
Abstract
Objective
To identify environmental features of multi-family housing (MFH) and their surrounding neighborhoods that influence residents’ physical activity (PA).
Data Source
Articles published between January 2000 and September 2023 were identified from major social science, medical, health, behavioral science, and urban studies databases.
Study Inclusion and Exclusion Criteria
Studies were included if they (a) were empirical studies published in peer-reviewed journals and written in English; (b) focused on the MFH environment or the surrounding neighborhood; and (c) had at least one PA outcome.
Data Extraction
Data was extracted regarding the study objective, location, study sample, research design, results related to MFH and neighborhood environment, and limitations.
Data Synthesis
Descriptive summary of study characteristics and analysis to identify emerging themes at three spatial scales (i.e., building, site, and neighborhood).
Results
Findings from 35 identified articles revealed factors influencing MFH residents’ PA. On the building level, typology (apartment, townhouse) and tenure (public, market rent) showed contrasting correlations with PA in different age groups. On the site level, the presence of PA facilities and safe, walking-friendly environments promoted PA. On the neighborhood level, safety, quality of PA and pedestrian infrastructure, upkeep, air quality, aesthetics, neighborhood satisfaction, street connectivity, walkability, land use mix, density, and public transport promoted PA.
Conclusion
Study findings highlight the importance of the MFH environments in promoting PA, especially in older adults and young children. With increasing housing demand, understanding diverse MFH typologies and the impact of interventions on multi-spatial scales can help promote healthy and activity-friendly communities.
Objective
Lack of physical activity (PA) is a leading public health problem in many countries. In the U.S., 25% of adults do not engage in sufficient PA to maintain their health. 1 Globally, 81% of adolescents and 27.5% of adults fall short of the World Health Organization’s recommended PA levels. 2 This deficiency not only impacts individuals and their families throughout their lifespan but also places a significant burden on health services and society as a whole.
The general influence of housing and neighborhood environment on residents’ PA is well established.3-5 Notably, a previous systematic review 6 has highlighted the strong association between neighborhood environments and PA, urging for a closer examination of environmental factors within various residential settings. Factors such as pedestrian-friendly streets, access to green spaces and parks, availability and access to recreational facilities, proximity to public transit, higher residential density, and safety from crime and traffic are some of the environmental factors that promote peoples’ PA.4,7,8 Understanding these dynamics is essential for crafting evidence-based policies and interventions that foster healthier lifestyles and contribute to the overall well-being of communities. However, previous studies have focused more on single-family housing. In contrast, not enough studies have examined the environmental features of multi-family housing (MFH) and their surrounding neighborhoods.
Considering the increasing housing demand, MFH is a potentially equitable and sustainable solution for affordable housing.9-11 Approximately 24.75% of housing units in the U.S. are categorized as multi-family. 12 Furthermore, the global market for MFH construction has exhibited sustained expansion in recent periods, with robust growth projected for forthcoming years. 13 The examination of physical environmental factors in MFH and their influences on residents’ PA is a critical area of study with profound implications for public health, urban planning, and housing design. Hence, understanding the MFH environment and its impact on population health, including residents’ PA, is essential.
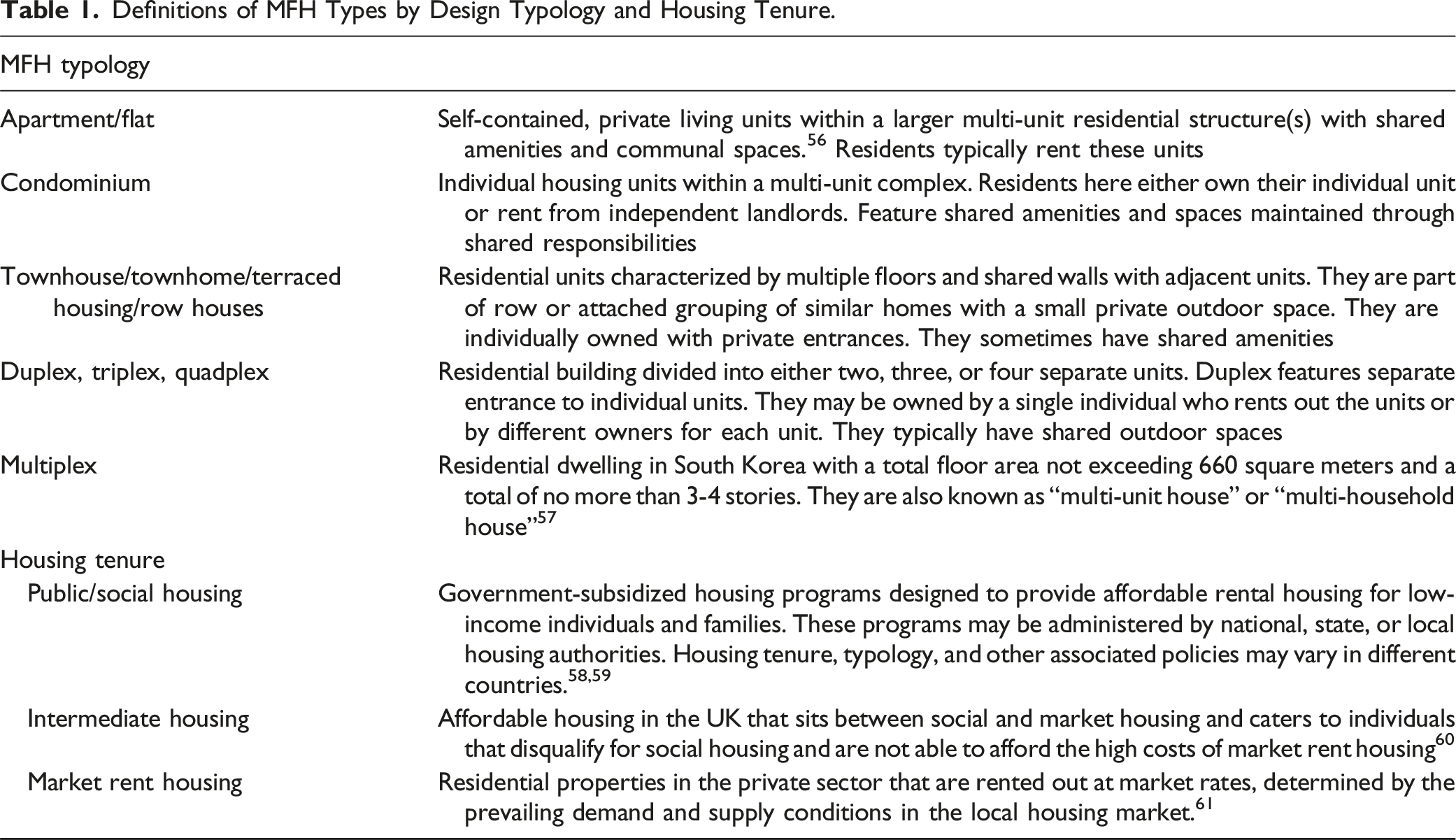
As in other building types, the design and layout of residential environments vary depending on the specific type of housing arrangement. MFH is typically significantly different from single-family housing in terms of design, density, space hierarchy, and the availability of spaces.14,15 Further variations also exist within MFH based on the typology. For example, townhomes and condominiums sometimes have a fenced-in yard, as compared to duplexes and fourplexes that have a shared yard, or apartments with outdoor spaces that are shared by more households. In general, MFHs have three spatial scales: (1) building level, which includes the individual units, the building that these units are located in, and sometimes a private yard; (2) site level, which includes the immediate outdoor surroundings that are within the property limits but shared with other residents; and (3) neighborhood level that is outside the property limits but within the neighborhood area.
The primary aim of this study is to systematically review previous studies that examined the impacts of MFH environments (built and natural) and their surrounding neighborhoods on residents’ PA. It explores (1) the correlations between housing and neighborhood environments of MFH and residents’ PA, and (2) the impacts of personal and social factors on MFH residents’ PA. At the end of the review, we discuss the importance of MFH environments and their crucial role in promoting health and healthy behaviors in its residents.
Methods
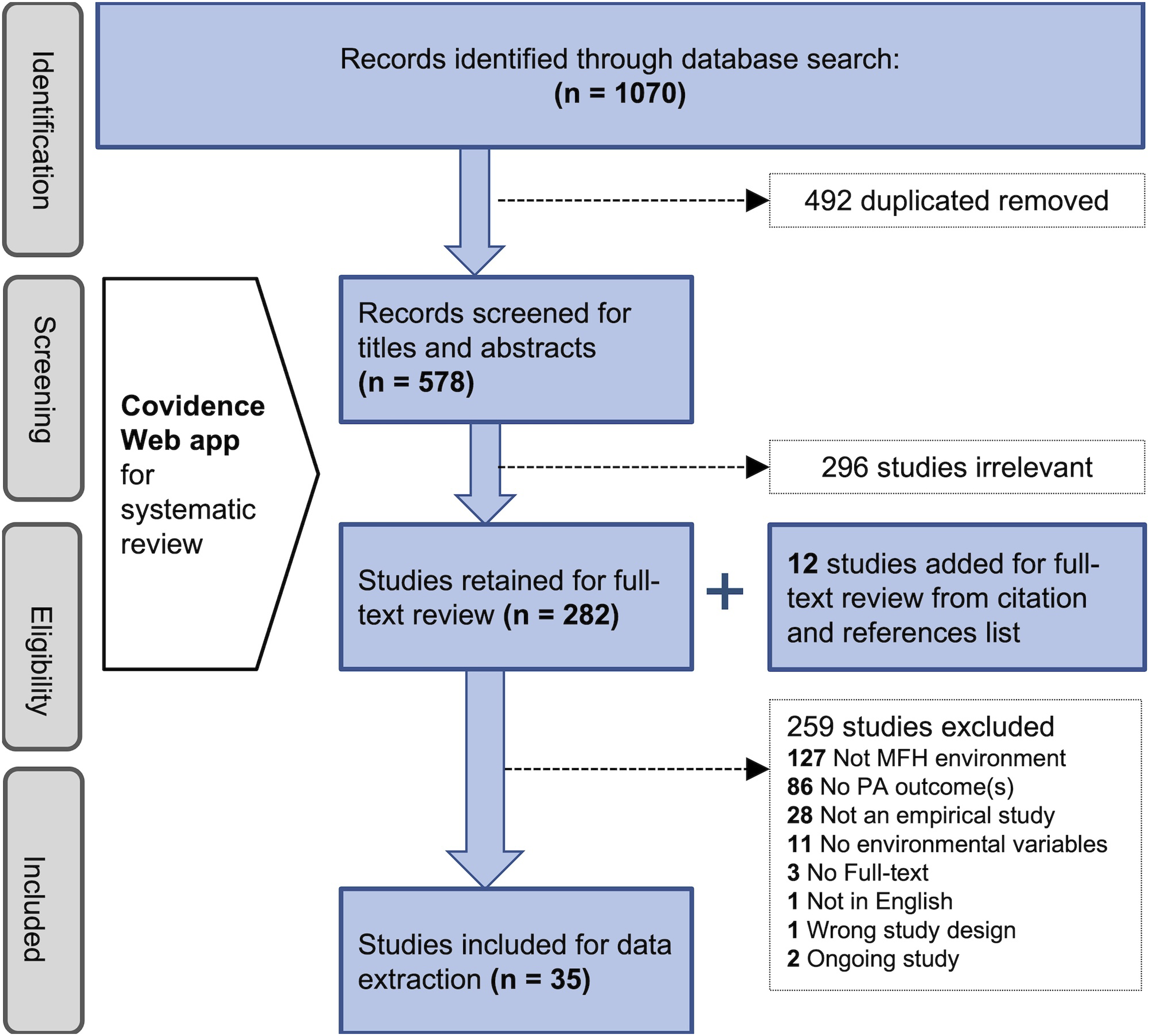
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, which outlined a four-phase flow diagram (Figure 1).
16
The search time frame ranged from January 2000 to September 2023. The year 2000 was selected because there was a push towards understanding the influence of the built environment on lifestyle PA, marked by programs such as the Healthy People 2000
17
by the CDC, and the establishment of the Active Living Research program
18
by Robert Wood Johnson Foundation. The search process concluded in September of 2023. PRISMA flow diagram showing the process of literature review.
16
The study team consisted of three researchers. Two lead researchers first reviewed three randomly selected articles to reach inter-rater agreements in their understanding of the screening criteria, study quality assessment tool, and data extraction process; a third researcher was involved to discuss and resolve conflicts in case of inconsistencies between the two reviewers. These two lead researchers also independently assessed the study quality of all identified articles using a standard quality assessment tool. More detailed data extraction for each article was conducted by one of the two lead researchers after they had reached inter-rater agreements.
Data Sources and Keywords
We searched for original studies that reported the impacts of MFH and its surrounding neighborhood environment on residents’ PA. Various keyword combinations were used to search online databases in the domains of (1) general health and PA - Web of Science, PubMED, Embase (OVID), CINAHL Ultimate, Academic Search Ultimate, Medline, Medline Ultimate; (2) health and PA in children - ERIC, Child Development and Adolescent Studies; (3) health and PA in older adults - AgeLine, Abstracts in Social Gerontology; (4) health and sports - Alt HealthWatch, SPORTDiscus; (5) healthy behavior - APA PsycInfo, Psychology and Behavioral Sciences Collection; and (6) environment and transportation - Environment Complete, Urban Studies Abstracts, Transport Research Information Services-TRIS. Studies with people of all ages were included. Search terms for MFH included “multi-family,” “apartment,” “flat,” “townhouse/townhome,” “terraced housing,” “condominium,” “duplex,” and “fourplex.” Keywords related to housing tenure included “public housing,” “social housing,” “cooperative housing,” and “affordable housing.” For environment, “neighborhood,” “built environment,” “natural environment,” “nature,” “greenery,” “green space,” or “outdoor space” were used. Finally for PA, “physical activity,” “MVPA,” “walking,” “biking,” “cycling,” “exercise,” “active living,” “sports,” or “physical fitness” were used. Literature review articles and citation and reference lists of the identified articles were also reviewed for additional relevant studies.
Inclusion and Exclusion Criteria
The screening process involved reviewing titles, abstracts, and full text using Covidence – a web-based application that supports a collaborative systematic literature review. 19 Studies were eligible for inclusion in the final data extraction if they were (1) published in peer-reviewed journals; (2) written in English; (3) empirical studies; (4) focused on populations living in MFH; (5) focused on the built/natural environmental factors of MFH or its surrounding neighborhood; and (6) had at least one PA outcome.
Data Extraction and Synthesis
Data were extracted from the identified articles using a template that included: (1) study title; (2) study objective(s); (3) research design (e.g., observational, natural experimental, pre-post intervention); (4) intervention details whenever applicable (e.g., type of intervention, duration, assessment time) (5) study location(s); (5) sample size and type; (6) study timeline; (7) data collection and analysis methods; (8) MFH (building and site) factors; (9) MFH type discussed in the study (e.g., apartment/flat, townhouse/townhome/terraced house, duplex, triplex, fourplex, condominium, row housing); (10) other MFH attributes(e.g., public housing, affordable housing, social housing, cooperative housing, commodity housing, intermediate housing [including affordable rent, shared ownership, and shared equity], market-rent housing); (11) neighborhood factors; (12) sociodemographic factors; (13) association between each independent/confounding variable and the dependent variable and their significance; and (14) conclusions and study limitations. The findings from the extracted studies were further reviewed and synthesized to provide summaries related to MFH and its neighborhood environment and their impact on residents’ PA. Three spatial scales, building, site, and neighborhood were used to organize the findings as each spatial scale provides distinctive opportunities in understanding the built environment and its impact on PA outcomes. A summary of key results is presented under each spatial scale to provide relevant details.
Study Quality Assessments
The Joanna Briggs Institute (JBI) Critical Appraisal Tool for cross-sectional studies 20 was used to assess the methodological quality of the study and determine the extent to which the study has addressed the possibility of bias in its design, implementation, and analysis. The appraisal checklist consists of seven questions regarding (1) well-defined inclusion criteria, (2) clear descriptions of study settings and samples, (3) outcome measure validity and reliability, (4) use of objective and standard measures of independent variables, (5) identifying confounding variables, (6) strategies used to deal with confounders, and (7) use of appropriate statistical analysis methods.
Results
The initial search yielded 1070 records, from which 578 were retained after excluding duplicates. After the screening process, 23 articles were identified for final data extraction. An additional 12 articles were added after reviewing reference lists of the retained studies, bringing the total number of studies ready for data extraction to 35 (Figure 1). We report findings from 35 studies about their study sample and design, study quality, PA-related outcome variables, MFH and neighborhood factors, any significant associations between the environmental and PA outcomes, and the sociodemographic confounders.
Study Design, Time, and Quality
Of the 35 studies, 83% (n = 30) used a cross-sectional study design. The remaining 17% included four natural experiment studies and one pre-post intervention design. In terms of years of publication (Figure 2), the distribution is consistent between 2006 and 2023 except for the 2018 – 2020 year range, which has the highest number (n = 11) of relevant studies. Number of reviewed studies by year of publication.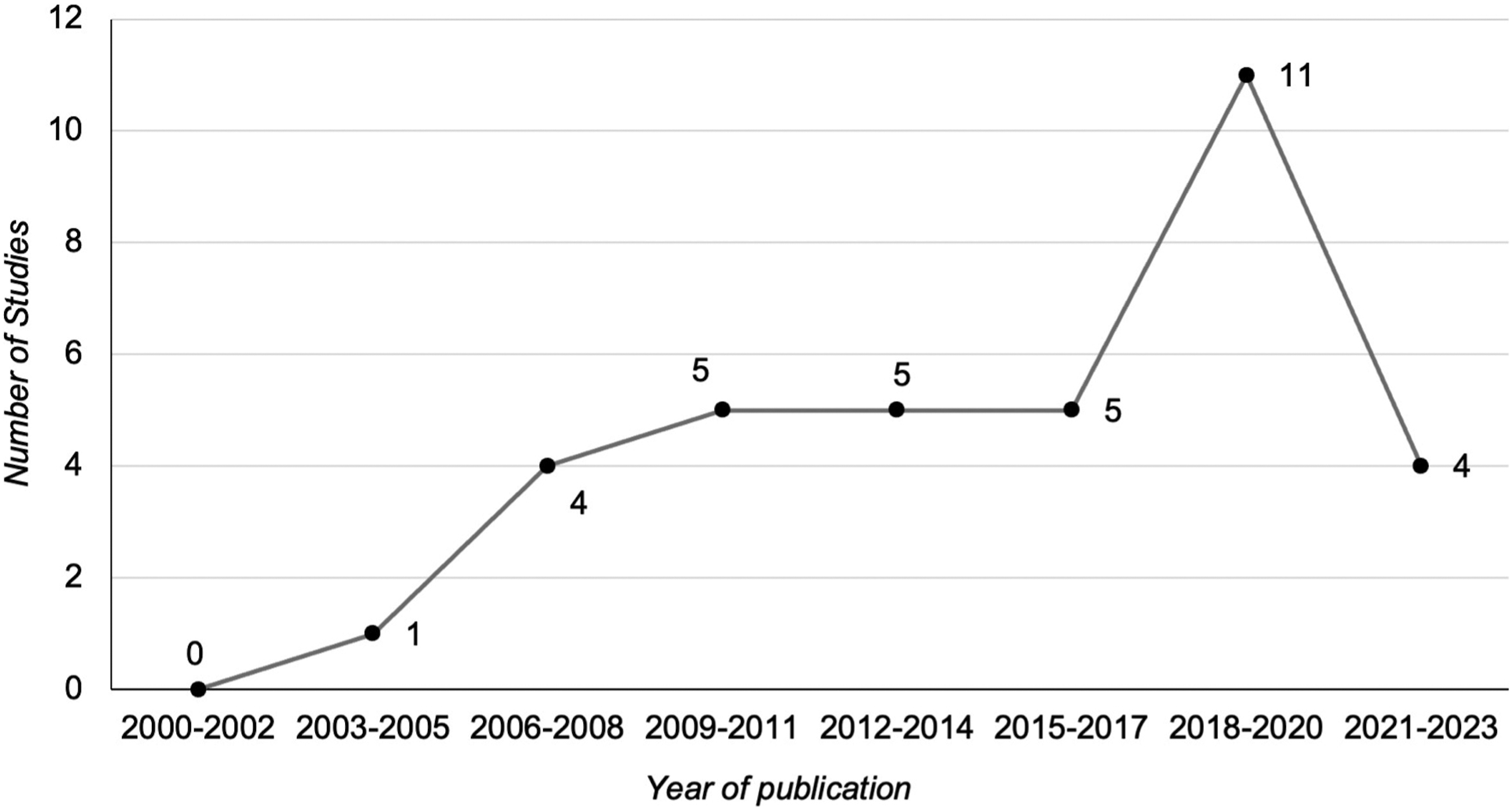
Study Setting and Sample
Studies identified were from across the world (Figure 3). The country with the highest number of studies (16 studies) is the U.S., followed by China (5 studies), Singapore (4 studies), UK (3 studies), and other countries. Number of studies included by study locations.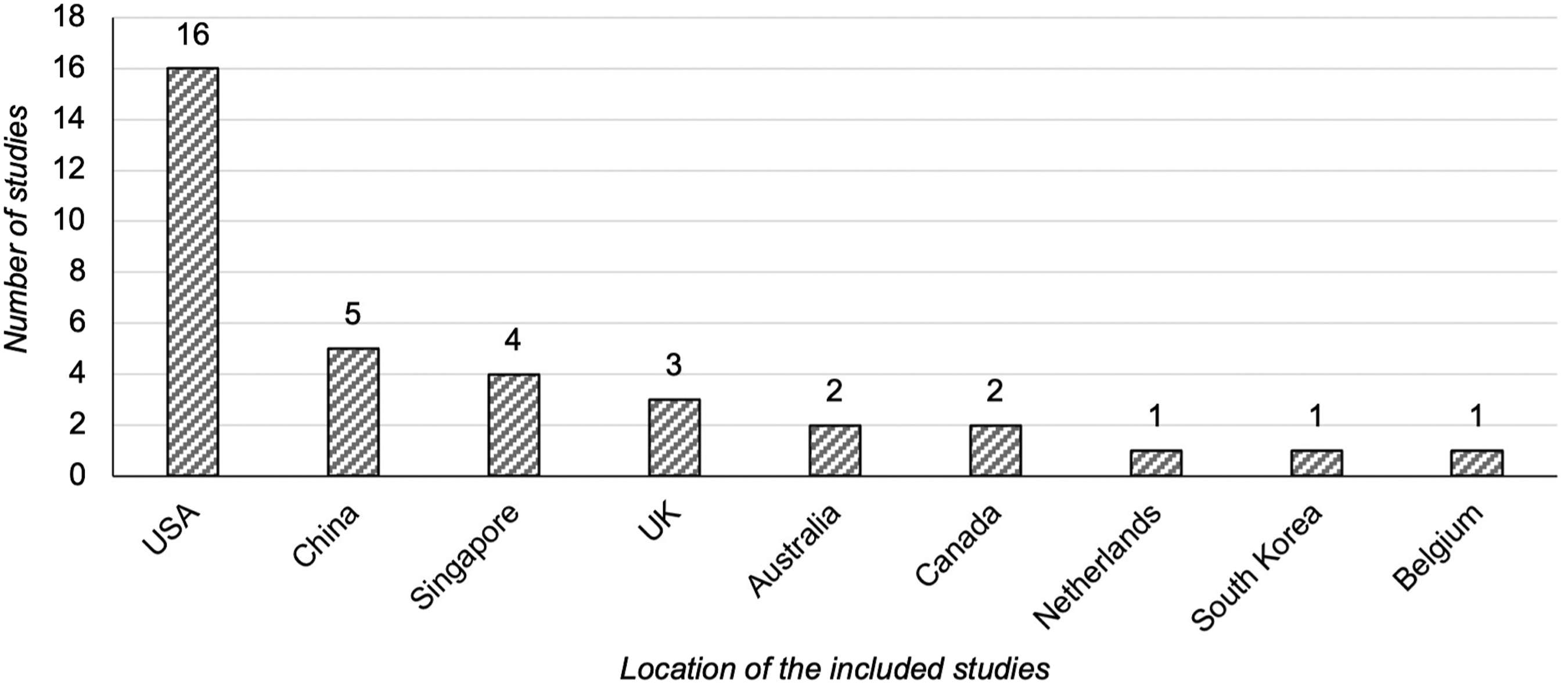
Study samples included individual residents such as older adults, adults, and children as well as others such as individual trips (Figure 4). Of the studies with individual resident participants, twenty studies included adults (average sample size = 1967, range = 11 to 26 767)21-40; twelve studies included older adults (average sample size = 1644, range = 26 to 13 468)41-52; and two studies included children (average sample size = 1122, range = 422 to 1822).53,54 Of the twelve studies with older adult participants, one study
46
also had a qualitative component that examined 820 photographs of the built environment. Additionally, one study used individual trips as the unit of analysis (sample size = 223,232).
55
Sample type and size by number of studies.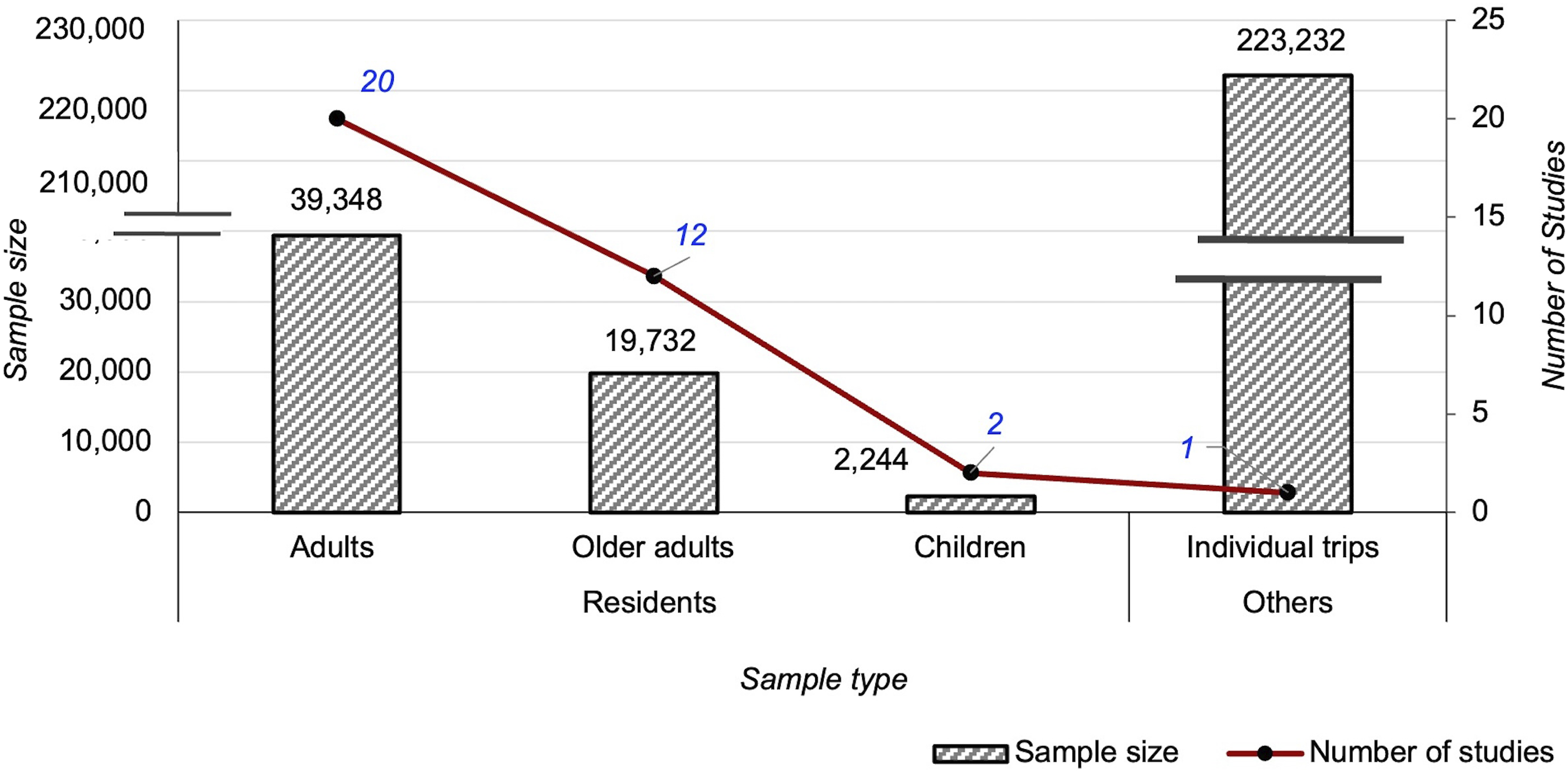
Outcome Measures
PA was measured objectively or through subjective self-report. Objective measures used included the Actigraph GT3X + accelerometer (n = 5)22,30,38,39,51 and pedometers (n = 2).21,28 Self-reported subjective measures included surveys (n = 24),21-53,55 interviews (n = 11),29,34,35,41,42,44-46,49,50,52 and focus groups (n = 3).37,43,49 Survey instruments included International Physical Activity Questionnaire (IPAQ) (n = 8),22,23,28,31,34,36,40,42 Global Physical Activity Questionnaire (GPAQ), 33 Recent Physical Activity Questionnaire (RPAQ), 33 7-day activity diary, 54 2-items about walking from the National Health Interview Survey, 24 PA measures from the Behavioral Risk Factor Surveillance System, 25 Transportation Tomorrow Survey, 55 Canada National Household Survey, 55 and the Hong Kong Travel Characteristics Survey.29,52
The PA outcomes examined can be classified based on purpose, PA type, and measure. In terms of the purpose of PA, one study looked at recreational PA, 53 seven studies examined transportation-related PA,22,25-27,44,52,55 two studies examined recreation- and transportation-related PA,40,42 one study examined work-, recreation-, and transportation-related PA, 33 while the other twenty-four studies examined PA for all purposes. Types of PA examined included walking22,24-42,44,48,50,52,55; biking26,27,33,55; outdoor play in children33,53; climbing stairs33,37; exercises such as yoga, aerobics, cardio, strength training, dance, and physical therapy37,43,48; and playing sports such as swimming, golf, shuffleboard, bowling, and others.34,46,48 Measures of PA varied based on the type. Walking was captured as mean steps per day,21,28,30,38,39 minutes per day of walking in a typical week,22,24,25,28,29,31,33,40,42,52 number of walking trips per week,26,27,52 odds and frequency of walking,29,38,44,52,55 and participation.41,48 Biking/cycling measures included the number and percentage of biking trips.26,27,33,55 Sports, outdoor play, and other forms of exercise were measured using participation,35,37,41,43,48 minutes per week of the reported activity,33,53 and weekly frequency. 47 Intensity of PA was measured using minutes of moderate and vigorous PA (MVPA),22-24,28,30,32,34,36,38,42,51,54 and percentage of residents meeting MVPA guidelines of at least 75 minutes per week of vigorous PA (VPA) or 150 minutes per week of moderate PA (MPA), or an equivalent combination.24,25 Finally, three studies measured total weekly minutes of PA,28,31,45 and one study examined the weekly frequency of MPA. 32
Sedentary behaviors (SB) were examined in four studies.33,34,36,39 Sitting was the primary SB, captured as the number of driving trips,26,27 minutes per week of sitting, 33 and daily sedentary minutes in a typical week. 39 Secondary outcomes impacted by PA were also measured such as body-mass index (BMI) (n = 3),30,33,36 fat mass percentage (n = 1), 39 obesity (n = 1), 32 waist-hip circumference ratio (WHR) change (n = 1), 33 and social interaction (n = 1). 50
Physical Environmental Factors as Independent Variables
The physical environmental factors examined in the reviewed studies are categorized into three spatial scales, including building, site, and neighborhood scales as defined previously. At the building level, factors related to MFH typology, tenure, and design were identified. At the site level, presence and maintenance of PA amenities were reported as significant correlates of PA. At the neighborhood level, factors related to safety, presence and quality of PA infrastructure, neighborhood upkeep and satisfaction, neighborhood aesthetics, street connectivity, walkability, land use mix, density, and public transport were identified.
Building Level Environmental Factors Influencing Residents’ PA
Definitions of MFH Types by Design Typology and Housing Tenure.
Relationship Between Building-Level Environmental Factors and PA.
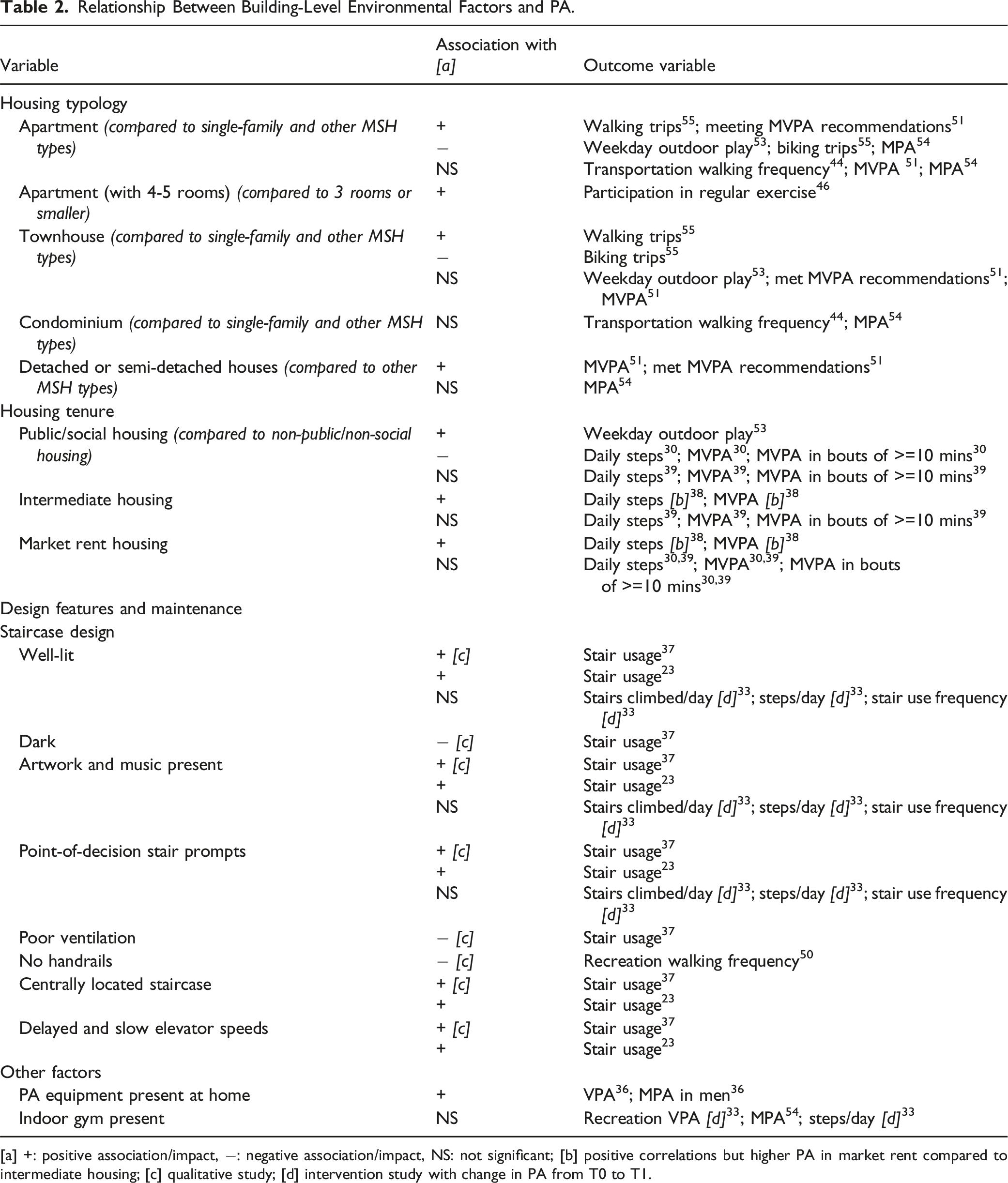
[a] +: positive association/impact, −: negative association/impact, NS: not significant; [b] positive correlations but higher PA in market rent compared to intermediate housing; [c] qualitative study; [d] intervention study with change in PA from T0 to T1.
Site Level Environmental Factors Influencing Residents’ PA
Relationship Between Site-Level Environmental Factors and PA.
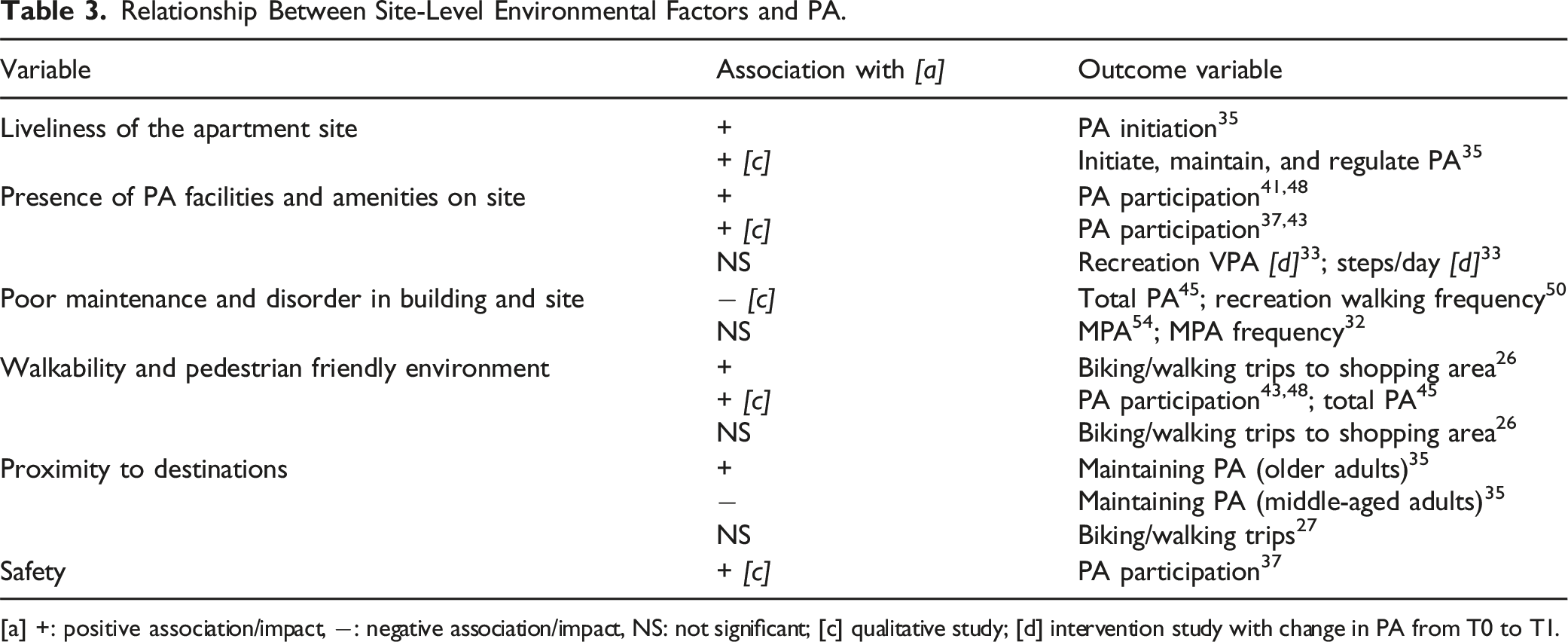
[a] +: positive association/impact, −: negative association/impact, NS: not significant; [c] qualitative study; [d] intervention study with change in PA from T0 to T1.
Neighborhood Level Environmental Factors Influencing Residents’ PA
Twenty-six studies21,22,24,28-32,34-36,38,40-44,46,47,49-55 focused on the neighborhood scale. Factors related to safety from crime and traffic, other traffic hazards, neighborhood amenities and characteristics, walkability, land use mix and density, neighborhood satisfaction, and others such as air quality and thermal comfort were examined. The correlations between these factors and the PA outcome varied significantly.
Night-time safety and overall neighborhood safety were associated with higher mean steps per day in women 21 and PA participation in older adults. 49 Traffic hazards and volume were negatively associated with PA participation 49 and weekly minutes of walking for transportation. 22 Higher speed limits, more number of lanes, and shorter crossing light duration resulted in lower PA participation, 43 and fewer weekly minutes of VPA, total PA, and walking. 28 Presence and perceived quality of PA amenities had mixed correlations. Perceptions of neighborhood quality, and presence of PA resources and pedestrian infrastructure was positively associated with participation in PA,41,46 daily steps, 30 and weekly minutes of MVPA.30,34 However, quality and presence of PA resources was negatively associated with weekly minutes of MVPA in men. 31 Incivilities such as litter and graffiti, poor upkeep and cleanliness were negatively associated with PA participation,49,50 and weekly minutes of walking. 24 Whereas physical disorder was positively associated with hours of weekday outdoor play in children. 53 Neighborhood aesthetics, presence of neighborhood greenery, and outdoor space (e.g. park) were positively associated with odds and minutes of walking,29,52 walking frequency for leisure and transportation,44,50 weekly minutes of MVPA,22,34 and PA participation.41,43,49,50 Neighborhood satisfaction was positively associated with weekly minutes of MPA. 36
Relationship Between Neighborhood-Level Environmental Factors and PA.
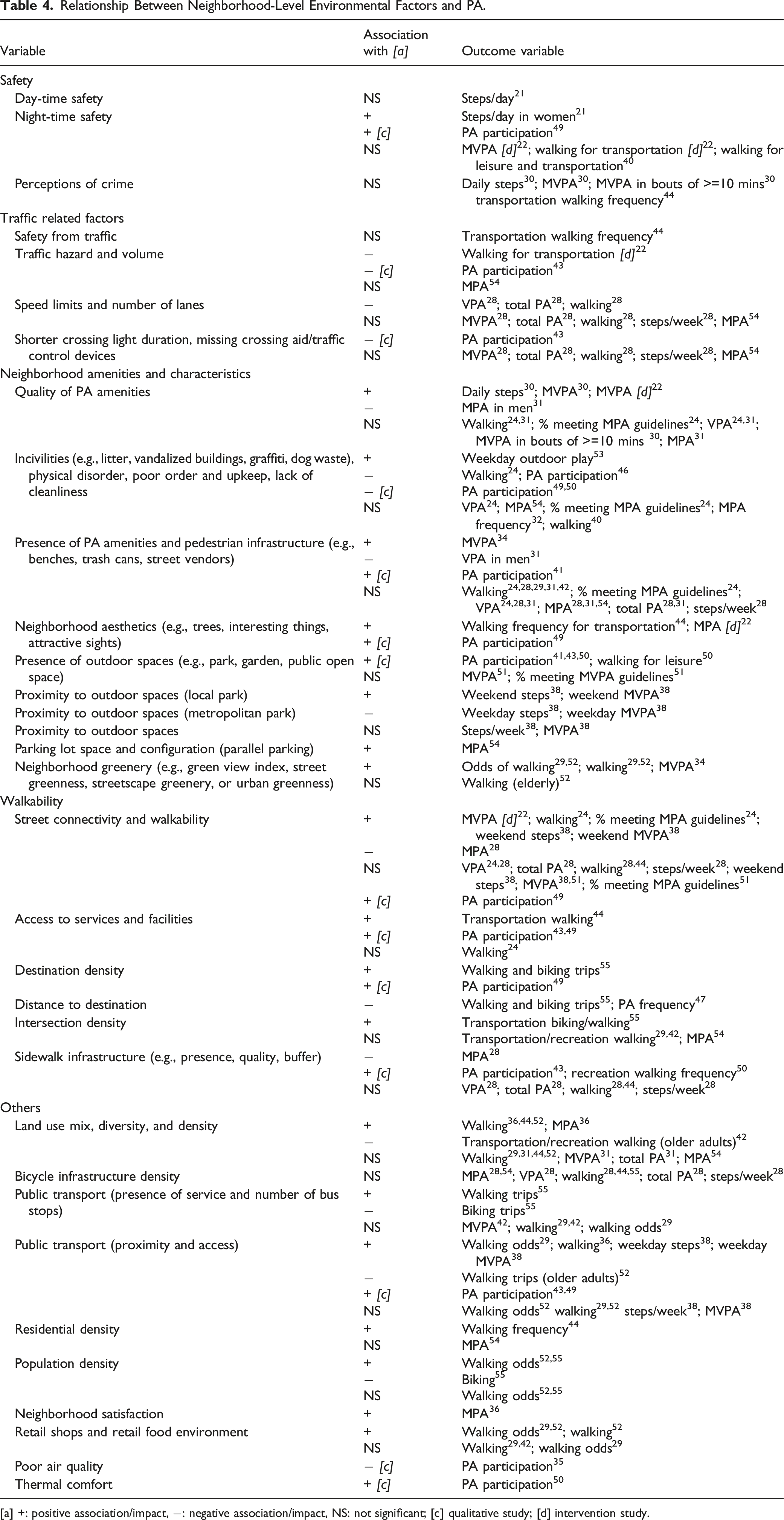
[a] +: positive association/impact, −: negative association/impact, NS: not significant; [c] qualitative study; [d] intervention study.
Sociodemographic Factors Influencing Residents’ PA
We also reviewed the confounding factors (see Supplemental Material) related to residents’ PA such as participants’ sociodemographic factors (e.g., age, sex, race and ethnicity, income, education); employment status; occupation type; physical, mental, and social health variables; household structure type and size; and travel behaviors. As expected, age, sex, race and ethnicity, education, income, and employment status had significant impacts on the PA outcome.
Age and sex had mixed associations with the outcome depending on the type of PA. Older residents had lower levels of MVPA and initiating PA but higher daily steps and walking for recreation and transportation.29,30,55 Additionally, higher BMI, and poor health were negatively associated with participation in PA, daily steps, and MVPA.22,35,36,46,51 On the contrary, one of the studies found that having multiple ailments was positively associated with PA regulation. 35 Similarly, being on regular medical checkup was positively associated with PA participation. 46 Black and Asian adult residents had negative correlations with daily minutes of MVPA and daily steps 30 whereas White residents showed positive correlations with walking and biking. 26 Subsequently, Hispanic and Asian children had fewer hours of weekday outdoor play. 53 Being unemployed, employed part-time, or employed in manufacturing, clerical, or retail jobs was negatively associated with walking and biking. 55 Education showed contrasting correlations36,44 with walking and a positive correlation with total PA. 47 A study 55 noted that trips from home to school positively correlated with biking and walking whereas trips to other destinations and non-home-based trips negatively correlated with biking and walking. Other personal factors such as poor mental health, and social isolation were negatively associated with frequency of walking, 25 change in PA,22,47 and participation in PA. 46
Conclusion
Key Findings and Implications
This systematic review examined the importance of multi-scale physical environments of MFH, including building-, site-, and neighborhood-scale features, illustrating how they promote or inhibit residents’ PA, with an overarching goal of promoting health and healthy behaviors. While the influence of neighborhood environments on health is well studied, the housing environment (i.e., building- and site-scale features) is understudied. In this literature review, we address important knowledge gaps as revealed by previous reviews.62-64 Two reviews focused on architecture interventions that promote PA by summarizing results from forty 64 and eighty-eight 62 articles respectively. However, design, prompts, and usage of stairs and presence of PA equipment, were the only factors examined at the housing level. Similarly, another 2021 review 63 examined the aspects of housing environments, such as housing design, type, condition, and location on residents’ physical and mental health. While the study investigates the impact of apartment-type housing on residents’ social interaction and physical and mental well-being, the overall discussion is mostly focused on detached housing. Despite these examinations, the literature highlights the significant gaps in the research, particularly MFH building and site level features, which the current review attempts to address.
This study identified factors related to MFH and its surrounding environment and their impact on residents’ PA. Living in apartments and townhomes instead of condominiums, and single-family homes had a statistically significant positive correlation with walking and taking public transit for transportation. However, a negative correlation was observed with bicycle usage as a transportation choice. This could be location specific or due to the availability of bike infrastructure, all of which needs further investigation. The review also notes that MFH factors related to housing conditions and maintenance significantly influenced residents’ PA. A lively atmosphere in the apartment site positively impacted the initiation of PA, whereas inadequate maintenance and disorderliness in the building and site had a negative effect on both the engagement and level of PA participation. Finally, like previous reviews,62,64 we found that staircase location, design, and PA promoting prompts positively influenced stair usage and MPA.
This review also included studies with populations of all age groups. We found that apartments were negatively associated with outdoor play in children, but public housing showed a positive correlation. A more in-depth understanding of children’s recreational PA, the micro-scale physical and social environment, and the housing typologies of public housing may provide a clearer picture. One study 31 observed a negative correlation between presence and quality of PA resources and MVPA in men which could be because men in this neighborhood performed MVPA outside their neighborhood. Similarly, another study 28 observed a negative correlation between sidewalk connectivity and men’s MPA which could be because of perceived safety issues such as high crime rate and traffic. Studies with older adults suggest that providing pedestrian-friendly environments with more recreational facilities that are onsite or within shorter walking distance, public transit stops, safety from traffic and crime, socially interactive environment, and better health status positively impacted their overall PA. However, one study found a negative correlation between land use mix and recreational and transportation walking in older adults which could be because of the much higher land use mix and diversity in Hong Kong compared to other countries. 42
The limitations of this review are largely related to the limited number of studies examining MFH environment, insufficiently explored site and building level environment, choice of metrics, and study design. Only twenty-three studies examined MFH environment, with contrasting correlations with PA outcomes. Additionally, housing typologies and the variations within site level outdoor areas are not sufficiently explored. Further studies that examine diverse site level outdoor areas and the PA amenities within are needed to better understand the interactions between the environment and residents’ PA. Variations in correlations with PA were observed depending on the population type and study location. Since local policy guidelines highly influence the design and structure of MFH and its neighborhood, conducting studies with a targeted focus can provide a comprehensive understanding of its impact on PA. Only seven studies used objective measures of PA which is considered more robust and reliable. While using these types of PA measures are not feasible in larger samples, studies that examine PA using the Actigraph GT3X + accelerometer, and pedometers can provide accurate understanding of the impacts of multi-spatial environments on residents’ PA. Finally, 87% of the studies (n = 30) included are cross-sectional and hence the causal relationships are unclear. Adopting longitudinal and intervention study designs can provide more robust understanding of this topic.
Conclusion and Suggestions for Future Research and Practice
MFH and its immediate surrounding environment have crucial influences on its residents’ health and healthy behaviors. This is especially true in low-income and vulnerable communities with limited access to paid subscriptions and dependence on the building and site level environments. Hence, it is necessary to understand the varying typologies of MFH and how the design of multi-scale environments can promote or inhibit residents’ PA. For future research, more intervention studies, focus groups, and interview-style studies are needed for an improved understanding of these environments. Design strategies such as incorporating smaller green spaces with well-lit walking paths, outdoor fitness zones with exercise equipment, interactive public art and installations, resident-maintained community gardens, seating and shade, and health promoting signages or prompts can encourage residents to participate in healthy behaviors. Policy recommendations such as incentivizing active design through tax incentives for developers and partnering with local fitness programs or trainers to provide on-site fitness classes are helpful. Implementing zoning regulations that promote mixed-use development, establishing inclusive design standards to create an environment that is safe for all ages and abilities, and collaborating with local schools to establish safe walking and biking routes for children have shown to promote healthy behaviors. Finally, implementing education programs to raise awareness about the importance of PA and the available facilities within the community can promote a healthier and more vibrant community. Neighborhood environment has a significant influence on residents’ health and healthy behaviors. But the roles of MFH and their surrounding neighborhoods have been understudied although MFH residents, especially those in low-income housing, are more likely to depend on the housing environments to stay active. This review explored the correlations between housing and neighborhood environments of MFH and residents’ PA, and the impacts of the underlying sociodemographic factors. We identify the gaps and need for further research in understanding building, site, and neighborhood level environments of MFH and their influence on residents’ healthy behaviors. The review also identifies the need for studies with objective measures of PA and more intervention, focus groups, and interview study designs. MFH and its immediate surrounding environment is a very crucial environment that highly influences its residents’ health and healthy behaviors. This is especially true in low-income and vulnerable communities with limited access to paid subscriptions and dependence on the building and site level environments, highlighting the importance of understanding the varying typologies of MFH and how the design of multi-scale environments can promote or inhibit residents’ PA.So What? Implication for Health Promotion Practitioners and Researchers
What is already known?
What does this article add?
What are the implications for health promotion practice or research?
Supplemental Material
Supplemental Material - Multi-Family Housing Environment and Physical Activity: A Systematic Review of the Literature
Supplemental Material for Multi-Family Housing Environment and Physical Activity: A Systematic Review of the Literature by Manasa Vigneshwar Hegde, Seokyung Park, Xuemei Zhu, and Chanam Lee in American Journal of Health Promotion.
Footnotes
Author Contributions
Manasa Vigneshwar Hegde: Conceptualized the systematic review, led the data search, extraction, and quality assessment, interpreted results, drafted, revised, and finalized the submitted manuscript. Seokyung Park: Contributed to data search, extraction, and quality assessment, and revised each manuscript draft crucially. Xuemei Zhu: Contributed to study conceptualization, data search, revised each manuscript draft crucially, and approved the final submission. Chanam Lee: Contributed to study conceptualization and revised the manuscript draft crucially.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.