
Abstract
Purpose
Develop a parsimonious model of individuals at heightened-risk for 3-year cardiometabolic multimorbidity (CM) onset.
Design
An observational, secondary analysis of Canadian Longitudinal Study on Aging (CLSA) data.
Setting
CLSA is a national cohort study in Canada. Baseline data were collected between 2010-2015, and follow-up data were collected between 2015-2018.
Subjects
CLSA included community-dwelling adults aged 45-85 at recruitment from across Canada.
Measures
Health conditions: stroke, heart disease or heart attack and diabetes. Personal factors: age, sex, marital status, household income, education, and ethnicity. Environmental factors: social support, personal assistance, and location of residence. CM cases: at least two of stroke, heart disease and diabetes at follow-up assessment.
Analysis
Hierarchical logistic regression analyses with backwards elimination procedures were used to develop a parsimonious prediction model.
Results
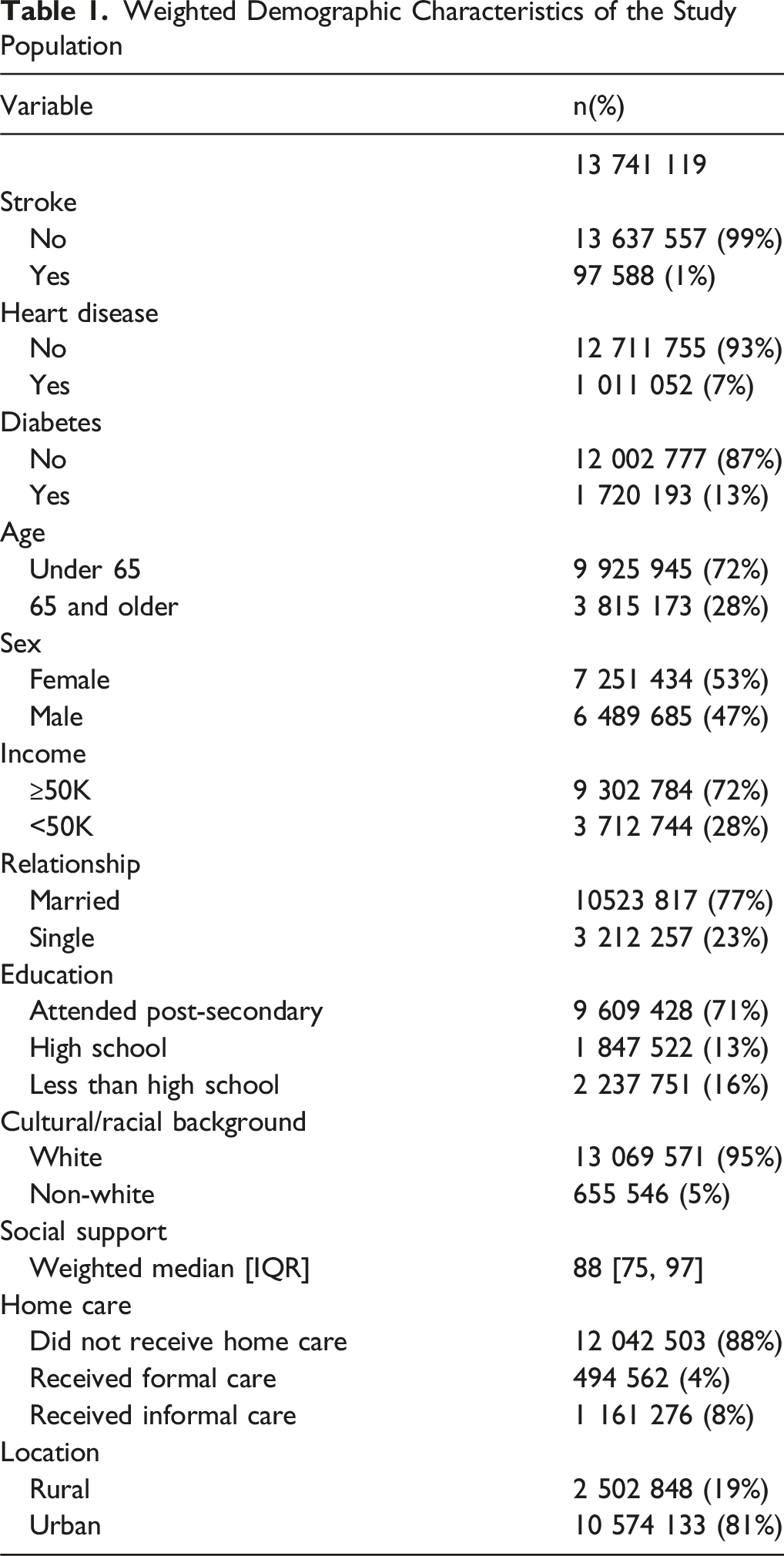
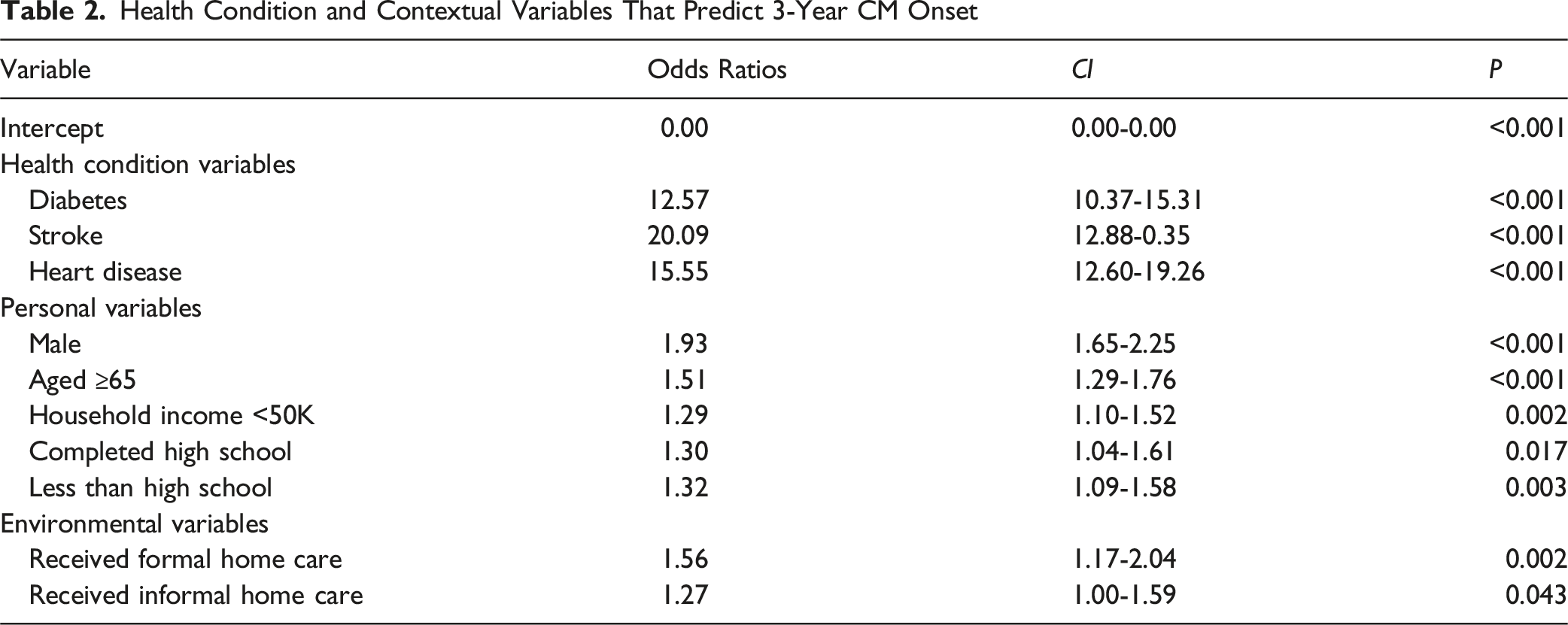
The sample consisted of 41 841 individuals, representing a weighted population of 13 741 119. The population had a mean age of 62.3 years (SD = 10.1), was 53% female, predominantly married or in common-law relationships (77%), post-secondary graduates (61%), white (95%), and lived in an urban area (81%). Males (OR:1.93, 95%CI:1.65-2.25, P < 0.001), ≥65 years (OR:1.51, 95%CI:1.29-1.76), P < 0.001), who had stroke (OR:20.09, 95%CI:12.88-30.35, P < 0.001), heart disease (OR:15.55, 95%CI:12.60-19.26, P < 0.001), or diabetes (OR:12.57, 95%CI:10.37-15.31, P < 0.001), not completed post-secondary (OR:1.30, 95%CI:1.04-1.61, P = 0.017), income of <50k (OR:1.29, 95%CI:1.10-1.52, P = 0.002), and received home care (OR:1.56, 95%CI:1.17-2.04, P = 0.002) were at heightened risk of CM.
Conclusions
Developing a profile of high-risk individuals may enhance the efficiency of CM prevention and reduce disease onset. Critical limitations include the CLSA exclusion criteria, and the small proportion of minoritized individuals that restrict generalizability in these populations.
Purpose
Cardiometabolic multimorbidity (CM) is the diagnosis of at least two of stroke, heart disease and diabetes. 1 CM is a serious health concern due to its association with an increase in premature mortality risk, 1 mental health 2 and cognition challenges, 3 and activity limitations. 4 One way to reduce the health and economic burden of multimorbidity is through prevention. By increasing our understanding of who is at a heightened risk of developing CM, we may prevent the onset of CM and subsequent exposure to increase risk of mortality and disability for many individuals. Therefore, the objective was to identify health conditions and contextual factor variables (i.e., personal and environmental factor variables as per the International Classification of Functioning, Disability and Health [ICF]) that predict 3 year CM onset to develop a profile of individuals at a heightened risk of developing CM.
Methods
Design
We performed a secondary analysis on data from the Canadian Longitudinal Study on Aging (CLSA), a large, national, population-based study of community-dwelling Canadians. Ethics approval (H22-01358) was obtained by the University of British Columbia Behavioural Research Ethics Board.
Sample
The CLSA seeks to examine aging-related health trajectories and explore determinants of healthy aging in Canada. It includes a stratified random sample of approximately 51 000 Canadians aged 45-85 at recruitment. 5 Baseline data was collected between 2010-2015, and 3 year follow-up data was collected between 2015-2018. The CLSA sample is comprised of a tracking and comprehensive cohort. Participants were selected through structured probability sampling methods which included using the Canadian Community Health Survey on Healthy Aging, Provincial Health Registries, and random-digit dialing. Data was collected through in-home interviews and at 11 data collection sites (Victoria, Vancouver, Surrey, Calgary, Winnipeg, Hamilton, Ottawa, Montreal, Sherbrooke, Halifax, and St. Johns) located in seven provinces across Canada in the comprehensive cohort. In the tracking cohort, individuals were recruited from all ten provinces with no geographic restrictions and data was collected through computer-assisted telephone interviews.
Excluded from the CLSA were people living in the three territories and some remote regions, persons living on federal First Nations reserves, full-time members of the Canadian Armed Forces, individuals living in institutions at recruitment, those unable to respond in English or French, or with cognitive impairment at recruitment. We also excluded those with CM at baseline and included all others who had data available for our variables of interest.
Measures
Variables included in the study were organized by The International Classification of Functioning (ICF). 6 As per the ICF, personal factor and environmental factor variables influence the health of individuals. A Delphi survey exercise of 64 international chronic disease experts systematically identified functioning and disability variables common among people with stroke, heart disease, and diabetes using the ICF as a guiding framework. 7 In the current study, we included variables identified during the Delphi survey that were also available in the CLSA.
Dependent Variable
3-year CM onset: CM cases are considered at least two of diabetes, heart disease (heart disease or heart attack), or stroke at 3-year follow-up.
Independent Variables
Health conditions: Participants were asked, “has a doctor ever told you that you: have experienced a stroke or CVA (cerebrovascular accident)?… Have heart disease (including congestive heart failure, or CHF)?… Have had a heart attack or myocardial infarction?… Have diabetes, borderline diabetes, or that your blood sugar is high?”.
Personal factors: (i) Age (<65 vs ≥ 65). (ii) Biological sex (male vs female). (iii) Marital status options included single or never married, married/living with partner, widowed, divorced, and separated. Responses were combined to married vs single. (iv) Household income (<50K vs ≥ 50K). (v) Education options included less than secondary school, secondary school graduation but no post-secondary education, some post-secondary education, and post-secondary degree or diploma. Responses were categorized into less than secondary school, secondary school graduation, and attended post-secondary education. (vi) Cultural/racial background had 13 response options. Responses were categorized into white and non-white, as the proportion of white only respondents was 95%.
Environmental factors: (i) Social support was measured using the 19-item Medical Outcomes Study: Social Support Survey (MOS). 8 This scale shows high internal-consistency reliability (α = 0.97), test-retest reliability (1-year stability coefficient = 0.78), and validity. The MOS has been validated within multiple countries and various populations. 9 We included a composite score calculated by the CLSA, which indicates the overall level of functional social support that is available to the participant. Scores range from 0-100, in which higher scores indicate more social support. 10 (ii) Personal assistance was collected with a CLSA derived variable which indicates the type of home care a participant received in the past 12 months. Informal care includes care provided by family, friends or neighbors, while formal care includes professional assistance because of a health condition or limitation. 11 Response options included did not receive home care, formal home care only, informal home care, and both formal and informal home care. We categorized responses into did not receive home care, formal home care (formal home care only and both formal and informal home care), and informal home care. (iii) Rural or urban location of residence was explored using the Canada’s Postal Code Conversion File to define the region using the participant’s postal code data. 12 Regions are categorized into rural, urban core, urban fringe, secondary core, and urban population center outside CMA (census metropolitan area) and CA (census agglomeration). For this analysis, responses were dichotomized into rural vs urban.
Analysis
Participants’ baseline and 3 year follow-up data were linked using their entity ID. Descriptive statistics were used to characterize the sample. Continuous variables are presented as medians and IQR while categorical variables are presented as frequency counts and percentages. Participants responses of “don’t know” and “refused” were treated as missing. The CLSA inflation weights were used in the descriptive analysis and analytic weights were used in the logistic regression analysis. Each CLSA participant is assigned a sample inflation weight constructed based their probability of inclusion in the study. The likelihood of selecting participants varied across different sub-groups, as did the probability of their agreement to participate. 13 Applying the weights mitigates bias by correcting for unequal sampling probabilities, frame coverage errors and non-response rates, and to improve the precision of estimates by using auxiliary information allowing for more valid inferences. 13
Hierarchical logistic regression analyses were used to develop the parsimonious prediction model identifying relevant health and contextual factors that predict 3 year CM onset. In the iterative process of developing the model, health condition variables (i.e., diabetes, stroke, and heart disease) were entered first, personal factor variables were entered second, and the environmental variables were entered third, consistent with previous literature. 14 At every stage, each variable had to have statistically significant (P < 0.05) odds of predicting CM and backwards elimination procedures were used. Multicollinearity was checked using the generalized variance inflation factor (GVIF). 15 Variables with a score less than 2 are considered to not have any multicollinearity concerns. If the score is higher than 2, the variable with the highest correlation with CM onset would be entered into the model. Model performance was assessed using the Brier score, Nagelkerke’s R2, and measures of discrimination and calibration. All analyses were performed using RStudio (version 4.3.1) at a significance level of P < 0.05.
Results
Weighted Demographic Characteristics of the Study Population
The GVIF was less than 2 for all variables in the models, indicating no multicollinearity. The scatterplot testing the linearity of the log-odds assumption showed a consistent pattern, with the relationship between social support and the logit appearing roughly linear. We then further confirmed this by fitting a linear regression model, which showed a significant, non-zero slope, indicating the linear assumption was met.
Health Condition and Contextual Variables That Predict 3-Year CM Onset
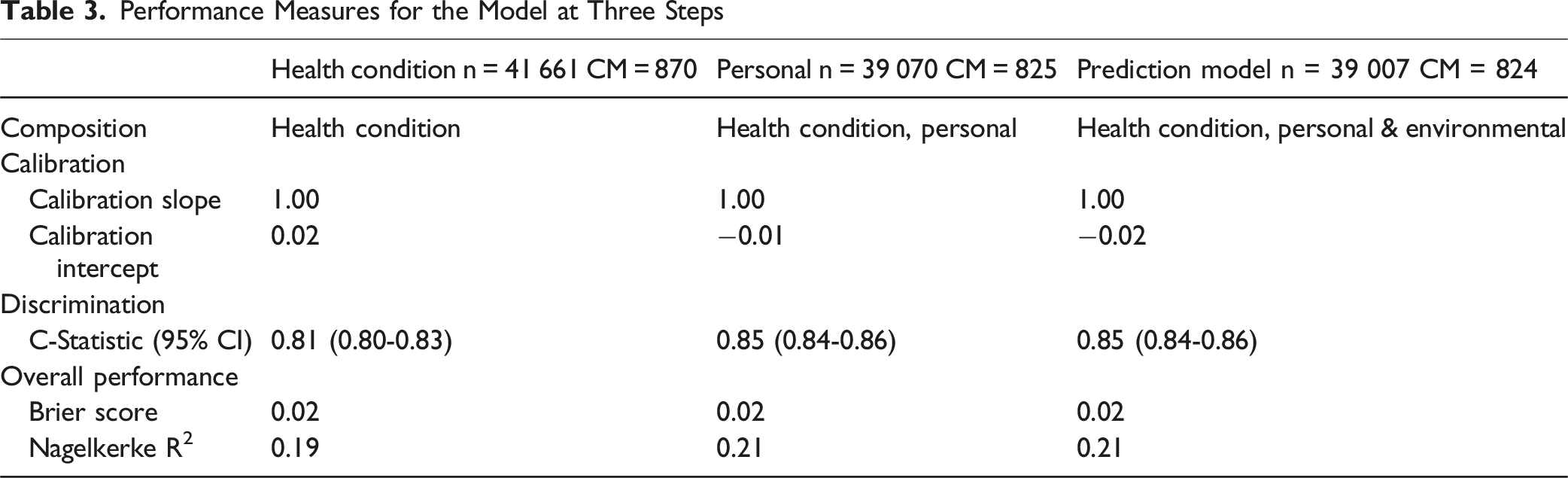
Performance Measures for the Model at Three Steps
Discussion
Summary
This large, population-based study adds to the existing literature by identifying who is most at risk of developing CM using a parsimonious model. Parsimonious models are more likely to be used routinely in clinical practise compared to more complicated models as they have improved interpretability and user experiences. 16 Given the association of CM with mortality risk, negative health outcomes, and high economic and healthcare resource burden, routine screening of high-risk individuals to reduce incidence is essential. Our findings indicate that males who had a previous condition, had not attended post-secondary education, had a low household income, and received home care had a higher risk of 3-year CM onset. The high odds ratios for stroke, heart disease and diabetes highlight the critical need for early intervention and (self-)management of individuals with these conditions to prevent CM. Our final model demonstrated strong predictive performance. The Nagelkerke R2 increased from 0.19 to 0.21 with the inclusion of additional risk factors, suggesting a modest improvement in the model’s explanatory power. More notably, the c-statistic improved from 0.81 to 0.85 in the final model, indicating excellent discrimination. Additionally, the calibration slope remained stable at 1.00, suggesting that the predicted probabilities closely aligned with observed outcomes, reinforcing the reliability of the model.
In agreement with our findings, previous literature shows an association between age 17 and low income 18 with CM. Our finding of incidence of CM onset being higher in males than females was surprising given previous literature reporting that in the progression from healthy to first condition, and from first condition to CM, females were more at risk compared to males. 19 We also showed that less education was an important risk factor. Well-educated individuals have been shown to be more capable of navigating more complicated self-care regimens, 20 as used in the treatment of multimorbidity. Thus, not only are individuals with lower education levels at a higher risk of developing CM, but they may also face subsequent challenges managing their CM and therefore require especially high preventative attention.
A surprising finding is that social support was not found to be an important predictor of CM onset. Higher levels of social support have been identified as a protective factor against multimorbidity by increasing a person’s resilience, 21 whereas social isolation poses numerous health risks and has been linked to multimorbidity onset. 22 The non-significance of social support may be due to the high baseline of social support, in that the protective effects may have reached a ceiling effect that most participants had reached. In addition, there may be insufficient variability within this variable making it difficult to detect a meaningful difference between those with lower and higher levels of social support and the risk of developing CM.
Treating multimorbidity is challenging, and effective prevention likely requires a broad assessment of multiple risk factors, with targeted interventions focusing on modifiable risk factors. 23 While prognostic models exist for individual diseases, fewer models specifically predict multimorbidity. 24 Relying on single-disease models in clinical settings is both burdensome and potentially inaccurate. 24 Establishing multimorbidity-specific risk factors is crucial for accurately identifying high-risk patients and informing prevention efforts. 24 Our findings improve clinicians’ ability to identify individuals at increased risk of developing CM, enabling earlier intervention and tailored prevention strategies. The focus can then shift towards addressing established modifiable risk factors of CM onset, 25 such as unhealthy diets, lack of physical activity, tobacco use, and excessive alcohol consumption, amongst high-risk populations.
Furthermore, collaboration between clinicians and policymakers is essential for comprehensive prevention strategies which integrate multiple risk factors. 23 Given the disproportionate risk among individuals with lower income and education, public health policies should prioritize screening and prevention programs in lower-income communities. In addition, our findings indicate that individuals receiving home care are at increased risk of CM, likely due to existing health conditions and barriers to traditional healthcare access. Strengthening home-based preventive care or screening programs could help ensure early identification and intervention for this vulnerable population. As policymakers and clinicians increasingly recognize the importance of multimorbidity prevention, 24 advancing predictive models and targeted interventions will be essential for reducing the burden of CM.
Limitations
Our reliance on self-reported measures and disease status may result in inaccurate diagnoses. Self-reports can introduce recall and social desirability bias, which can threaten internal validity. There is also an overestimation in the prevalence of diabetes as the CLSA grouped people with type 1 diabetes, type 2 diabetes, and those with prediabetes into one variable. Follow-up questions about the type of diabetes were not available in the baseline tracking cohort. To maintain consistency, we used the grouped variable available in all datasets. We are limited by the CLSA exclusion criteria, most notably excluding individuals who lived in long-term care, those living in the three territories, Indigenous populations living on federal First Nations reserves, and full-time members of the Canadian Armed Forces. Moreover, the CLSA has a small proportion of minoritized individuals, 26 and the demographic profile of CLSA participants may not be fully representative of local populations. As a result, our findings may not capture the experiences of individuals with different healthcare access, social determinants of health, or environmental exposures. For instance, individuals in remote or northern regions of the territories face unique barriers to healthcare access that may influence CM onset. Additionally, Indigenous populations and military personnel may have different CM risk factors due to distinct social, occupational, and historical factors. Future research is required within these populations to increase generalizability and to ensure a comprehensive understanding of CM risk across diverse groups. We also acknowledge that some degree of selection bias is likely given the nature of the study design. However, the CLSA’s use of probability-based recruitment strategies and the use of CLSA weights in our analyses helped to mitigate its impact and increase generalizability. Lastly, excluding those with missing data for our study outcomes may have introduced bias if data were not missing at random. Future research should explore methods to account for these biases, such as data imputation techniques, to enhance the robustness of findings.
Significance
This study highlights the critical need for early identification and management of individuals at risk for CM, emphasizing the importance of addressing socioeconomic factors in prevention strategies. By integrating these insights into clinical practice, healthcare providers can more effectively allocate resources and tailor interventions to those most in need, ultimately reducing the incidence and burden of CM. CM is a growing public health concern due to its association with increased mortality and disability. Prevention strategies that focus on early identification of high-risk populations are essential for reducing the incidence of CM. We developed a profile of individuals who are at a high risk of CM onset, which is males who had diabetes, heart disease or stroke, had not attended post-secondary education, had a low household income, and received home care. The findings have direct health promotion implications for targeted prevention strategies in high-risk populations to reduce CM incidence. Clinicians should prioritize screening for individuals with a history of diabetes, stroke, or heart disease, particularly those with lower socioeconomic status. Given the socioeconomic disparities in CM risk, policy makers should focus on increasing access to preventive care, including chronic disease management programs for vulnerable populations.So What?
What is already known on this topic?
What does this article add?
What are the implications for health promotion practice or research?
Footnotes
Acknowledgements
This research was made possible using the data collected by the Canadian Longitudinal Study on Aging (CLSA). This research has been conducted using the CLSA Baseline Comprehensive Dataset version 7.0, Baseline Tracking Dataset version 4.0, Follow-up 1 Comprehensive Dataset version 3.2, and Follow-up 1 Tracking Dataset version 2.3 under Application ID 2201014. The CLSA is led by Drs. Parminder Raina, Christina Wolfson and Susan Kirkland. The opinions expressed in this manuscript are the author’s own and do not reflect the views of the Canadian Longitudinal Study on Aging.
Consent to Participate
This study received ethical approval from the University of British Columbia Behavioural Research Ethics Board (H22-01358) on July 7, 2022. This was a secondary-analysis, all participant information was de-identified and participant consent was not required.
Author Contributions
Nicole Ketter and Brodie Sakakibara conceptualized the study, developed the research design and acquisitioned the data. Nicole Ketter analyzed the data and drafted the manuscript. All of the authors interpreted the data. Mary Jung and Suzanne Huot were involved in early stages of study and concept formation. Mary Jung, Suzanne Huot and Brodie Sakakibara revised the manuscript critically for important intellectual content. All the authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by The Canadian Institute for Health Research through the CGS-M program (to NK). Funding for the Canadian Longitudinal Study on Aging (CLSA) is provided by the Government of Canada through The Canadian Institutes of Health Research (CIHR) under grant reference: LSA 94473 and the Canada Foundation for Innovation, as well as the following provinces, Newfoundland, Nova Scotia, Quebec, Ontario, Manitoba, Alberta and British Columbia. Heart and Stroke Foundation of Canada National New Investigator Award (to BMS).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.