
Abstract
Objective
To explore the empirical literature on gender/sex differences in vaccine acceptance among U.S.-based adults and adolescents in approximately the first 2 years of the pandemic.
Data source
Embase, Medline, PsycINFO, EBSCO, CINAHL, Web of Science
Study inclusion and exclusion criteria
Peer-reviewed studies conducted in the U.S. with those aged 12 and older, published in English before January 12, 2022, examining the relationship between gender/sex on COVID-19 vaccine intentions and/or uptake.
Data extraction
Three authors screened studies and extracted data.
Data Synthesis
Univariate and multivariate results are summarized.
Results
A total of 53 studies met inclusion criteria (48 intentions, 7 uptake), using mostly cross-sectional designs (92.5%) and non-random sampling (83.0%). The majority of studies supported men’s greater intentions to vaccinate compared to women, and men’s greater vaccine uptake in univariate analyses, but most multivariate analyses supported no gender differences in uptake. Few studies examined gender beyond binary categories (women/men), highlighting a gap in the studies inclusive of transgender or gender-diverse populations in analyses.
Conclusion
Women may have been more hesitant to get the vaccine than men early in the pandemic, but these differences may not translate to actual behavior. Future research should include non-binary/transgender populations, explore the gender-specific reasons for hesitancy and differences by sub-populations, utilize more rigorous designs, and test gender-sensitive public health campaigns to mitigate vaccine concerns.
Introduction
The COVID-19 pandemic has caused nearly 7 million deaths globally as of May 2023, 1 including over 1 million in the United States (U.S.), 2 and has had enormous social and economic consequences. 3 Among the stark health disparities that have resulted from the pandemic, disparities are apparent by gender. There have been more COVID-19 hospitalizations and deaths in the U.S. among men compared to women which have been attributed to differences in engagement in COVID-19 prevention related to gender rather than biological differences related to sex.4,5 In addition, some evidence shows that transgender and non-binary people are at elevated risk for negative COVID-19 outcomes, but public health data often fails to report data beyond the binary model of gender/sex.6,7
Studies have shown women use health services more than men,8-10 and emerging research suggests that they may also engage in COVID-19 prevention strategies (e.g., mask-wearing, social distancing, handwashing) more than men. 11 However, acceptance of the COVID-19 vaccine may stray from these typical gender patterns. Prior to the emergence of COVID-19, greater vaccine hesitancy had been documented among women compared to men.12,13 Specific to COVID-19, a recent global meta-analysis reported lower vaccine intentions among women compared to men, but this varied by country. 14 The review did not examine non-binary gender populations, 14 but research shows COVID-19 may exacerbate structural inequalities for transgender and gender-diverse communities. 7 Other reviews on gender and COVID-19 vaccination are also global in scope, or broadly examine determinants of COVID-19 vaccination, but are not explicitly focused on gender/sex differences.15-19 Thus, a review focused on gender/sex differences in vaccination in the U.S. population would fill a gap in the literature.
We conducted a scoping review which sought out studies that examined gender/sex differences in COVID-19 vaccine acceptance (intentions/uptake) among adults and adolescents in the U.S. published in approximately the first 2 years of the pandemic, with the goal of summarizing the existing evidence and identifying gaps for future research. Given that COVID-19 acceptance changes over time, the focus on the early stages of the pandemic allows us to explore acceptance in a timeframe crucial to pandemic control before and soon after vaccine availability. Scoping reviews include the “mapping” of evidence originating from a broad range of methodologies to convey the breadth, depth, and gaps of a field through a team-based iterative review and analytic reinterpretation of the literature. 20 Scoping reviews are appropriate for emerging research areas, as they can demonstrate the scope of the literature on a given topic, provide insight on the quantity of published papers about a topic, and produce specific questions for the purposes of further research and investigation. 21 In addition to synthesizing the literature on gender/sex differences in vaccine acceptance, we were interested in exploring how studies conceptualized gender (i.e., biological sex vs gender identity) and whether the current literature could shed light on vaccination intentions/uptake across the gender spectrum. We were also interested in exploring whether gender differences in vaccination varied by other sub-populations (such as by race/ethnicity, adolescents vs adults, etc.). This review was part of a larger search that also sought studies on gender/sex differences in other COVID-19 prevention behaviors (i.e., mask-wearing, social distancing, adherence to CDC guidelines). Due to space limitations, these outcomes will be reported separately in a companion review.
Methods
Database and Search Strategy
The search was carried out by a librarian specializing in public health (MH) on January 12th, 2022, and included 6 databases: Embase, Medline, PsycINFO, EBSCO, CINAHL, and Web of Science. The search strategy included terms related to COVID-19, gender/sex differences, and the COVID-19 prevention outcomes of interest (see Table S1 for the search terms). We adhered to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) where appropriate (checklist provided in Table S2). 22
Study Selection
Studies were eligible for inclusion in this review if they examined gender or sex differences in vaccine intentions (self-reported plans/willingness/reluctance to be vaccinated) and/or vaccine behavior (self-reported or clinic record extraction on receipt of the COVID-19 vaccine). The search was inclusive of biological sex and self-identified gender identities on a spectrum (inclusive of non-binary identities). However, since the main research question of interest is gender/sex differences in the stated outcomes, studies could only be included if they made comparisons between groups (thus, a study on only men, only women, or only a non-binary population were excluded). The examination could have been quantitative or qualitative. Studies were published before January 12, 2022, but after the start of COVID-19 pandemic (search start date: January 1, 2020), were peer-reviewed, published in English, and were conducted within the U.S. with adult (18 years or older) and/or adolescent populations (12 years or older, chosen based on the cut-off age for COVID-19 vaccine availability at the time in the U.S.).
Studies identified during searches were merged using Endnote (version X7), and duplicate records were removed. The references were then imported from Endnote into COVIDENCE, a systematic review data management tool. 23 Three authors (KMS, IMH, RLL) and a research assistant reviewed titles and abstracts to determine eligibility based on the inclusion criteria, working in pairs. If there was disagreement within pairs, the article was discussed with a third reviewer; if consensus could not be reached, the article was included in the full-text review. These same teams then reviewed full-text articles in pairs against the review’s inclusion criteria. Any study in question or with inconsistent classification between authors was discussed between the team and consensus was reached.
Data Extraction
A data extraction tool was created and piloted to extract key information related to study design, sampling strategy, target population and setting, outcome measurement, gender/sex definition, main study findings related to gender/sex’s association with the review outcomes including univariate (unadjusted) and multivariate (adjusted) results, as applicable, and limitations as stated by study authors. Given the review’s secondary interests in exploring gender differences in vaccine outcomes by relevant subgroups, the results of moderation analyses were extracted when available (e.g., gender by race, age, or other interactions). Two reviewers (IMH, RLL) reviewed studies, with reviewer 1 conducting the initial extraction, reviewer 2 reviewing extraction and suggesting changes and together coming to consensus. Reviewer 3 (KMS) completed a final review, focusing on the extraction of outcome measurement and results, and acted as a tiebreaker to resolve any discrepancies, as needed. We contacted study authors in cases where clarification was needed on extracted data. In cases where the author’s information altered the extracted results, it is noted in the results tables.
Data Analysis Approach
We did not pool the study findings through meta-analysis, given the wide breadth of this scoping review, and disparate measurement of the outcomes of interest. We summarize each study and report findings for studies individually in the format that they were reported in the original paper by study authors. We extracted and present the association of gender/sex and the outcomes of interest obtained from both univariate and multivariate results, when available (with a summarized overview of other variables in the multivariate model). If papers only reported descriptive results (without tests of statistical significance conducted) but made a statement on differences, these results are reported as stated by the study authors.
Results
A total of 3191 unique citations were identified through the database search after the exclusion of duplicates. Of the 195 reports that underwent full-text screening, 142 were excluded for reasons outlined in Figure 1. See Table S3 for a list of ineligible studies reviewed as full-text with reasons for exclusion. In total, 53 studies met criteria for inclusion in this review, and contributed data for the following outcomes: vaccine intentions (k = 48, 52 total outcomes assessed) and vaccine uptake (k = 7, 8 total outcomes assessed). PRISMA flowchart for study inclusion/exclusion.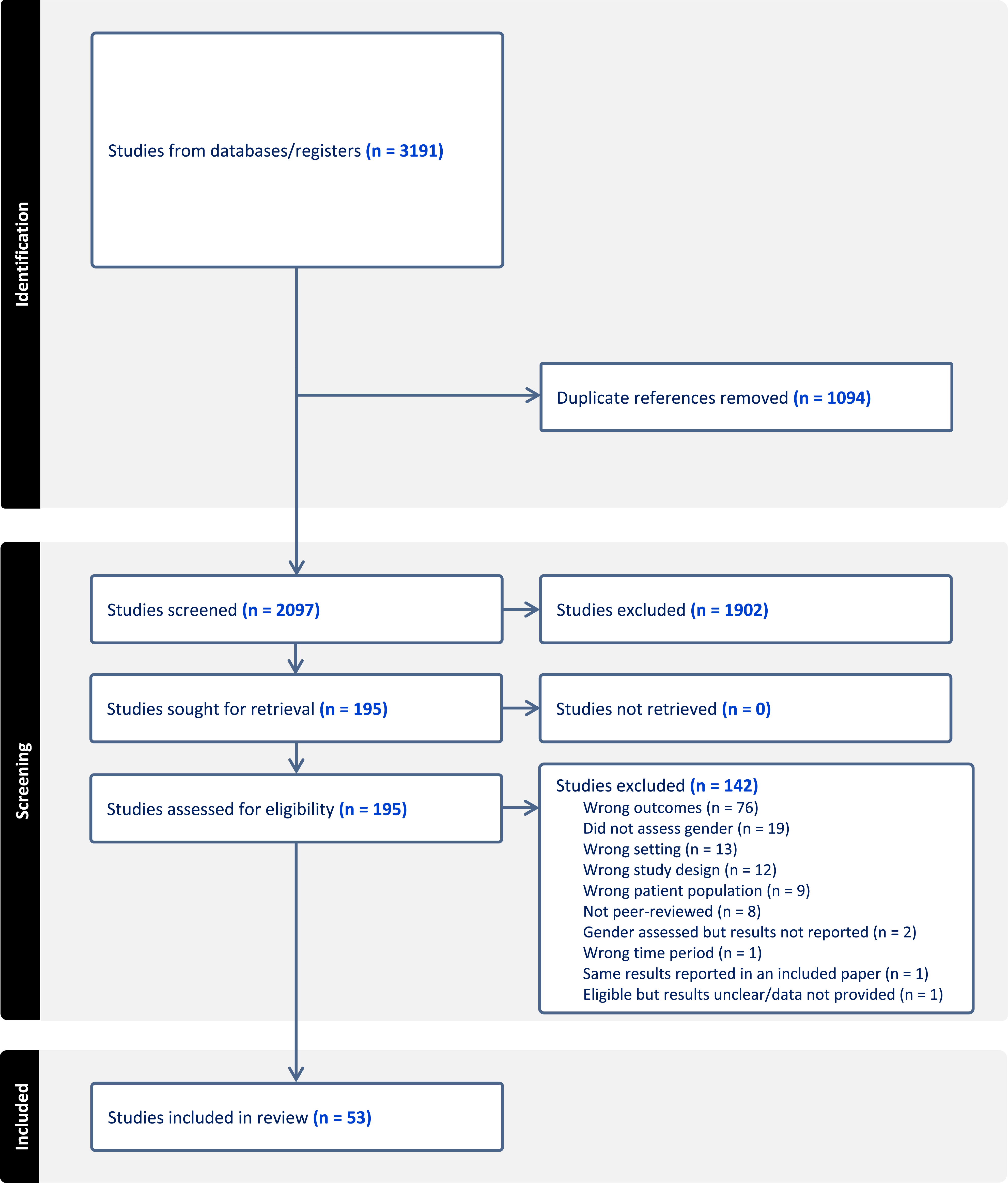
Characteristics of Included Studies
Summary of study characteristics.

Abbreviations: M = Mean, SD = Standard Deviation; IQR = Interquartile range; Notes: *More than the percent female is reported for studies that included more than binary (male/female) gender categories in their analyses (reported in Table 2) **San Francisco, CA; Oakland, CA; Fresno, CA; Sylmar, CA; Seattle, WA; Iowa City, IA; Detroit, MI; Ann Arbor, MI; New Orleans, LA; Philadelphia, PA; Durham, NC; Baltimore, MD; Camden, NJ; Boston, MA; The reporting of age varied; it is reported as reported in the paper. Age and percent female were sometimes calculated by the review authors from other data provided.
Reported Results of Gender/Sex Differences in Vaccine Outcomes
Summary of study results on sex/gender differences in COVID-19 vaccination intentions and uptake in the first year of the pandemic, U.S. populations (age 12 and above).

Notes: Symbols indicate greater intentions COVID-19 vaccine acceptance in ⬤ = Women (vs. men),  = Men (vs. women), or
= Men (vs. women), or  = No difference; NR = not reported; OR = Odds Ratio; AOR = Adjusted Odds Ratio; CI = Confidence Interval; SE = Standard Error; ref = reference group; ***Univariate results sent from study authors and multivariate not extracted due to difficulty in interrupting published results.
= No difference; NR = not reported; OR = Odds Ratio; AOR = Adjusted Odds Ratio; CI = Confidence Interval; SE = Standard Error; ref = reference group; ***Univariate results sent from study authors and multivariate not extracted due to difficulty in interrupting published results.
Vaccine Intentions
The measurement of vaccine intentions varied considerably across studies, but most often used a single item constructed by study authors asking about the likelihood that respondents would get a vaccine (sometimes hypothetically, in cases when it was not yet available) or their plans to get the vaccine. Response options used included a range of options, including binary (e.g., yes/no), categorical (e.g., I plan to, I do not plan to, I am not sure), and continuous outcomes (e.g., Likert scale on likelihood of vaccination in the future).
The vast majority of studies examined gender/sex in binary categories24-34,36-38,40-44,46-52,55-59,61-63,65-69,71,72,75,76 with only five studies reporting analyses inclusive of other gender identities for vaccine intentions.35,45,53,60,64 We summarize the findings first for gender binary comparisons. In univariate analyses, 73.7%, or 28 of the 38 analyses (k = 27), found greater vaccine intentions among men compared to women,24-26,29,31,33-38,44,46,48,50,55-58,60-64,68,69,72 and 7.9%, or 3 of the 38 analyses (k = 3), found greater vaccine intentions among women compared to men.42,45,47 Finally, 18.4% or 7 of the 38 analyses (k = 7), found no differences between men and women in COVID-19 vaccine intention.30,41,43,47,71,75,76
A total of 37 studies examined differences between men and women's vaccine intentions using multivariate analyses across 40 outcomes (i.e., controlling for other variables). In summary, 72.5%, or 29 of 40 analyses (k = 27), found greater vaccine intentions among men compared to women,24,26,27,30-33,35,36,38,42,43,45,48-51,53,56,58,60,62,66-68,72,75 and only one study (1 outcome) or 2.5% of the 40 analyses found greater vaccine intentions among women compared to men. 76 Finally, 25.0%, or 10 of the 40 analyses (k = 9), found no differences between men and women in COVID-19 vaccine intentions.28,37,40,44,47,52,57,59,65 A visual overview is provided that showcases these findings in brief (symbols only) in Table S4.
The results of the five studies that examined gender beyond binary categories for vaccine intentions are mixed and difficult to compare due to varying classifications and reference groups (detailed statistics in Table 2 and highlighted separately in Table S5).35,45,53,60,64 In summary, 2 studies with general U.S. samples reported no differences in COVID-19 vaccine intentions in non-binary or “other” gender categories compared to males (univariate and multivariate analyses),45,60 although one of these studies reported lower intentions in those not responding to the gender question compared to males. 45 All other studies were with health workers and/or health system employees. Dowdle et al. 35 reported greater intentions in gender non-conforming groups compared females (univariate and multivariate analyses). Momplaisir et al. 53 reported lower intentions in those in the “other” sex category compared to males (multivariate analysis). Shaw et al. 64 reported overall lower vaccine intentions in non-binary/gender not-disclosed employees compared to males and females, with a wider difference compared to males (univariate analysis).
Vaccine Uptake
Out of the 7 total studies measuring vaccine uptake, the outcome was most often measured through self-report (71.4%, k = 5)42,54,64,70,73; usually self-reported outcomes were obtained through constructed questions asking whether one had been vaccinated against COVID-19 (yes/no).39,74 The remaining 2 studies used electronic clinic records to extract vaccine status (28.6%, k = 2). Across both self-report and clinic record outcomes, there was variation in the definition of vaccination based on doses, which in some cases can be attributed to the varying timeframes of the studies (availability of second dose varied). Most studies defined vaccination as uptake of at least one dose (57.1%, k = 4),39,42,54,74 while others asked whether respondents were vaccinated without specifying doses (42.9%, k = 3),64,70,73 and only one study examined receipt of the second dose (14.2%, k = 1). 74
All but one study examined vaccine behavior using only a binary variable for gender/sex, which we summarize first.39,42,54,70,73,74 A total of 7 studies examined differences between men and women in vaccine uptake using univariate analyses across 7 outcomes. In summary, 57.1%, or 4 of the 7 analyses (k = 3), found greater vaccine uptake among men compared to women,42,64,74 while one study (1 outcome), or 14.3% of 7 analyses, found greater vaccine uptake among women compared to men. 39 Finally, 28.5%, or 2 of the 7 analyses (k = 2), found no differences between men and women in COVID-19 vaccine uptake.54,73
A total of five studies examined differences between men and women in vaccine uptake using multivariate analyses across 6 outcomes. Most analyses (66.7%, 4 outcomes, k = 4) reported no differences between men and women in COVID-19 vaccine uptake.39,42,54,70 The only exception was Ioannou et al., 74 a study with Veterans Affairs (VA) enrollees, with mixed multivariate results; the study reported lower odds of receiving at least one dose of the vaccine among males compared to females, but females had higher odds of missing the second dose compared to males. 74 Similar to intentions, a visual overview is provided that showcases these findings in brief (symbols only) in Table S6.
Shaw et al. 64 was the only study to examine vaccine uptake beyond binary gender/sex categories (highlighted in Table S5). In their study of health care workers, they reported lower uptake of the vaccine among non-binary/gender not-disclosed employees compared to males and female employees (univariate analysis).
Subgroup Comparisons
The review authors attempted to draw conclusions based on the results, from within and across studies, about whether gender/sex differences in vaccine acceptance varied by sub-groups (e.g., age, race/ethnicity). Within studies, Green-McKenzie et al. 39 was the only study that examined interactions between gender/sex and other identities of interest, reporting on the effect of gender on vaccine uptake by health worker occupational category. No differences were found by gender among physicians, nurses, and health workers with some patient contact (technicians, therapists, nursing aides, and phlebotomists). However, for health workers with no patient contact (finance, coders, information technology, environmental and food services), females (72.6%) were less likely than males (79.1%) to receive the first vaccine dose (P < .001).
Across studies, 9 (17.0% of total studies) included samples of health workers and/or employees of health systems.29,33,35,37-39,53,56,64 The findings of these studies support greater intentions to vaccinate among men compared to women; which was the reported result for all (100%) of the 7 univariate and five multivariate analyses conducted in these studies. Only 2 studies with health workers/employees examined behavior, one supporting women’s greater vaccine uptake, 39 and the other supporting men’s greater uptake using univariate analyses. 64 No other homogeneous subpopulations (e.g. race/ethnicity) were represented in a sufficient number of studies to summarize and make conclusions about their findings separately.
Discussion
This scoping review provides an overview of the empirical literature that examined the relationship between gender/sex and COVID-19 vaccine intentions and uptake in approximately the first 2 years of the pandemic in U.S.-based samples of adults and adolescents. The search yielded 54 studies that examined this question – a reflection of the scientific community’s rapid response to conduct research to understand the COVID-19 pandemic. There were more studies that examined intentions than behavior, due to the timeframe of the scoping review and vaccine availability. Overall, approximately 3 quarters of all studies’ results (univariate and multivariate) support higher intentions to be vaccinated among men compared to women in the first years of the pandemic. Over half of analyses on vaccine uptake assessed through univariate analysis also favored greater uptake among men, but 2 thirds of multivariate analyses supported no gender/sex differences in vaccine uptake. Thus, while there was variation in both outcomes, the overall findings of the review support women’s lower vaccine acceptance in the first years of the pandemic in the U.S., but the findings are stronger for intentions than for behavior. Notably, few studies included transgender or non-binary populations and those that did had varying categories limiting our ability to make meaningful conclusions in this review.
Our results for differences between men and women could mean that hesitancy may not always translate into differences in men and women’s behavior, especially when other socio-demographic and related variables are considered. However, given the low number of studies examining uptake, more research is needed to strengthen these conclusions. Our findings align with the results of other reviews that have been published with similar aims. Systematic and scoping reviews on determinants of vaccine acceptance/hesitancy report being male as a prominent correlate of higher vaccine acceptance/willingness and lower hesitancy.14-17,19 Most reviews were conducted globally, and report that this finding is consistent across cultures (in the U.S. and other countries),15-18 although the only meta-analysis among them found variation by country. 14 Notably, within our review, one study with a repeated cross-sectional design and a nationally representative U.S. sample reported that women were more hesitant towards the COVID-19 vaccine than men, but vaccine hesitancy declined faster overtime in women compared to men, with gender differences no longer statistically significant by the final time period. 49 While we cannot say that this trend is occurring across studies in our review, it provides one possible explanation (i.e., that women’s hesitancy was high initially but reduced overtime) for this review’s support for women’s greater hesitancy but less support for a gender difference in actual vaccine behavior.
Our review’s findings can be considered against research that examines gender-specific reasons for vaccine hesitancy. Irrespective of gender, studies report the following among the main reasons for COVID-19 vaccine hesitancy: being against vaccines in general, concerns about safety and side effects, low risk perception specific to COVID-19 infection, public health/government mistrust, efficacy doubts, beliefs about current immunity. 18 In research that examines hesitancy by gender, women’s hesitancy has been more associated with circumspection (weighing of benefits and costs of taking a particular vaccine based on evolving information), and men’s with complacency (perceiving the risks of vaccine preventable diseases as low). 49 In addition, some of the most common side effect concerns among both women and men specific to COVID-19 relate to reproductive health and fertility77,78; with pregnant and breastfeeding women excluded from the early clinical trials, this may have been especially concerning for women of reproductive age.79,80 In addition, research with transgender individuals as part of the broader lesbian, gay, bisexual, transgender, queer, intersex, and asexual (LGBTQIA) community highlights unique barriers to COVID-19 vaccine uptake, such as medical trauma, misgendering, and fear of violence, underscoring the need for more research with this population. 81
In contrast to this review’s findings, the results of our companion review that examined gender/sex differences in social distancing, mask-wearing, and adherence to CDC guidelines more broadly found women’s greater engagement in these prevention behaviors compared to men, or no gender differences, but rarely supported men’s greater prevention behaviors compared to women (to be reported in a separate manuscript). These findings align with other literature grounded in gender theory positing that the socialization of men and women results in women’s greater health care engagement than men, shaped by gender norms that deem self-care and health-seeking as feminine behaviors.82,83 On the surface, this review’s findings might appear to contradict the gender norm and health behavior literature. However, women’s greater early hesitancy could be a reflection of women’s greater conscientiousness around health, making them more likely to weigh the risks and benefits of vaccination, but ultimately still adopt the behavior if deemed beneficial to health and due to their socialization to be agreeable and compliant.49,84
Further, gender theory posits that women and men are less likely to engage in behaviors that are considered a threat to their fulfillment of socially ascribed gender roles and norms.82,83 As such, engagement in preventative behaviors is theorized to be lower in men because they are counter to masculine norms, such as the idea that men should be tough and self-reliant.82,83 Vaccine intentions may be an exception to the typical gendered pattern of health-seeking behavior because fears around fertility and pregnancy outcomes are most threatening to the role of mother. Further, given norms of masculinity around risk-taking,85-87 men may have been more willing to take on the risks of a new experimental vaccine than women. Research is needed to explore how gender norms intersect with vaccine hesitancy. Cassino et al. 88 found that men and women who report adherence to the most traditional gender identities had significantly lower intentions to vaccinate against COVID-19 compared to their less rigid counterparts. Other studies that examine COVID-19 outcomes through the lens of adherence to traditional masculine/feminine norms similarly report strict adherence to associate with less prevention behavior.89-91 Future research should explore adherence to social structures of gender further, rather than just identification with binary categories of male/female or man/woman, in relation to vaccine hesitancy.
This review highlighted numerous gaps in the literature, which can inform future research, but are also important to consider as limitations to the extrapolation this review’s findings more broadly. First, most studies were cross-sectional designs. Thus, they capture a single point in time in the first 2 years of the pandemic. Since vaccine intentions and uptake are not static, but changing overtime, longitudinal studies on this topic would shed light on how hesitancy/uptake evolved over time by gender, especially as more data on vaccine efficacy, safety, etc. became available. In addition, most studies used non-random sampling, which reduces the likelihood of representative samples and introduces the risk of selection bias. Forty percent of studies were broadly with the U.S. population, but only a quarter of them used sampling or analytic methods to achieve population representation. In addition, the generalizability of the review’s finding specific to vaccine uptake is limited by the relatively small number of studies identified with that outcome, and most of those studies were limited in their reliance of self-reported measurements of vaccination (rather than clinic record extraction), which could introduce social desirability bias. In addition, few studies examined gender identity outside of binary definitions of woman/man or male/female. In those that did, differences were found, but the results were mixed and the studies too few to make meaningful conclusions. Future research and public health data need to include better defined measures of gender/sex that are inclusive of non-binary populations.
This review is also limited in its ability to make comparisons by subpopulations. Only one study did any sub-analysis to examine if gender/sex’s association with COVID-19 vaccine intentions/uptake differed by subpopulation. Given the large portion of studies whose samples were broadly geography-based (e.g., U.S. adults, residents of specific states), the review was limited in being able to make conclusions about differences by subpopulations across studies. If gender/sex differences were examined by factors such as race/ethnicity, age, or political affiliation, the findings might explain the variation identified across study results. The one group that was represented enough to make comparisons across studies were health care providers/employees of health systems, which largely supported greater vaccine hesitancy among women compared to men. Future research should be conducted that examines how gender affects COVID-19 vaccination across intersecting identities. Research on this topic could also benefit from the inclusion of qualitative methodologies, which were absent in the studies meeting our inclusion criteria, but that may have been a result of our inclusion criteria/research question requiring comparisons between groups.
Conclusions
Heirdari et al.
92
posit that the success of COVID-19 vaccine programs will require a gender transformative approach to address vaccine hesitancy and increase vaccine acceptance and access, arguing that these factors are gendered and shaped by gender norms. This scoping review supports their argument by highlighting the important role gender/sex plays in health seeking behavior specific to COVID-19 vaccination. Overall, the studies included in this review provided evidence to support more hesitancy among women, and some support for gender differences in vaccine uptake among U.S. samples in the first 2 years of the pandemic, but there was variation in both outcomes. Transgender and gender diverse populations were largely missing in the analyses included in this review, highlighting the need for more research with these populations and better-defined measures of gender/sex that are inclusive of non-binary populations. This review also highlights the need for more research in this area, especially research employing rigorous research designs and exploring context and population-specific differences in, and drivers of, hesitancy and uptake. The findings of this review highlight the need for the development of tailored, gender sensitive vaccine campaigns; additional research is needed to inform the content of such programs, so that they can address the core drivers of hesitancy across the gender spectrum. In the United States, there are significant gender disparities in COVID-19 outcomes. Prior research suggests women may be more hesitant to vaccinate than men, and gender diverse populations face unique barriers to COVID-19 vaccination. This is the first study to synthesize the literature on gender differences in COVID-19 vaccine acceptance in the United States. Women may have been more hesitant to get the vaccine than men early in the pandemic, but findings were mixed on whether these differences may translate to actual behavior. The review highlights a gap in research inclusive of gender diverse individuals and a need for more rigorous designs. Future research should include gender diverse populations, explore gender differences by sub-populations, utilize more rigorous designs, and test gender-sensitive public health campaigns to mitigate vaccine concerns.So What?
What is already known on this topic?
What does this article add?
What are the implications for health promotion practice or research?
Supplemental Material
Supplemental Material - A Scoping Review on Gender/Sex Differences in COVID-19 Vaccine Intentions and Uptake in the United States
Supplemental Material for A Scoping Review on Gender/Sex Differences in COVID-19 Vaccine Intentions and Uptake in the United States by Katelyn M. Sileo, Inara M. Hirani, Rebecca L. Luttinen, Matt Hayward, and Paul J. Fleming
Supplemental Material
Supplemental Material - A Scoping Review on Gender/Sex Differences in COVID-19 Vaccine Intentions and Uptake in the United States
Supplemental Material for A Scoping Review on Gender/Sex Differences in COVID-19 Vaccine Intentions and Uptake in the United States by Katelyn M. Sileo, Inara M. Hirani, Rebecca L. Luttinen, Matt Hayward, and Paul J. Fleming
Ethical Statement
Ethical approval
This review does not constitute human subjects research.
Footnotes
Acknowledgments
The authors acknowledge and thank Suyapa Muñoz for assistance in the screening of studies.
Author Contributions
KMS conceptualized the aims of the review with input from PJF. KMS developed the review protocol, with input from all review authors. KMS and MH developed the search terms and MH ran the search. KMS, IMH, and RLL screened all studies by abstract, full text, and extracted the data. KMS, IMH, and RLL synthesized the results. KMS and IMH led the writing of the manuscript. All review authors contributed to the writing, review, and editing of the manuscript and consent to be authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Katelyn M. Sileo was supported by a Mentored Research Scientist Career Development Award from the National Institute of Mental Health of the National Institutes of Health [K01MH121663]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Correction (November 2023):
This article was updated to correct the article type to Literature Review.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.