
Abstract
Purpose
Evidence suggests differential impacts of community development, including gentrification and displacement. Public health practitioners and advocates are key stakeholders involved in the community development process related to active living, yet little is known about their perceptions of its impacts. We explored the perspectives of relevant leaders of public health departments and key community and advocacy organizations on community development, gentrification, and displacement.
Approach
Purposive key informant interviews.
Setting
CDC State Physical Activity and Nutrition (SPAN) funding recipients.
Participants
CDC SPAN recipient leadership (n = 10 of 16) and advocacy organizations they partnered with (n = 7 of 16).
Method
Interviews were recorded, transcribed, coded, and thematically analyzed with direct quotes representing key themes.
Results
Both groups felt community development held important benefits, specifically by creating healthy living opportunities, but also potentially leading to the displacement of long-time residents. Practitioners reported the benefits were for all community members, whereas advocates noted the benefits were seen in those with privilege, and the consequences were disproportionately seen in disadvantaged communities. Both mentioned the importance and difficulty of getting diverse representation for community engagement.
Conclusions
Learning how key stakeholders perceive and navigate the community development process can help inform recommendations for better equity in active living community improvements. More work is needed to further elucidate best practices for health and social equity in the community development process.
Purpose
Community development has been described as a means to elicit social, economic, political, and environmental change in communities in response to dismal conditions and areas in decline. 1 Community development strategies may be federally funded initiatives such as Community Development Block Grants, but can also be driven by community members or non-profit organizations. 2 Historically, these strategies have focused on improving social and economic outcomes, 3 typically in the form of ensuring housing and providing social services. Recently, there has been a shift in focus on community development as a way to support healthy living.2,4,5 This support is realized through addressing the social determinants of health– the conditions in which people live, learn, work, and play which affect health. 6 Specifically, community development may help to ensure that community members are able to have control over their living environment and have empowerment over the social factors that influence their lives (eg, housing, employment, hopefulness). 7
Another process by which community development can influence health is through improvements in the neighborhood environment; which have consistently been shown to be associated with reduced obesity8-12 as well as promoting physical activity behaviors.13,14 In order to maintain healthier lifestyles and create sustainable opportunities for community members to be physically active, recent evidence-based recommendations include strategies such as changes in community design that make neighborhoods more supportive of active living.15-18 These are illustrated by the Task Force on Community Preventive Services recommendation for built environment approaches that combine improvements in transportation such as sidewalks, bicycle lanes, and expanded public transit, with land use and community design changes such as improved parks and recreation facilities and mixed-use development that enable housing in proximity to destinations such as businesses and schools. 19 Broadly, these recommendations may be characterized as smart growth strategies which encourage a mix of building types, and housing and transportation options to promote active living and community engagement. 20 A key example of expanded transportation options includes the implementation of complete streets policies which require streets to be accessible to users of all ages, and of all modes of transport. 21 These built environment recommendations are in line with the idea that where people live and play has the biggest influence on how long and how well they live.22-24
However, there is too often an inequitable distribution of opportunities for healthy behaviors in certain communities (eg, people with lower incomes, or people from racial and ethnic minority groups) that also have higher rates of physical inactivity and related chronic diseases.25,26 Historically, these communities have been underserved and disinvested in both structurally and systematically. Zoning and land use policies including historic redlining have helped to widen health disparities in communities of color.27-29 As such, there is increasing interest in community initiatives to improve access to healthy environments for low-income neighborhoods and communities of color, and promote health equity. Health equity means not only reducing/eliminating health disparities, but also achieving social justice and equalizing opportunities to be active and lead longer healthier lives. 30 Though community groups including advocacy organizations have sought more equitable neighborhood development. Only recently has there been historic investments in infrastructure to help benefit all communities including the Justice40 Initiative, Bipartisan Infrastructure Law, and American Rescue Plan .31-33 However, an unintended consequence of these community initiatives may be decreased affordability and gentrification of neighborhoods. 34 The Urban Displacement Project defines gentrification as “a process of neighborhood change that includes economic change in a historically disinvested neighborhood —by means of real estate investment and new higher-income residents moving in - as well as demographic change - not only in terms of income level, but also in terms of changes in the education level or racial make-up of residents.” 35 The historical disinvestment in an area experiencing gentrification may amplify existing socioeconomic inequalities and potentially increase health disparities among residents.36-38 This is highlighted by a recent systematic review on the health impacts of gentrification, which found that people with lower incomes and Black persons suffered negative effects of gentrification including mental health issues and poor self-rated health. 39
Furthermore, a key negative outcome associated with gentrification is displacement of long-term residents. There are clear social and economic impacts of displacement such as a loss of social networks, housing stability, and educational opportunity.40,41 Similar to gentrification, displacement may lead to negative health effects for marginalized communities. This is partially due to a loss of resources or social capital that can lead to negative health behaviors. For example, displacement may lead to lower accessibility to healthy food options or transportation choices.37,42 Additionally, displacement of residents may lead to loss of health care access as well as an increase in mental health issues.43,44
In order for community development strategies to be effective and benefit the intended communities, several studies have highlighted the importance of building community partnerships and collaboration between key stakeholders such as health departments, advocacy organizations, and community members.45-48 These stakeholders may play an important role in community development, including decision making power, but less is known about perceptions of community development, gentrification, and displacement from these key stakeholders involved in community development related to active living. The current study will explore the perspectives of relevant leaders of public health departments and key community and advocacy organizations on community development, gentrification, and displacement.
Approach
To develop the most relevant questions for the key informant interviews, a literature review was conducted exploring the relationship between community development strategies and physical activity, as relevant stakeholders focus on community development as it relates to active living. Language and themes from this review, along with recent studies related to perceptions of community development and displacement were used to develop a list of questions and a draft interview guide.37,49 The guide was developed to assess general perceptions of community development including impact of community development, and perceptions of gentrification and displacement, including potential mitigation or prevention strategies for both. The guide was pilot tested with a former health department employee and a current advocate who had relevant contextual experience, which resulted in minor changes in wording, but no substantive thematic revisions.
Setting
The CDC’s current State Physical Activity and Nutrition (SPAN) Program 50 funding recipients (2019 – 2024) were used as a sampling frame of public health practitioners who represented all regions across the United States and that we were certain were working around community development related to active living. As part of the SPAN program, the “CDC funds 16 state recipients to implement evidence-based strategies at state and local levels to improve nutrition and physical activity,” with most states employing strategies related to infrastructure for active living. Examples of SPAN funded projects include the introduction of a bike share program, safe streets initiatives, and the development of bike and pedestrian trails and paths. We invited the principal investigator or director of each state’s SPAN program to participate. From this list, we identified key advocacy organizations that worked with the SPAN program recipients on active living related work, including on engagement with community members or implementation of programs.
Participants
Two interviewers were trained to conduct interviews on video. Training included topics on conducting, coding, and analyzing interviews. Practice sessions and read throughs were also held prior to interviewing with participants. All interviewees had prior experience conducting interviews with public health practitioners as part of a research study. Members of the research team (NS, LS) sent emails to 32 potential key informants (16 public health practitioners, 16 active living advocates) to request participation in a video interview. Each interviewee conducted at least 4 interviews with the other interviewee present to ensure consistency in delivery. Participants who agreed to the study were interviewed over video chat with videos on for both the interviewer and interviewee, at times/days convenient to their schedule. Interviews were conducted across February and March of 2021. This project was approved by the Institutional Review Board of the sponsoring institution. All methods were carried out in accordance with relevant guidelines and regulations. Verbal informed consent was obtained from all participants prior to the start of the video interviews. Interviews were audio recorded and professionally transcribed. Interviewer notes supplemented the transcriptions.
Method
A codebook was developed to facilitate analysis of the transcripts. Two members of the research team (NS, LS) read over the same 4 transcripts and came up with a draft list of code categories. They then had a discussion of these codes and refined the list. Using this new list, both team members coded 1 transcript in detail to ensure consistent interpretation of the coding schemes. Two team members coded each transcript using constant comparative coding methodology, 51 and a pursuant discussion on the coded documents rectified any discordance. Once all transcripts were coded and discussed, text within each code was grouped and thematically summarized. Direct quotes were used to represent the main themes that emerged.
Results
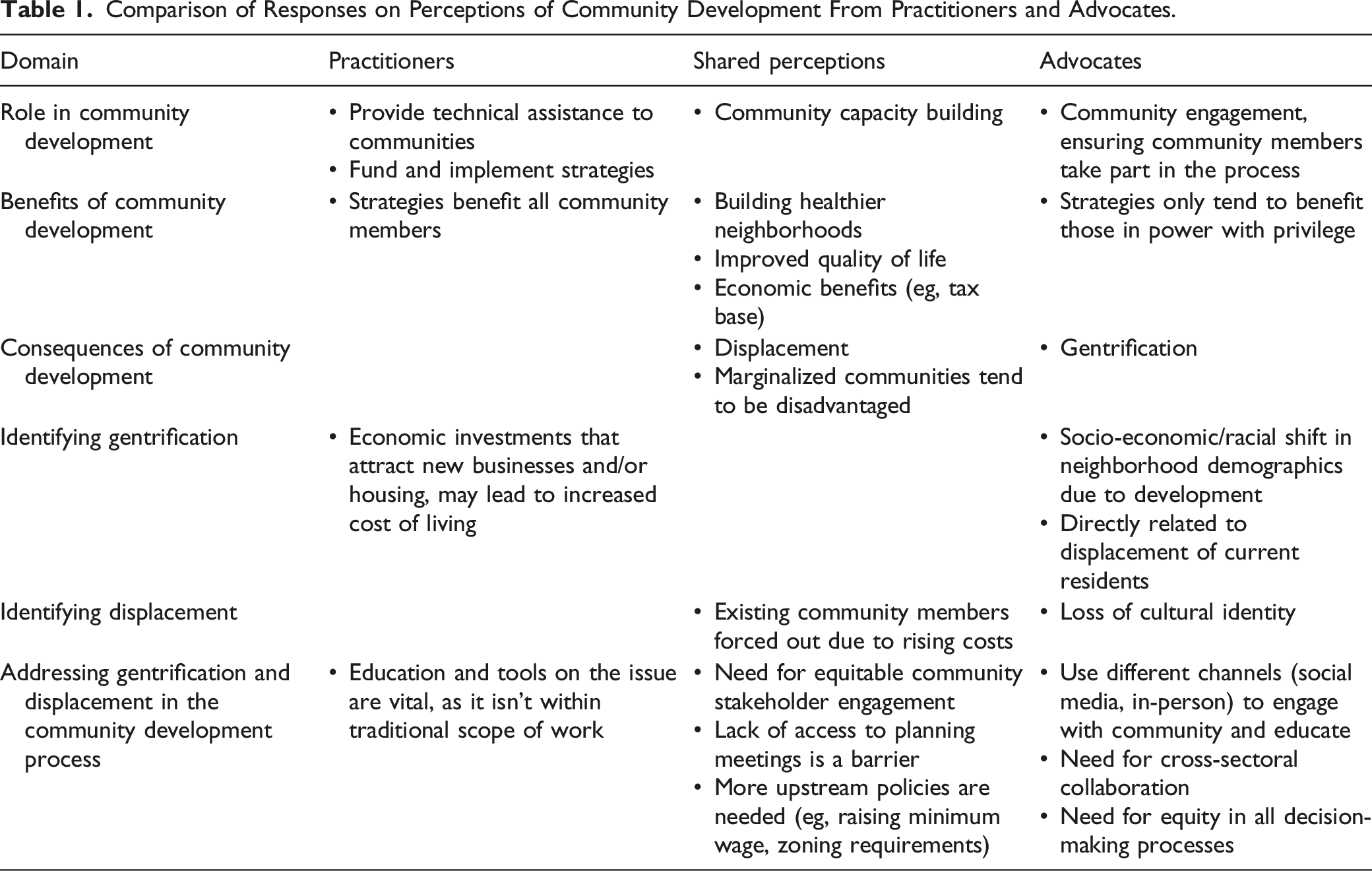
Comparison of Responses on Perceptions of Community Development From Practitioners and Advocates.
The Impacts of Community Development
Both practitioners and advocates felt they had a vital role in the community development process. This included a role in building up capacity for communities to be involved in the community development process, while also ensuring their input was considered throughout. However, there were some key differences in how advocates and practitioners viewed their roles in the community development process. Practitioners reported more often than advocates that they provide technical assistance (eg, health impact assessments, data analysis), and play a significant role in the actual community development process (ie, what community development projects are being funded or implemented). Advocates noted more often than practitioners that they participate in community engagement and ensuring community members play an active role in the community development process. “the work that we do is related to primarily implementing or encouraging strategies around policy system and environmental changes within local communities” -Practitioner # 5 “we do a lot of turning people out to local planning meetings about different projects that are happening, different planning processes, that kind of thing. And also educating and building the grassroots capacity for people to engage in those processes.” -Advocate # 1
Perceived Benefits and Beneficiaries of Community Development
When considering the benefits and consequences of community development there were notable similarities between practitioners and advocates. Both groups considered the building of healthier neighborhoods (eg, creating walking/biking trails, increased fresh food accessibility, transportation systems), improved quality of life, and increased property values/tax base to be a benefit. However, there was a sharp contrast on who each group felt benefited from this development. Practitioners asserted that through their process of community development everyone shared or should share the benefits, whereas advocates considered developers and those community members with privilege, power, or political ties to be the beneficiaries of community development. “in really purposeful community development that's equity driven, you would hope that it's the community that benefits from it” -Practitioner #4 “So the people who benefit are inevitably like those who have power and voice, and that looks different in different places.” -Advocate #2
Perceived Consequences and Disadvantaged Communities of Community Development
Practitioners and advocates agreed that displacement, including the loss of culture in a neighborhood, is a potential consequence of community development. However, practitioners mentioned gentrification as a consequence less often than advocates, who talked about it as a consequence if it led to displacement. Both felt that traditionally marginalized communities including people with lower incomes, those from racial and ethnic minority groups, and people with disabilities were the groups who were disadvantaged by community development; and commented on the fact that they may not have a role or voice in the process. “If you go in converting neighborhoods from low value to high value, and let's bring in some more business or let's improve the housing, and then you nudge out the folks who live there and work there, we lose some of that community's history, and culture, and the social capital that was there. It gets pushed out to be replaced by something that maybe is a little more palatable to the general public.” -Practitioner # 6 “So I don't necessarily think gentrification is negative if it doesn't lead to displacement. However, if gentrification leads to displacement, that's when I think the gentrification is bad.” -Advocate # 4 “poor folks and black and brown people and young folks, older people, immigrants, people living with disabilities, all these folks I would say are probably disadvantaged, when they're also the ones who stand to benefit the most from good investment in community development.” -Advocate # 2
Gentrification and Displacement
When asked to define gentrification, practitioners noted it as economic investment in a community that attracts new businesses and/or housing that raises the cost of living in the community. A general theme among practitioners was that this economic investment improves the existing community, though there was mention that it is probably for newer and wealthier residents. Advocates defined gentrification as a socioeconomic and racial shift in a neighborhood demographics due to development. Advocacy groups, more often than practitioners, incorporated displacement in their definition of gentrification, either directly or indirectly. Though these groups identified these communities as likely to be low-income and/or from racial and ethnic minority groups, their language used fewer negative connotations when compared to the practitioners (eg, “rundown, low value”) “you might have a rundown neighborhood and then some developers decide that they like it and they're going to invest in it…with the intention that because of that, it's making this neighborhood better” -Practitioner # 2 “it quickly turns into what was a lower middle class income neighborhood is filled with primarily a richer neighborhood often more homogenous and less diverse” -Advocate # 1
Both defined displacement as a process whereby existing community members are forced out due to being unable to afford to continue to live in this community. Advocacy groups talked more about the demographic changes and loss of cultural identity (ie, changes in the history and diversity of a neighborhood, including its social capital in response to gentrification) than did practitioners. “Gentrification 2.0, we've finally done it. We've booted people out because they can't afford to live where they've always lived and again it is such an interesting thing that there aren't in many cases intentional efforts to move people out of a location” -Practitioner # 1 “like the loss of the cultural identity and people who grew up in a neighborhood and it no longer feels like home. So there's also just that also just social hostility that comes along with that kind of change” -Advocate # 3
Solutions for Successful Community Development and Anti-Displacement
Both practitioners and advocates identified lack of equitable community stakeholder engagement in the planning process as a barrier to ensuring community development benefits those who need it most. This includes traditionally marginalized communities. Both groups identified a lack of access to planning meetings due to time, location, or technology as the primary barrier to community stakeholder engagement. These issues were identified in connection with the lack of diverse representation in community engagement in connection with community development. “making sure that all the right partners are at the table. So you talked about making sure we’re connecting to the community, which I think can be more challenging than we think. We sometimes think we have partners at the table, but there’s probably partners and people that either don’t, haven’t been reached or are reluctant to be reached by a State Health department” -Practitioner # 3
Practitioners also identified developers’ focus on profits, limitations on their scope of work, and un-representative local government as barriers. They also described that their role in working with communities was to “lend a voice,” “guide,” or as a “connector,” but admitted to not having control over displacement. Advocates identified use of social media and holding meetings at locations convenient for community members as facilitators to community engagement. Advocates also identified support of local government and education of community members as other overall facilitators of equitable community development. However, they also mentioned lack of cross-sectoral collaboration as barrier. “it's about process, taking the time and having the respect for the history of a neighborhood and for the experiences that people have had in that neighborhood, especially low-income black neighborhoods that have a traumatic history when it comes to development, it comes to how they were treated” -Advocate # 5 “I feel like the planning process is so short, it's really not designed to get meaningful public input. It’s designed for developers to just get their project off the ground as quickly as possible” -Advocate # 1
Practitioners mentioned governmental stakeholders in the community development process ranging from various levels including local, Tribal, and Federal. Most practitioners who identified government as a stakeholder also mentioned specific entities within their health departments whose work focuses on community development (eg, “Center for Community Capacity Development,” “State Department of Economic and Community Development”). Advocates were more likely to talk about local or city-level government and did not address Federal-level government. Advocates also discussed a wider range of stakeholders than did practitioners, which included unions, colleges, and faith-based organizations. “There’s a lot of distrust within that community and then you add in, here’s the county commissioner and here's the state government and here’s the federal government that it just becomes this tug of war between resources and policy…” -Practitioner # 1 “we primarily work with community organizations, so it might be other advocacy based organizations, transportation organizations, political action committees, also RCOs which are residential community organizations. And so lots of neighborhoods, neighborhood organizations, and also nonprofits.” -Advocate # 7
In addition, both groups discussed potential solutions for displacement. Practitioners and advocates both identified upstream policies,
52
which address the social determinants of health of communities as the predominant strategies for both mitigating and preventing displacement. Practitioners identified policies, such as raising minimum wage or requiring developers to build low-income housing, as well as improving equity within impacted communities to be potential mitigation strategies. Advocates identified policies such as supporting transportation infrastructure and changes to property tax. Additional non-policy mitigation strategies include ensuring equity in the development process and educating communities on planning decisions and issues regarding affordable housing All prevention strategies identified by advocates fall within the upstream policies category, including control of prices (rental, property taxes, utilities), requiring racial equity assessments, and policies that regulate development. Overall, both groups considered this to be a challenging issue. “making sure that there’s plans for affordable housing in any type of development that’s proposed… You can't leave it up to the corporation. So it has to be government policies” -Practitioner # 4 “focusing more on process, equity in the process and decision making process as our policy… It’s who has power in setting the agenda and controlling resources…how are we going about setting our advocacy agenda and whose voice matters in that? So it’s building the infrastructure and trust and relationships and processes to make sure that our work is being driven by people who are most impacted. And that we have a clear understanding of who we’re talking about when we say that” -Advocate # 6
Conclusions
These findings provide insight into the perspectives of community development, including the unintended consequences such as displacement, from 2 key stakeholder groups relevant to active living opportunities. As studies have highlighted the necessity of stakeholder collaboration in the community development process,53-55 it is important to understand perspectives from these groups.
Both practitioners and advocates in this study discussed playing an important role in the community development process. Practitioners more often described having a key role in the actual process (ie, implementing and funding community development) whereas advocates more often noted their participation in community engagement. Both groups felt community development held important benefits, specifically by creating healthy living opportunities for being physically active and eating healthy, while also potentially leading to the displacement of longtime residents. This finding is similar to other studies showing the potential health benefits of community development strategies, including the benefits of increased active living opportunities.56-59 Additionally, this study resonates with other evidence highlighting the potential harm caused by the gentrification of neighborhoods.36,39,60 However, practitioners reiterated that benefits were intended for
Both practitioners and advocates understood gentrification as a change in the demographic breakdown of a neighborhood, but the practitioners’ perspective focused on development and economic change whereas advocates focused on the demographic and cultural changes (ie, changes in cultural identity) occurring. While the original coining of the phrase “gentrification” focused on class, these thoughts of participants are in line with contemporary definitions particularly in the U.S. context, which tend to include both class and racialized components, in addition to a recognition of structural socioeconomic complexities.60,61 Both groups also noted gentrification may lead to the displacement of long-term residents of a neighborhood, but advocates more often highlighted the potential resultant cultural changes. This is consistent with a publication highlighting the impacts of gentrification on the health of legacy or long term residents. 62 These impacts can both directly and indirectly impact health. Direct impacts may include housing instability, loss of social networks, and a loss of social capital and resources connected to a neighborhood.40,41 Indirect impacts may be related to a disconnection to one’s neighborhood and resources, including the potential to move to neighborhoods with lower access to healthy food options or transportation choices.37,42 Both direct and indirect impacts from gentrification may also be harmful for mental health, potentially leading to financial stress and anxiety.43,44
A common theme in both groups was the need for community development to be “done right.” However, practitioners and advocates had different ways of framing this. Both felt the need for equitable strategies that combated the lack of diverse community engagement throughout the entire community development process. Both also mentioned the difficulty in getting diverse representation for community engagement. Practitioners discussed this as if it was out of their control (mainly up to governments or developers), whereas advocates actively discussed solutions for getting engagement from a more diverse group of community members that included marginalized communities. This may be part of the reason why practitioners focused on developers and federal government as being key stakeholders in this process whereas advocates also discussed a diverse group of neighborhood and community organizations.
Several studies have highlighted this need for community engagement throughout the community development process, as well as the need for cross-sectoral collaboration.53,63,64 Additionally, to ensure community development and community health benefits for the intended communities it is important to consider engagement with communities, but also consideration of the different systems or sectors that are involved (eg, Housing, Transportation, Planning). 65 This can even occur prior to community development implementation. Prior to a major redevelopment of San Francisco’s largest public housing site (Sunnydale), researchers and community developers engaged with the community to understand what was important to them. 66 Similarly, 1 study described the importance of improving communication between researchers and advocates with policymakers, including the translation of evidence. 67 This can help bring up barriers or issues before they would even occur. A possible solution to issues involving community engagement may be the use of community engaged data collection methodologies such as citizen science. 68 Citizen science involves public participation in research that can be beneficial for communities by increasing research capacity, but perhaps more importantly by providing better knowledge and benefits to community members. 69 These techniques may better address participation barriers related to transportation and childcare, location, and times of day among other factors. Though cross-sectoral coalitions and collaborations are vital for the implementation of evidence based programs or policies, it is also important to note that long term funding is necessary for the sustainability and success of such coalitions. 70
When discussing how to combat displacement, both groups perceived mitigation and prevention of displacement as connected to more upstream policies having to do with developers, local governments, and affordable housing. This is consistent with current toolkits to combat displacement, which suggest that displacement is only an issue of affordable housing.35,71 However, advocates also noted that ensuring an equitable community development process would help against issues of displacement (and gentrification), highlighting that more could be done outside of only providing affordable housing options.
Limitations and Strengths
Limitations of the present study include the use of a purposive, convenience sample in recruiting public health practitioners and advocates. However, this allowed the authors to recruit a sample from different regions of the United States that had a key role in active living related community development. Still, community development is a process that includes a variety of sectors and stakeholders including transportation, housing, urban planning, social policy, among others. Though this study captures unique and important perspectives, there is more to be understood from these other sectors. Another limitation was the small sample (n = 2) of interviewees piloting the interview guide. A plan was put in place to amend the interview guide during initial study interviews; however, it became clear that this was not necessary.
Among the strengths of the study, it is among the first to gain perspectives of the community development process from key stakeholders. This may help inform policymakers and others in decision making roles how to best communicate and engage with practitioners and advocates. A lack of social, economic, and political context is a key challenge in promoting health equity within communities.
72
This paper identifies some gaps in how communities are perceived by key stakeholders, and the need for knowledge on how to best engage with community members in the community development process. Community development strategies are useful tools that can benefit community members, but this benefit may not be equitable for all, especially disadvantaging traditionally marginalized community members. Understanding how practitioners and advocates navigate the community development process provides insight to help ensure it is an equitable process. More work is needed to further elucidate best practices for health and social equity in the community development process. Both groups identify displacement as an issue of concern but suggest that more context and understanding is needed to combat it. Future studies should explore perspectives across a variety of sectors such as transportation, housing, and urban planning in order to better understand the system in which community development operates in. This may help to inform more equitable implementation of community development strategies, including protecting against gentrification and displacement.So What?
What is Already Known on the Topic?
What Does This Article Add?
What are the Implications for Health Promotion Practice or Research?
Ethical Statement
Ethical Approval
This study was approved by the Institutional Review Board of Washington University in St. Louis (IRB#202101013).
Footnotes
Acknowledgments
The authors would like to thank Rodrigo Reis, Deborah Salvo, and Joseph Steensma for their constant feedback; as well as Linda Dix and Mary Adams for their administrative support.
Author Contribution
Study conception and design, N.S. and A.E.; Preparation of data collection materials, N.S., A.E., L.S., Data collection, N.S. and L.S., Analysis and interpretation of results N.S., A.E., L.S., R.B., Draft manuscript preparation N.S., A.E., L.S., R.B.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The lead author was supported by a National Cancer Institute training grant (T32CA057699). The findings and conclusions in this paper are those of the authors and do not necessarily represent the official positions of the National Institutes of Health.