
Abstract
Purpose
To examine associations between preschooler screen time trajectories and physical activity outcomes at age 5.5.
Design
A longitudinal cohort study of Canadian parents with preschoolers.
Setting
Data were collected in Nova Scotia, Canada, during the COVID-19 pandemic in Spring/Summer 2020 and 2021, and Summer/Fall 2022.
Sample
A community-based convenience sample of 315 parents of preschool-aged children (54% boys) was followed longitudinally when children were 3.5 (2020), 4.5 (2021), and 5.5 years old (2022).
Methods
Parent-reported screen time at 3.5, 4.5, and 5.5 years was used to estimate preschooler screen time trajectories. Using growth mixture modeling (GMM), three groups were identified: low (mean = 0.89 h/day, 23%), average (mean = 2.96 h/day, 56%), and high (mean = 6.42 h/day, 21%) screen time trajectory groups. At age 5.5, physical activity was directly assessed using accelerometers to capture light, moderate, and vigorous-intensity physical activity. Parents also reported child sex, family configuration, and educational attainment.
Results
Children in the high screen time trajectory group engaged in significantly less light-intensity physical activity (b = −29.98, P < .05) compared to children in the average screen time trajectory. No significant differences were observed between the low and average screen time trajectory groups for light-intensity physical activity. Additionally, no significant differences in moderate or vigorous-intensity physical activity were observed between the screen time trajectory groups.
Conclusions
Higher screen time in preschoolers is associated with reduced engagement in light-intensity physical activity. These findings highlight the importance of monitoring screen time to ensure that children have opportunities to engage in light-intensity physical activities such as active and outdoor play. Limiting early childhood screen time may support healthier physical activity patterns and promote early childhood development.
Purpose
Early childhood is a sensitive time for the development of habits towards physically active and sedentary behavior. 1 This has led to growing concerns over how preschool-aged children spend their free time. 2 The amount of time young children have been spending on screen-based devices, including televisions, smartphones, and tablets, has increased.3,4 Before the COVID-19 pandemic, the average screen time of Canadian preschoolers was 1.9 h per day. 5 According to a meta-analysis, screen time increased by 66 min per day among preschoolers during the pandemic. 6 Furthermore, a recent review found that only 35.6% of children aged 2 to 5 meet the World Health Organization’s recommendation to limit screen time to 1 h per day or less.7,8
Excessive screen time may lead to a deficit in opportunities for more enriching activities that contribute to a child’s overall development in physical, cognitive, and social areas. 9 In particular, spending too much time with screens during the preschool years has been linked to worse child locomotor, object control, and stability skills.10,11 According to one prospective study, screen use in preschool children also predicted worse fine motor skills 1 year later. 12
Engaging in physical activity in early childhood provides a wealth of benefits for physical health, including cardiometabolic health, fitness, and bone health as well as opportunities for social, cognitive and motor development.13,14 Even light-intensity physical activity can foster developmental benefits 15 and has been identified as an independent predictor of all-cause mortality. 16 Furthermore, physical activity during this period can support development by providing children with opportunities to practice important social and motor skills. 17 In contrast, child sedentary behavior is a recognized risk factor for obesity and a variety of chronic diseases, including hypertension, cardiovascular diseases, and diabetes. 18 Additionally, 37 million children under the age of 5 worldwide are affected by overweight or obesity, 19 and only 30% meet the WHO guidelines recommending at least 1 h of moderate to vigorous-intensity physical activity daily.5,7
Screen time can displace the time allocated for physical activity, 20 as reducing screen time has been shown to increase physical activity levels in children.21,22 Additionally, a significant negative association was observed between TV hours and physical activity levels in children aged 3 to 4 years. 23 However, other studies have reported no significant relationship between screen time and physical activity, suggesting that the impact of screen time on physical activity may vary across different contexts and developmental stages.11,24,25
Previous research has used cross-sectional designs to examine associations between early childhood screen time and physical activity.26,27 As such this approach can obscure how screen use habits over an extended period of early childhood prospectively contributes to physical activity habits. Additionally, few studies have used accelerometer devices to objectively track physical activity in preschoolers.
Child screen time and physical activity are also linked to various individual and family characteristics including child sex, parent education, and family configuration.9,28-30 As such, it remains important to consider these characteristics as control variables. The objective of the present study is to estimate how preschooler screen time trajectories between the ages of 3 and 5 contribute to engagement in physical activity at age 5. Our hypothesis is that higher levels of screen time across the ages of 3 and 5 would be associated with less light, moderate and vigorous-intensity physical activity, controlling for child sex, family configuration, and parent education.
Methods
Data Collection
Child screen time was collected during the COVID-19 pandemic, specifically in the Spring/Summer of 2020 and 2021 (Waves 1 and 2), and in the Summer/Fall of 2022 (Wave 3). To assess child screen use, we remotely administered the Media Assessment Questionnaire (MAQ), 31 which was completed by parents. The MAQ, which has demonstrated predictive and discriminant validity in previous studies,31-33 also includes questions about the child’s sex, family configuration, and parent education. Child physical activity data were collected at Wave 3 using an accelerometer worn by the child. All study measures are described below.
Our analysis plan was not pre-registered. However, the current research hypotheses were initially formulated for a Canadian Institutes of Health Research grant awarded in 2022 (application #474993). The research protocol was approved by the internal review board at Université Sainte-Anne (#0090.d) and Université de Sherbrooke (2021-2927). Written informed consent to participate was obtained from the parents. Parents were compensated with a CAD $50 gift card for each of the first two data collection waves and with the amount of CAD $300 for the third wave, which involved a home visit, the child wearing the accelerometer device, and completing questionnaires.
Sample
Parents were recruited in Nova Scotia, Canada, through posters and flyers distributed in family clinics, preschools, and kindergartens, as well as through newspapers, radio advertisements, and a Facebook page. A total of 315 children in the present study were followed longitudinally at ages 3.5, 4.5, and 5.5. Mothers were the primary respondents (93.4%). The average age of the responding parents was 34.9 years (SD = 4.38, range: 22-52), and they were primarily married (82.0%), born in Canada (91.0%), and self-identified as White (90.5%). Our sample included a slightly higher number of boys (54.0%) than girls.
Procedure
Trained research assistants provided parents with an ActiGraph wGT3X-BT accelerometer and instructions on how to use the device with their child during a home visit that took place between May 2022 and March 2023. The accelerometer was worn around the child’s waist at hip level to capture body movement, physical activity, and sleep. Children were asked to wear the device for 1 week, 24 h a day, except during bathing and water-based activities. Data were collected at a sampling rate of 30 Hz. Parents were provided with a prepaid envelope to return the device.
Measures
Screen time
Parents reported child screen time separately for weekdays and weekend days for each of the following activities when the child was 3.5, 4.5, and 5.5 years old 1 : Watching TV or DVDs 2 ; Using a computer 3 ; Playing video games on a console; 4 ; Using an iPad, tablet, LeapPad, iTouch, or similar mobile device (excluding smartphones); or 5 Using a smartphone. Response options included 1 : Never 2 ; Less than 30 min 3 ; 30 min to 1 h 4 ;1–2 h 5 ;2–3 h 6 ; 4–5 h 7 ; more than 5 h. We then converted these categorical responses into variables reflecting the number of hours spent with each type of media device. Our approach involved using the midpoint for each response range, apart from “Never” where a score of 0 was used, and “5 or more hours a day” where a more conservative score of 5 was used. Weighted daily averages of time spent with each type of media device were then created by multiplying weekday estimates by 5 and weekend day estimates by 2 and dividing the total by 7. An overall daily screen time estimate was calculated by summing the weighted daily average across media devices.
Physical Activity
Child hysical activity was measured objectively at the third assessment when the child was 5.5 years old using an accelerometer device. The data were processed using ActiLife software (ActiGraph), with a 10-s epoch length. The average steps and vector magnitude counts per minute (CPM) were calculated based on total wear time. Activity intensity was categorized using published cut points for preschoolers 34 as follows: light-intensity physical activity (820 to 3907 cpm), moderate-intensity (3908 to 6111 cpm), and vigorous-intensity (6112 and above cpm).
Control Variables
Parents reported child sex (coded as 0 = boy or 1 = girl), family configuration (coded as 0 = unmarried or 1 = married), and their educational attainment (coded as 0 = high school or college or 1 = undergraduate or graduate degree).
Data Analysis
We used growth mixture modeling (GMM) to estimate trajectories of screen time among preschoolers. GMM is increasingly valued for its ability to uncover unobserved subgroups based on individual growth patterns. We first estimated the unconditional mean trajectory for the entire sample to assess significant variances in the mean intercept and slope. Then, we fitted GMMs with varying intercepts, slopes, and variances, exploring solutions ranging from 1 to 6 groups to capture distinct patterns of screen time. Our choice of the optimal solution was based on several fit indices proposed in the literature. 35 After establishing the best-fitting screen time trajectories, we estimated separate linear regression models to examine the contribution of these trajectories to physical activity at age 5.5. To better isolate the unique contribution of screen time to child physical activity outcomes, we controlled for child baseline sex, family configuration, and parent education at age 3.5. All models were weighted according to the classification probabilities derived from the GMM and were run using Mplus software version 8.10.
Missing Data
At the third wave, data were missing for 33 participants for several reasons: some participants did not consent to accelerometry, refused to wear the device, did not wear it for the full duration. Some participants refused participation in the accelerometer portion of our study and one accelerometer was lost in the mail. As a result, 62.2% of the 315 participants had missing data on one of the observed outcome variables. To assess whether the missing data were completely random (MCAR), Little’s test was performed. The test was non-significant (χ2 = 0.155, DF = 1, P = .694), suggesting that the missing data could be considered MCAR. Therefore, general linear models using full-information maximum likelihood estimation (FIML) and GMM were employed to handle the missing data in subsequent analyses. 36
Results
Descriptive Statistics
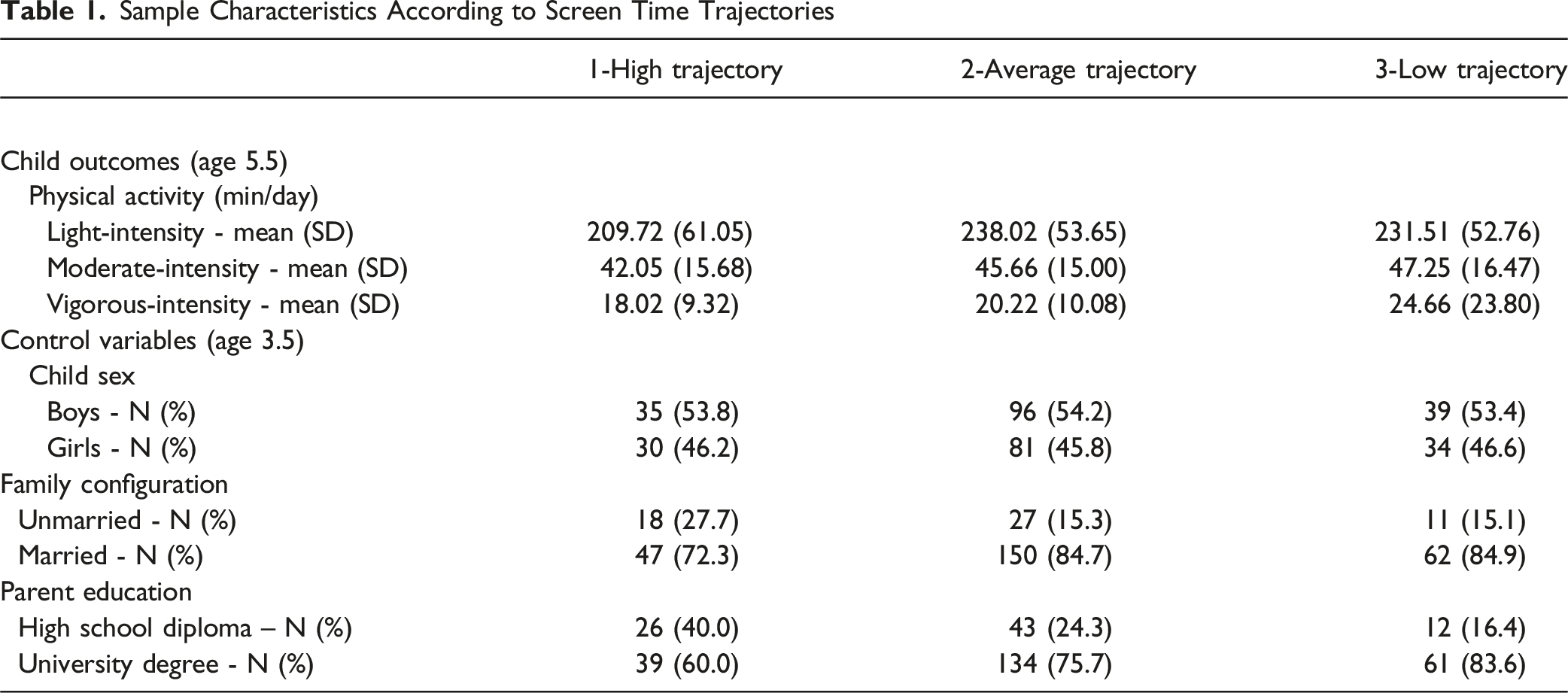
Sample Characteristics According to Screen Time Trajectories
Attrition Analyses
An attrition rate of 15.9% was observed across the first two assessments, with 315 children providing complete data on screen time at age 3.5 (T1) and 265 children at age 4.5 (T2). The attrition rate increased to 21.1% by the final wave, with 209 children having complete data at age 5.5 (T3). To compare participants with complete data to those with missing data, we conducted an attrition analysis. Participants with complete data did not differ from those with missing data on screen time trajectories (P = .208). Additionally, missing data was not related to child sex (r = .09, P = .112), screen time exposure at T1 (r = −.01, P = .817), family configuration (r = −.03, P = .561, or parents’ education status (r = .07, P = .191).
Estimation of Screen Time Trajectories
To address extreme values, all measures of screen time were winsorized at the 2nd and 98th percentiles prior to modeling the trajectories. Using GMM, we identified three screen time trajectories: low (23.2% of the sample, 3-year mean = 0.89 h/day), medium (56.2% of the sample, 3-year mean = 2.96 h/day), and high (20.6% of the sample, 3-year mean = 6.42 h/day). These trajectories are shown in Figure 1. A 3-class model was selected because it had a significant Vuong-Lo-Mendell-Rubin likelihood ratio test P-value, a lower BIC value compared to the 2- or 4-class solutions and provided group sizes of at least 5% of the sample. This decision was based on previously established criteria.
37
Additionally, all physical activity measures were winsorized at the 2nd and 98th percentiles due to the substantial asymmetry observed in the data. A more robust estimator was applied to account for this asymmetry. Trajectories of Preschooler Screen Time Between 3.5 and 5.5 Estimated Using GMM. Note. The y-Axis Indicates Average Hours of Daily Screen Time. The X-Axis Indicates Child Age Between 3.5 and 5.5 years of Age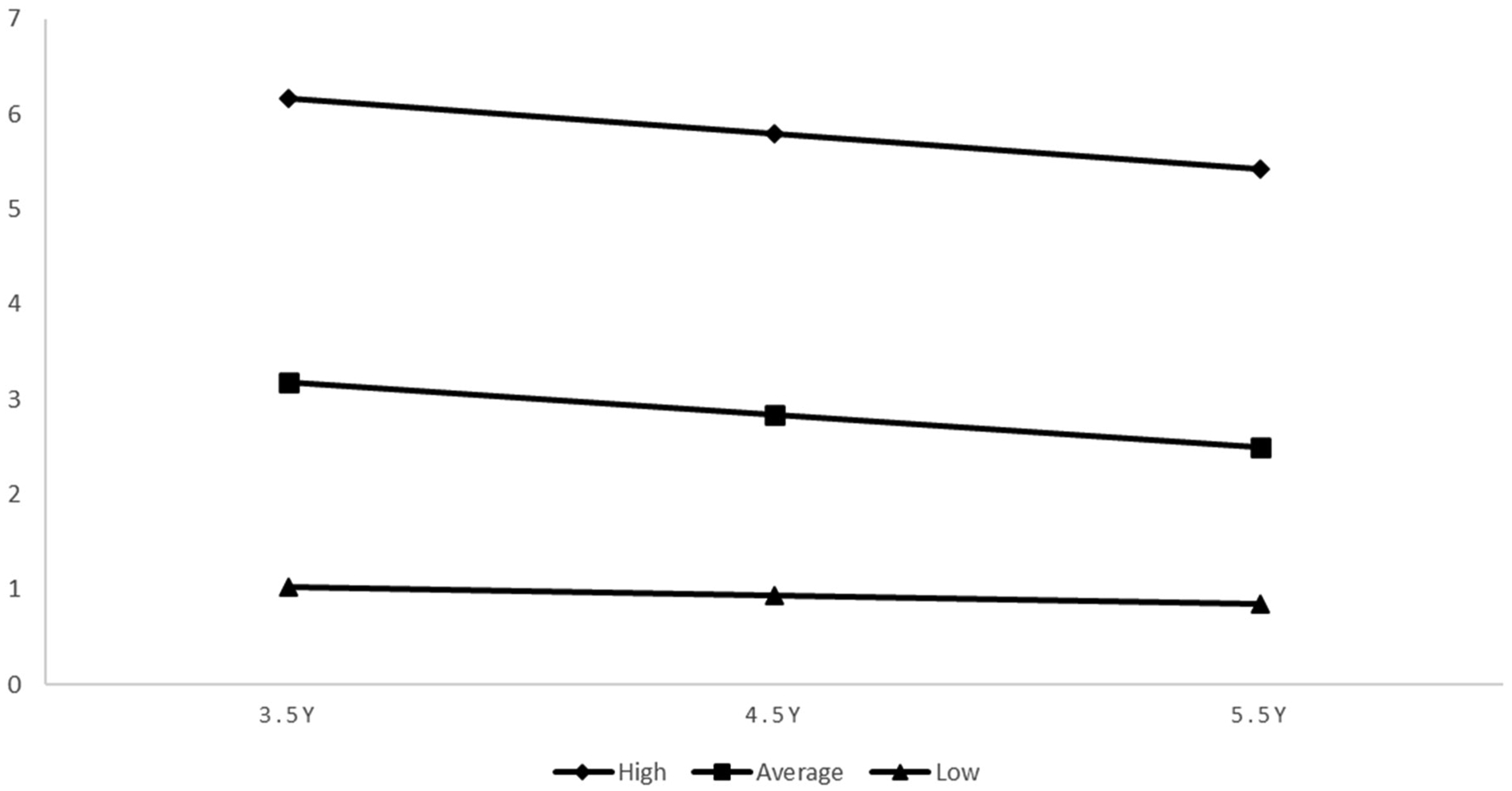
Associations Between Screen Time Trajectories and Physical Activity
Linear Regression Models Estimating Associations Between Child Screen Time Trajectories and Physical Activity at Age 5.5
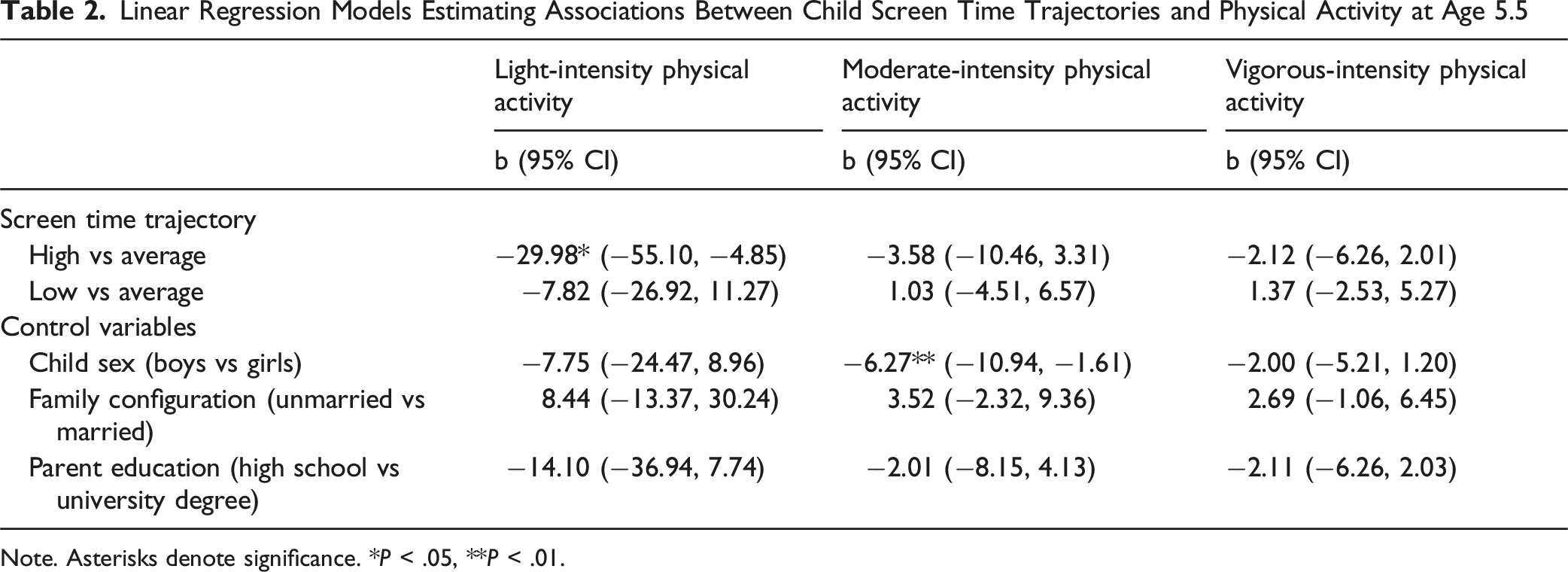
Note. Asterisks denote significance. *P < .05, **P < .01.
Discussion
To our knowledge, our study is the first to examine associations between preschool-aged children’s screen time trajectories and objective measures of their physical activity at different intensities during the COVID-19 pandemic. Our findings indicate that a significant portion of the sample did not adhere to the recommendation of 1 hour or less of daily screen time, with 56% of preschoolers averaging 3 h of daily screen time and 21% averaging 6 h per day during the pandemic. Only, 23% of preschoolers met the recommendation, which aligns with recent findings from urban Spanish children, indicating similarly elevated screen time levels among preschoolers. 38 Our analysis also revealed that preschoolers’ screen use habits remained relatively stable from 3.5 to 5.5 years old. In partial support of our hypothesis, children who were in the high screen time trajectory group engaged in less light-intensity physical activity compared to the average and low screen time groups by age 5.5, which aligns with previous research from Singapore indicating that higher screen time among preschoolers is associated with lower levels of light and moderate to vigorous-intensity physical activity. 39 Contrary to expectations, no significant difference was observed between the low and average screen time trajectories for light-intensity physical activity, and no associations were found between all screen time trajectories and moderate or vigorous physical activity.
Children in the high screen time trajectory group may have experienced a significant decrease in light-intensity physical because their high intake of screen time could have displaced opportunities for engagement in activities that demand intense levels of physical activity. There are several possible explanations for our observed pattern of findings. First, preschoolers spend a significant portion of their time engaged in light-intensity physical activity during active play. 7 Similarly, children are likely to engage in light physical activity when spending time outdoors. Both outdoor time and active play may therefore be reduced in children who accumulate a lot of time in front of screens.40-43 As such, future research could explore which light-intensity physical activities are being displaced by excessive screen time. These may include outdoor time, active and imaginary play alone, with parents or with other children, and walking to daycare or school. 41
In contrast, moderate or vigorous-intensity physical activities, frequently occur in the context organized sports (eg, being part of a soccer team). The scheduled nature and associated costs of these activities could make them less susceptible to replacement by screen time. In line with this, our findings revealed that preschoolers spent significantly more time in light-intensity physical activity (around 209-238 min per day) compared to moderate (42-47 min) and vigorous-intensity activity (18-25 min) across the different screen time trajectory groups. This is consistent with other studies, which have shown that preschoolers typically engage in low levels of moderate to vigorous-intensity physical activity, while spending a larger portion of their time in sedentary and light-intensity activities.15,44
Early childhood involvement in light-intensity physical activity plays a crucial role in reducing sedentary behavior and makes a significant and complimentary contribution to health and wellbeing beyond involvement in moderate to vigorous-intensity physical activity. 45 Indeed, to promote a non-sedentary lifestyle, the WHO recognizes the importance of including light-intensity physical activity in healthy lifestyle habits. 15 However, current guidelines do not yet provide specific recommendations for this type of activity in early childhood. 46
The present study is not without limitations. First, our findings are based on a low-risk, community-based convenience sample, which may not be generalizable to other Canadian preschoolers. The use of parent-reported measures of screen time is also a limitation, which could have been influenced by social desirability and recall biases. Furthermore, baseline data on child physical activity were not available in the present study, which prevents us from establishing the direction of association between preschooler screen time and physical activity. As another limitation, accelerometers may not accurately measure certain activities, such as biking, especially during isometric efforts, which could lead to an underestimation of some types of physical activities. 47 Finally, it is important to note that data collection occurred during the COVID-19 pandemic, which affected preschooler’s screen time and physical activity due to changes in daily routines. 48
In terms of strengths, the present study was able to track child screen use habits across 3 years. In addition, our findings are strengthened by the use of objective, independent assessments of physical activity via accelerometers, which helps reduce the probability of shared measurement error. The inclusion of measures of multiple intensities of physical activity (light, moderate, vigorous) is also a strength of this study. To date, most studies have focus exclusively on moderate to vigorous-intensity.
Our results align with previous research highlighting the importance of parental monitoring of child screen time and physical activity during the preschool-aged years. A cross-sectional study found that preschoolers in settings where screen time was supervised exhibited higher levels of physical activity and spent less time being sedentary, compared to those with more unrestricted access to screens. 20 Fostering health-promoting habits starting in early childhood is particularly important, given that lifestyle habits adopted at a young age are more likely to be sustained over time.49,50 From a public health perspective, childhood sedentary behavior continues to represent a significant and costly burden for individual and society.51,52 Consequently, education and health campaigns should continue to sensitize parents about the potential health consequences of early childhood excessive screen time. One strategy could be to encourage parents to adopt screen use and physical activity plans, 53 including setting clear limits and scheduled active breaks, to help them establish healthy routines. Such efforts may not only support immediate health and development in early childhood but also contribute to reducing the risk of adverse health outcomes later in life.
In addition, prevention efforts should aim to sensitize parents and early childhood professionals, particularly those working in childcare settings, to the importance of ensuring consistent messages and opportunities in children’s home and daycare environments. Our findings further highlight that health promotion initiatives should explicitly incorporate guidance on light-intensity physical activity, alongside moderate to vigorous-intensity physical activity, to more effectively counteract the sedentary effects of excessive screen time in early childhood. From a population health perspective, interventions in early childhood can have exponential long-term returns, especially when integrated into family, childcare, and policy-level strategies.
Conclusion
Excessive screen time in early childhood is related to both physical and mental health risks.
54
Currently, only 15% of Canadian preschoolers aged 3 to 4 years meet the Canadian Sedentary Behaviour Guidelines for the Early Years.
55
Our results indicate that higher levels of screen time in preschoolers are associated with less light-intensity physical activity, specifically and help document the potential health burden associated with excessive screen time in early childhood. Early childhood screen time is a growing concern among parents and professionals. Excessive screen use has been linked to poorer motor development and reduced opportunities for physical activity. However, limited research has examined associations between child screen time across the ages of 3 and 5 and objectively measured physical activity by age 5. Our study suggests that higher levels of screen time between the ages of 3 and 5 are associated with less light-intensity physical activity at age 5. Our longitudinal approach and use of accelerometer devices to measure child physical activity strengthen the present results. Findings underscore the importance of reducing screen time among preschoolers to promote light-intensity physical activity. Health promotion should encourage parental monitoring of child screen use to support healthy habits with lasting benefits.So what? (Implications for Health Promotion Practitioners and Researchers)
What is already known on this topic?
What does this article add?
What are the implications for health promotion practice or research?
Footnotes
Acknowledgments
We would like to acknowledge the work of Rachelle Wakeham Lewis and Samantha Bédard for their assistance in the data collection and all the participating families for their time. The authors also acknowledge the contribution of Annie Lemieux, M.Sc., statistician, in the validation of the analyses.
Ethical Consideration
The studies involving humans were approved by the Université Sainte-Anne Comité d’Éthique. The studies were conducted in accordance with the local legislation and institutional requirements.
Consent to Participate
Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author Contributions
RS: Conceptualization, Writing – original draft. DL-M: Methodology. DB: Writing – review & editing. FB: Writing – review & editing. JL: Writing – review & editing. CF: Conceptualization, Data curation, Funding acquisition, Project administration, Writing – review & editing, Formal analysis, Supervision.
Funding
The authors declare that financial support was received for the research, authorship, and/or publication of this article. All phases of the study were funded by grants from the Canadian Institutes of Health Research (474993-2022), the Social Sciences and Humanities Research Council (CRC-2021-00009), and Research Nova Scotia (2061-2019). The authors also acknowledge funding from the Canada Research Chair’s program from the Social Sciences and Humanities Research Council and the financial support from the Social Sciences and Humanities Research Council of Canada under the Canada Graduate Scholarships Doctoral program under grant 767-2025-2377.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data for the present study are not readily available. As per the participant consent form, data are only available to the research team. Any requests for the raw data should be addressed to the corresponding author.