2016 to a group of non-users with similar characteristics from 2015 to 2016. Attrition rates ranged from 3% to 31% (Supplemental Table 4).
Intervention Outcomes
Table 2 presents the goals and target conditions of each intervention and indicates whether the intervention yielded between-group differences that were significantly positive (i.e., clinical improvement), significantly negative (i.e., clinical worsening), or non-significant, comparing results for the intervention group to the control/comparison group. Table 3 collapses the condition-specific findings across interventions to summarize the total number of interventions that found significant vs non-significant results by each condition type. Of note, the study by Cheon et al 43 incorporated three distinct intervention arms (i.e., one focused on diabetes prevention, another on hypertension prevention, and the third was a nutrition program). Each of these three arms is counted as a separate intervention for the purpose of Table 3, which in turn summarizes results from 20 interventions across the 18 included articles. Additionally, Table 3 only reports results from the first follow-up time point for the two studies that reported results at multiple follow-up time points.46,57
There were 16 interventions across 14 studies that targeted both SBP and DBP as clinical outcomes of interest,41,43,45-47,49,50,52-58 with one additional study targeting SBP but not DBP. 51 Across the 17 SBP-focused interventions, about half (47.1%) found non-significant results41,43,45,46,49,55,56,58 while the other half (47.1%) found significant improvements for the intervention group compared to the comparison/control group.43,47,50-54,57 In contrast, only 5 of the 16 interventions (31.3%) targeting DBP observed significant improvements.47,52,54,56,57 Significant worsening in both SBP and DBP was observed for the hypertension prevention arm in the multi-armed intervention study by Cheon et al. 43
There were also 16 interventions across the 14 studies that targeted diabetes as a clinical outcome of interest. Blood glucose levels were used as a biomarker for diabetes in 11 interventions,41,43,48-50,52,55,57,58 HbA1C was used in 8 interventions,41,44,47-51,53 and 2 interventions measured effects on insulin resistance (e.g., HOMA: Homeostasis Model Assessment for Insulin Resistance).42,50 Taken together, results across the various interventions tended to err toward non-significance. For example, 45.5% of the interventions targeting blood glucose levels and 62.5% of the interventions targeting HbA1C were non-significant, respectively. However, four of the 11 interventions (36.4%) targeting blood glucose levels43,52,57,58 yielded significant improvements for the intervention group, as did 3 of the 8 interventions (37.5%) targeting HbA1c.50,51,53 Of note, Weinhold et al 57 observed mixed results when examining outcomes at stratified time points, including significant improvements in glucose levels for the intervention group at their 4-month follow-up which were no longer significantly different from trends in the control group by the time of the 7-month follow-up. Likewise, findings differed by clinical subgroups in the study designed by Cohen et al, 44 wherein there were significant improvements in HbA1C levels for the diabetic group, but not for the prediabetic group or the combined group of diabetics plus pre-diabetics.
There were 15 interventions across 13 studies that targeted cholesterol as a clinical outcome and measured participants’ lipid profiles.41-43,47-53,55,57,58 Thirteen of the interventions measured changes in total cholesterol,41-43,47,49,50,52,53,55,57,58 11 measured HDL cholesterol,41,42,47-50,52,53,55,57,58 10 measured LDL cholesterol,41,42,47,49-53,57,58 and 9 measured triglycerides.41,42,47,49,50,52,53,57,58 The majority of interventions examining total cholesterol (10/13; 76.9%), HDL cholesterol (9/11; 81.8%), LDL cholesterol (8/10; 80%), and triglycerides (8/9; 88.9%) reported non-significant changes in the intervention group compared to the control/comparison group. Significant between-group improvement was reported in HDL cholesterol in one intervention. 47 A third study by Weinhold also observed significant improvements in HDL cholesterol at a final (7-month) follow-up, but not in an earlier 4-month follow-up. 57 Two interventions reported significant improvements in LDL cholesterol51,53 and one found significant improvements in triglycerides. 53 The hypertension intervention arm of the study by Cheon observed significant worsening in total cholesterol for the intervention group compared to comparison groups, 43 and Schweitzer observed significant worsening for HDL cholesterol. 53
Quality of Evidence
Table 4 assesses the quality of evidence in each article, guided by the NHLBI quality rating tools. 40 Only one article was a before-after (pre-post) study with no control group. Instead, the study used a propensity-matched non-employee comparison group cared for by the same physicians as the intervention participants. 51 All other studies were based on a conventional case-control research design.
Most articles clearly described their objectives and study populations; however, many did not report or clearly describe key methodological elements. Most articles did not provide a power estimate or sample size justification or clarify the approach used to measure and statistically adjust for potential confounders. The research question or objective and study population were clearly stated and appropriate in 17 of the 18 articles. Of the 17 articles reporting case control studies, only four provided a sample size justification. There was also a high dropout rate among participants in many studies. The attrition rate varied between 3% and 31% across the included studies. However, a high number of articles (n = 5) did not report attrition rates or discuss participant withdrawal from the study. Also, a number of studies reported that some participants (considered completers) did not complete all parts of the intervention or measurement (n = 5) (Supplemental Table 4).
Sixteen articles reporting case control studies included sufficient definitions, inclusion and exclusion criteria, and algorithms or processes used to identify or select cases and controls and 14 articles clearly defined and differentiated the cases from controls. The measures of exposure/risk were clearly defined, valid, reliable, and implemented consistently across all study participants in nine of the case-control articles. Other articles did not clearly describe an approach for consistent intervention exposure or fidelity. There were 14 articles reporting case control studies that selected individuals for the control group from the same or similar population as the case group and there were 12 articles that used concurrent controls. Most articles (13/17; 76%) described a study methodology in which data analysts of the exposure/risk were blinded to the case or control status of participants. Only four articles clearly reported whether key potential confounding variables were measured and adjusted statistically in the analyses.
Discussion
This systematic review assessed the effectiveness of WWP targeting CVD risk factors among at-risk populations. The quality and consistency of results varied considerably across studies, which included a wide range of industries and interventions.
Interventions targeting hypertension, diabetes, and cholesterol showed mixed results. This variability might reflect the heterogeneity in the design of WWP targeting CVD. Furthermore, blood pressure, glucose, and lipid outcomes may be influenced by many factors in addition to individual health behaviors, such as job demands, environmental stressors, workplace culture, and organizational supports. The variety of types of interventions was wide and interventions that focused on individuals’ behavior change (i.e., diet or exercise counseling) may have overlooked structural or psychosocial factors that impede sustained improvement. For example, past research has shown that WWP with favorable outcomes are often embedded within organizations where the corporate culture encourages wellness to improve employees’ lives (not only to reduce costs), where employees and leadership are invested in supporting the WWP, and where corporate policy and the physical environment encourages WWP participation. 59 The inconsistency across studies may signal missed opportunities to address broader organizational determinants of health that WWP should be designed to address. Rather than “just” enacting individually-focused interventions in the workplace, WWP should be designed to take advantage of the workplace environment, leadership, and culture to enhance the intervention. It is not clear that the included studies were designed to take advantage of these opportunities.
Evidence Quality Summary
The quality of research designs varied widely, reflecting findings from other systematic reviews of workplace health interventions.9,15,32,60,61 Major quality issues included a lack of sample size justification, high participant dropout, and inconsistent intervention exposure.
The quality review of the studies highlighted limitations around methodological rigor. From a broader perspective, these methodological gaps also limit our understanding of how and why certain interventions were successful. For instance, few studies reported on implementation fidelity or contextual factors such as management support, incentives, or workload adjustments. These factors are all central to the Total Worker Health 21 framework’s call for organization-level integration. Strengthening study designs to include mixed-method or effectiveness and implementation approaches could capture these critical contextual variables and help to inform scalable program interventions.
Study Implications
This review suggests that, while workplace interventions targeting cardiometabolic outcomes can be beneficial, their effectiveness is variable. This conclusion is consistent with prior meta-analytic evidence extending beyond the U.S., which has found modest improvements but substantial heterogeneity in WWP, particularly among multicomponent interventions targeting dietary behaviors across the general workforce. 27 Our study, which restricted inclusion to studies with objectively measured biomarkers and comparative designs, may reveal more tempered program effects. Additionally, several factors including intervention duration, mode of delivery, and specific health conditions targeted, likely contribute to variability in outcomes. Interventions with longer follow-up periods (e.g., 1-2 years) may provide more sustainable health improvements compared to shorter interventions (e.g., 2-24 weeks). Additionally, interventions combining in-person and digital components may be more effective than those using a single delivery mode, particularly as businesses increasingly incorporate hybrid or fully-remote working environments. As post-pandemic workplace structures continue to evolve, digital and hybrid WWP may become increasingly central to reaching dispersed workforces and sustaining engagement over time.
Limitations
The current systematic review has limitations. Generalizability of the findings is limited since the search was restricted to English-language articles and U.S.-based studies. The search also focused on peer-reviewed articles, which may introduce publication bias, however many studies reported non-significant or negative findings. Since the studies did not provide sample size justifications or power analyses, our review may underestimate potentially clinically important but statistically non-significant results. The heterogeneity of interventions, ranging from in-person to web-based or telephonic, with different durations and delivery mechanisms, made it difficult to directly compare results or draw firm conclusions about intervention effectiveness. There was also variability in outcome measures (e.g., blood pressure, HbA1C) and assessment methods, making it difficult to synthesize findings. Also, body-mass index was not included as an outcome in this review. The research on employer-sponsored weight management interventions is robust and the current review focused on other, less studied CVD risk factors.
Despite these limitations, this review contributes to the literature by systematically synthesizing evidence on WWP focused on CVD risk factors, an area often overshadowed by studies of workplace weight management. The current investigation also had various strengths, particularly the comprehensive and systematic approach informed by the PRISMA framework and the use of an established quality appraisal tool. 40 Additionally, the involvement of a health science librarian and queries across multiple databases ensured a broad and reproducible search strategy. Taken together, these approaches allowed a thorough analysis of the current literature that identifies shared weaknesses that can guide future research.
Conclusions
This review highlights both the promise and the limitations of WWP for improving CVD risk factors among at-risk employees. The mixed evidence reflects not only differences in program design and rigor, but also the broader challenge of achieving sustained health improvements in complex work environments. In conclusion, the following key findings were derived from this systematic review: 1. Employee-sponsored WWP targeting at-risk populations show potential but are not uniformly effective. The review demonstrated that WWP targeting cardiovascular and metabolic health in at-risk employees can lead to significant improvements in specific outcomes (e.g., blood pressure, cholesterol, HbA1C), but the results were inconsistent across studies. This suggests that while WWP hold promise, they may need to be better tailored or refined to achieve consistent, significant health improvements. WWP effectiveness might also benefit from taking a more wrap-around or team-based approach, such as working in combination with a case manager or provider to offer medication management and individualized health services in combination with behavior modification. 2. There is a need for stronger study designs and reporting greater detail of the intervention components. The review highlights gaps in study quality, particularly in areas such as sample size justification, controlling for confounders, and clearly defining control groups. More rigorous study designs, including RCTs, are needed to provide clearer evidence of intervention effectiveness. 3. Significant improvements were observed in certain health outcomes (e.g., HDL cholesterol, systolic blood pressure) more often than others (e.g., total cholesterol and glucose levels). This variability suggests that specific types of interventions may be more effective for certain conditions, again underscoring the importance of tailoring interventions to the specific health needs of at-risk employee populations. 4. Longer-term follow-up and sustained engagement in WWP models are needed. Many interventions had relatively short durations, and the long-term sustainability of the health benefits remains uncertain.
Future research should focus on addressing the methodological limitations identified in this review, particularly regarding sample size determination, control of confounding variables, and consistent implementation of interventions. Furthermore, interventions should be tailored to the specific health risks of different subpopulations to maximize their effectiveness. Multi-component WWP that target at-risk groups might also consider more comprehensive and holistic approaches,10,62 such as complementing the core WWP with access to primary care physicians, nutritionists, or other clinicians that can individualize care and offer wrap-around services. Research is also needed to examine the impact of WWP on organizational financial or economic outcomes to extend sustainability and scalability or to promote upfront investment and employer buy-in. Finally, future analyses should focus on the long-term clinical effectiveness of WWP and the impact that sustained participant engagement may have on ongoing health outcomes.
Ultimately, WWP represent an underused but potentially useful mechanism for positively impacting cardiometabolic outcomes. To fulfill this potential, WWP should be clear and well-designed, consider integrating wrap-around services, and should leverage the unique contextual attributes of the workplace at the organizational level rather than only focusing on individual behavior change. By integrating organizational support into intervention design, WWP will better align with principles of organizational change and support (i.e., Total Worker Health framework
21
) and effectiveness of these interventions may foster sustained improvement in CVD risk factors. Workplace wellness programs (WWP) are widely promoted as a strategy to reduce cardiovascular disease (CVD) risk, yet prior evidence on their effectiveness, especially among at-risk employees, has been inconsistent and limited in scope. This systematic review synthesizes evidence from 18 U.S.-based studies evaluating WWP targeting at-risk employees. It reveals mixed results across key outcomes (e.g., blood pressure, cholesterol, HbA1C), identifies gaps in methodological rigor, and highlights the need for longer interventions and tailored approaches. Health promotion practitioners should design WWP with greater attention to duration, population-specific tailoring, and implementation fidelity. Researchers must strengthen study designs through randomized controlled trials, longer-term follow-up, and improved reporting. Without methodological rigor and sustained engagement, the potential of workplace interventions to reduce CVD risk will remain unrealized.So What?
What is Already Known on This Topic?
What Does This Article Add?
What are the Implications for Health Promotion Practice or Research?
Supplemental Material
Supplemental Material - Workplace Wellness Programs for Employees at Risk for Cardiovascular Disease: A Systematic Review
Supplemental Material for Workplace Wellness Programs for Employees at Risk for Cardiovascular Disease: A Systematic Review by Mary Louise Pomeroy, Carolyn Hoffman, Sravya Vunnam, Axucillia Moyo, Kathleen Butler, Ali A. Weinstein, Debora Goetz Goldberg in American Journal of Health Promotion.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Health Services and Outcomes Research for Aging Populations training program funded by the National Institute on Aging (grant #T32AG066576) and the Epidemiology and Biostatistics of Aging training program funded by the National Institute on Aging (grant #T32AG000247.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.