
Abstract
Purpose
Food insecurity has far-reaching consequences for health and well-being, especially during pregnancy and postpartum periods. This study examines a food-is-medicine approach that aimed to reduce food insecurity, maternal stress, depression, anxiety, preterm labor, and low birthweight.
Design
Pre-post interventional study of FreshRx: Nourishing Healthy Starts, a pregnancy focused food-is-medicine program led by a local hunger relief organization and obstetrics department.
Setting
St. Louis, Missouri, a Midwestern U.S. city with higher-than-average infant mortality, low birthweight, and preterm birth rates.
Sample
Participants (N = 125) recruited from a local obstetrics clinic had pregnancies earlier than 24 weeks gestation; spoke English; and were enrolled in Medicaid. At baseline, 67.0% reported very low food security and none reported high food security, while 34.7% indicated depressive symptoms.
Intervention
FreshRx included weekly deliveries of fresh food meal kits, nutrition counseling and education, care coordination, and supportive services.
Measures
18-Question U.S. Household Food Security Survey, Edinburgh Postnatal Depression Scale, birthweight, gestational age.
Analysis
Single arm pre-post analysis.
Results
Average gestational age of 38.2 weeks (n = 84) and birthweight of 6.7 pounds (n = 81) were higher than rates for the general population in the area. For study participants who completed a sixty-day post-partum assessment, 13% (n = 45) indicated maternal depression (P < .01).
Conclusion
Food-is-medicine interventions may be an efficient, effective, and equitable tool for improving birth and maternal health outcomes.
Purpose
Food insecurity is “a household-level economic and social condition of limited or uncertain access to adequate food” 1 with wide-ranging consequences such as increased adverse health outcomes and healthcare costs. 2 During pregnancy, food insecurity can increase maternal stress, depression, and anxiety3,4 as well as preterm labor and low birthweights. 5 Notably, the U.S. ranks last against peer countries in low-birthweight and pre-term deliveries, 6 while Black and Hispanic families in the U.S. experience increased risk of food insecurity,5,7 less access to prenatal care, lower birthweight infants, and higher infant mortality. 8 Research also indicates that increased nutrition reduces adverse birth outcomes and chronic disease risk later in life, 9 making food security particularly critical during pregnancy. While households with lower income levels may qualify for Federal Nutrition Assistance Program support, food insecurity persists for pregnant individuals with recent studies suggesting rates ranging from comparable to the general population (12.8%) to as high as 69% within certain groups.10,11 This research brief presents results from an innovative food-is-medicine intervention that integrated fresh food provision and counseling during pregnancy alongside traditional medical treatment within a local healthcare system.
Methods
Design
FreshRx: Nourishing Healthy Starts (FreshRx NHS) is a food-is-medicine delivery program developed by Operation Food Search, a hunger relief organization in St. Louis, Missouri. FreshRx NHS addresses the cyclical relationship between food insecurity and chronic disease—in which chronic disease incidence can increase food insecurity and food insecurity can increase risks of chronic disease 12 —by providing nutrition support during pregnancy. Program staff formed and facilitated a participant advisory council that met monthly to advise on program design, guided food options, and reviewed study materials and assessment tools. The study was approved by the Washington University in St. Louis Institutional Review Board.
A baseline and sixty-day post-partum assessment collected sociodemographic and health information; household food insecurity; maternal mental health; participation in Federal Nutrition Assistance Programs; and other home cooking and nutritional information. Participants received a $25 gift card for completing each program assessment.
Sample
Staff at a local obstetrics care center that provides services regardless of an individual’s ability to pay screened for program eligibility during routine prenatal care visits using the validated Hunger Vital Sign™ two-item screening assessment. 13 Eligible participants needed to be pregnant; earlier than 24 weeks gestation; receiving care throughout pregnancy; English speaking; older than 14 years of age, and a Missouri resident enrolled in one of three state Medicaid Plans. Additionally, eligible participants resided in a pre-determined area with proximity to a central location to facilitate food deliveries and pickups. Overall, 125 participants enrolled in the FreshRx NHS program between September 2018 and July 2021.
Measures
While baseline food insecurity and maternal depressive symptoms were collected for all enrolled participants (N = 125), data collection including the completion of validated measures post-intervention varied. This included the 18-question USDA Household Food Security Survey Module (n = 21), 14 which measured food insecurity, and the Edinburgh Postnatal Depression Scale (EPDS) (n = 45), which assessed for maternal depressive indicators.15,16 Birthweight (n = 81), gestational age (n = 84), and NICU days (n = 33) were collected via Electronic Health Records.
Intervention
Cognizant of common food prescription program barriers around transportation and nutrition literacy, 17 FreshRx NHS provided fresh food, cooking and nutrition supports, counseling, and increased case management during pregnancy through 6 weeks post-partum. Following review of informed consent, baseline assessment, and program orientation, participants received weekly meal kits to prepare three meals for their household focused on fresh, seasonal, and locally available foods. Participants who missed a delivery could request an additional drop off or opt to receive the following week as scheduled. Participants received meal preparation essentials such as cooking oil and other pantry staples, and program staff provided mental health services, cooking and nutrition education, and connected participants with resources to navigate cooking barriers such as malfunctioning appliances, disconnected utilities, and pest mitigation. Appendix A includes additional detail about the intervention and program design.
Analysis
For describing sample characteristics, we include all 125 participants regardless of attrition or missing data. Outcome variable sample size varies as our single arm pre-post results only include those for whom we have data for each outcome measure. We additionally obtained local birthweight and gestational age rates through the Missouri Department of Health and the Missouri Information for Community Assessment (MICA) system.
Results
We found decreased maternal depression and lower rates of pre-term and low birthweight infants. Participant demographics reflect the geographic area in which the program focused. 43.9% of participants were 16-24 years old, 46.3% were 25-34, and 9.8% were 35-44. Most participants identified as Black (77.4%) and 16.9% identified as White. At baseline, participants had high rates of very low (67.0%) and low (27.8%) household food security, with less observed marginal food security (5.2%) and no participants indicating high food security (n = 115).
To examine participant birth outcomes, we used publicly available data for St. Louis Medicaid recipients. We defined low birthweight as having a baby below 2500 grams (5.51 pounds) and pre-term births as earlier than 37 weeks as described by the World Health Organization and U.S. Centers for Disease Control and Prevention. Study participant gestational age at birth (mean = 38.2, median = 38.6, n = 84) and average birth weight (mean = 6.7, median = 6.7, n = 81) are considered normal or comparable to national rates in the U.S. (Figure 1). Compared to St. Louis citywide rates obtained from the Missouri Information for Community Assessment (MICA) system, program participant pre-term birth rate (12.0%) and low birthweight rate (9.9%) are lower than St. Louis city overall rates of 12.3% preterm and 13.0% low birthweight. Even of the participant pre-term births, the median gestational age was 36.3 weeks, and only five births required intensive care or time spent in the NICU. Notably, while overall rates are lower, Black mothers in the program still experienced a higher percent of low birthweight and pre-term births. Birthweight and gestational age at birth.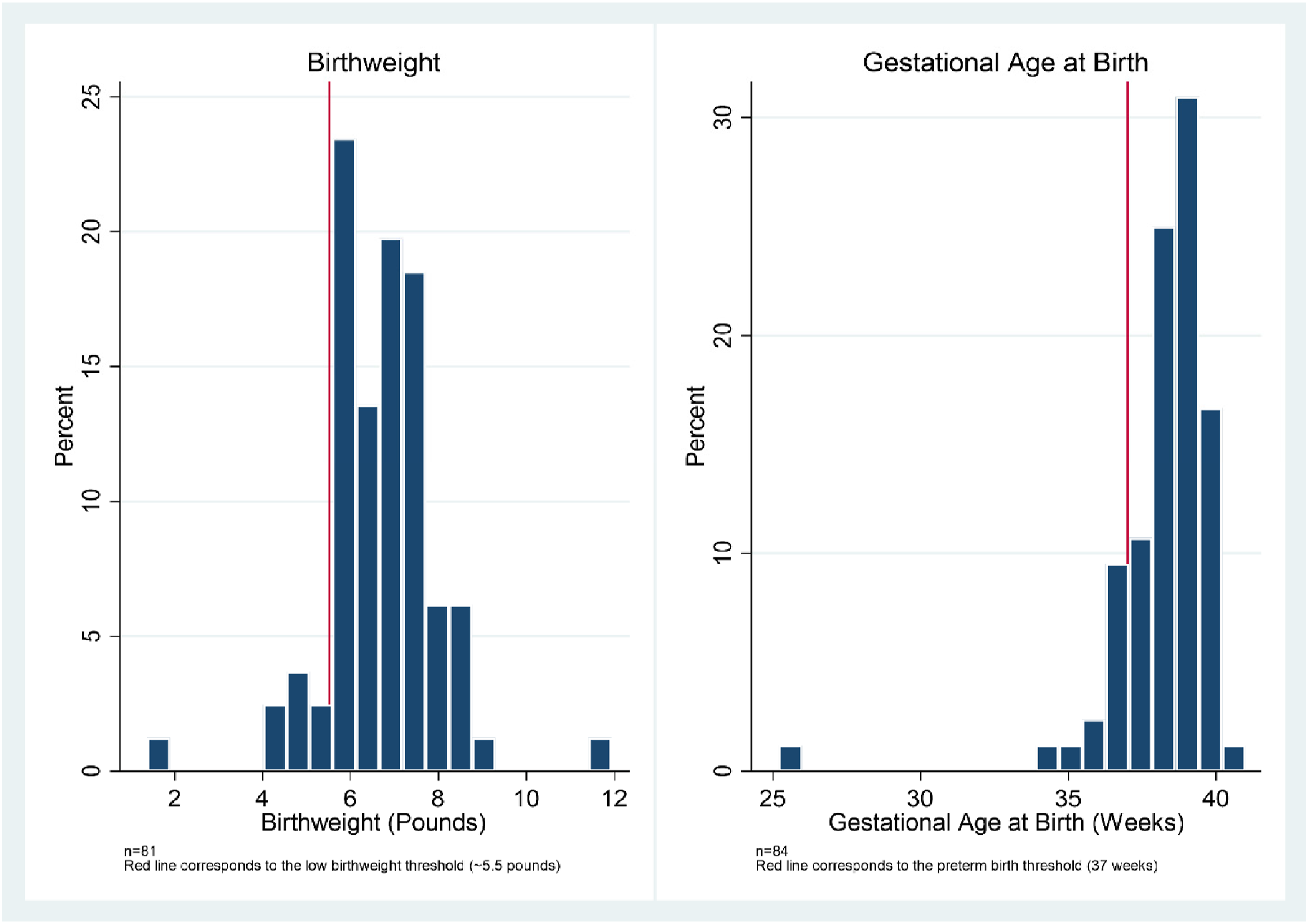
At baseline, 34.7% of participants (n = 121) demonstrated clinically significant depressive symptoms. Comparing participants for whom both pre and post-test data are available (n = 45), we observe a statistically significant (P < .01) decrease in depressive symptoms as 13.3% of participants 60 days post-partum had clinically significant depressive symptoms (Figure 2). Tables B1 and B2 in the Appendix summarize the study outcomes and provide additional detail on study participant characteristics. Maternal depressive symptoms for participants completing pre- and post-program assessments.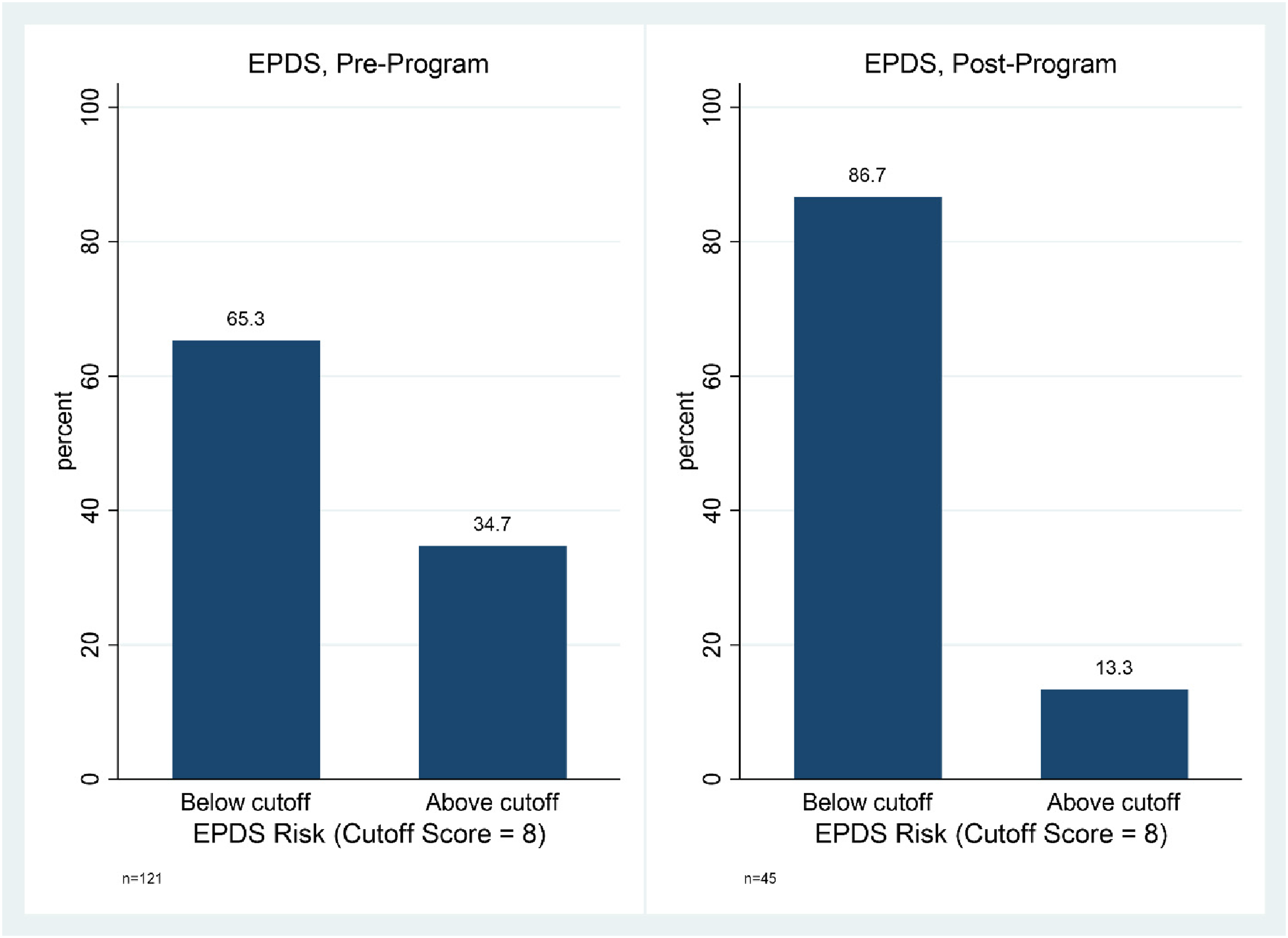
Discussion
Summary
Food insecurity persists despite an array of public nutrition assistance programs and community-based interventions. FreshRx NHS was the first program during pregnancy and post-partum periods to incorporate fresh food deliveries, counseling and mental health supports, and cooking and nutrition education. Participants experienced less depressive symptoms and fewer low birthweight and pre-term births compared to local rates, while previous food-is-medicine research has shown mixed results. One cluster randomized control trial of a food box delivery program found decreased household expenditures on food, however no sustained reduction of food insecurity. 18 A WIC-based fruit and vegetable voucher program during pregnancy was found to increase food security and lower the odds of preterm birth, 19 and a medically tailored meal program for adults with serious medical conditions lowered participant food insecurity and improved mental health. 20 Early results from other programs, such as the Geisinger Fresh Food Farmacy focused on individuals with type 2 diabetes, estimates per-year-per-participant medical savings of $16,000 - $24,000. 21
Limitations
The FreshRx NHS study design and sample size did not allow for measuring isolated program components. Loss to follow-up also limited our analysis and findings for the program’s effect on food insecurity, and the lack of a control group limits our ability to make any causal claims. Furthermore, participants who opted into the program during pregnancy may not reflect those who opted out. Undoubtedly, the COVID-19 pandemic affected FreshRx NHS participant experience, study attrition, and data collection. However, among those who completed both baseline and post-partum assessments, observed study outcomes showed considerable improvement.
Significance
Improvements in maternal mental health and birth outcomes present immediate considerations for policymakers, practitioners, and researchers. While prevention accounts for a small share of U.S. healthcare spending, health insurance plans have incentive to increase access to effective services not traditionally considered Medicaid billable. Government investment has grown as the National Institutes of Health recently included food-is-medicine as part of its first strategic plan for nutrition research and USDA has directed $69 million for food prescription programs. Wider improvement of maternal and birth outcomes would generate significant immediate and long-term cost savings alongside meaningful improvements in perinatal and birth outcomes. Cross-sector partnerships in food-is-medicine interventions, especially during pregnancy, are ripe for replication and expansion while being cognizant of the FreshRx NHS experience with study attrition and limitations. The loss to follow-up for participants for food insecurity assessment suggests future consideration for using the recently validated eight-question Abbreviated Child and Adult Food Security Scale.
22
Food insecurity is associated with numerous adverse outcomes during the critical developmental period of pregnancy. Interventions such as medically tailored meals, fruit and vegetable vouchers, and food delivery programs have demonstrated mixed results across a number of target populations and outcomes of interest. FreshRx NHS is distinct in its target population, comprehensive program model, and participant improvements in maternal mental health and birth outcomes. The program design also directly addresses research-identified barriers to successful food prescription programs such as transportation and nutrition literacy. Programs such as FreshRx NHS have the potential to improve outcomes for mother and child and drastically reduce healthcare expenditures through the supported provision of a holistic, comprehensive food-is-medicine program. Scaling up FreshRx NHS and similar programs for greater impact will require cross-sector collaboration across levels of direct practice, policy, and research.“So What?” Implications for Health Promotion Practitioners and Researchers
What is Already Known on This Topic?
What Does This Article Add?
What Are the Implications for Health Promotion Practice or Research?
Footnotes
Acknowledgements
The authors would like to acknowledge colleagues and collaborators who have offered significant support, feedback, and contributions to the FreshRx program and associated research: Dr. Carolyn Pryor, Brittney Stone, Brittany Rudy, Lyndsey Cavender, Jennie Oberkrom, Genevieve Davis, Yueh-Ya Hsu, Adam Pearson, Sydney Rothman, & Jennifer Potts.
Authors’ Contribution
All authors have contributed significantly and agree with the content of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research of the Fresh Rx: Nourishing Healthy Starts program is made possible by funding support from Operation Food Search donors.
Ethical Statement
Detailed Program Overview
Supplemental Results
In this section of the Appendix, we present two tables to provide additional detail on the study results. Table B1 outlines an array of key participant demographics at baseline, as well as their participation rates in WIC and SNAP, their baseline food insecurity and EPDS indicators, and their birth outcomes, including birthweight and gestational age at birth. Table B2 summarizes the changes in food insecurity and EPDS scores that we discuss in the main analysis.
Selected Study Indicators. Note: Observations differ by indicator due to missing data for some participants.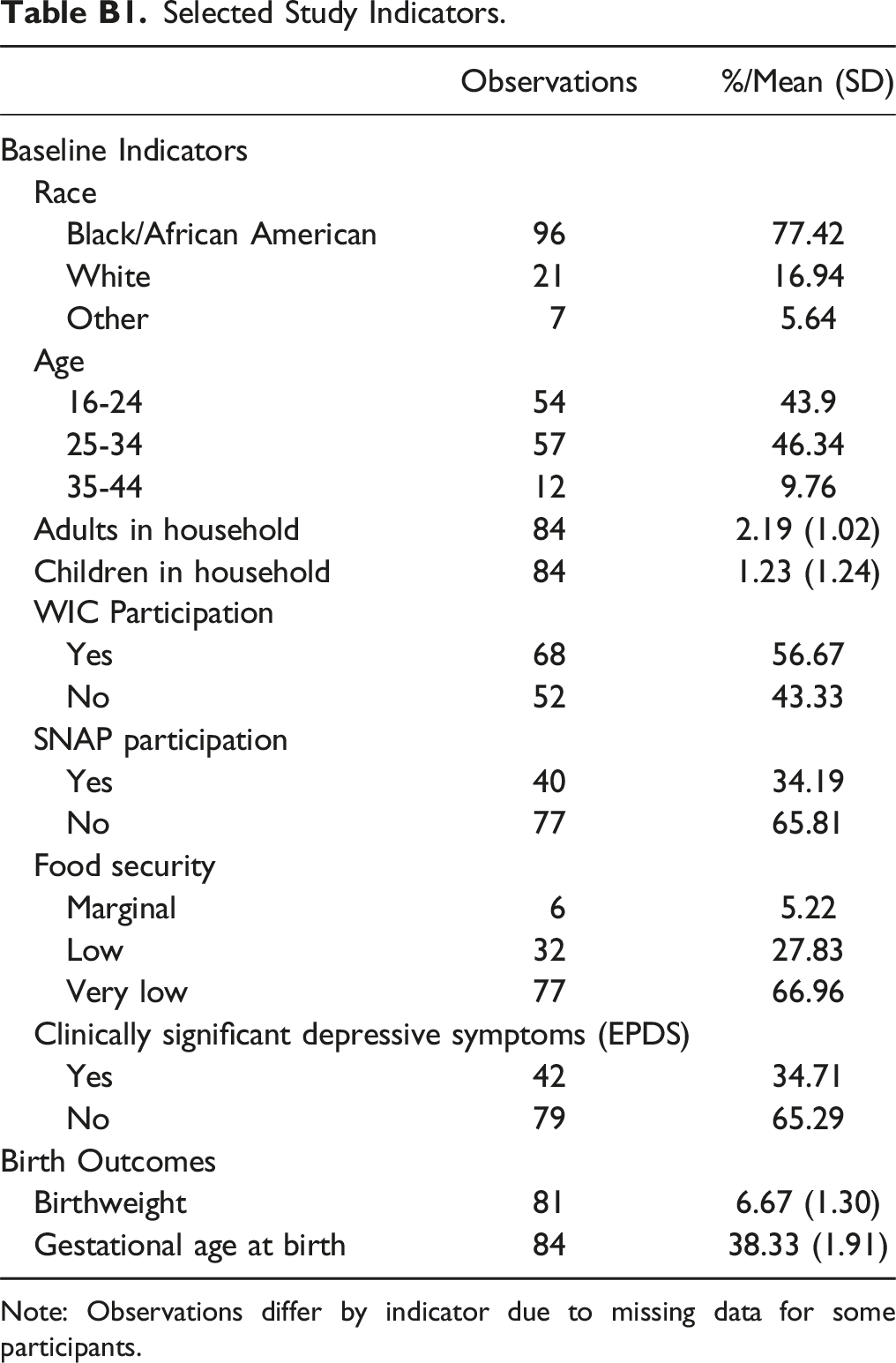
Observations
%/Mean (SD)
Baseline Indicators
Race
Black/African American
96
77.42
White
21
16.94
Other
7
5.64
Age
16-24
54
43.9
25-34
57
46.34
35-44
12
9.76
Adults in household
84
2.19 (1.02)
Children in household
84
1.23 (1.24)
WIC Participation
Yes
68
56.67
No
52
43.33
SNAP participation
Yes
40
34.19
No
77
65.81
Food security
Marginal
6
5.22
Low
32
27.83
Very low
77
66.96
Clinically significant depressive symptoms (EPDS)
Yes
42
34.71
No
79
65.29
Birth Outcomes
Birthweight
81
6.67 (1.30)
Gestational age at birth
84
38.33 (1.91)
Pre- and Post-program Outcome Summary. Note: These results only include study participants for whom there were both pre- and post-program data available. Observations differ by indicator due to missing data for some participants.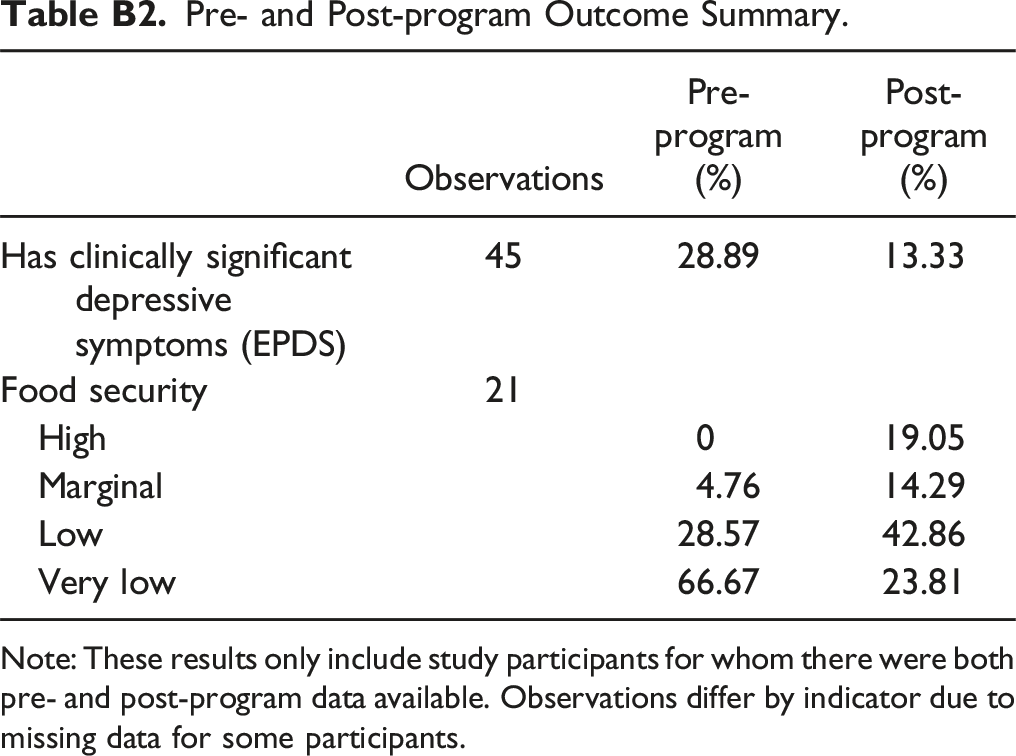
Observations
Pre-program (%)
Post-program (%)
Has clinically significant depressive symptoms (EPDS)
45
28.89
13.33
Food security
21
High
0
19.05
Marginal
4.76
14.29
Low
28.57
42.86
Very low
66.67
23.81