
Abstract
Purpose
To investigate how physical function performance and arthritis-related pain relate to sensor assessed movement behaviors in a diverse sample of inactive adults with various forms of arthritis.
Design
Cross-sectional study.
Setting
Columbia, SC.
Subjects
Adults with arthritis (n = 267; 60.0% Black, 92.0% female, 64.1 ± 9.4 years) from a telephone-based walking intervention.
Measures
Movement behaviors (moderate to vigorous intensity physical activity, MVPA; sedentary time) were assessed with ActiGraph accelerometers at baseline. Physical function was assessed through the six-minute walk test (6MWT) and the 30-second chair stand test (30CST). Arthritis-related pain was measured through a visual analog scale.
Analysis
Multiple linear regression was used to examine the extent to which physical function performance and pain predicted movement behaviors while adjusting for sociodemographic and health characteristics.
Results
Better 6MWT performance was positively associated with more MVPA per week (P < 0.001). Worse performance in the 6MWT (P < 0.001) and less pain (P = 0.02) were associated with more daily time spent sedentary. Performance in the 30CST was not significantly associated with either movement behavior.
Conclusion
These findings emphasize the importance of functional endurance and pain management in promoting physical activity and sedentary behavior among inactive adults with arthritis. Future public health interventions should prioritize strategies to enhance these components to effectively promote physical activity and less sedentary time.
Clinical Trial Registry Name: Phone-Based Walk with Ease Program for Adults with Arthritis
Introduction
Arthritis is one of the leading causes of disability in the United States, impacting one-quarter of the United States population. 1 Commonly reported symptoms of arthritis include joint pain, stiffness, and limited range of motion with varying degrees of severity depending on the type and progression of the disease. 2 Collectively, the presence of these symptoms has resulted in attributable activity limitations for nearly 45% of those with doctor-diagnosed arthritis in the United States. 1
Regular engagement in physical activity has been recognized as a non-pharmacological approach to arthritis management.3,4 Although routine participation in aerobic activity has been demonstrated to improve arthritis-related symptoms, 5 only 36.2% of adults with arthritis meet the national guidelines of 150 minutes/week of moderate-to-vigorous-intensity physical activity activity (MVPA). 6 Among different forms of arthritis, it has been reported that only 29% of adults with rheumatoid arthritis and just 11% of those with osteoarthritis met the recommended levels of aerobic physical activity.7,8 Additionally, adults with arthritis spend at least two-thirds of their waking day engaged in sedentary behavior. 9 Failure to attain recommended levels of physical activity and the adoption of a sedentary lifestyle can negatively impact physical health in adults with arthritis by exacerbating arthritis-related symptoms, reducing functional capacity, and raising the risk of disability.10-12
Of these, better physical functioning has been shown to be one of the most consistent factors associated with appropriate levels of physical activity 13 and reduced sedentary time 9 among adults with arthritis. While the existing scientific literature supports the positive association between functional performance and attainment of recommended levels of physical activity among adults with arthritis, 14 few studies have specifically examined the association between 6MWT performance and sensor-assessed MVPA across a diverse sample of inactive adults with various forms of arthritis. Additionally, previous research has shown that regular physical activity can help manage pain in certain types of arthritis including osteoarthritis 12 or rheumatoid arthritis. 11 However, there is also evidence that lower arthritis-related pain to be associated with higher fitness levels, such that those experiencing less pain have maintained longer-term adherence to physical activity. Therefore, this evidence presents a challenge for public health efforts, as it highlights a complex relationship between pain, fitness, and inactivity that must be considered when developing interventions for inactive adults with arthritis. Further, certain populations with arthritis may lack awareness of the negative impact prolonged sedentary time can have on arthritis-related outcomes and believe that increasing MVPA alone can offset the effects of excess sedentary behavior. 15 Since physical activity and sedentary behavior are distinct movement behaviors, further research is needed to understand how pain and functional performance differentially relate to each behavior among inactive adults with diverse arthritis conditions.
Therefore, the purpose of the current study was to examine how physical function performance and arthritis-related pain relate to sensor-assessed movement behaviors, specifically MVPA and sedentary time, in a diverse sample of inactive adults diagnosed with various forms of arthritis.
Methods
Study Overview
This cross-sectional analysis of secondary data included adults with arthritis enrolled in a randomized controlled trial examining the effects of a 6-week telephone-delivered walking intervention. Only baseline data, collected before randomization, were used. All procedures were approved by the University of South Carolina Institutional Review Board and complied with the Declaration of Helsinki. Written informed consent was obtained from all participants prior to participating in any study procedures.
Participants
Participants were recruited from the community using a variety of strategies, including print (eg, flyers, magazines) and digital (eg, radio, social media, television) advertising. Study inclusion for the parent study were: doctor diagnosis of some form of arthritis derived from the Centers for Disease Control and Prevention’s definition, 16 ability to read and write in English, willingness to be randomized to immediate or delayed physical activity intervention condition, and no plans to relocate away from the study area for the next year after enrollment. Participants were excluded if there were medical contraindications to exercise, if they were pregnant, breastfeeding, or planning to become pregnant in the next year, or if they had a serious cognitive impairment.
Demographic, Health, and Anthropometric Measures
Demographic characteristics, including income, age, sex, race, marital status, education level, and employment status, were obtained. Height and weight were measured using a stadiometer and digital scale, respectively. Participants removed their outerwear, shoes, and personal belongings before each measurement. Weight was recorded to the nearest 0.1 kg and height to the nearest 0.1 cm. Body mass index (BMI) was calculated as kg/m2. Participants also self-reported their arthritis diagnosis (eg, osteoarthritis, rheumatoid arthritis, fibromyalgia, gout, lupus).
Movement Behaviors
Movement behaviors of MVPA and sedentary time were measured with waist-worn ActiGraph GT9x link accelerometers. Participants were instructed to wear the accelerometer for 7 days during waking hours. Previously reported cut-off points were used to distinguish MVPA (≥2020 counts/min) and sedentary time (<100 counts/min). 17 Non-wear time was defined as ≥90 minutes with zero consecutive activity counts based on 1-minute time intervals. 18 Individuals with ≥4 valid days (≥10 hours of wear time) were included in the analyses. 19 Minutes of MVPA per week and percentage of daily waking time spent sedentary were used.
Physical Function
Physical function was assessed through the 30-second chair stand (30CST) and the 6-minute walk test (6MWT), following the Osteoarthritis Research Society International guidelines. 20 For the 30CST, participants were instructed to perform as many sit-to-stand repetitions as possible within 30 seconds. For the 6MWT, participants were instructed to walk as quickly but as safely as possible between each end of a 50-foot course for a period of 6 minutes. Distance traveled during the 6MWT was calculated in feet.
Pain
Severity of arthritis-related pain was assessed with a visual analog scale (VAS). Participants placed one mark on a 100-mm line scored from 0-100, with higher scores indicating greater symptom pain severity. The VAS for pain severity has excellent test-retest reliability when used in various rheumatic populations such as osteoarthritis 21 and rheumatoid arthritis. 22
Data Analysis
All statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC, USA). Descriptive statistics were used to describe the baseline characteristics of the sample. Multiple linear regression was used to test the association of physical function performance (30CST, 6MWT) and pain with each movement behavior (MVPA, daily sedentary time) after adjusting for age, sex, BMI, race, education, income, and employment. Accordingly, one model was constructed for each movement behavior (ie, MVPA, daily sedentary time), using pain and the two physical function performance measures as predictor variables while adjusting for relevant sociodemographic and health-related factors. Because MVPA (skewness = 2.50, kurtosis = 7.44) had a positively skewed distribution, natural logarithm transformation was applied. Statistical significance was set as P < 0.05 for all analyses.
Results
Sample Characteristics
Sociodemographic Characteristics, Movement Behaviors, Physical Function, and Arthritis-Related Pain of the Study Sample
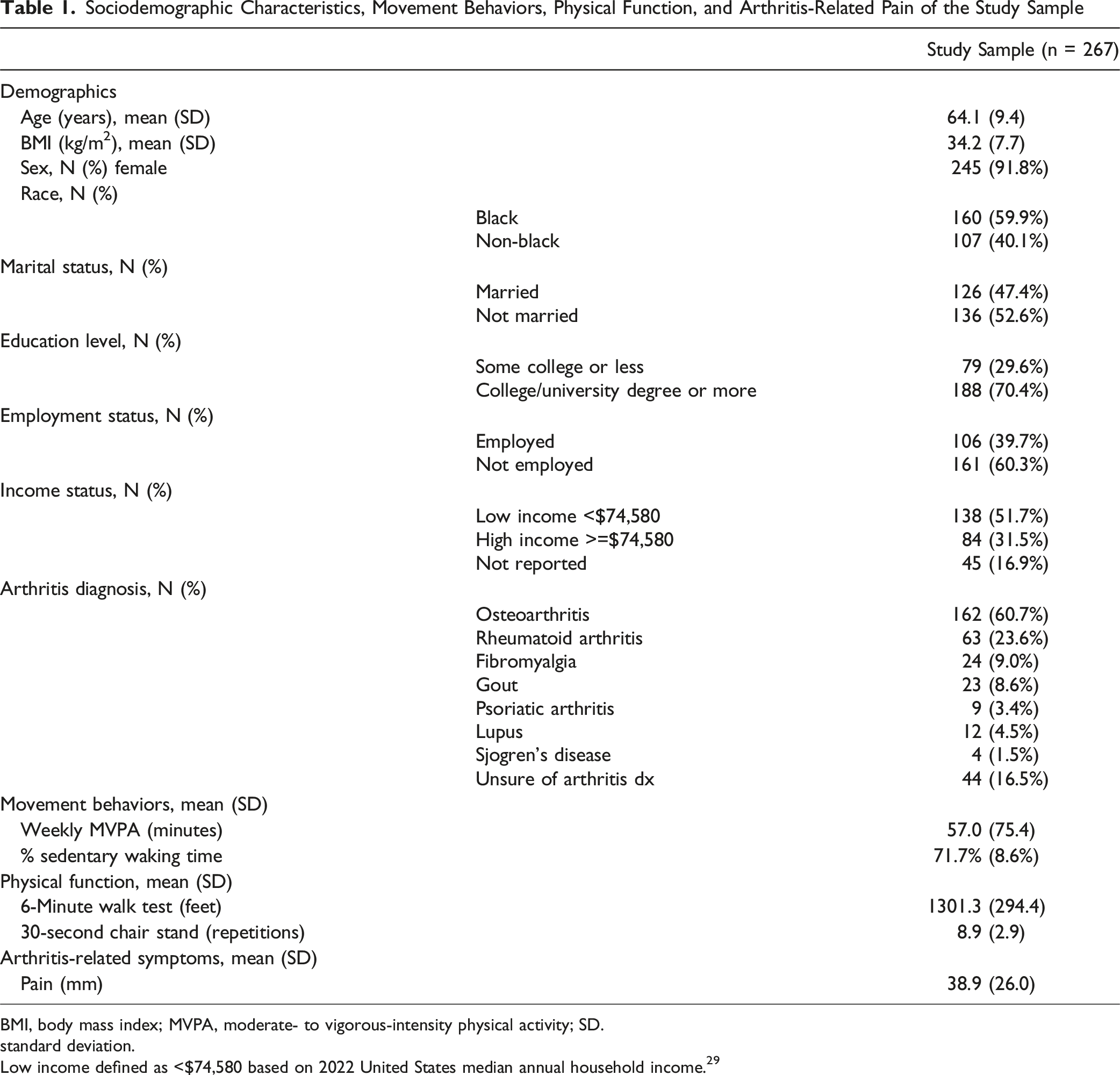
BMI, body mass index; MVPA, moderate- to vigorous-intensity physical activity; SD.
standard deviation.
Low income defined as <$74,580 based on 2022 United States median annual household income. 29
Association of Physical Function and Pain with Movement Behaviors
Associations Between Physical Function Performance and Arthritis-Related Pain on Movement Behaviors
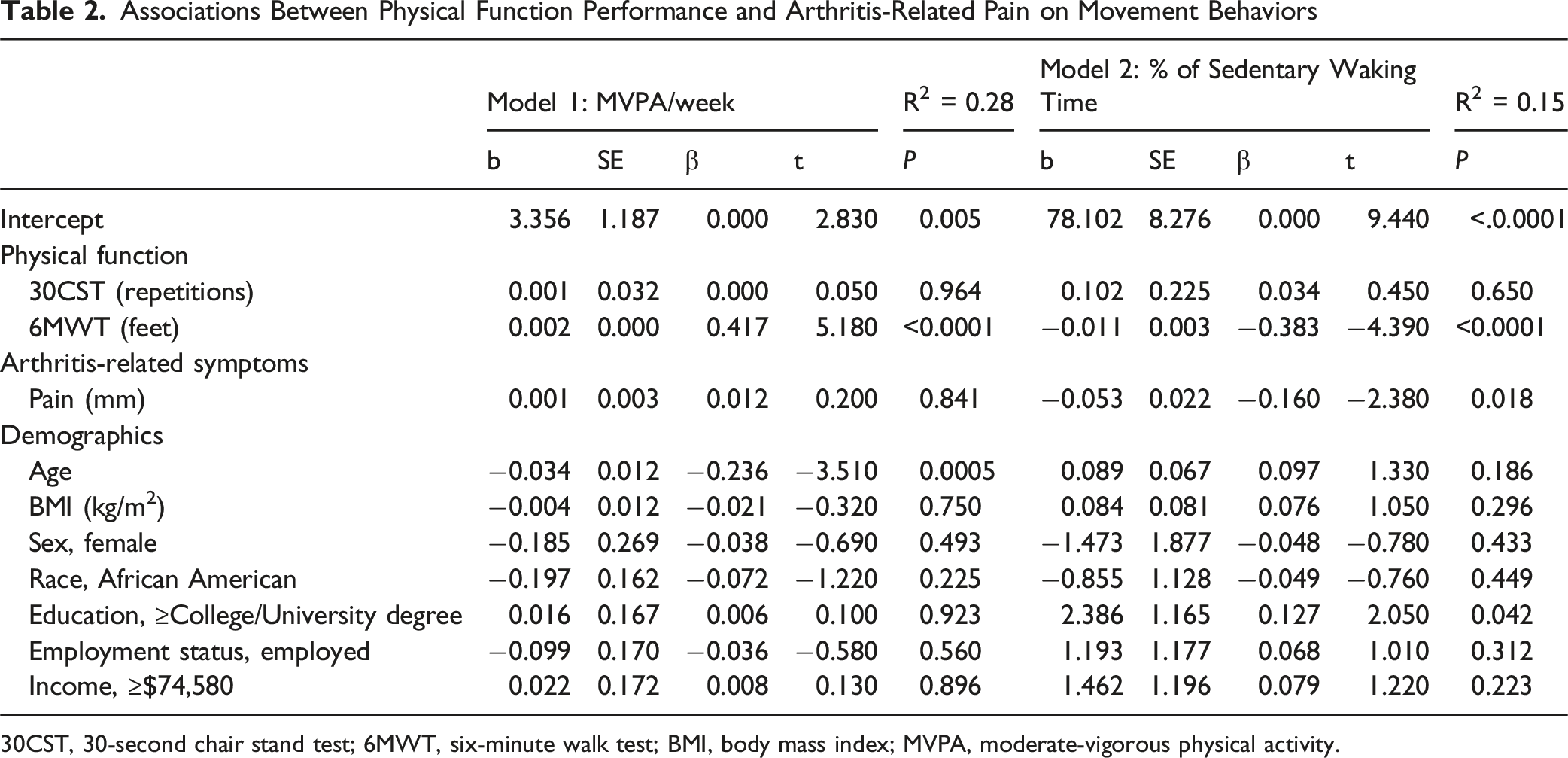
30CST, 30-second chair stand test; 6MWT, six-minute walk test; BMI, body mass index; MVPA, moderate-vigorous physical activity.
Discussion
The purpose of this study was to examine the relationships between physical function performance and pain on sensor-assessed movement behaviors among inactive adults with arthritis. Overall, better 6MWT performance was associated with more time spent per week engaging in MVPA. Further, lower 6MWT performance and less arthritis-related pain were associated with more daily time spent sedentary. Lastly, performance in the 30CST was not associated with weekly MVPA or daily time spent sedentary.
Findings in this study suggest that individuals with better physical functioning (higher 6MWT scores) engaged in higher levels of sensor-assessed MVPA. The results are consistent with previous literature highlighting the association of better 6MWT performance with meeting guidelines of 150 min/week of self-reported 23 and sensor-assessed MVPA. 24 The results of this study highlight the potential of using the 6MWT as an indicator of MVPA, should sensors not be available to measure physical activity levels, as well as using future research to explore ways to improve 6MWT performance in adults with arthritis.
As observed in this study, worse physical functioning (lower 6MWT scores) was associated with higher levels of sensor-assessed daily sedentary time. Findings from this study complement existing literature demonstrating an inverse association between physical function performance and sedentary behavior, 9 including prior evidence specifically linking 6MWT performance to sensor-assessed daily sedentary time among adults with inflammatory arthritis. 24 Further, previous reports among those with various forms of arthritis have reported sensor-assessed daily sedentary time ranging from 67%–71%,9,25,26 which is similar to the findings of this study where the study sample spent 72% of their waking day engaged in sedentary behavior. Collectively, these results further emphasize the high amount of time that adults with arthritis spend in sedentary time, as well as the importance of distinguishing sedentary behavior and MVPA as independent behaviors. Previous qualitative work has suggested that adults with osteoarthritis may not be aware of the consequences of excess sedentary behavior on health 15 ; thus, it may be helpful to increase awareness of the risks of excess sedentary time. Further, helping to improve performance in the 6MWT time may not only aid in increasing MVPA, but also reduce the time spent in sedentary time.
Interestingly, the findings of this study suggest that while pain was not predictive of MVPA, lower levels of pain were associated with more time spent in sedentary behavior. Results from the pain and physical activity literature have been mixed with positive, negative, and null relationships all reported. 27 In terms of sedentary time, the current results are similar to a previous study using ecological momentary assessment to examine the association between pain and sensor-assessed sedentary behaviors in adults with osteoarthritis. 28 Their results found that more sedentary time was associated with less pain in the short term. It is possible that individuals with arthritis may have reductions in pain following sedentary behavior, which reinforces or further encourages spending more time in sedentary behavior. More studies are needed to determine the temporal relationship between sedentary time, pain, and physical activity in adults with arthritis.
Despite the associations of 6MWT performance with both weekly MVPA and daily time spent sedentary, no association was found between 30CST performance and either movement behavior. Results from the Osteoarthritis Initiative indicated that individuals with knee arthritis who were in the most sedentary quartile demonstrated significantly lower chair stand performance compared to those who were less sedentary, however a different chair stand measure was used (ie, five time sit to stand test). 9 In addition, our study’s two measures of function measure different underlying domains, which might explain the different pattern of findings. The 6MWT is a measure of aerobic capacity and endurance, whereas the 30CST is a measure to assess lower body strength. Given that the sensor-based assessment of MVPA used in the current study assesses aerobic activity such as walking, it aligns more closely with the 6MWT than with the 30CST. Thus, among a diverse sample of inactive adults, functional assessments targeting the aerobic system may be more applicable in predicting movement behaviors such as MVPA and sedentary time as compared to functional assessments for strength.
Strengths associated with this study include the use of sensor-assessed movement behaviors captured through waist-worn accelerometers and physical function performance measured with the 6MWT and 30CST. Furthermore, objective measurements of activity and function were taken with a large sample across numerous arthritis diagnoses. However, this study is not without limitations. The study sample consisted of adults with arthritis in the southeastern region of the United States, and all participants were interested in joining a physical activity program; thus, physical activity and function levels may not be generalizable to other regions or to those not interested in physical activity. Future research should include more diverse populations to improve generalizability and to better understand the influence of arthritis-related outcomes on movement behaviors across the broader arthritis populations.
In conclusion, the findings of this study suggest that better physical function, as measured by the 6MWT, is associated with increased engagement in MVPA, while poorer functional performance and lower pain levels are associated with more time spent daily in sedentary behavior. Further, performance in the 30CST was not associated with either movement behavior, suggesting that lower extremity strength may be less influential when aiming to improve MVPA or reduce sedentary behavior among adults with arthritis. Overall, the results underscore the importance of endurance-related functional capacity in influencing activity patterns and sedentary behavior. Regular participation in physical activity has been shown to improve arthritis-related symptoms; however, 36% of U.S. adults are physically inactive and spend approximately two thirds of their day engaged in sedentary behavior with even lower activity levels observed among individuals with osteoarthritis and rheumatoid arthritis. Factors such as physical functioning have been shown to influence specific movement behaviors, however the extension of these findings to performance-based measures as seen in the 6MWT across diverse inactive arthritis populations remains limited. Further, while some evidence suggests less arthritis-related pain to be associated with less time spent sedentary and higher levels of MVPA, the extension of these findings remain mixed when applied to inactive adults with various forms of arthritis. This cross-sectional study contributes to the existing scientific literature such that among a sample of inactive adults with arthritis, better performance in the 6MWT was associated with higher levels of weekly MVPA while poorer performance was associated with more daily time spent sedentary. Additionally, among a diverse sample of inactive adults with various forms of arthritis, more daily time spent sedentary was associated with less arthritis-related pain. Overall, these findings highlight the complex relationship between objective measures of physical functioning and arthritis-related pain in the context of sensor-assessed movement behaviors. Although causality cannot be established, findings from this study can help inform future physical activity interventions aimed at adults with arthritis by prioritizing strategies to enhance better functional endurance and pain management. Given the observed relationship between 6MWT performance and both MVPA and sedentary time, attention should be directed towards improving these distinct movement behaviors by prioritizing more sedentary breaks throughout the day and tailoring physical activity plans to support improvements in functional capacity. Lastly, due to the mixed evidence regarding the association between arthritis-related pain and movement behaviors, findings from this study found that among a sample of adults with various forms of arthritis less pain was associated with more daily time sedentary, while no relationship was observed between pain and MVPA. Therefore, future physical activity interventions targeting inactive adults with arthritis should include strategies to manage arthritis-related pain throughout the program to promote long term adherence towards increased physical activity and reduced sedentary time.So what?
What is Already Known on This Topic?
What Does This Article Add?
What are the Implications for Health Promotion Practice or Research?
Footnotes
Ethical Considerations
This retrospective study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board at the University of South Carolina (IRB # Pro00115106) on 09/28/2021. All participants provided written informed consent prior to participating.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by Cooperative Agreement Number U48DP006401 from the Centers for Disease Control and Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the Department of Health and Human Services. This research was also supported in part by the USC Behavioral-Biomedical Interface Program, which is a NIGMS/NIH-T32 supported program. Contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of the NIGMS or NIH.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.