
Abstract
Purpose
This study aimed to explore the role of bilingual provider preferences in mediating healthcare anxiety and cross-border healthcare access.
Design
A multi-channel sampling was employed to recruit participants from Brownsville, Texas from March to September 2024.
Setting
The research team distributed bilingual (English/Spanish) survey links through partners and community events and promoted the survey via city broadcasts and social media.
Sample
The final analytic sample comprised 144 adult residents of Brownsville.
Measures
The survey items included measures of healthcare anxiety related to providers, preference for bilingual providers, and access to cross-border healthcare, with socio demographics included as covariates.
Analysis
Structural equation modeling examined the relationships between provider-related healthcare anxiety, bilingual provider preferences, and cross-border healthcare access, using path analysis to assess direct and indirect effects.
Results
The analysis revealed a significant positive relationship between provider-related healthcare anxiety and bilingual provider preferences (β = 0.20, P = 0.018). Additionally, bilingual provider preferences were strongly associated with cross-border healthcare access (β = 0.47, P < 0.001). A mediation effect was observed, where bilingual provider preferences mediated the relationship between healthcare anxiety and cross-border healthcare access (β = 0.10, P = 0.04).
Conclusion
Bilingual provider preferences significantly mediate the relationship between provider-related healthcare anxiety and cross-border healthcare access in U.S.-Mexico border communities. These findings emphasize the importance of language concordance in reducing healthcare anxiety and enhancing access to care.
Keywords
Introduction
Healthcare access is a critical determinant of public health and individual physical, mental, and social well-being. 1 Adequate access to healthcare services is essential for managing chronic conditions, preventing diseases, and ensuring optimal health outcomes.2,3 According to previous studies, regular engagement with healthcare services facilitates preventive measures such as screenings and vaccinations, which play a critical role in reducing the incidence and progression of chronic diseases.4,5 In addition, individuals who have consistent access to healthcare services are more likely to receive timely interventions, which can lead to not only improvements in health status but also quality of life. 6 Conversely, restricted healthcare access is associated with delayed diagnoses, inadequate disease management, and poorer overall health outcomes, disproportionately affecting underserved populations. 7
Despite the importance of healthcare utilization, multiple barriers (i.e., structural, financial, cultural, or psychological in nature) can hinder individuals from seeking and receiving necessary care. 8 Structural barriers, such as transportation issues, lack of insurance, and geographic distance from healthcare facilities, can significantly limit individuals’ ability to seek and receive care.9-11 Financial constraints, including high out-of-pocket costs and lack of health insurance, are often cited as key reasons individuals delay or forgo necessary medical care.12,13 Cultural barriers, such as unfamiliarity with the healthcare system and mistrust of medical professionals, can further compound the challenges in accessing care.14,15 Furthermore, among these challenges, language barriers can represent a particularly significant obstacle, 16 especially for individuals with limited English proficiency. 17 The limited English proficiency populations experience increased difficulty in navigating healthcare systems, leading to reduced patient-provider communication quality, misinterpretation of medical instructions, and a higher likelihood of medical errors. 18 These barriers can contribute to healthcare disparities, exacerbating existing inequities in service utilization and health outcomes among minority populations, including Hispanic communities in the U.S.. 19
While language barriers are often cited as a significant issue in healthcare utilization, in U.S.-Mexico border communities,17,20 where most individuals speak Spanish, these barriers may not be as pronounced as expected. However, Spanish-speaking individuals may still experience discomfort or anxiety when interacting with non-Spanish-speaking healthcare providers in the U.S.. 21 Provider-related healthcare anxiety—characterized by apprehension or distress associated with healthcare interactions—can further deter individuals from seeking necessary medical care, 22 contributing to delays in treatment and worsening health conditions. 23 Language and cultural barriers are known to increase healthcare anxiety and decrease health-seeking behaviors,24,25 but the specific impact of these factors in U.S.-Mexico border communities remains understudied, and it is unclear how linguistic and cultural incongruences between patients and providers influence healthcare experiences in this context. In addition, the pattern of healthcare utilization in border communities might differ from conventional conceptualizations of medical tourism, which primarily involve individuals traveling abroad for medical procedures based on cost advantages. 26 Instead, cross-border healthcare access among border residents is often driven by pre-existing social and familial ties, as well as a perception of an interconnected community rather than 2 distinct healthcare systems.27,28
Despite these findings, a gap exists in the literature regarding the role of bilingual provider preferences in mediating healthcare access barriers, particularly in cross-border contexts. While much research has focused on the impact of language barriers on healthcare utilization and the advantages of bilingual providers in mitigating these barriers, there is limited empirical evidence exploring how these factors interact with provider-related healthcare anxiety and the decision to seek care across borders. While studies have separately addressed the barriers of language and cross-border healthcare utilization, the intersection of these factors has not been sufficiently explored. Specifically, there is a lack of research examining how preference for bilingual providers may mediate the relationship between provider-related healthcare anxiety and the likelihood of seeking care across the U.S.-Mexico border.
This study aims to address these gaps by examining the relationships between provider-related healthcare anxiety, bilingual provider preferences, and cross-border healthcare access in U.S.-Mexico border communities. Specifically, this study employs structural equation modeling (SEM) to assess the hypothesized pathways between these variables, providing insights into the mechanisms underlying healthcare utilization behaviors in this population (Figure 1). Hypothesized relationships of the research model; Solid arrows indicate hypothesized direct effects; the dashed arrow indicates the hypothesized indirect (mediated) effect via bilingual provider preference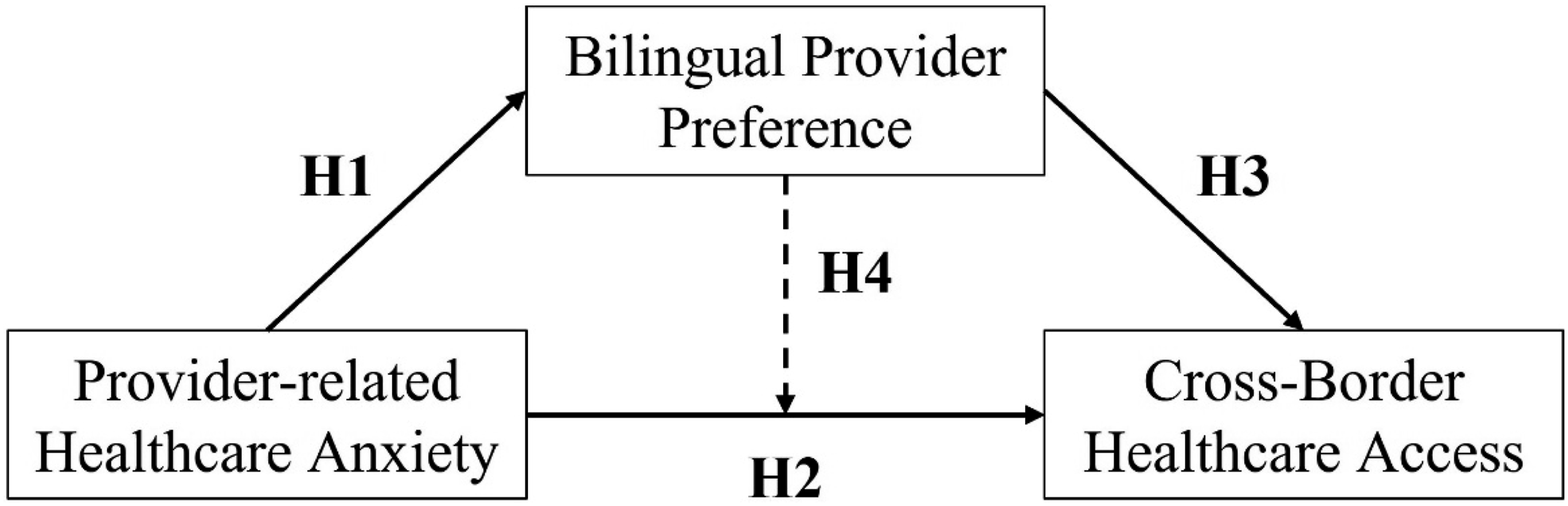
Within the framework of the study’s general purpose, the following hypotheses were formulated:
Provider-related healthcare anxiety is associated with bilingual provider preference.
Provider-related healthcare anxiety is associated with cross-border healthcare access.
Bilingual provider preference is associated with cross-border healthcare access.
There is an indirect effect of bilingual provider preference on the relationship between provider-related healthcare anxiety and cross-border healthcare access.
Methods
Participants and Procedures
A multi-channel sampling strategy was employed to recruit participants from Brownsville, Texas from March to September 2024. The research team partnered with healthcare providers, social service agencies, and religious institutions, who distributed unique survey links to their constituents. To reach populations that may not typically engage with digital methods, intercept surveys were conducted at community events, health fairs, and cultural festivals. In addition, the survey was promoted through city broadcasts, social media platforms, and municipal communication channels to expand its reach.
A total of 722 responses were initially collected. After applying rigorous quality control procedures, several responses were excluded for the following reasons: participants were located outside the target area (n = 215), had completion rates under 15% (n = 156), lacked Institutional Review Board (IRB) consent (n = 199), did not meet the age criteria (n = 6), or had missing IP addresses (n = 2). As a result, the final analytic sample comprised 144 adult residents of Brownsville. The bilingual (English/Spanish) survey, which assessed key health domains, included validated measures where applicable and underwent a comprehensive review for cultural and linguistic appropriateness. Informed consent was obtained from all respondents before participation and the Institutional Review Board (IRB) of Texas A&M University approved the study protocol (STUDY2024-0132).
Measures
Provider-Related Healthcare Anxiety
Provider-related healthcare anxiety was measured by using the National Health Interview Survey (NHIS). 29 Participants were asked, “There are many reasons people delay getting medical care. Have you delayed getting care for any of the following reasons in the past 12 months? You were nervous about seeing a health care provider?” Response options included: 0 = Never, 1 = Sometimes, 2 = About half the time, 3 = Most of the time, and 4 = Always.
Bilingual Provider Preference
To assess bilingual provider preference, participants were asked the following question: “When considering high-quality healthcare, how important is it to you that healthcare providers are bilingual?” Responses were recorded on a 10-point Likert scale, with 1 representing “least important” and 10 representing “most important.”
Cross-Border Healthcare Access
Participants were asked, “How many times do you travel to Mexico for health or medical related reasons each year?” to measure cross-border healthcare access. Response options included: 0 = Never, 1 = 1-2 times, 2 = 3-4 times, 3 = 5-6 times, 4 = More than 6 times.
Covariates
Age (21 years or older), gender (male, female, non-binary, and other), race/ethnicity (Hispanic, Latino/a/x or Spanish origin and Other), educational levels (categorized as less than high school, some college or 2-year degree, and 4-year degree or higher), employment status (A student, employed, disabled, retired, and not employed), marital status (classified as married, partnered, never married, or divorced/separated/widowed), annual household income (reported primarily in $25,000 USD increments), current insurance coverage (yes or no), and 20 chronic conditions; (1) asthma, emphysema, or other chronic breathing problems; (2) arthritis or rheumatic disease; (3) cancer or being a cancer survivor; (4) chronic pain; (5) depression or anxiety disorders; (6) type 1 diabetes; (7) type 2 diabetes; (8) heart disease; (9) high cholesterol; (10) hypertension (high blood pressure); (11) kidney disease; (12) memory problems (e.g., dementia, Alzheimer’s disease); (13) obesity; (14) osteoporosis (low bone density); (15) obstructive sleep apnea (e.g., snoring or trouble breathing during sleep); (16) schizophrenia or other psychotic disorders; (17) stroke; (18) thyroid problems (e.g., hyperthyroidism, hypothyroidism); (19) urinary incontinence; and (20) other chronic conditions.
Statistical Analysis
To summarize the demographic and health-related characteristics of the participants, frequencies, means, and standard deviations were calculated. Associations among provider-related healthcare anxiety, bilingual provider preference, and cross-border healthcare access were estimated using an observed-variable path analysis within the using Structural Equation Modeling (SEM) framework; no latent measurement model was specified because each focal construct was measured with a single item. Within this study framework, path analysis was conducted to examine both direct and indirect effects among the variables (e.g., Provider-related healthcare anxiety, bilingual provider preference, and cross-border healthcare access), with results presented as coefficients, standard errors, and 95% confidence intervals. The indirect effects in this study were estimated using the “nlcom” package in STATA, which calculates the product of coefficients from 2 or more paths in the model, specifically the path from the independent variable to the mediator and from the mediator to the dependent variable. This approach yields an estimate of the direct and indirect effect, accompanied by the standard error (SE), z-statistic, and 95% confidence interval (CI), all of which are essential for assessing the significance of the mediation. Model fit was evaluated with several standard indices: the Root Mean Square Error of Approximation (RMSEA), where values between 0.05 and 0.10 indicate an acceptable fit, and values less than 0.05 indicate a good fit; the Standardized Root Mean Square Residual (SRMR), where values less than 0.10 suggest a good fit; and the Comparative Fit Index (CFI), with values greater than 0.90 reflecting a good fit. 30 All models adjusted for age, gender, race/ethnicity, education, employment status, marital status, current insurance coverage, and number of chronic conditions. Statistical analyses were performed using STATA version 17 (Stata Corporation, College Station, TX, USA), and statistical significance was defined as P < 0.05.
Results
Participants’ Characteristics
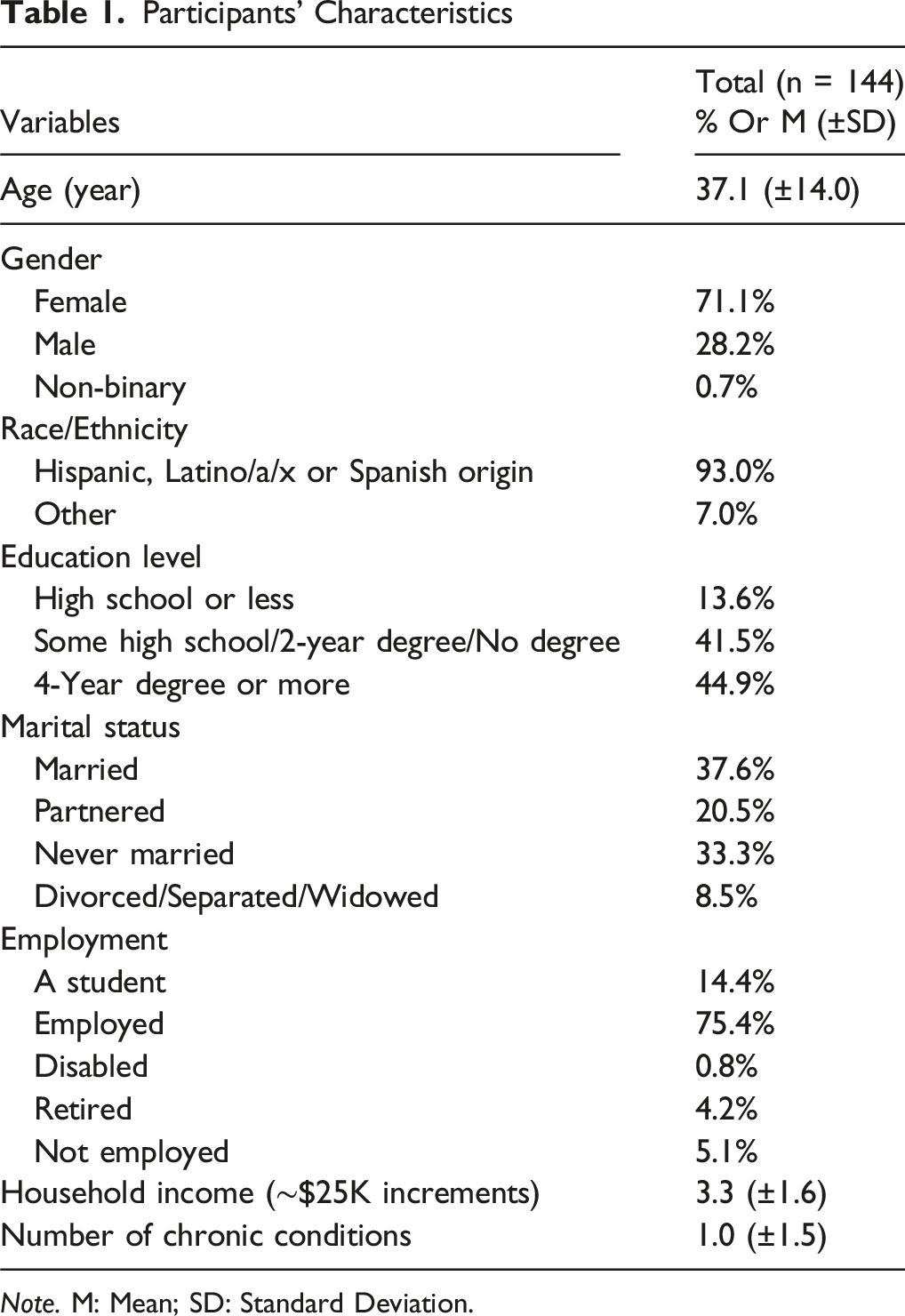
Note. M: Mean; SD: Standard Deviation.
The final tested path model with standardized coefficients and significance values was shown in Figure 2. Final tested path model with standardized coefficients and mediation; Solid arrows indicate hypothesized direct effects; the dashed arrow indicates the hypothesized indirect (mediated) effect via bilingual provider preference. All coefficients were standardized. Models were adjusted for age, gender, race/ethnicity, education, employment, marital status, insurance, and chronic conditions. *P < .05, **P < .01, **P < .001; n.s. = not significant. Model fit: Root Mean Squared Error of Approximation (RMSEA) = .014; Comparative Fit Index (CFI) = .987; Standardized Root Mean Square Residual (SRMR) = .051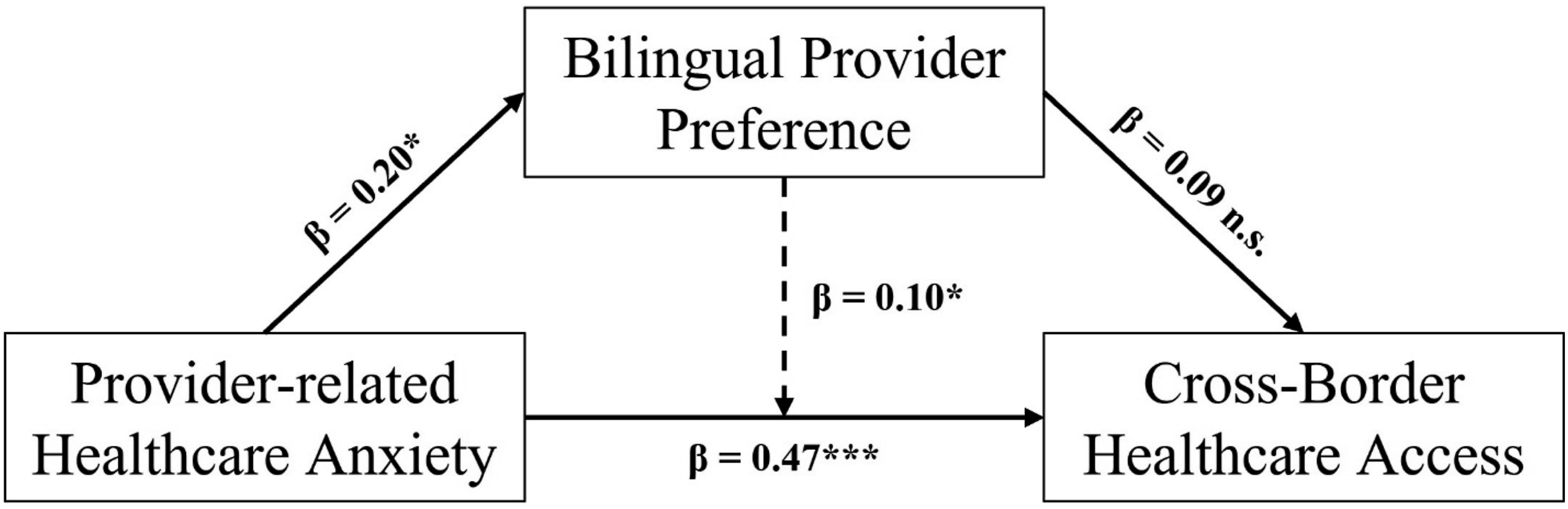
Path Analysis and Estimated Path Coefficients
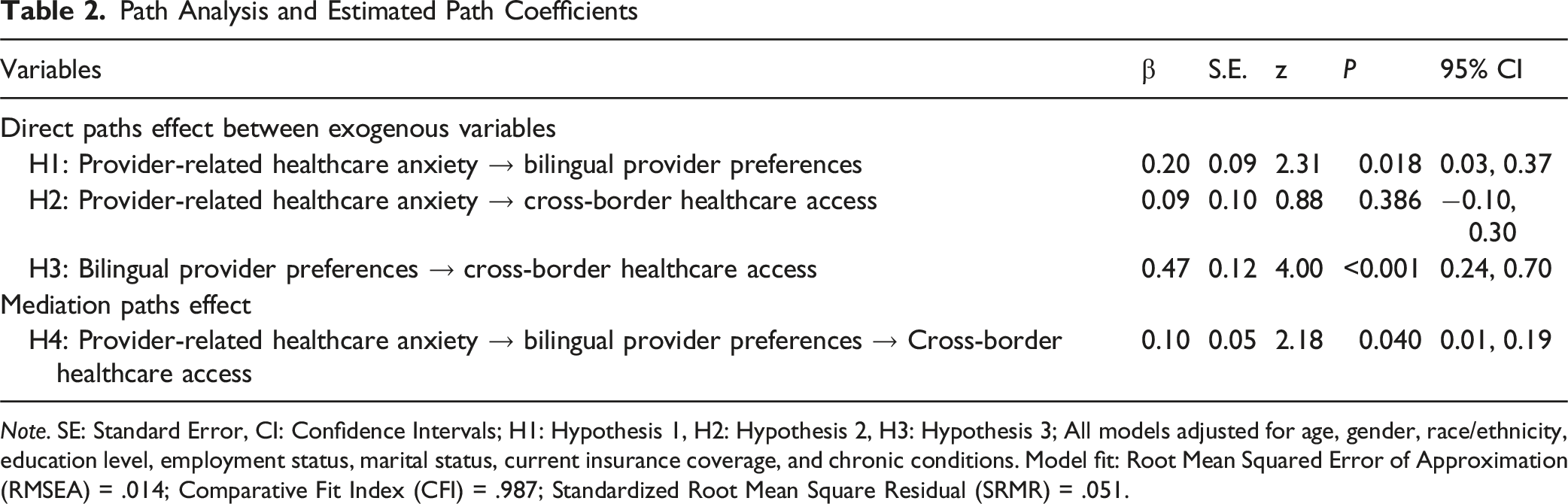
Note. SE: Standard Error, CI: Confidence Intervals; H1: Hypothesis 1, H2: Hypothesis 2, H3: Hypothesis 3; All models adjusted for age, gender, race/ethnicity, education level, employment status, marital status, current insurance coverage, and chronic conditions. Model fit: Root Mean Squared Error of Approximation (RMSEA) = .014; Comparative Fit Index (CFI) = .987; Standardized Root Mean Square Residual (SRMR) = .051.
Discussion
This study aimed to explore the relationships between provider-related healthcare anxiety, bilingual provider preferences, and cross-border healthcare access in U.S.-Mexico border communities. The key findings revealed a significant positive relationship between provider-related healthcare anxiety and bilingual provider preferences. Additionally, bilingual provider preferences were strongly associated with cross-border healthcare access, and a mediation effect was observed where bilingual provider preferences mediated the relationship between healthcare anxiety and cross-border healthcare access. However, the direct effect of provider-related healthcare anxiety on cross-border healthcare access was found to be non-significant.
The path analysis revealed a significant positive relationship between provider-related healthcare anxiety and bilingual provider preferences. This finding is consistent with a previous study indicating that individuals who experience healthcare anxiety, especially in linguistically discordant settings, may seek providers who share their language proficiency to alleviate the discomfort associated with language barriers. 25 The relationship is supported by literature suggesting that language barriers often increase provider-related anxiety, especially in immigrant populations with limited English proficiency.16,19 Our study suggested that bilingual providers can serve as a buffer, reducing the psychological burden of healthcare encounters, as individuals perceive them to be more understanding and accessible. Psychologically, provider-related healthcare anxiety stems from fears or discomfort with medical encounters, exacerbated by language barriers. Previous studies have highlighted that anxiety can stem from concerns about misunderstanding medical information, miscommunication, or negative judgments by healthcare professionals.18,21 Spanish-speaking individuals often report difficulties in healthcare interactions due to language mismatches, 21 therefore, the anxiety experienced may compel individuals to prioritize bilingual providers, whose linguistic skills are perceived as essential for clear and effective communication. These findings suggest that bilingualism in healthcare providers may play a crucial role in reducing anxiety and fostering trust, which are vital for positive healthcare outcomes.
Our findings determined that there is a strong and statistically significant relationship between an individual’s preference for a bilingual medical provider and seeking healthcare services in Mexico. This finding suggests that language preference is a primary driver of decisions to cross the border for medical care and supports previous research, which demonstrates the importance of language and cultural context in the health-seeking decisions of Latinos.31,32 Preference for a bilingual provider may indicate a preference for a shared cultural context between the patient and the provider that could make it easier for the patient to both navigate the healthcare system and understand the care instructions provided by their provider. Previous literatures have also suggested that individuals in border communities often seek care in Mexico due to both cultural and linguistic familiarity, as well as affordability.33,34 Bilingual providers are not only trusted for their language skills but also for their cultural competence, which is seen as an essential factor in healthcare satisfaction and utilization. 27 This finding also expands the understanding of health-seeking behavior among border community residents by emphasizing the importance of language as a driver for health-seeking behavior, separate from health insurance coverage. While previous studies have identified health insurance coverage as a primary motivator for border community residents to seek care in Mexico, particularly given the high prevalence of underinsurance or lack of insurance in the U.S.,35-37 our study suggests that language preference serves as a distinct and unique driver of this behavior. Since individuals in bilingual communities, such as those along the U.S.-Mexico border, often prioritize language concordance in healthcare interactions to promote trust and enhance the patient experience, 18 our findings highlight the pivotal and independent role of bilingual provider preferences in shaping health-seeking behavior, even though insurance coverage remains an important factor in cross-border healthcare utilization. Also, beyond language-concordant communication, preferences for bilingual providers may also reflect deeper cultural and social dimensions, including perceived trustworthiness, shared cultural norms, and protection from discrimination. Patients may associate language concordance with feeling respected, understood, and less stigmatized within healthcare settings. Future studies should explicitly examine how constructs such as medical mistrust, perceived discrimination, and cultural identity intersect with bilingualism to shape healthcare-seeking behaviors in border communities.
Additionally, our analysis indicated a significant mediation effect, where bilingual provider preferences act as an intermediary between provider-related healthcare anxiety and the decision to seek care in Mexico. This suggests that individuals do not seek cross-border healthcare solely due to anxiety about healthcare interactions; instead, their preference for a bilingual provider appears to be a key factor in mitigating these anxieties. These findings build on the findings from previous research that advocate for increased linguistic and cultural awareness and sensitivity in healthcare settings and health-related communications. 38 Also, this finding is consistent with previous studies that have demonstrated that a lack of cultural competency and the inability to accommodate the linguistic needs of patients can contribute to feelings of fear and reluctance in seeking medical care.39,40 Therefore, for individuals experiencing anxiety due to language barriers or unfamiliarity with healthcare systems, the availability of bilingual providers can offer a sense of reassurance and trust, making the healthcare experience less daunting. By investing in bilingual healthcare services, institutions could not only increase patient confidence but also potentially mitigate healthcare-related anxiety. These investments may result in greater healthcare access for non-English-speaking or limited English-speaking residents of border communities, thus improving the overall utilization of healthcare services and reducing reliance on cross-border healthcare as well as addressing healthcare disparities in border regions.
These findings point to several actionable implications for practice and policy. Healthcare systems serving border communities should prioritize the recruitment, retention, and training of bilingual and bicultural providers, as well as the expansion of high-quality interpreters and patient-navigation services. Local policymakers and binational partners could invest in cross-border referral networks, shared care protocols, and workforce-development initiatives that increase the availability of language-concordant care on both sides of the border. By centering language and cultural concordance in health system planning, stakeholders may reduce provider-related healthcare anxiety and narrow disparities in access to care for Latino residents of border regions.
This study has several strengths and limitations. One of the key strengths is that our study’s findings provided valuable insights to examine the mediating role of bilingual provider preferences in the relationship between provider-related healthcare anxiety and cross-border healthcare access, offering a unique perspective on cross-border healthcare behavior. Additionally, the study advances literature by considering not only direct relationships but also the indirect paths that mediate healthcare decisions, thereby providing a more comprehensive understanding of healthcare access in border communities. This study had a great model fit, suggesting that the study’s model effectively captured the relationships between the variables and that the findings reflect real-world phenomena. However, there are limitations to consider. First, the analytic sample was relatively small (n = 144) and recruited from a single U.S.-Mexico border city (Brownsville, Texas). As such, these findings may not generalize to other border communities or Latino populations living in non-border settings. Future multi-site studies with larger and more diverse samples across multiple border regions and interior U.S. communities are needed to more fully assess the external validity of the observed pathways. Second, the cross-sectional design precludes establishing temporal ordering among provider-related healthcare anxiety, bilingual provider preferences, and cross-border healthcare access; therefore, the mediation pathways identified in this study should not be interpreted as causal. Longitudinal and experimental designs are needed to clarify whether changes in provider-related anxiety or access to language-concordant care led to subsequent changes in cross-border healthcare utilization. Third, all focal constructs were assessed with single survey items, which may not capture the full complexity or reliability of provider-related healthcare anxiety, bilingual provider preferences, or cross-border healthcare access. In addition, we did not assess several potentially important determinants of cross-border care, such as prior healthcare experiences, immigration and documentation status, or detailed insurance characteristics (e.g., underinsurance, deductibles), which may further explain variability in cross-border healthcare use. Future research should incorporate validated multi-item scales and a broader set of structural and psychosocial variables to provide richer explanatory power.
Conclusion
In conclusion, this study highlights the pivotal role of bilingual provider preferences in shaping healthcare-seeking behavior within U.S.-Mexico border communities. In other words, it is evident a significant mediation effect, with bilingual provider preferences serving as an intermediary between provider-related healthcare anxiety and the decision to seek care in Mexico. While health insurance coverage continues to be a key determinant of cross-border healthcare utilization, our results demonstrate that language preference stands as an independent and crucial driver of healthcare decisions. The psychological burdens associated with language barriers and cultural differences can be mitigated by bilingual providers, who significantly reduce anxiety and enhance the healthcare experience, thereby encouraging patients to seek care within their communities. Continued investment in bilingual healthcare services within border regions has the potential to decrease reliance on cross-border healthcare and address healthcare disparities. As such, healthcare institutions in these areas should prioritize bilingualism and cultural competence to improve patient care, increase satisfaction, and enhance overall health outcomes in these underserved populations.
Footnotes
Ethical Considerations
This study was approved by the Institutional Review Board of Texas A&M University approved the study protocol (STUDY2024-0132).
Consent for Publication
Informed consent was obtained from all respondents before participation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.