
Abstract
Purpose
Patient satisfaction is a key principle of high-quality care, important to all health systems. While evidenced-based guidelines recommend tobacco use counseling to all hospitalized patients who use tobacco, scant knowledge exists about patient satisfaction with these services. The Satisfaction with Inpatient Tobacco Treatment Study (1) proposes a novel survey tool to measure patient satisfaction with inpatient tobacco treatment and (2) provides survey results from our hospital’s Tobacco Treatment Program.
Design
Creation and administration of an 8-item Likert scale survey to assess inpatient tobacco use counseling.
Setting/Subjects
A random sample of inpatients who received remote inpatient tobacco use treatment at UNC Health’s Tobacco Treatment Program were selected for participation. The survey was administered by telephone and email.
Measures
Survey items assessed constructs of patient satisfaction, resource availability pre- and post-discharge, the perceived benefits of inpatient tobacco treatment counseling, and patient-reported smoking cessation.
Analysis
Survey responses were analyzed using descriptive statistics and Fisher’s Exact Tests.
Results
The majority of respondents reported satisfaction with tobacco use counseling. 92% strongly agreed or agreed that the consultations improved their overall hospital experience and 90% said they quit or cut down on their tobacco use after discharge. Results did not vary significantly by race, insurance status, or gender.
Conclusion
Patient satisfaction with inpatient tobacco cessation treatment was high across multiple domains, as was patient-reported smoking cessation. The survey instrument can be further validated and adapted for program assessment and quality improvement in other tobacco treatment programs.
Keywords
Purpose
Tobacco use continues to be the leading preventable cause of death and disease in the United States. 1 Effective tobacco treatment should be an integral part of the healthcare system, for the purposes of improving patient quality of life and lowering healthcare costs. 1 Since tobacco use causes and worsens illnesses that lead to hospitalization, inpatient status provides a unique opportunity to introduce smoking cessation interventions. 2
In 2012, the Joint Commission released tobacco treatment guidelines, recommending that hospitals screen for tobacco use during hospitalization and provide both cessation counseling and nicotine replacement therapy (NRT) to inpatients who smoke. 3 Prior studies have shown inpatient smoking cessation treatment to be effective in reducing short-term and long-term tobacco use.4,5
Because of their ability to successfully treat tobacco dependence, inpatient tobacco treatment programs should be scaled up and evaluated across multiple dimensions, including both patient and provider satisfaction. Patient satisfaction is a key principle of high-quality care, important to all health systems. 6 Patient-reported satisfaction is a crucial metric that allows healthcare providers to incorporate patient perspectives and preferences in quality improvement. 7 Despite this, patient satisfaction with inpatient smoking cessation is rarely explored, 8 particularly the degree of satisfaction with inpatient tobacco treatment conducted via telehealth. 9 To fill this knowledge gap, we designed a pilot survey to assess the degree of satisfaction of inpatients with remote tobacco treatment services.
Methods
Design
The study team designed a brief survey to retrospectively measure patient satisfaction with tobacco use counseling. We hypothesized that inpatients who use tobacco and received an inpatient consult would report high degrees of satisfaction, defined as 80% or higher who agree or strongly agree to each construct. 10 This is in part because of the opportunity to discuss their tobacco use behaviors and any linkages to their inpatient admission with a trained counselor. Counselors also helped inpatients avoid withdrawal symptoms while hospitalized by offering NRT.
Measures
To our knowledge, no validated patient satisfaction questionnaire exists for inpatient tobacco use treatment. Therefore, we attempted to devise a brief inpatient satisfaction survey that would offer descriptive responses from patients who had previously received treatment by an inpatient tobacco treatment counselor. Given concerns about the lack of available incentives for survey completion, we chose to keep the survey brief to attempt to maximize response rate. We initially examined relevant content from 2 validated patient satisfaction surveys, the PSQ-18 and the Satisfaction With Therapy and Therapist Scale--Revised (STTS-R).11,12 We attempted to use questions, if available, that were used in both the PSQ-18 and STTS-R and that appeared to have the highest face validity when applied to tobacco use treatment. For instance, the STTS-R states “I am now able to deal more effectively with my problems.” We translated this to the context of tobacco treatment to “I felt more prepared to reduce tobacco use after speaking with the tobacco treatment counselor than I did before speaking with the counselor.” Since some of the constructs we were most interested were specific to resources and interactions with tobacco treatment, and since these constructs are not captured by the PSQ-18 or STTS-R, we added several questions addressing resource availability, care, and respect regarding nicotine withdrawal. These constructs are aligned with core domains of hospital patient satisfaction surveys. 13
Our final survey included 8 items assessing constructs related to patient satisfaction, resource availability pre- and post-discharge, and the perceived benefits of inpatient tobacco treatment counseling. Participants were asked to read each statement and provide their level of agreement using a 4-point Likert scale (“Strongly Agree,” “Agree,” “Disagree,” and “Strongly Disagree”). Two additional items assessed patient-reported tobacco use post-discharge. We treated each satisfaction item as a distinct construct to capture specific elements of patient experience and care, rather than assuming one-dimensionality across items. Survey questions are provided in the Supplemental Digital Content.
Sample
UNC Health is the academic health system at the University of North Carolina-Chapel Hill. The UNC Tobacco Treatment Program (TTP) began in 2008. Cessation services have been offered to inpatients at the 1,000-bed UNC Medical Center since 2010 and at the 83-bed UNC Hillsborough Hospital since 2019, the sites of this tool implementation. Former inpatients who had received inpatient tobacco use treatment during their hospitalization were randomly selected using the Excel RandBetween and Sort functions applied to a list of patients who received inpatient tobacco use treatment services in the 3 months preceding survey administration. Each patient was sorted by their randomly generated number and patients with the lowest 239 random numbers were selected for study participation.
The treatment intervention consisted of motivational interviewing and cognitive behavior therapy, usually lasting between 5 and 10 min, to assess patients' readiness-to-quit and help them develop strategies to remain tobacco-free post-discharge. This treatment is provided remotely via telephone. Nicotine replacement therapy is offered during their hospital stay and post-discharge, as well as referrals at discharge for outpatient counseling and medication support.
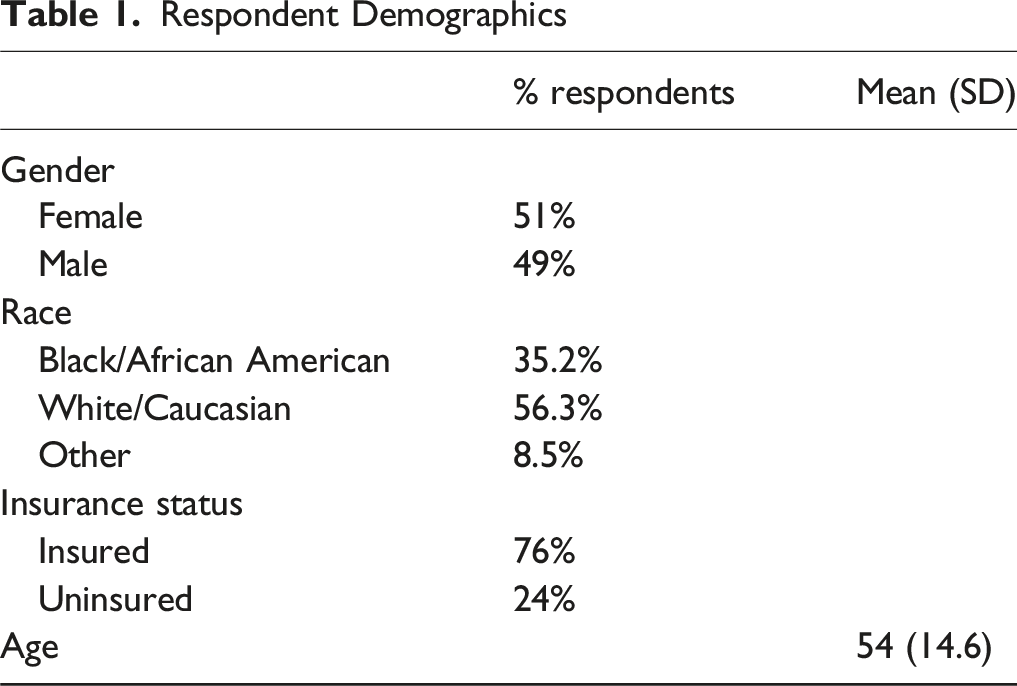
Out of 239 patients contacted, 71 agreed to participate (30% response rate). Demographics showed 51% female, 56.3% White/Caucasian, 35.2% Black/African American, and 8.5% other race. Survey respondents had a mean age of 54, with a standard deviation of 14.7.
Intervention
Data collection took place approximately 3 months after participants were discharged from the hospital to facilitate recall and assess outcomes post-discharge. The survey was administered using a multi-modal outreach process to increase response rates. Participants were initially contacted by email with an invitation to participate via their unique link. A follow-up email was sent to nonrespondents. If no response was received after a second email, study subjects were contacted via telephone up to 2 times. Less than 10% of survey responses were received via email. Phone survey calls were made by individuals who did not treat study participants to avoid response bias. Survey respondents were permitted to skip any question.
This study was reviewed by the UNC-Chapel Hill Human Subjects IRB and deemed not human-subjects research (IRB #22-2679).
Analysis
Survey analysis results involved primarily descriptive statistics. We used Fisher’s Exact Test in an exploratory analysis to examine whether satisfaction or smoking reduction/cessation varied significantly by race, insurance status, or gender.
Results
Overall, patients expressed very high satisfaction with their inpatient tobacco treatment experiences across multiple dimensions. Survey results related to patient satisfaction are shown in Figure 1. Survey participants strongly agreed/agreed that their cessation counselor was interested in improving their overall health (97%) and cared about their cravings for tobacco (90%). Almost all patients reported being provided with the resources necessary to reduce or quit tobacco use after discharge (91% strongly agree/agree). Almost all (97%) strongly agreed/agreed that tobacco treatment counselors provide an important service to help patients quit or reduce their tobacco use. Overall, patients reported that the time spent with a tobacco treatment counselor improved their overall hospital experience (84% strongly agree/agree). Satisfaction Survey Results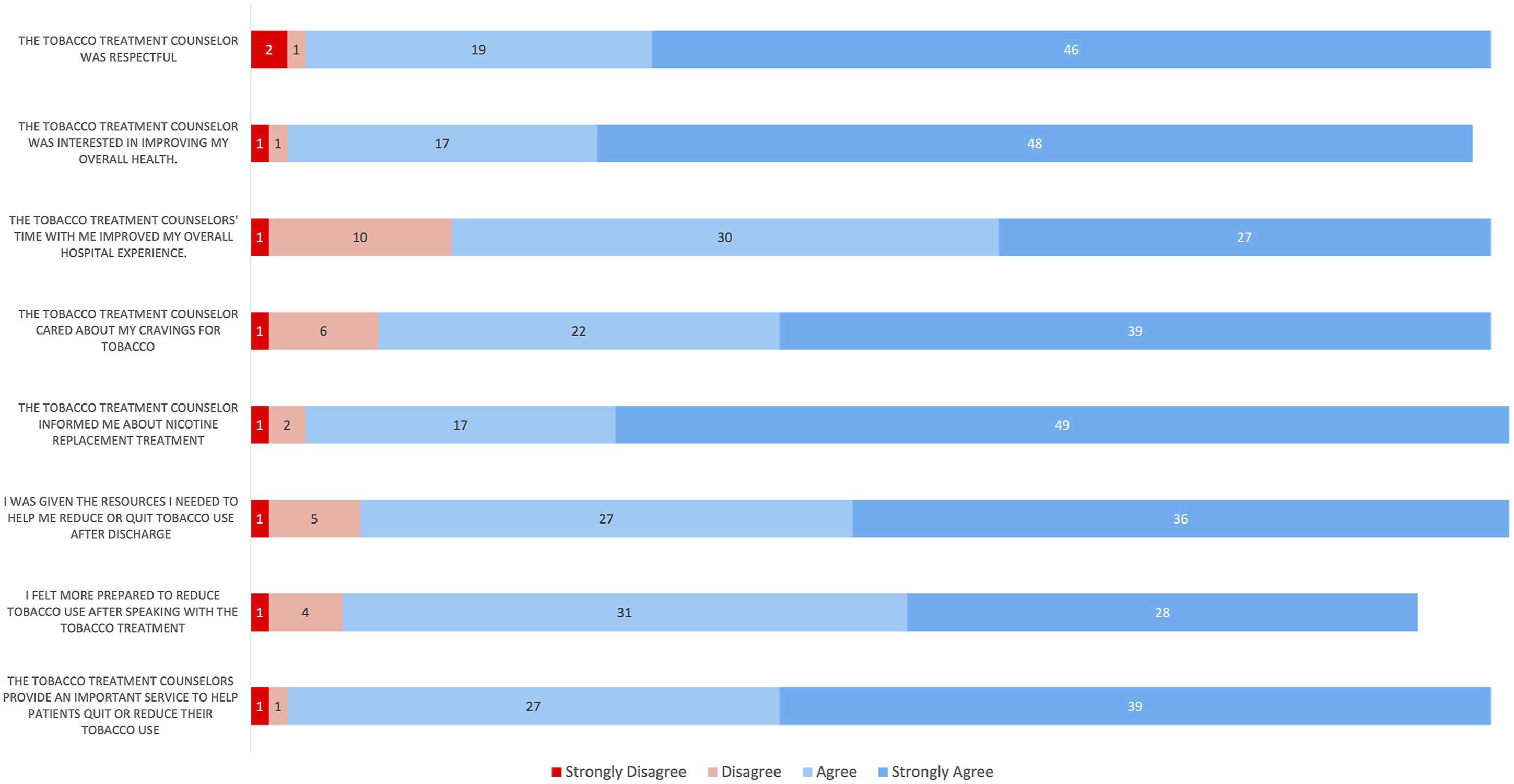
Respondent Demographics
Discussion
This report shows that remote inpatient tobacco cessation treatment with motivational interviewing, offers of pharmacotherapy support, and cessation resources post-hospitalization was met with high patient reports of satisfaction. Furthermore, a large majority of participants reported quitting or reducing their smoking after the inpatient consult. The fact that satisfaction was consistent across race, insurance status, and gender was reassuring, as clinical and policy guidelines emphasize that underserved population should receive similar counseling to all other populations. 14
Current research and national guidelines for tobacco use treatment emphasize many of the counseling competencies we measured through patient reports.15,16 For instance, respecting and engaging patients improves counseling success and cessation outcomes. 16 Key guideline strategies also include providing resources, information, and skills about cessation. 15 Other researchers have also reported that high satisfaction with counseling about preventive behaviors is associated with reports on behavior change outcomes. In 1 outpatient tobacco treatment study, patients who received comprehensive counseling in tobacco use treatment reported significantly higher satisfaction and intentions to quit, compared to those who did not receive comprehensive counseling. 17
This survey has several limitations. First, we acknowledge that the survey we used did not undergo psychometric validation, such as combining the items into a composite scale, thereby limiting our ability to assess internal consistency and overall satisfaction. We provide the survey here and encourage future research to test the construct validity of the survey items. The survey also had a low response rate. Higher response rates are needed to ensure generalizability, and future studies should incentivize responses if possible. Furthermore, only patients who expressed interest and participated in smoking cessation during their hospitalization were eligible to participate in this survey. We also do not know which survey respondents utilized NRT and how this may have impacted satisfaction. In general, the survey does not allow for exploration of patient experiences and factors influencing satisfaction. This research has been explored elsewhere in patient interviews. 18 Patients who were uninterested in smoking cessation support during their inpatient stay were not provided with such services and ineligible to participate in the survey. The acceptance rate for smoking cessation counseling during hospitalization is high (approximately 88%), but future studies should attempt to understand barriers to engagement among patients who use tobacco and decline tobacco use treatment services. Another limitation is the use of self-report. While biochemical evaluation was not feasible due to time and cost constraints, prior studies have shown a positive correlation of biochemically-confirmed and self-reported abstinence. 19 Finally, we did not track either utilization of or satisfaction with follow-up counseling. While our institution has high utilization of outpatient counseling post-discharge, we could not link any instances of post-visit follow-up to specific survey respondents.
Despite these limitations, this is one of the first studies to investigate patient satisfaction with inpatient tobacco cessation consults using a patient-centered survey instrument. While the survey will benefit from validation studies, this pilot shows promise, especially considering no differences appeared across gender, race, or insurance status, suggesting the questionnaire may be useful to a broad population. These findings suggest that inpatient tobacco treatment counseling may play a role in patient satisfaction and patient-reported smoking cessation, outcomes that are important to health system patients, providers, and administrators. Tobacco use treatment should be an integral, standard part of a hospital’s admission orders for patients who smoke because of tobacco cessation programs’ ability to improve health, lower healthcare costs, and provide a positive patient experience.4,20
The Satisfaction with Inpatient Tobacco Treatment Study, and future validations and iterations in other care settings, may help support the continuation of these programs. We have also provided this survey (Supplement 1) to support evaluation of other inpatient tobacco use treatment programs. The UNC Tobacco Treatment Program plans to implement this survey for use at the Lineberger Comprehensive Cancer Center to evaluate the program’s acceptability among patients with cancer and tobacco use. We invite and encourage other institutions to test, adapt, and implement this tool to evaluate their tobacco treatment programs. The Satisfaction with Inpatient Tobacco Treatment Study utilized a novel survey instrument to examine patient satisfaction with inpatient tobacco treatment. Inpatients were generally satisfied with the smoking cessation counseling provided during hospitalization. The survey instrument is provided such that future research may continue to test, refine, validate, and use it to assess satisfaction with their own tobacco treatment programs. Tobacco treatment services should be an integral, standard part of a hospital’s admission orders for inpatients who smoke because of their potential to improve health, lower healthcare costs, and provide a positive patient experience.So What?
Supplemental Material
Supplemental Material - Patient Satisfaction Survey for Inpatient Tobacco Cessation Treatment
Supplemental Material for Patient Satisfaction Survey for Inpatient Tobacco Cessation Treatment by Ana Jafarinia, Kimberly A. Shoenbill, Eiman H. Newcomer, Julie A. Hartzell, Brittany P. Sealby, Girolamo J. Finazzo, Flannery M. Jones, and Adam O. Goldstein in American Journal of Health Promotion
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The UNC Inpatient tobacco treatment program is funded through institutional support from UNC Health and the Lineberger Comprehensive Cancer Center and National Cancer Institute (P30CA016086).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.