
Abstract
Purpose
The purpose of this study is to refine and establish measures of multilevel barriers and facilitators to HIV testing and PrEP for Latino sexual minority men (LSMM).
Design
Cross-sectional measure validation.
Setting
Participants from Miami, FL.
Subjects
290 LSMM from the DÍMELO study.
Measures
Based on prior qualitative work, we developed two measures that evaluated multiple determinants (i.e., barriers and facilitators) to (1) HIV testing and (2) PrEP use.
Analysis
All measures included in this analysis assessed a set of theoretically distinct barriers and facilitators. We performed 11 exploratory factor analyses (EFA) to assess the dimensionality of theoretical groupings of items informed by prior qualitative work, including: knowledge, perceived need and benefit, mistrust and concerns, stigma and normalization, cultural competence, navigation support, provider demeanor, clinic and medical system issues, privacy concerns, cost, and language and immigration barriers. Based on EFA results, we conducted two confirmatory factor analyses (CFA), one for each measure.
Results
Within each measure, the 11 EFAs extracted 10 barrier factors and 7 facilitator factors. The CFAs for HIV testing and PrEP measures were consistent, such that all models retained the structures identified in the EFAs.
Conclusion
Findings support the use of these measures with LSMM. These measures can inform multilevel implementation strategies for health promotion professionals to scale up and disseminate HIV prevention services to LSMM.
Purpose
Despite improvements in HIV prevention and treatment implementation, HIV continues to disproportionately affect marginalized groups. Specifically, sexual minority men (SMM; e.g., gay, bisexual, men who have sex with men) and Latinos are subgroups who face HIV-related health inequities. In 2019, 29% of new HIV diagnoses occurred among Latina/o/x 1 individuals 2 and 70% among SMM. These disparities intersect for Latino SMM (LSMM). Since 2015, HIV incidence among LSMM has steadily increased whereas incidence has decreased among non-Latino White SMM. 2 In South Florida, an epicenter of the U.S. HIV epidemic, 3 LSMM made up approximately half of all new HIV diagnoses, 4 making this a key population for health promotion professionals to focus their HIV prevention efforts.
Social and structural determinants of health and syndemic factors explain HIV disparities among sexual and ethnic minority groups. Syndemic theory suggests that co-occurring epidemics (e.g., depression, HIV) synergistically work together to exacerbate health challenges among affected groups. In the context of HIV, factors such as substance use, mental health, and trauma are syndemic conditions that are associated with increased behavioral vulnerability for HIV transmission among people who experience these conditions. 5 Additionally, structural factors associated with socioeconomic marginalization such as poverty, suboptimal access to health insurance, housing instability, and a history of incarceration are barriers to engaging in HIV prevention services among racial, ethnic, and sexual minorities.6-8 These social determinants and syndemic factors limit access to HIV prevention and treatment tools such as HIV testing and pre-exposure prophylaxis (PrEP). 9 There is an urgent need for professionals in health promotion disciplines to support efforts to disseminate evidence-based HIV prevention tools to populations most impacted by HIV to achieve Ending the HIV Epidemic goals in the United States. 10 Yet, with the number of potentially distinct social determinants and syndemic factors that could affect these dissemination efforts, it is important to provide tools to health promotion professionals to assess the most important determinants (i.e., barriers and facilitators), which in turn can inform prioritizing which determinants to act on within these dissemination efforts.
For LSMM, barriers and facilitators to utilizing preventative health services may be unique due to cultural factors. Latina/o/x individuals may be more inclined to provide emotional, psychological, and even physical support to their own family members than outside the family unit for assistance regarding health challenges due to factors such as familismo (obligation to family) and personalismo (warm, caring relationships with others). 11 On the one hand, these cultural values may be barriers such that LSMM may internalize values like familismo and, in turn, sacrifice their own health and well-being needs to maintain familial harmony. 11 In this case, cultural values could perpetuate internalized and interpersonal stigma toward HIV prevention services (e.g., PrEP, HIV testing) and potentially decrease LSMM’s likelihood to initiate services. 12 Alternatively, cultural values could serve as facilitators. For instance, familial or relational support for getting preventive services could uniquely influence LSMM’s decisions to uptake these preventive services. 13
Although many factors, as discussed above, could impede or promote LSMM's use of HIV prevention services, there are no quantitative measures, to the authors’ knowledge, that can be used by health promotion professionals to comprehensively assess and directly compare and prioritize barriers and facilitators to HIV prevention. Therefore, a quantitative assessment of multilevel factors that can either be obstacles (i.e., barriers) or leverage points (i.e., facilitators) to HIV prevention can be a useful tool for health promotion professionals to determine which to prioritize mitigating or leveraging within health promotion efforts to engage LSMM in HIV testing and PrEP. Because quantitative measurement tools can be used both longitudinally and across different populations, they are often employed to collect data that is then used to guide future public health practice and policy development. Therefore, this gap in measures of multilevel barriers and facilitators of HIV prevention services is of major concern, because it limits health promotion professionals from systematically and comprehensively assessing, and in turn addressing, constructs that have potential to greatly influence HIV prevention service utilization among LSMM.
To begin to fill the gap in multilevel measures of HIV testing and PrEP use barriers and facilitators, our team conducted qualitative interviews with 28 LSMM with varying degrees of engagement in HIV prevention services and 10 stakeholders with experience delivering HIV prevention and behavioral health services to LSMM. 14 Through this qualitative work, we identified multilevel barriers and facilitators to accessing HIV prevention services for LSMM. Drawing from our qualitative findings regarding these multilevel barriers and facilitators, as well as existing theory (e.g., syndemics, minority stress, and intersectionality theories)13,14 we developed quantitative measures of multilevel barriers and facilitators of LSMM’s HIV testing and PrEP use. Given the dearth of measures that assess multilevel barriers and facilitators of HIV testing and PrEP that are also culturally grounded in LSMM’s lived experiences, the purpose of this study is to examine the psychometric properties of our measures of multilevel barriers and facilitators to HIV testing and PrEP for LSMM, thereby promoting their potential use among health promotion professionals and researchers.
Methods
Sample
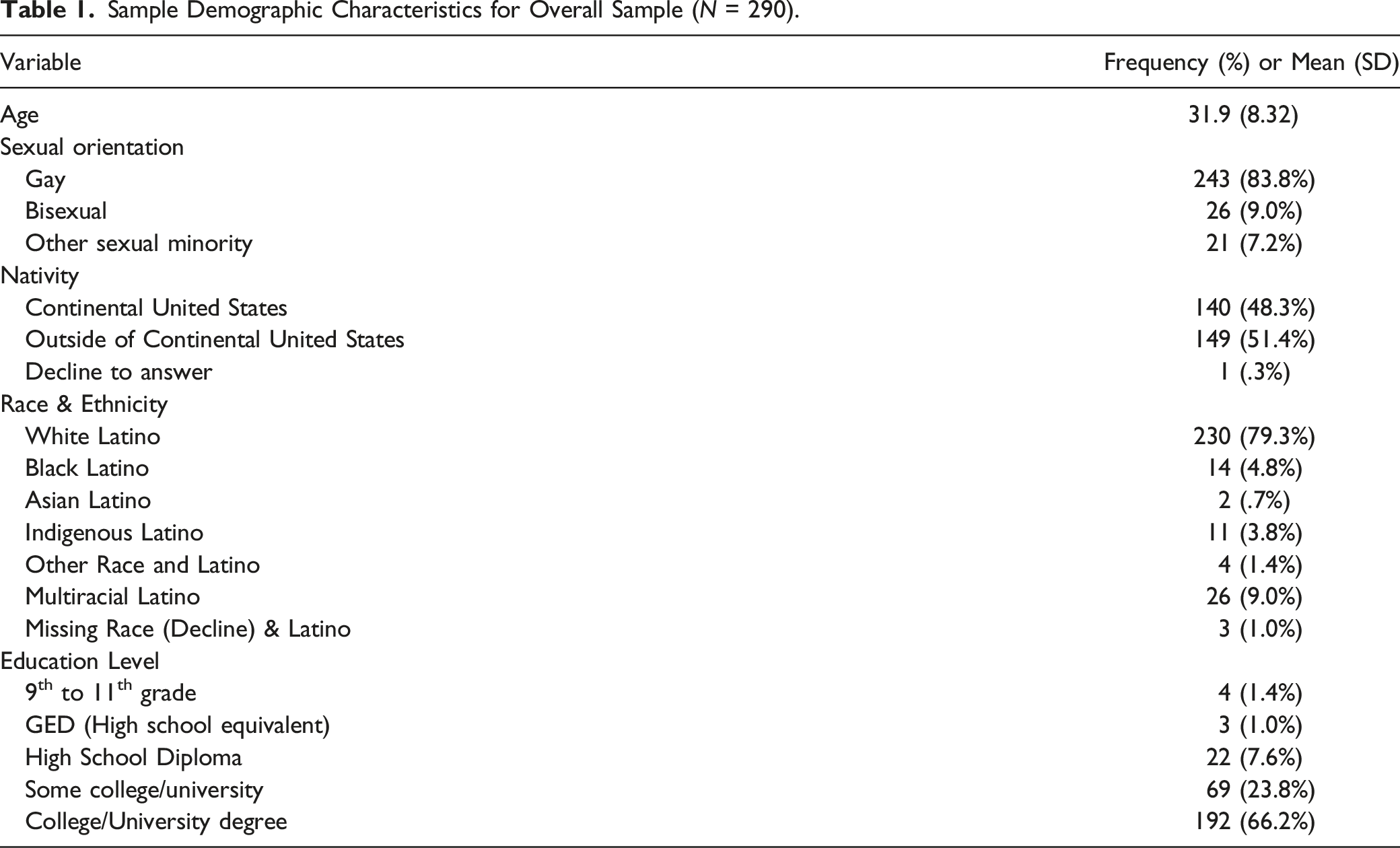
The study included 290 LSMM who participated in the DÍMELO study, a cohort study evaluating LSMM’s engagement in evidence-based HIV prevention and behavioral health services. Eligible participants were LSMM between the ages of 18-60, lived in the greater Miami, FL area, and reported being HIV-negative or unknown HIV status. Complete participant demographics are reported in the main outcome paper for the parent study. 13 The [MASKED FOR REVIEW] Institutional Review Board approved this study with a waiver of signed consent (No. 20181006). Participants reviewed consent information within REDCap, where the study was administered, and clicked a box indicating consent to participate.
Measures
Sample Demographic Characteristics for Overall Sample (N = 290).
Multilevel Barriers and Facilitators to HIV Testing and PrEP
Informed directly by our prior qualitative work with LSMM in South Florida, 14 we developed measures of 1) multilevel barriers and facilitators to PrEP use and 2) multilevel barriers and facilitators to HIV testing among LSMM. Each measure evaluated a set of theoretically derived barriers and facilitators to PrEP use and HIV testing, that were selected based on our prior qualitative work and related theory (i.e., syndemic, minority stress, intersectionality theories). We intentionally created measures that were comprehensive; and therefore, contained numerous items to ensure that the theoretical domains identified from our qualitative work were assessed. The multilevel barriers and facilitators to PrEP use measure contained 49 barrier items and 29 facilitator items. The multilevel barriers and facilitators to HIV testing measure contained 46 barrier items and 28 facilitator items. Sample barrier items included, “Concerns about side effects or negative effects of PrEP” and “Not knowing that HIV testing services exist.” Facilitator items included, “PrEP being available for free or low cost” and “Someone helping me figure out where to go for HIV testing.” Participants rated all barriers from 1 (didn’t get in the way of using the service at all) to 5 (completely got in the way of using the service). All facilitators were rated from 1 (didn’t or wouldn’t help me get the service at all) to 5 (completely did or would help me get the service). Of note, we developed these measures with the idea that the measures would not produce an “overall” multilevel barriers and facilitators scale; rather, as with our qualitative work, we anticipated that the measures would be scored within their theoretical domains (e.g., producing a score for degree of cost-related barriers, immigration-related barriers, etc.). Measures were first written in English, then translated to Spanish using an established three-step translation process (forward translation, back translation, and comparison of original to back translated version). 15
Analysis
Below is an outline of the steps in our analytic plan. Our goal within the manuscript is to describe the analytic plan in an accessible way for all readers. For readers interested in additional technical details, please see the Technical Appendix (Supplementary File 1).
Step 1: Determine Theoretical Groupings
The multilevel barriers and facilitators to PrEP use and HIV testing measures were developed based on our prior qualitative work. 14 As noted above, we did not develop these measures with the expectation that they would yield one overall score; rather, we expected that the measures, would yield scores within the theoretical domains identified in our qualitative work. As such, we used the findings from our prior qualitative study to group the items within each of our measures (in other words, the theoretical item groupings directly map onto our prior qualitative findings). The resulting theoretical groupings of items for both measures included: (1) knowledge, (2) perceived need and benefit, (3) mistrust and concerns, (4) stigma and normalization, (5) cultural competence, (6) navigation support, (7) provider demeanor, (8) clinic and medical system issues, (9) privacy concerns, (10) cost, and (11) language and immigration barriers. Therefore, we expected to derive scores within each of these theoretical groupings, not at the overall measure level.
Step 2: Conduct Exploratory Factor Analyses
Exploratory factor analysis (EFA) is useful when minimal research has been conducted regarding the structure of a construct or measure, as was the case in this study. Because we had 11 theoretical groups of items per measure, we conducted 11 exploratory factor analyses (EFAs) for the multilevel barriers and facilitators to PrEP measure and the multilevel barriers and facilitators to HIV testing measure (i.e., one EFA was performed for each theoretical domain – for example, one EFA was run for the “knowledge” domain on the multilevel barriers and facilitators to PrEP measure, one EFA was run for the “perceived need and benefit domain of the multilevel barriers and facilitators to PrEP measure, and so on). It would not be possible to run one large EFA for each of the measures because some of the theoretically derived groupings would not be associated with each other. If the EFA was unidimensional, meaning that all items in the domain “hung together,” the theoretical grouping became a scale. If the EFA was multidimensional, meaning that the items were grouped into two subgroups that “hung together,” the theoretical grouping became two scales.
Step 3: Conduct Confirmatory Factor Analyses
Confirmatory factor analysis (CFA) can be subsequently used to evaluate if the structure(s) that emerged from the EFA are consistent in an independent sample. We conducted the CFAs based on the results of the EFAs.
Results
Exploratory Factor Analyses
Multilevel Barriers and Facilitators to PrEP Measure
PrEP EFA.

aTheoretically derived domains are based on our prior qualitative work. 14
bParticipants rated all barriers from 1 (didn’t get in the way of using the service at all) to 5 (completely got in the way of using the service). All facilitators were rated from 1 (didn’t or wouldn’t help me get the service at all) to 5 (completely did or would help me get the service).
cItems removed from model. Information for preceding items is after model was respecified.
Multilevel Barriers and Facilitators to HIV Testing Measure
HIV Testing EFA.

aTheoretically derived domains are based on our prior qualitative work. 14
bParticipants rated all barriers from 1 (didn’t get in the way of using the service at all) to 5 (completely got in the way of using the service). All facilitators were rated from 1 (didn’t or wouldn’t help me get the service at all) to 5 (completely did or would help me get the service).
cItems removed from model. Information for preceding items is after model was respecified.
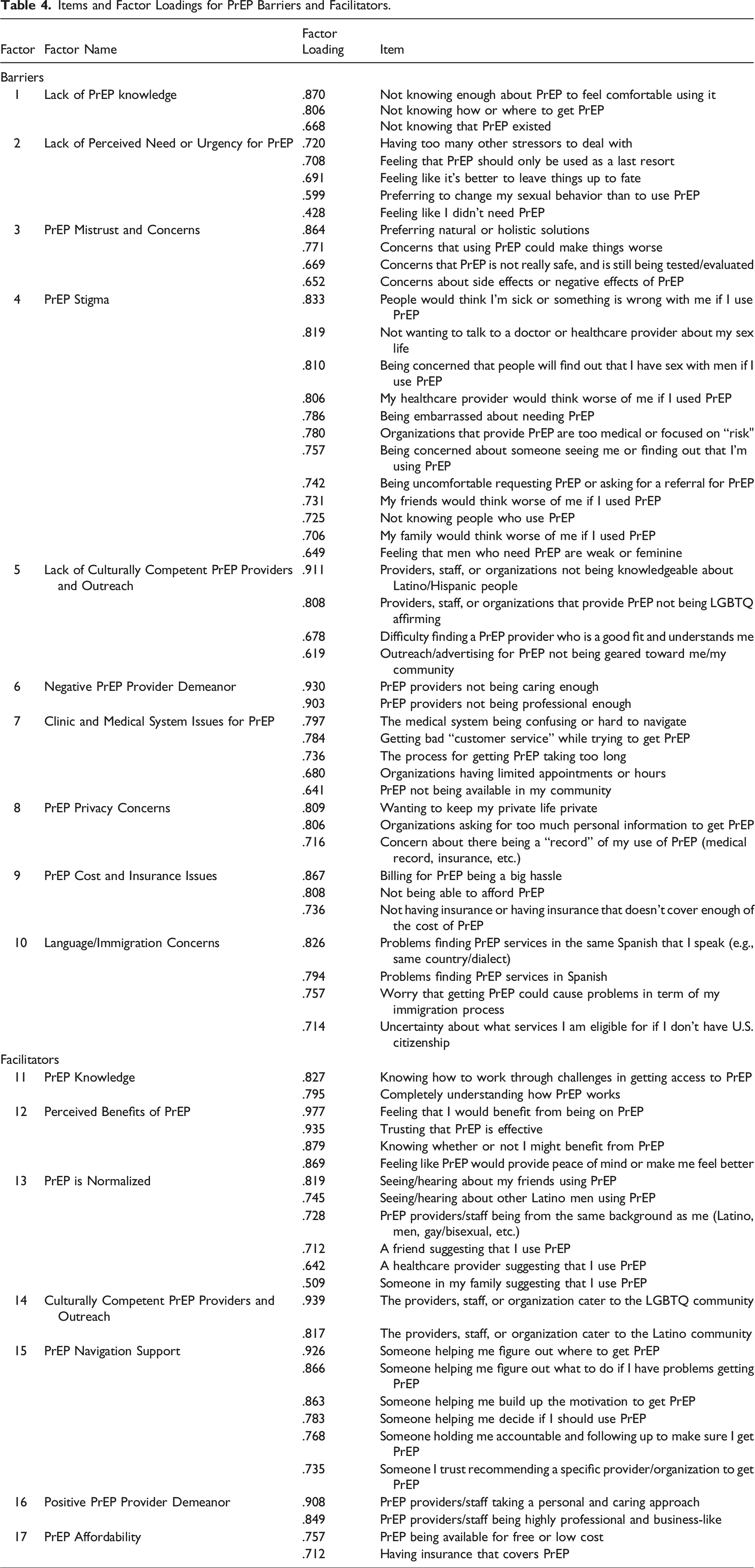
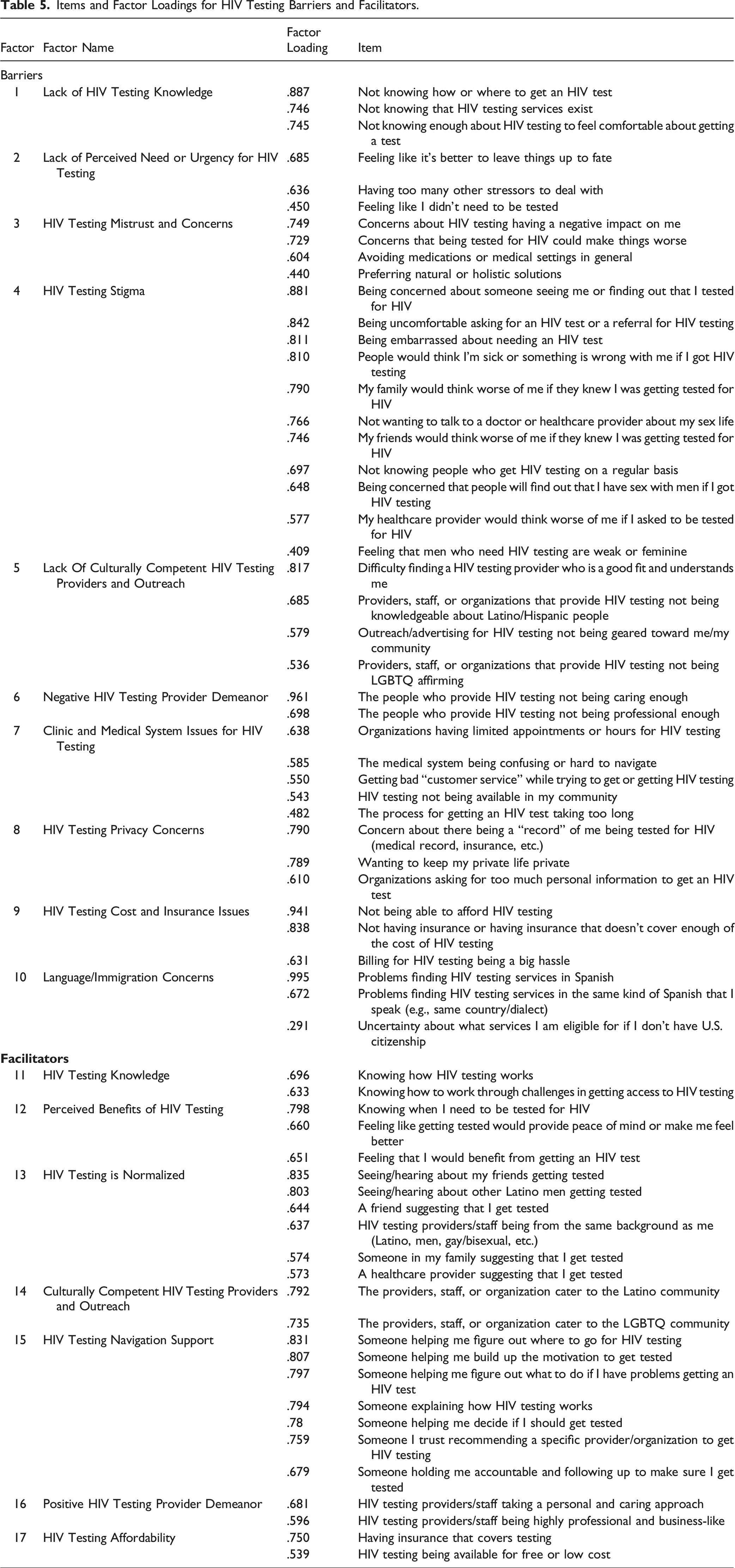
Confirmatory Factor Analyses
Items and Factor Loadings for PrEP Barriers and Facilitators.
Items and Factor Loadings for HIV Testing Barriers and Facilitators.
Discussion
The results of this study contribute to the existing literature by establishing the psychometric properties of the multilevel barriers and facilitators to PrEP and HIV testing measures, developed based on qualitative work with LSMM. This is critical to advancing health promotion practice and research because this type of measure comprehensively evaluates both facilitators and barriers to critical prevention services, allowing practitioners and researchers to prioritize among many different potential determinants. We found consistency in the factors (i.e., scales) for each of the measures such that barriers and facilitators for both PrEP and HIV testing were similar. These findings provide evidence for measures of multilevel, culturally grounded determinants of PrEP and HIV testing that may be used among LSMM. The final and complete Multilevel Barriers and Facilitators to PrEP Measure and Multilevel Barriers and Facilitators to HIV Testing Measure can be found in Supplementary File 2.
The measures evaluated in the current study are multilevel, meaning that they assess discrete barriers and facilitators at the individual, interpersonal, and cultural/structural level that could positively or negatively affect LSMM’s PrEP use and HIV testing behaviors. These multilevel measures do not yield overall scores; rather, they serve to provide health promotion professionals and researchers with a quantitative assessment of different types of obstacles (i.e., barriers) and leverage points (i.e., facilitators) to engaging LSMM in HIV prevention across multiple levels of influence. This approach is consistent with the National Institute on Minority Health and Health Disparities Research Framework, which encourages research to document and address multilevel determinants in order to reduce health disparities. 16 Tools such as the Multilevel Barriers and Facilitators to PrEP and HIV Testing measures can help health promotion professionals to decide which factors, within multiple levels (i.e., system/cultural-, interpersonal-, and individual-level), to target. Health promotion professionals are often required to make difficult choices about where to focus their efforts; these measures can help in ensuring that the most important and influential determinants are targeted through health promotion efforts.
A barrier for LSMM was related to PrEP and HIV testing stigma. Items within the stigma scale (in both the PrEP and HIV testing measures) were related to LSMM’s concerns that they would be perceived as weak or feminine, that something was wrong with them, or that others may find out that they have sex with men if they were to pursue these services. Even if LSMM are seeking HIV prevention services, internalized and interpersonal stigma may impede them from accessing HIV prevention care.17,18 Provider cultural competence was also a key determinant for both measures and may relate to the stigma that LSMM encounter; it may be difficult for LSMM to find a PrEP/HIV testing provider who is a good fit for them because they may not be LGBTQ affirming and/or may not be knowledgeable about LSMM. 19 By administering the measure, stigma at the interpersonal-level and cultural competence at the structural-level may arise as factors deterring LSMM from obtaining PrEP services. As a response, a health promotion tactic may be to develop stigma reduction campaigns and/or cultural training.
Other pervasive system-level barriers for LSMM were related to clinic and medical system issues. LSMM may have even more trouble accessing HIV testing/PrEP when organizations have limited appointments or hours, when the process takes too long, and when the medical system is difficult to navigate. Notably, for both PrEP and HIV testing, items which indicated that services may not be available in the LSMM communities were included in both models, highlighting the lack of systems in place to provide HIV prevention services to LSMM. Collectively, our findings suggest the importance of thinking beyond individual-level influences on engagement (e.g., knowledge, perceived need) when developing health promotion interventions.
Importantly, these measures also identified language and immigration-related barriers to PrEP and HIV testing among LSMM as a unified set of items. In our prior qualitative work, LSMM in South Florida noted that strategies to equitably scale up HIV prevention services should be available in multiple languages, most importantly, Spanish and English. 19 Additionally, LSMM’s immigration status should be considered with regard to engagement in HIV prevention services; research has shown that a fear of deportation had an indirect effect on reduced HIV testing among Latina/o/x individuals. 20 in practice, it may be useful in some settings for health promotion professionals to determine whether higher scores on this factor are driven more by language, immigration, or both when using the findings to inform their work.
Existing literature on PrEP and HIV testing determinants often focuses on factors that impede engagement. Contributing to the literature, our measures also include culturally grounded PrEP and HIV testing facilitators. Among the facilitator scales identified in our analyses was “perceived need and/or benefit”, a facilitating factor found within both the PrEP and HIV testing measures. Items in this scale reflected the degree to which LSMM perceived that they would benefit from using PrEP or getting an HIV test or if they felt that receiving PrEP or getting an HIV test would provide them with peace of mind. This is consistent with prior literature showing that men who have sex with men (MSM) of color identified belief in the benefit of knowing one’s HIV status as a factor that can increase general HIV testing uptake. 21
Many PrEP and HIV testing outreach campaigns target perceived risk (i.e., a loss prevention message) rather than perceived benefits (i.e., a health promotion message) 22 which may be a missed opportunity in engaging LSMM in HIV prevention efforts. To the degree that perceived benefits is rated as an influential facilitator for LSMM in a given setting, this suggests the need to develop programs and campaigns that leverage this health promotion mentality rather than a risk prevention perspective. For instance, campaigns that underscore the positive benefits of being on PrEP and getting HIV testing, rather than messaging the negative outcomes of not getting PrEP or HIV testing may have a greater likelihood in engaging LSMM in HIV prevention services.
Additionally, the navigation support factor, again found in both the HIV testing and PrEP measures, highlights the importance of evaluating whether LSMM have someone who can provide suggestions and/or support throughout the process of engaging in HIV testing and/or PrEP services. In fact, in our prior quantitative work with LSMM in South Florida, we found that this PrEP Navigation Support scale was positively associated with LSMM’s engagement in PrEP services. 13 Patient navigation is a frequently used and implemented health promotion program to enhance PrEP uptake, and our findings suggest the relevance and need for this type of programming particularly for LSMM.
This study is not without limitations. First, the data used in this secondary analysis are cross-sectional; it is possible that the factors identified may vary as a function of time and might be confounded by additional factors such as immigration status. Future studies should examine these factors longitudinally and consider additional influences that are specific to LSMM which may impact uptake of these services. Although we have found in our prior work that some of the scales in the multilevel barriers and facilitators to PrEP measure are associated with PrEP engagement among LSMM 13 (e.g., PrEP mistrust and concerns was negatively associated with PrEP engagement and PrEP Navigation Support was positively associated with PrEP engagement, suggesting predictive validity), future studies should examine how the multilevel barrier and facilitator HIV testing and PrEP measures predict HIV and PrEP related outcomes. Second, due to the narrow geographical area of the sample, results can only be generalized to LSMM living in South Florida. These measures should be validated in other geographic areas and explore whether these measures are consistent among LSMM living in other HIV epicenters and within Latina/o/x’s more broadly. Relatedly, our sample of LSMM may not be generalizable to national samples of LSMM because approximately two-thirds of participants obtained college and/or other degrees; this suggests the need to validate the measures with a more nationally representative group of LSMM. Third, issues with bias (e.g., desirability, recall, selection) should also be considered due to the self-report nature of the survey data collection. Fourth, given the size of the half-sample utilized for the EFAs (n = 152), the HIV knowledge EFA was under-identified and was conducted on the full study sample, however, the results were consistent with the results of the PrEP knowledge EFA and the CFA confirmed the extracted structures. Similarly, although the ratio of items to subject size was large, models still had good fit to the data. Future studies with larger samples of LSMM should replicate this finding. Finally, given that the items were theoretically grouped together, but in groupings that would not necessarily be associated with each other, it would not be possible to run one large EFA analysis for the entire measure.
However, there are notable strengths. Foremost, this study contributed to the establishment of much-needed multilevel measures that are culturally grounded (through our prior qualitative work) in LSMM’s lived experiences. Although further research is needed to validate the measures more broadly, our study contributes an essential starting point. This study allowed us to examine the psychometric properties of measures of multilevel barriers and facilitators to HIV testing and PrEP for use among LSMM. The fact that the results were similar across both HIV testing and PrEP also speaks to the consistency of the results and measures. This ensures that when developing multilevel health promotion programs and outreach campaigns to increase uptake of HIV prevention services among LSMM, health promotion professionals can tailor their efforts to the most relevant barriers and facilitators, which is key in resource limited contexts. These measures provide insights into a breadth of domains that capture several different barriers and facilitators of HIV testing and PrEP use among LSMM and can subsequently inform health promotion professionals’ efforts to increase uptake of such services.
HIV prevention tools such as HIV testing and PrEP are insufficiently disseminated to Latino sexual minority men (LSMM). Yet, few measures exist to evaluate these multilevel barriers and facilitators and inform health promotion practice efforts. Evidence supporting the psychometric properties of the multilevel barriers and facilitators to PrEP and HIV testing measures, suggesting the utility of these measures in health promotion practice and research settings. The Multilevel Barriers and Facilitators to HIV testing and PrEP measures can be used among health promotion professionals to provide a quantitative assessment of system/cultural-, interpersonal-, and individual-level factors that can be obstacles (i.e., barriers) or leverage points (i.e., facilitators) to engaging LSMM in HIV prevention. This can subsequently inform health promotion program development, ensuring that the key facilitators and barriers are targeted.SO WHAT?
What is already known on this topic?
What does this article add?
What are the implications for health promotion practice or research?
Supplemental Material
Supplemental Material - Refining Multilevel Barrier and Facilitator Measures for HIV Testing and PrEP Among Latino Sexual Minority Men
Supplemental Material for Refining Multilevel Barrier and Facilitator Measures for HIV Testing and PrEP Among Latino Sexual Minority Men by Alyssa Lozano, Elliott R. Weinstein, Alejandra Fernandez, Sierra Bainter, Pranusha Atuluru, Abigail Hurtado, Vanessa Morales, Guillermo Prado, Steve A. Safren, and Audrey Harkness in American Journal of Health Promotion.
Supplemental Material
Supplemental Material - Refining Multilevel Barrier and Facilitator Measures for HIV Testing and PrEP Among Latino Sexual Minority Men
Supplemental Material for Refining Multilevel Barrier and Facilitator Measures for HIV Testing and PrEP Among Latino Sexual Minority Men by Alyssa Lozano, Elliott R. Weinstein, Alejandra Fernandez, Sierra Bainter, Pranusha Atuluru, Abigail Hurtado, Vanessa Morales, Guillermo Prado, Steve A. Safren, and Audrey Harkness in American Journal of Health Promotion.
Footnotes
Author Contributions
All authors met the four ICMJE requirements for authorship. All authors made substantial contributions to the conception or design of the work, the acquisition, analysis, or interpretation of data for the work, drafted the work or revised it critically for important intellectual content, approved the final version to be published, and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Safren receives royalties for books published by Guilford Press, Oxford University Press, and Springer/Humana Press. No other potential conflict of interest was reported by the authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research reported in this publication was supported by the Center for AIDS Research (CFAR) at the University of Miami under Award Number P30AI073961 (Pawha), the National Institute on Minority Health and Health Disparities under Award Number U54MD002266 (Behar-Zusman) and K23MD015690 (Harkness), and the National Institute of Mental Health under Award Number P30MH116867 (Safren). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Ethics Statement
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.