
Abstract
Purpose
The current study investigates associations between mHealth apps and healthcare decision-making and health communication among informal caregivers in the US.
Design
Cross-sectional study employing secondary data.
Setting
The Health Information National Trends Survey (HINTS5, Cycles 2 through 4, 2018 – 2020).
Sample
Self-identified informal caregivers (n = 1386; had mHealth apps = 61.3%, female = 63.2%, some college or more in education = 80.3%) who reported owning at least a smartphone or a tablet computer (i.e., ownership of a “smart device”).
Measures
Sociodemographic characteristics, reports of having mHealth apps, smart device utilization in healthcare decision-making and health communication.
Analysis
Accounting for the complex design features of the HINTS data, we constructed multiple hierarchical logistic regressions to compute adjusted odds ratios (aOR) and their 95% confidence intervals (CI).
Results
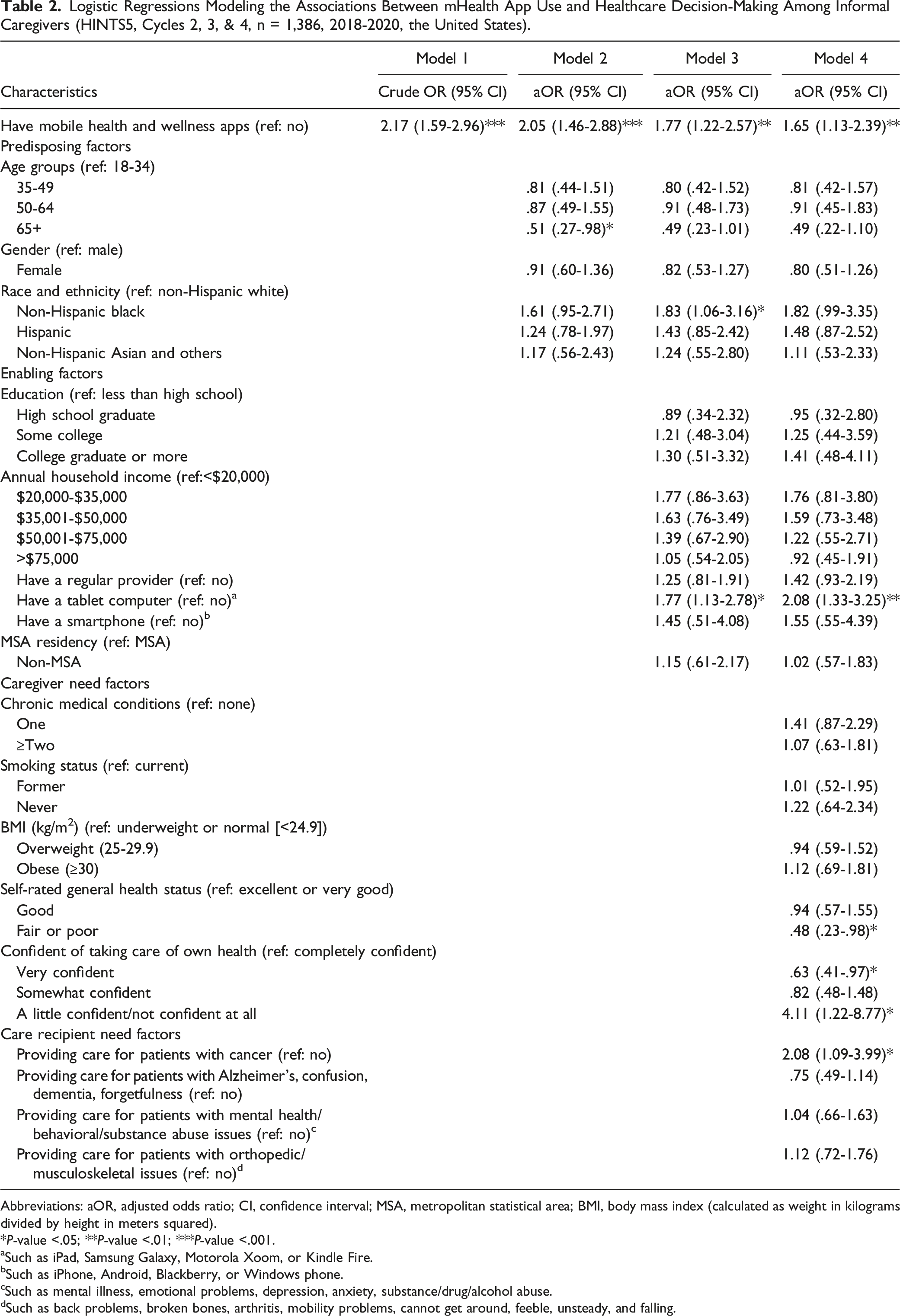
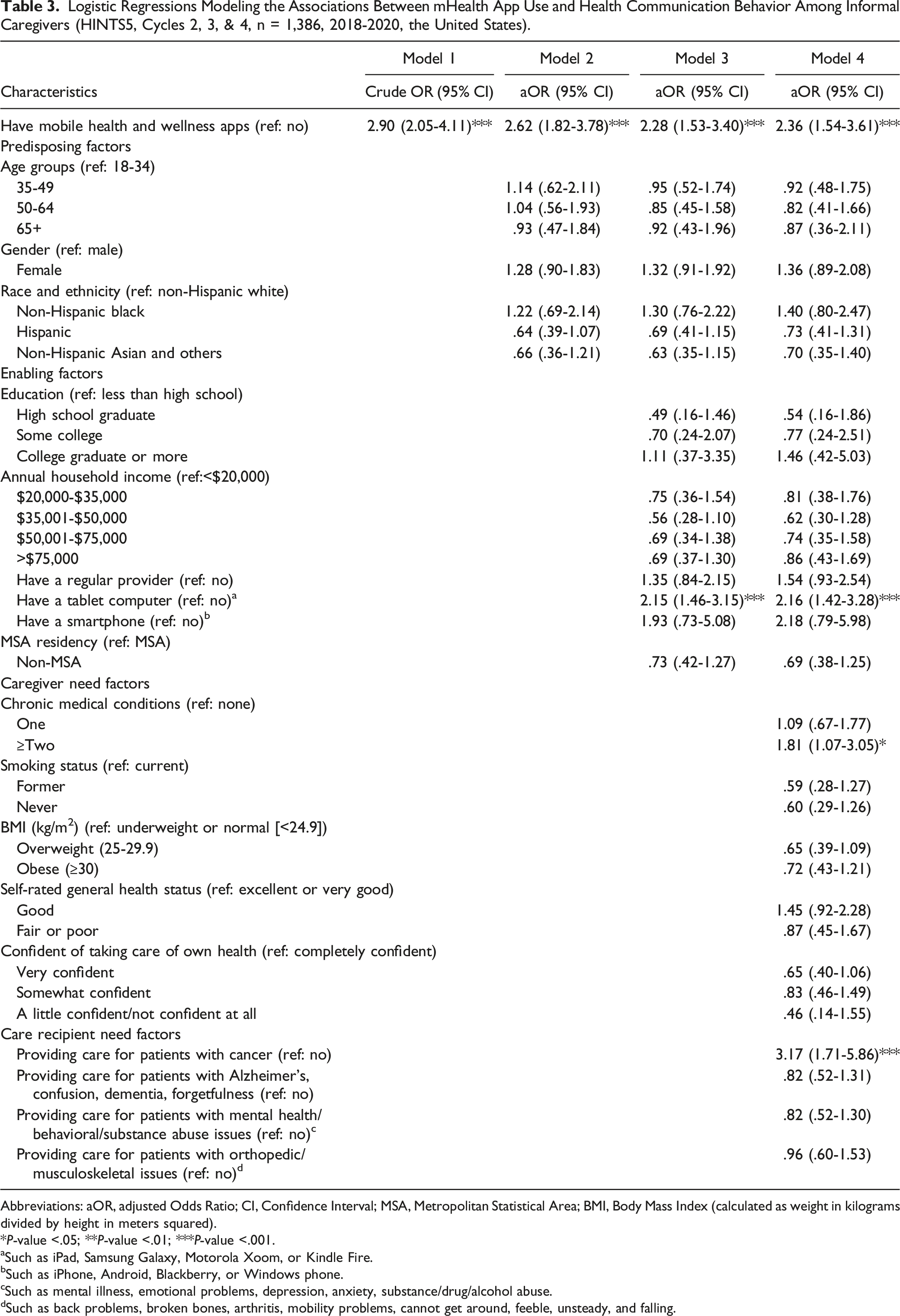
Compared to caregivers without mHealth apps, those with the apps had higher odds of utilizing their smart devices to make a health-related decision, such as how to treat a disease or a medical condition (aOR = 1.65; 95% CI: 1.13-2.39, P < .01), or engage in health-related discussions with a healthcare provider (aOR = 2.36; 95% CI: 1.54-3.61, P < .001).
Conclusion
Having mHealth apps was associated with a higher likelihood of using smart devices in healthcare decision-making and health communication by informal caregivers. Empowering caregivers to make informed health-related decisions and communicate effectively with healthcare providers are both crucial to health promotion and well-being. Future studies should investigate facilitators as well as barriers to using mHealth apps and smart devices in health-promoting strategies involving informal caregivers.
Keywords
Background and Purpose
Informal caregivers play a critical role in the United States (US) healthcare system. As of 2020, there were about 53 million informal caregivers in the US, an increase of 9.5 million since 2015. 1 They are typically family members, relatives, or close friends who provide essential and mostly unpaid care; 2 their caregiving duties may include aiding in routine tasks such as bathing and dressing, managing household responsibilities, or providing transportation. Aside from assisting with everyday tasks, they may also provide patients with emotional support and assist with managing chronic diseases or disabilities. 3 The burdens associated with providing this type of care frequently lead caregivers to experience physical and mental distress, financial challenges, time constraints, and unhealthy lifestyle behaviors such as poor sleep and diet. 4 For example, those who care for the chronically ill (e.g., cancer patients or persons with Alzheimer’s disease or dementia) often experience severe health consequences because of the additional demands placed on their time. More specifically, the current literature suggests that caregivers of older cancer patients face greater difficulty in providing care; they also experience a higher risk of fatigue and poor sleep,5-7 or depressive symptoms. 8 Given the current trend of an increase in aging populations along with those with chronic conditions, the health and emotional burdens for informal caregivers are expected to rise. 9
In recent years, new technologies have made a huge impact on healthcare delivery in the US and beyond. Increasingly, mobile health applications (mHealth apps) are being used for health information, healthcare decision-making, and health communication.10,11 Estimates suggest that there are over 350 000 mHealth apps available across mobile platforms,12-14 with a projected 3.7 billion downloads of mHealth apps expected to occur annually. 15 These apps are shown to be effective in altering health-related behaviors, including smoking cessation, weight loss, and healthy eating. 16 Recent studies further indicate that mHealth apps for chronic illnesses, which are now widely used by both healthcare providers and their patients, can improve disease management and patient outcomes.11,13,14,17 For example, a recent review study reported that Diabetes-specific mHealth apps were associated with improved glycemic control by significantly reducing HbA1c values in patients with type 1 and type 2 Diabetes. 18
Informal caregivers have greatly benefited from the rapid growth of mHealth apps.11,13 mHealth apps can equally empower patients and their caregivers through the provision of relevant and beneficial health and medical information. 19 While numerous mHealth apps have shown their efficacy and effectiveness in improving health outcomes among patient populations,20,21 interest in mHealth apps for informal caregivers is growing. For example, a quantitative content analysis that identified and assessed mHealth apps for caregivers of older and frail elderly found that among the 44 apps available, 15 apps satisfied caregivers’ needs for information and resources for caregiving. 22 These apps were found to offer features such as information on symptom tracking as well as videos to provide healthcare and medical information and professional opinions on how to care for the elderly, including patients with dementia and Alzheimer’s disease. Furthermore, 10 apps provided features to address caregiver burdens, such as information on social networks or support groups and assessments to manage stress. Further, evidence suggests that mHealth apps enhance healthcare decision-making and health communication by providing opportunities to engage in real-time with healthcare providers23,24 and to utilize readily accessible medical information. 25
Numerous other studies point to the advantages of using mHealth for informal caregivers. For example, a randomized controlled trial examined the efficacy of a caregiver-focused psychological intervention provided via a mHealth app; the intervention was specifically designed for informal caregivers of people with a physical disability or mental health disorder. 26 The trial results showed the intervention was associated with a significant reduction in caregivers’ stress and depressive symptoms, as well as improvements in other health outcomes––including subjective and emotional well-being, self-esteem, and optimism. 26 Furthermore, mHealth apps have been shown to assist informal caregivers in educating and supporting people with dementia,27,28 children with asthma, 29 as well as cancer patients. 30
Evidence from a few small-scale studies also indicates that mHealth apps have helped facilitate healthcare decision-making, improved communication with healthcare providers, and health behavior change among caregiver groups. For instance, Wittenberg et al. 31 assessed the Caregiver Communication about Cancer mHealth app, which was developed to support communication among informal cancer caregivers. 31 The authors reported that the app demonstrated the potential to increase caregiver communication knowledge as well as positively impacted family caregiver concerns and caregiver support-seeking strategies; these benefits were attributed to its implementation of evidence-based communication strategies and dissemination of information at an appropriate health literacy level for the target population. 31 Further, a meta-analysis of studies related to mHealth interventions and health outcomes among individuals aged 18 and under found that mHealth interventions show potential in eliciting meaningful improvements in adolescent health behavior, such as promoting physical activity. 32 This meta-analysis reported that mHealth interventions with caregiver involvement produced greater changes in health outcomes, which supported findings from previous studies that caregiver involvement can have positive impacts on health promotion and management of chronic illnesses among youth.33,34
Despite the potential benefits of mHealth apps, evidence on the adoption of these tools among informal caregivers is still scarce. Further, to the best of our knowledge, the benefits of mHealth apps in healthcare decision-making and health communication among informal caregivers at the broader population levels in the US have not been examined. This study contributes to the burgeoning research on mHealth apps among caregivers by examining how mHealth apps are used by informal caregivers in a nationally representative sample. More precisely, our specific aims were: (1) to identify the sociodemographic and other characteristics of US informal caregivers who own mHealth apps on their smart devices and (2) to investigate the associations between having mHealth apps and healthcare decision-making and health communication among these caregivers. We hypothesize that caregivers’ owning mHealth apps is associated with caregivers’ healthcare decision-making and health communication behavior.
Methods
Data Source, Settings, and the Study Participants
Data for the present study were obtained from the Health Information National Trends Survey (HINTS), a nationally representative survey in the US, which is conducted every few years by the National Cancer Institute since 2003. 35 The surveys employ random sampling among civilian non-institutionalized adults aged 18 years and older to collect information on the use of, access to, and needs for health-related information, perceptions, knowledge, and behaviors.36,37 We extracted data for 1386 self-identified informal caregivers from HINTS5 Cycles 2 through 4, which were conducted in 2018, 2019, and 2020. This sample of informal caregivers was identified based on HINTS participants’ responses to two questions. In the survey, respondents were asked “Are you currently caring for or making health care decisions for someone [a child/children, a spouse/partner, a parent/parents, another family member, a friend or other non-relative] with a medical, behavioral, disability, or other condition?” Participants with an affirmative response were then asked a follow-up question, “Do you provide any of this care professionally as part of a job (for example, as a nurse or professional home health aide)?” Participants with an affirmative response to the first question and a non-affirmative response to the second were determined as “informal caregivers.” The HINTS5 cycle 1 data were not included in the current study because the survey did not differentiate formal from informal caregivers in the follow-up question.
For this study, we limited our sample to informal caregivers who indicated that they owned at least a smartphone or a tablet computer (i.e., ownership of a “smart device”). All HINTS5 cycles involved self-administered mailed questionnaires except for Cycle 3; this cycle, which occurred in 2019, involved a multi-mode survey that incorporated a Web pilot in addition to the mail-in surveys. The response rates for Cycles 2 through 4 were 32.39%, 30.2%, and 36.7%, respectively. Further details about the survey design, methodology, and access to data are available at https://hints.cancer.gov/. All study results were reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. This study utilized de-identified, publicly-available secondary data and was exempt from obtaining additional institutional review board approval.
Measures of Healthcare Decision-Making, Health Communication, and mHealth Apps
The study’s two main outcomes were constructed from responses to survey questions assessing healthcare decision-making and health communication in the HINTS5. Caregivers who indicated having a smart device were asked if such devices benefited them in making decisions about treating health and medical conditions and in communicating with healthcare providers. Specifically, caregivers’ healthcare decision-making was assessed through the survey question, “Has your tablet or smartphone helped you make a decision about how to treat an illness or condition?” The caregivers’ communication with healthcare providers was measured through the survey question, “Has your tablet or smartphone helped you in discussions with your healthcare provider?” Both outcomes had a binary response of (yes vs no). Our key independent variable, whether the caregiver downloaded and had mHealth apps on his/her smart devices, was assessed through the survey question, “On your tablet or smartphone, do you have any "apps" related to health and wellness?”, with a binary response of (yes vs no).
Study Covariates
The Andersen Behavioral Model of Health Services Utilization (Andersen Model), was used as a conceptual framework to guide the selection of the study covariates.38-41 The selected predisposing factors include age in years (18-34, 35-49, 50-64, 65+), self-reported gender (male vs female), and race and ethnic identity (non-Hispanic White, non-Hispanic Black, Hispanic, non-Hispanic Asian and others). The enabling factors include educational attainment (less than high school, high school graduate, some college, college graduate or more), annual household income (<$20,000, $20,000-$35,000, $35,001-$50,000, $50,001-$75,000, >$75,000), having a regular provider (yes vs no), a tablet computer (yes vs no), a smartphone (yes vs no), and metropolitan statistical area (MSA) residency (MSA vs non-MSA). Finally, two sets of need-for-care factors were included. Those directly related to caregivers themselves, such as chronic medical conditions (none, one, ≥two), smoking status (current, former, never), body mass index (BMI) calculated as weight in kilograms divided by height in meters squared (kg/m2) (underweight or normal [<24.9], overweight [25-29.9], obese [≥30]), self-rated general health status (excellent or very good, good, fair or poor), and confidence in taking care of own health (completely confident, very confident, somewhat confident, a little confident/not confident at all). Need-for-care factors related to care recipients include whether the caregiver is providing care for patients with cancer; patients with Alzheimer’s, confusion, dementia, forgetfulness; patients with mental health, behavioral, and/or substance abuse issues; or providing care for patients with orthopedic/musculoskeletal issues. Each of these four need factors was treated as a binary variable (yes vs no) in the analyses.
Statistical Analysis
Our data analysis begins with an exploration of data and a careful check for missing data. The SAS MI procedure was used to check for missing data patterns and we found no such patterns. The few missing observations in the data were deemed completely at random. We then analyzed the general characteristics of all respondents in the study sample; followed by hierarchical logistic regressions model-fitting to examine the associations between having mHealth apps and caregivers’ healthcare decision-making and health communication while controlling for the covariates. The design-adjusted Rio-Scott chi-square test was used to evaluate all cross-tabulated associations. For the associations between having mHealth apps and each dependent outcome, (i.e., healthcare decision-making and health communication), we initially ran simple logistic regressions to generate crude odds ratios (ORs) and 95% confidence intervals (CIs). In the hierarchical multivariable regression models, we sequentially adjusted for predisposing, enabling, and need-for-care factors to compute adjusted ORs (aORs) and 95% CIs. Multicollinearities were checked at several steps of model building. We also accounted for the complex design features of the HINTS data in all analyses to generate population-level values, and the associated variance estimates, to make the results relevant to the US population. The SAS 9.4 statistical software program (SAS Institute Inc., Cary, NC, USA) was used to analyze the data, and the significance threshold was set at P-value <.05.
Results
General Characteristics of the Informal Caregivers and Proportions of Those Who Reported Having mHealth Apps (HINTS5, Cycles 2, 3, & 4, n = 1,386, 2018-2020, the United States).
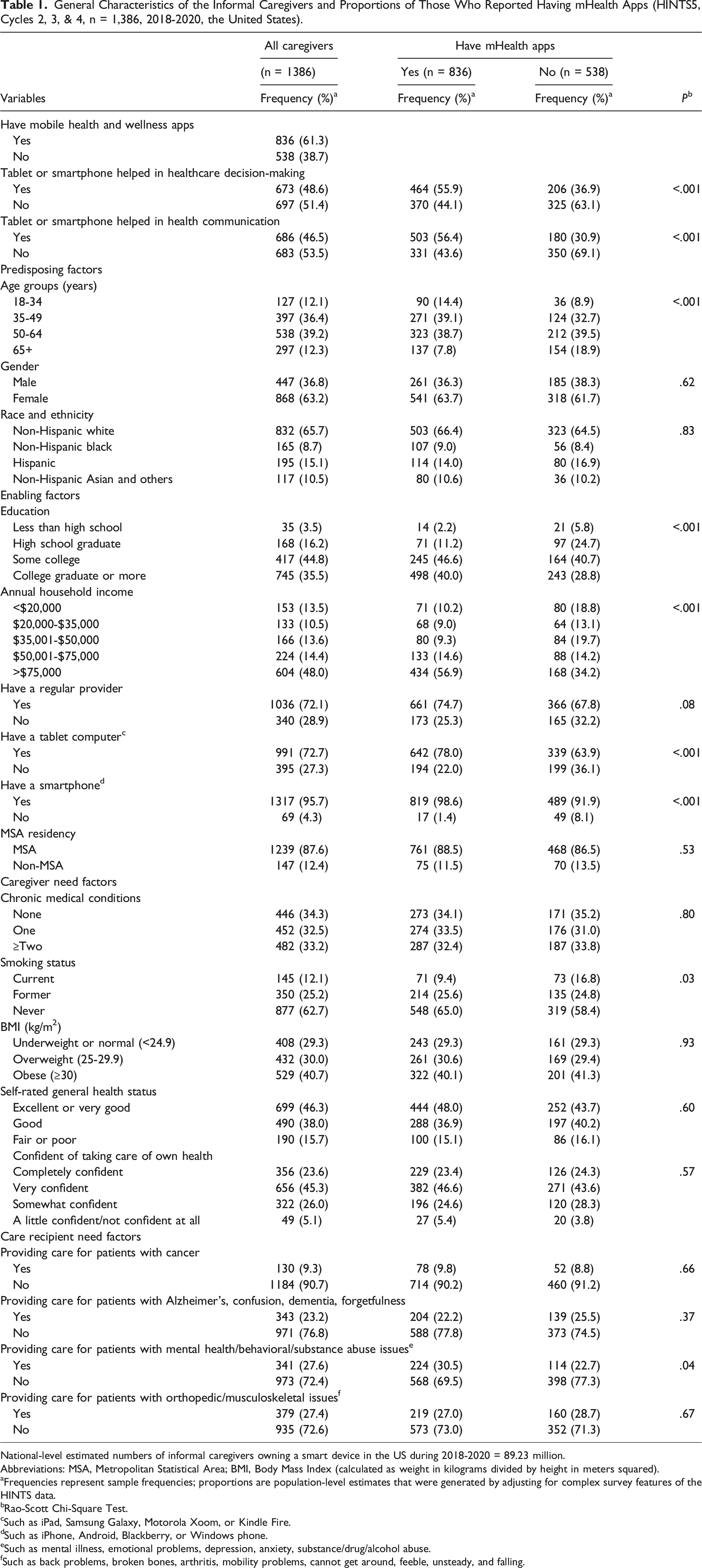
National-level estimated numbers of informal caregivers owning a smart device in the US during 2018-2020 = 89.23 million.
Abbreviations: MSA, Metropolitan Statistical Area; BMI, Body Mass Index (calculated as weight in kilograms divided by height in meters squared).
aFrequencies represent sample frequencies; proportions are population-level estimates that were generated by adjusting for complex survey features of the HINTS data.
bRao-Scott Chi-Square Test.
cSuch as iPad, Samsung Galaxy, Motorola Xoom, or Kindle Fire.
dSuch as iPhone, Android, Blackberry, or Windows phone.
eSuch as mental illness, emotional problems, depression, anxiety, substance/drug/alcohol abuse.
fSuch as back problems, broken bones, arthritis, mobility problems, cannot get around, feeble, unsteady, and falling.
The chi-square tests for cross-tabulations in Table 1 indicate the presence of significant associations between having mHealth apps and caregivers’ healthcare decision-making, improved communication with healthcare providers, age, education, annual household income, having a tablet, a smartphone, caregivers’ smoking status, and providing care for patients with mental health, behavioral, and/or substance abuse issues (see Table 1). Among mHealth app owners, a higher proportion reported their smart devices helped in healthcare decision-making (55.9%) and communicating with healthcare providers (56.4%). A higher proportion of younger (aged 35 to 64 years) caregivers (77.8%), while a lower proportion (7.8%) of 65+ years reported having mHealth apps. About 86.6% of the caregivers with mHealth apps had some college or more education, and 56.9% had an annual household income of >$75,000. Caregivers who had a tablet or a smartphone made up 78.0% and 98.6% of mHealth app owners, respectively. Further, 30.5% of caregivers who reported caring for people with mental health/behavioral/substance abuse indicated they own mHealth apps, whereas only 9.8% of those caring for patients with cancer reported mHealth ownership (see Table 1).
The majority of caregivers (34.8%) indicated that they are providing informal care and making healthcare decisions for a child/children, followed by 29% who had such responsibilities for a parent/parents in need of care. Close to 13% of informal caregivers selected more than one group of care recipients –– indicating that they are responsible for informal healthcare and decision-making for multiple groups of care recipients (see Figure 1). Frequency and proportions of caregiving responsibilities and informal caregiving recipients (HINTS5, Cycles 2, 3, & 4, n = 1386; 2018-2020, the United States).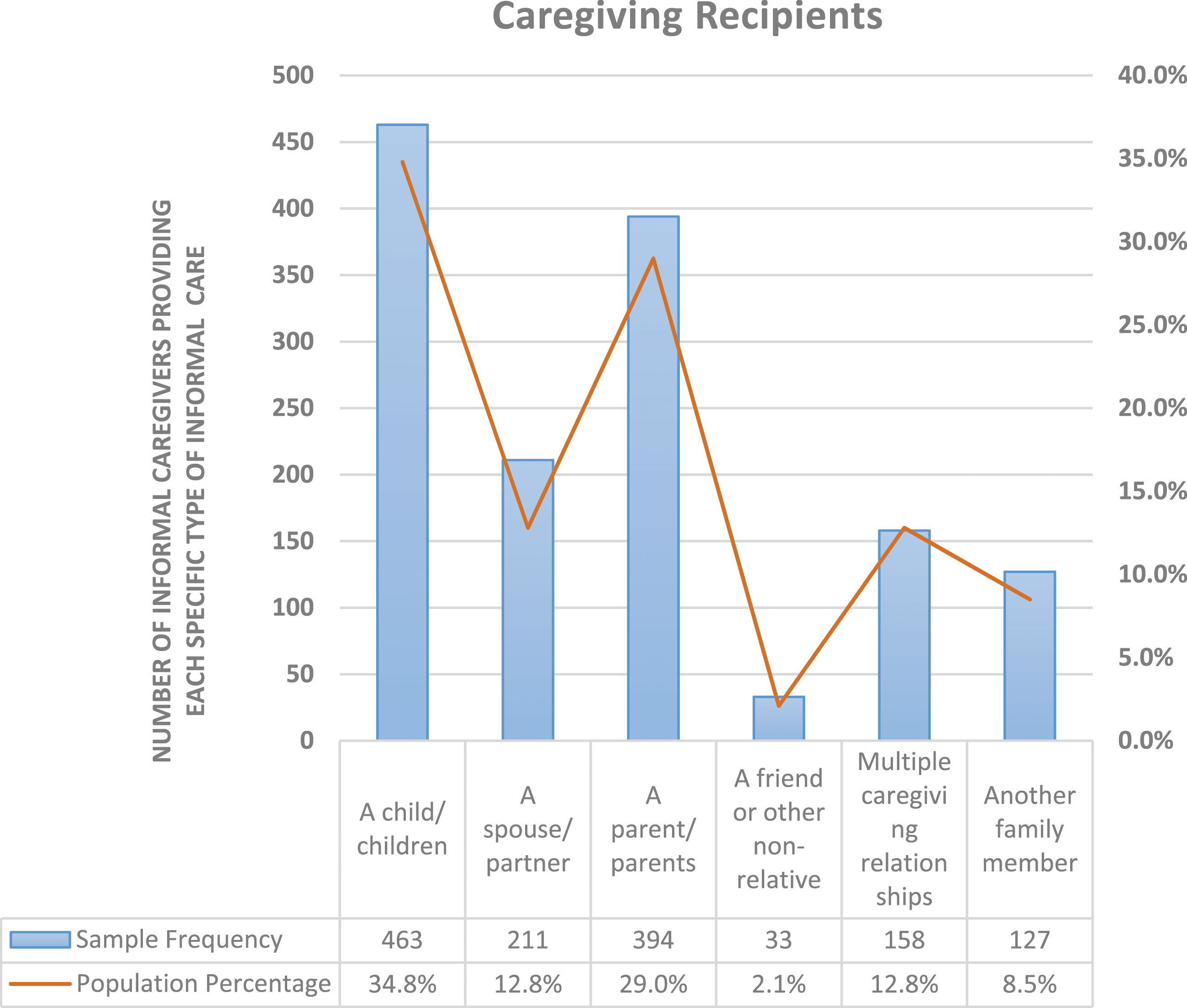
Logistic Regressions Modeling the Associations Between mHealth App Use and Healthcare Decision-Making Among Informal Caregivers (HINTS5, Cycles 2, 3, & 4, n = 1,386, 2018-2020, the United States).
Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; MSA, metropolitan statistical area; BMI, body mass index (calculated as weight in kilograms divided by height in meters squared).
*P-value <.05; **P-value <.01; ***P-value <.001.
aSuch as iPad, Samsung Galaxy, Motorola Xoom, or Kindle Fire.
bSuch as iPhone, Android, Blackberry, or Windows phone.
cSuch as mental illness, emotional problems, depression, anxiety, substance/drug/alcohol abuse.
dSuch as back problems, broken bones, arthritis, mobility problems, cannot get around, feeble, unsteady, and falling.
Logistic Regressions Modeling the Associations Between mHealth App Use and Health Communication Behavior Among Informal Caregivers (HINTS5, Cycles 2, 3, & 4, n = 1,386, 2018-2020, the United States).
Abbreviations: aOR, adjusted Odds Ratio; CI, Confidence Interval; MSA, Metropolitan Statistical Area; BMI, Body Mass Index (calculated as weight in kilograms divided by height in meters squared).
*P-value <.05; **P-value <.01; ***P-value <.001.
aSuch as iPad, Samsung Galaxy, Motorola Xoom, or Kindle Fire.
bSuch as iPhone, Android, Blackberry, or Windows phone.
cSuch as mental illness, emotional problems, depression, anxiety, substance/drug/alcohol abuse.
dSuch as back problems, broken bones, arthritis, mobility problems, cannot get around, feeble, unsteady, and falling.
Caregivers who had a tablet (aOR = 2.08; 95% CI: 1.33-3.25, P-value <.01 vs no tablets), those who were a little confident/not confident at all about taking care of their own health (aOR = 4.11; 95% CI: 1.22-8.77, P-value <.05, vs completely confident), and those who provided care for patients with cancer (aOR = 2.08; 95% CI: 1.09-3.99, P-value <.05, vs no) had higher odds of using their smart devices in healthcare decision-making. Furthermore, caregivers who self-rated their general health status as fair or poor (aOR = .48; 95% CI: .23-.98, P-value <.05, vs excellent or very good) and those who reported being very confident about taking care of their own health (aOR = .63; 95% CI: .41-.97, P-value <.05, vs completely confident) had lower odds of using their smart devices in healthcare decision-making (see Table 2, Model 4). Similarly, caregivers who had a tablet (aOR = 2.16; 95% CI: 1.42-3.28, P-value <.001, vs no tablets), those who had ≥ two chronic medical conditions (aOR = 1.81; 95% CI: 1.07-3.05, P-value <.05, vs none), and those who were providing care for cancer patients (aOR = 3.17; 95% CI; 1.71-5.86, P-value <.001, vs no) had higher odds of using their smart devices for health communication (see Table 3, Model 4).
Discussion
This study used survey data from a nationally representative sample of informal caregivers in the US to identify the characteristics of informal caregivers who use mHealth apps on their smart devices. We also examined associations between having mHealth apps and caregivers’ healthcare decision-making and health communication behavior. Although informal caregivers play an essential role in healthcare delivery by caring for their care recipients/loved ones, they may frequently deal with challenging circumstances that could adversely affect their own and/or their loved ones’ health. With mHealth apps incorporating numerous public health interventions or programs to improve individual health and healthcare, there is a substantial opportunity to address the caregiving burden among informal caregivers and promote their health by utilizing the innovative features of mHealth apps.
Our findings demonstrate that informal caregivers who reported having mHealth apps had higher odds of using their smart devices to make health-related decisions such as treating a disease or a medical condition and in health-related discussions with a care provider, compared to those who did not have mHealth apps on their devices. mHealth and wellness apps use by caregivers can be encouraged and supported by healthcare providers and policymakers, which can help address the caregiving burden and improve caregiver health by facilitating health-related decision-making and health communication. mHealth apps can also be beneficial to caregivers’ care recipients as they can be used as health education and as health management tools or resources.
Given that caregivers’ burden is expected to increase due to growing aging populations and an increase in the prevalence of chronic conditions, eHealth tools (including mHealth apps), could be further incorporated into health-related interventions or programs targeting caregiver populations. Also, since caregivers’ health is vitally important in providing care to others, it is critical to provide them with appropriate, efficient health promotion strategies and interventions through mHealth apps. The findings from our study align with some of the existing literature on mHealth use among other population groups. For example, in a study among adults with chronic medical conditions, Mahmood et al. 42 found that having mHealth apps was associated with 77% higher odds of using smart devices in healthcare decision-making and twofold higher odds of using such devices in health communication behavior. 42 Similarly, Langford et al., 43 in a cross-sectional analysis among a sample of adults, found that respondents with mHealth apps were more likely to report that their smart devices helped them in medical decision-making, compared with those who did not.
Strengths and Limitations
One of the strengths of HINTS data lies in providing a nationally representative sample to track health communication and health information technology use. However, it is important to acknowledge the dataset’s limitations. First, due to its cross-sectional nature, inferring causality and the direction of the associations is difficult. Furthermore, even though individuals often download health and wellness apps, we do not have information on whether the informal caregivers included in the current study indeed utilized the apps; additionally, some mHealth apps run in the background even if device owners do not intend to use them. Moreover, despite adjusting for numerous caregiver and care recipient characteristics based on the conceptual model, there still could be other confounding factors, not accounted for in this study. Any additional unmeasured confounding factors may have correlations with smart devices, and mHealth app use, as well as with the caregivers’ sociodemographic characteristics. Such factors may include caregivers’ experiences with mobile apps, the extent of caregivers’ knowledge and proficiency with mHealth applications, privacy and security concerns, ease of use, costs of using applications, perceived usefulness, readiness for change, self-efficacy, and health literary or consciousness that each could influence downloading and using mHealth apps.44-47
Further, data were not collected consistently about the intensity and type of caregiving services across all cycles of HINTS-5 and we were unable to account for these factors in the current study. Questions assessing the study outcomes, namely, healthcare decision-making and health communication, are more generally structured and do not specify whether these behaviors pertain to the caregivers, their care recipients, or both. Other unmeasured confounding factors that could distort the examined associations include information about utilizing other means or tools for health-related decisions and health communication with providers such as employing a desktop, or a laptop computer, for health information seeking and decision-making, and making in person health communications with providers. Hence, we were limited by the nature of the survey questionnaire for the HINTS dataset, and the available information. Finally, the HINTS is a self-administered survey and is thus susceptible to bias such as misinterpretation of the survey questions, social desirability, and recall bias. These limitations provide an opportunity for future researchers to design and conduct prospective, longitudinal, and more robust studies to support a causal relationship and impacts of mHealth apps use on healthcare decision-making and health communication among informal caregivers.
Conclusion and Recommendations
Among a nationally representative sample of 1386 self-identified informal caregivers in the US, reports of having mHealth apps were associated with higher odds of using smart devices in healthcare decision-making and health communication. Empowering caregivers and patients to make informed health-related decisions and effective health communication are both crucial to improving health and well-being. 48 Several of the Healthy People 2030 objectives in the US focus on increasing health communications and shared healthcare decision-making through implementations of health information technology tools including mHealth apps, 48 and reducing caregiver burdens such as anxiety and depression by providing the support and resources they need to keep themselves and their care recipients healthy. 49 Further, one of the primary aims of the World Health Organization (WHO) is to improve the health and well-being of individuals through the interventions of digital health. 50 Thus, channeling health and healthcare to informal caregivers and the people they are caring for through effective and science-based mHealth apps and smart devices has the potential to be a successful strategy.
Smart devices and mHealth apps are expected to continue to transform the practice and reach of healthcare and research in the foreseeable future. Thus, healthcare providers and policymakers can suggest successful, effective, and validated mHealth apps for informal caregivers to increase their use and maximize health benefits for both caregivers and their care recipients. mHealth app developers share similar responsibility to work with researchers and healthcare professionals to design and deliver evidence-based mHealth apps that improve health outcomes and are specifically tailored towards the needs of informal caregivers. Future studies should investigate other facilitators as well as barriers to using mHealth apps among this specific group of the population within the community. With the growth of information technology and smart handheld devices (i.e., smartphones and tablet computers), mobile health (mHealth) applications (apps) are increasingly used to promote health and quality of life for caregivers and their care recipients. However, there is limited scholarship about how these apps’ use impacts informal caregivers’ healthcare decision-making and health communication. The current study demonstrates that informal caregivers who reported having mHealth apps had a higher likelihood of using their smart devices in health-related decisions such as treating a disease or a medical condition, and in health-related communications with care providers, compared to those who did not have mHealth apps on their devices. Channeling health and healthcare to informal caregivers through effective and science-based mHealth apps and smart devices has the potential to be a successful health promotion strategy. Healthcare providers and policymakers should suggest validated and effective mHealth apps for informal caregivers to increase their use and maximize health benefits for both caregivers and their care recipients.So What?
What is Already Known on This Topic?
What Does This Article Add?
What are the Implications for Health Promotion Practice or Research?
Footnotes
Author Contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research Ethics and Patient Consent
This study employed de-identified, publicly available, secondary data and was exempt from obtaining additional institutional review board approval.