
Abstract
Purpose
To examine differences in lifestyle behavioral and psychosocial factors between rural African American women with Class 3 obesity and those with overweight, and Class 1-2 obesity.
Design
Cross-sectional study.
Setting
Rural Southeastern United States.
Subjects
Participants included 289 African American women with a mean age of 56 years, 66% with a high school education or less, and a mean body mass index (BMI) of 38.6 kg/m2; 35% (n = 102) were classified with Class 3 obesity.
Measures
We objectively measured height, weight, and physical activity steps/day. Self-reported dietary and physical activity behaviors, general health-related quality of life, mental health, and social support were measured with validated surveys.
Analysis
Chi-Square analysis for categorical variables and analysis of variance (ANOVA) – via multiple linear regression – for continuous variables.
Results
There were no significant demographic differences between BMI groups, except for age, where women with Class 3 obesity were on average younger (51 vs 58 y, P < .001). Although dietary behaviors did not differ significantly between groups, we observed significant group differences in self-reported and objective measures of physical activity. The age-adjusted difference in means for self-reported total physical activity minutes/wk. was 91 minutes, with women categorized with Class 3 obesity reporting significantly fewer weekly minutes than those with overweight/Class 1-2 obesity (64.3 vs 156.4 min/wk. respectively, P < .01). Among psychosocial variables, only in the physical component scores of health-related quality of life did we find significant group differences – lower physical well-being among women with Class 3 obesity compared to those with overweight/Class 1-2 obesity (P = .02).
Conclusion
For African American women with Class 3 obesity living in rural setting, these findings suggest behavioral weight loss interventions may need to target physical activity strategies that address physical, psychosocial, and environmental barriers.
Keywords
Purpose
Rural African American women (AAW) experience the highest prevalence of Class 3 obesity (Body mass index (BMI) ≥ 40 kg/m2; 15.5%) compared to other women (9.8%), men (5.5%), or those living in urban areas (4.1% to 6.2%). 1 Higher rates of severe obesity translate into higher rates of adverse health outcomes (e.g., diabetes, hypertension, and certain cancers). Hence, AAW living in rural or non-metropolitan areas are at greatest risk for developing chronic diseases associated with obesity-related status. [NOTE: Throughout this paper we use “person/people first language” 2 (i.e. adults living with or affected by the chronic disease of obesity) and clinical categorizations (i.e., obesity Class 1-3). The authors recognize that the word “obesity” may be stigmatizing when used as a personal characterization rather than a clinical description of a chronic disease. The word “obesity” is not used when speaking to clients or patients. This report solely uses “obesity” as a clinical or diagnostic term.]
Research demonstrates that the obesity burden can effectively be addressed by behavioral weight loss programs3-5 that promote modest weight loss through healthy lifestyle changes.6,7 Rural AAW are underrepresented in behavioral weight loss intervention research;8,9 with few programs have including AAW with severe obesity.10,11 Existing data from high quality weight loss intervention research consistently shows that AAW do not lose as much weight as other groups.12,13 Most weight loss studies have included participants in the overweight category (BMI 25 to 29.9 kg/m2) and obesity Classes 1 and 2 (BMI 30-39.9 kg/m2),14,15 providing limited evidence of their effectiveness among individuals with Class 3 obesity. [NOTE: An alternative obesity reduction approach—bariatric surgery—has been shown effective for severe obesity, but evidence suggests that it may not be a viable treatment for AAW due to economic barriers and cultural concerns].16-18
In this exploratory study, we examine differences in selected lifestyle behavioral and psychosocial factors between AAW with Class 3 obesity and those in overweight, and Class 1 & 2 obesity categories living in rural Southeastern United States (US). Our research question focused on identifying if rural women with Class 3 obesity differed meaningfully in dietary and physical activity (PA) behaviors and related their psychosocial factors. Given the exploratory nature of this cross-sectional research, we aim to provide potentially valuable insights into designing behavioral weight loss interventions that fit the needs of AAW with severe obesity living in rural communities.
Methods
Sample
The Heart Healthy Lenoir (HHL) Project (previously described in detail)19,20 aimed to create long-term, sustainable approaches to reducing cardiovascular disease (CVD) risk disparities in Lenoir County, North Carolina – a rural, low-income county in eastern North Carolina. HHL included three coordinated studies: The Lifestyle Study (ClinicalTrials.gov number: NCT01433484), The Hypertension Control Study (ClinicalTrials.gov number: NCT01425515), and The Genomics Study. The Lifestyle Study was a community-based randomized controlled trial evaluating a dietary, PA and weight loss intervention. 20 The Hypertension Control Study was a clinic-based randomized controlled trial evaluating a medication and lifestyle management intervention for patients with poorly controlled high blood pressure. Written informed consent was obtained from all participants included in the study. The study was approved and monitored by the Institutional Review Board.
For the present study, our analytic cohort included baseline HHL Lifestyle and Hypertension Control Study data.
Measures
Validated questionnaires were administered at baseline.
Analysis
Chi-Square analysis was used to assess differences between the two BMI groups for categorical variables. Analysis of variance (ANOVA) – via multiple linear regression (MLR) to adjust for covariates – was used to assess the differences for all continuous variables. Potential demographic covariates such as age, gender, education, and income were selected a priori based on a review of the literature.21,29 Data were analyzed using SAS version 9.3 (SAS Institute, Cary, NC). The significance level was set at .05.
Results
Participant characteristics.
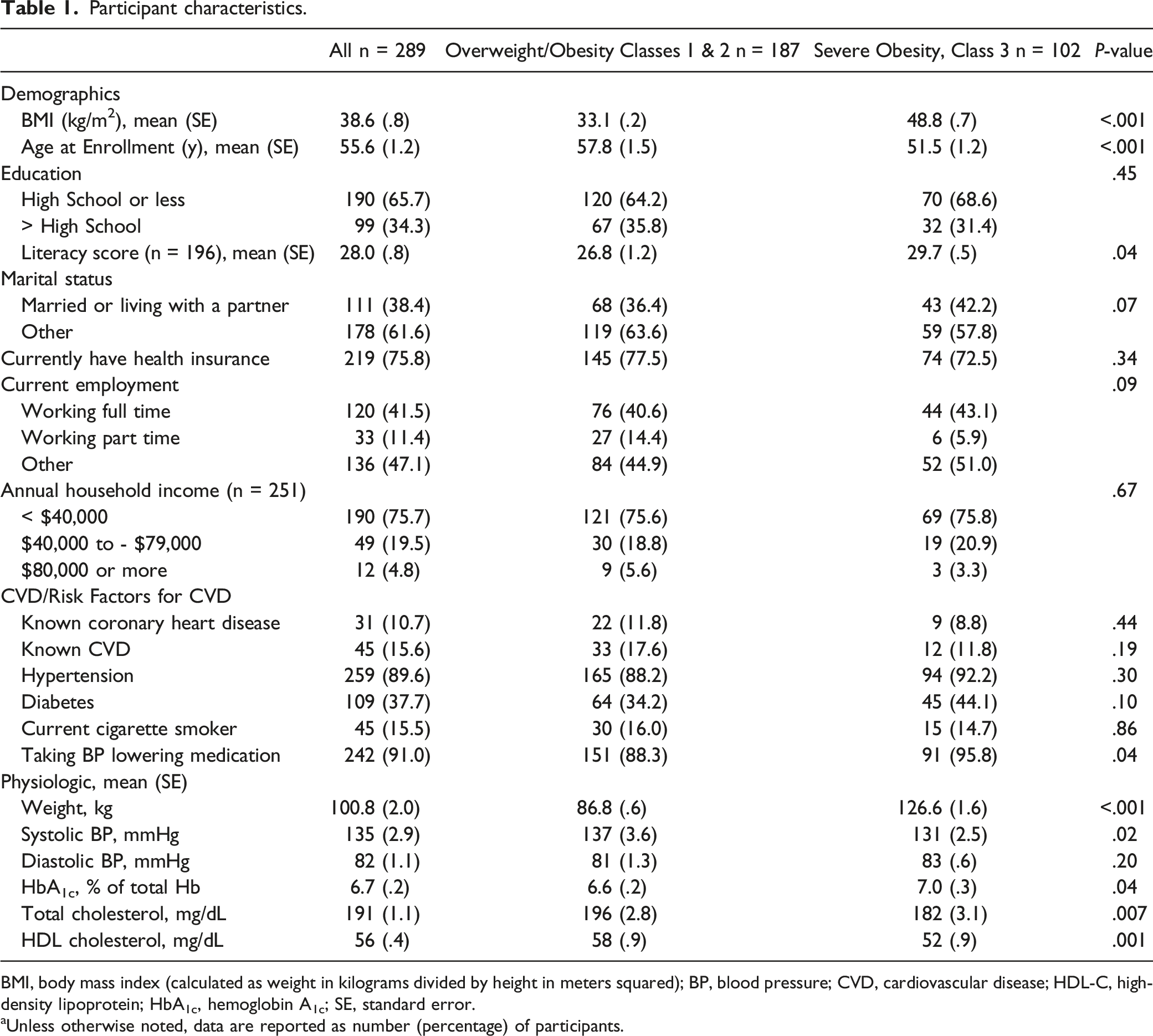
BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); BP, blood pressure; CVD, cardiovascular disease; HDL-C, high-density lipoprotein; HbA1c, hemoglobin A1c; SE, standard error.
aUnless otherwise noted, data are reported as number (percentage) of participants.
Crude and adjusted means for diet and physical activity behaviors among lifestyle study participants (n = 289). a
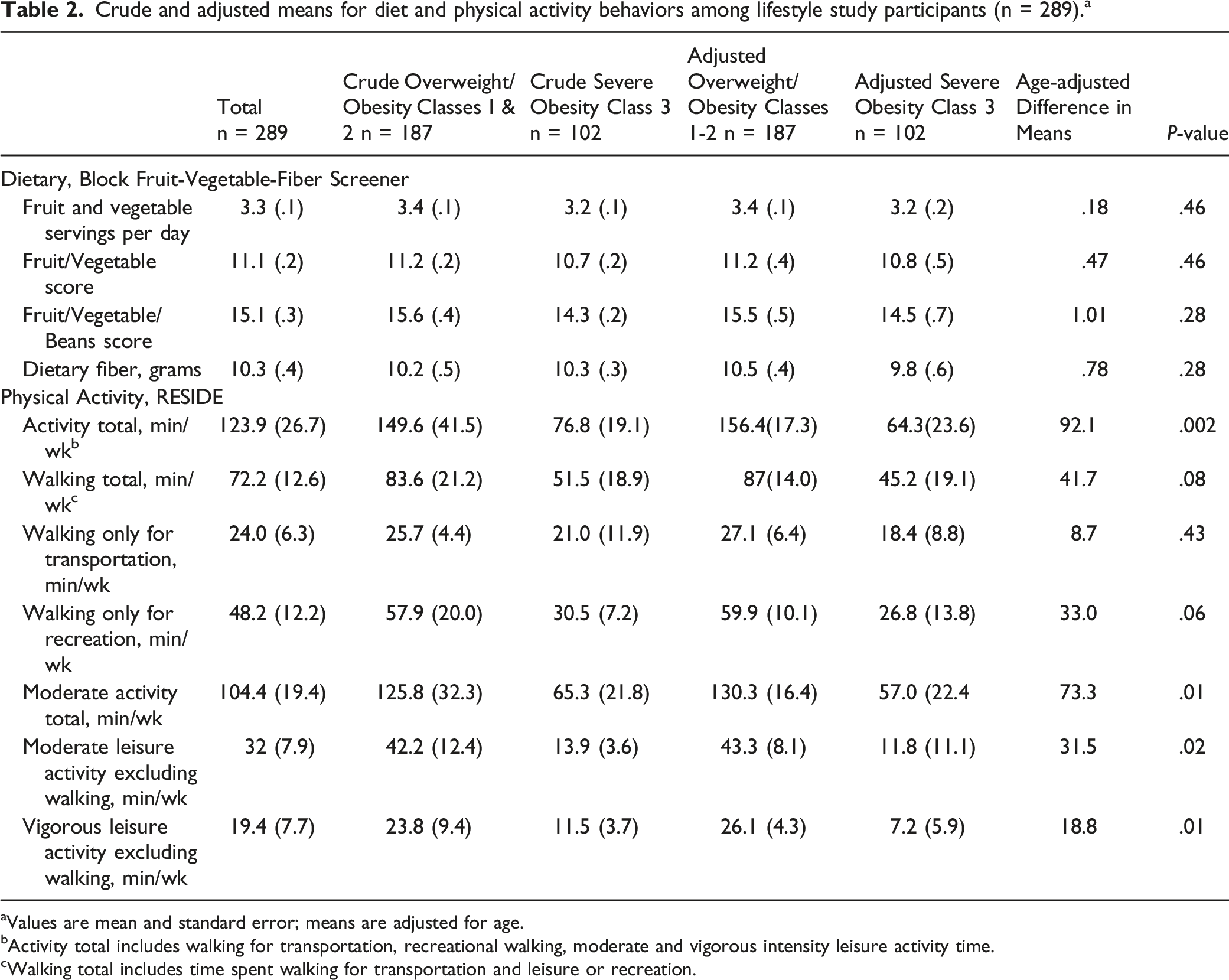
aValues are mean and standard error; means are adjusted for age.
bActivity total includes walking for transportation, recreational walking, moderate and vigorous intensity leisure activity time.
cWalking total includes time spent walking for transportation and leisure or recreation.
Crude and Adjusted Means for Social support, physical health, and mental health measures. a
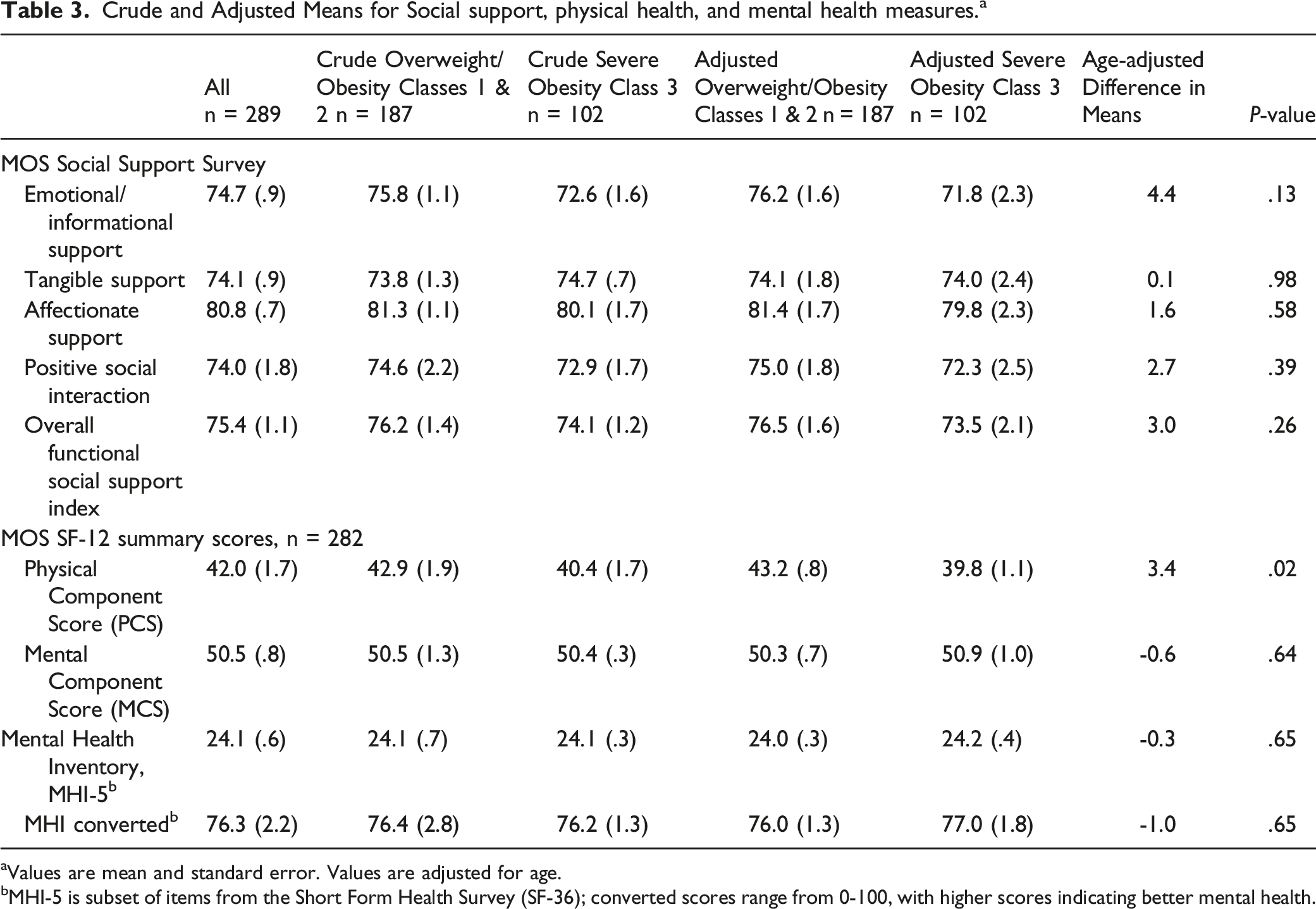
aValues are mean and standard error. Values are adjusted for age.
bMHI-5 is subset of items from the Short Form Health Survey (SF-36); converted scores range from 0-100, with higher scores indicating better mental health.
Discussion
Findings indicate that in this sample of Southern AAW, women classified with Class 3 obesity are differentiated from those with overweight or less severe obesity by PA behaviors. The women in this sample with Class 3 obesity had higher literacy which correlated with their younger age, were taking more blood pressure lowering medications, had higher A1c and less desirable HDL than their counterparts classified with lower BMIs. Dietary behaviors did not differ meaningfully, while weekly minutes of PA reported contained significantly less moderate and vigorous intensity PA. Additionally, women with Class 3 reported significantly poorer physical health-related quality of life (e.g., physical health and bodily pain limiting physical activities and work).
While there is a paucity of literature on the lifestyle behaviors of rural AAW living with Class 3 obesity in the Southeastern US, the existing data supports our findings.30-32 A 2018 study by Sterling et al sampling AAW classified with overweight and obesity living in rural Southeastern US found that between women classified with a more healthful eating pattern (i.e., more salads, water & whole grains) vs a less healthful pattern (i.e., more cereals, fast foods/fried foods & desserts), there was no difference in BMI status;
30
thus confirming our findings. While there may not be a difference in dietary patterns in those classified with BMI
Consistent with our finding of lower moderate and vigorous intensity PA, the Jackson Heart Study (N = 3174 African Americans from the Jackson, Mississippi metropolitan statistical area) found that the prevalence of moderate and vigorous intensity PA declined in a dose response pattern with increasing BMI. 32 Similarly, assessments of PA among US adults with normal weight and those eligible for (Class 3 obesity) and receiving bariatric surgery showed that compared to those with normal weight, those eligible (with Class 3 obesity) were significantly more likely to report lower physical functioning (i.e., mobility), and less PA (111.9 min/wk). 33
If our findings are representative of other Southern AAW living in rural settings, they have important implications for how we approach behavioral lifestyle weight loss interventions targeting this group of women. In the paragraphs below we discuss our findings in the context of existing weight loss intervention research and describe implications for future intervention research to address the PA needs of Southern AAW living with severe obesity.
Disparities in Treatment Among Individuals With Severe Obesity
AAW living in the rural South are the most vulnerable group for severe obesity. Obesity prevalence is higher in the South than other parts of the US. 34 Plus, severe obesity among women (BMI ≥ 35 kg/m2) is projected to become the most common US BMI category by 2030, with non-Hispanic African Americans and low-income adults projected to have the highest prevalence (32% vs 24% overall). 35
Currently, bariatric surgery is the most effective treatment for severe obesity. Only 1-2% of all eligible patients undergo surgery each year. 36 While eligibility is higher amongst AAW compared to White women (22% vs 12%), twice as many White women receive bariatric surgery meaning African American uptake is extremely low. 37 One of the barriers to uptake is health insurance requirements that patients lose at least 5% of their body weight before surgery. 37 Recent updates to the clinical practice guidelines for the perioperative nutrition, metabolic, and nonsurgical support of patients undergoing bariatric surgery state that more recent studies “argue against weight loss as a prerequisite” for bariatric surgery not because of the potential benefits of improved preoperative health associated with weight loss on postoperative outcomes, but because this requirement is likely to pose a barrier to a potentially life-saving procedure if patients fail to achieve the required weight loss. 38 The strongest predictors of not having bariatric surgery include having a BMI ≥ 50 kg/m2, and having a higher physical comorbidity burden 36 (lower physical function in this population being a finding reported in our study and others).
The picture painted by these data indicates that AAW living in the rural South are a priority population for prevention and treatment of severe obesity.
Weight Loss Interventions Among African American Women With Severe Obesity
To reduce severe obesity disparities, effective weight loss interventions for AAW are essential. Very few clinical trials for treatment of severe obesity focus on weight loss 15 with even fewer including AAW as a fully powered subgroup. The limited research available demonstrates that adults with severe obesity benefit from weight loss intervention trials. Interventions may result in modest clinically significant weight loss but with no improvement in cardiometabolic risk factors. 39 The addition of PA components may boost intervention effects yielding greater reductions in waist circumference and hepatic fat content. 15 However, low adherence to PA prescriptions limits the positive impact PA has on weight loss/maintenance and caloric prescription adherence. 40
Individuals with higher body weight exhibit higher total daily energy expenditure and activity energy expenditure; they need more energy to execute the same tasks compared to lower weight individuals. The higher energy expenditure is often confused for more minutes engaged in moderate to vigorous PA 41 when in reality individuals with sever obesity are seen to engage in less PA weekly minutes.
Because severe obesity is predicted to become more prevalent, improving the effectiveness of severe obesity weight loss interventions will become more important, particularly for those at highest risk—African American women.
Barriers to Physical Activity in African American Women With Severe Obesity
AAW face a unique set of multifactored barriers that contribute to low levels of PA engagement. According to the National Center for Health Statistics, as of 2020, only 16.5% of AAW engage in the recommended amount of PA. 42
Qualitative study on the thoughts and practices of PA in AAW living in a southern rural region of the US found that intrapersonal, interpersonal, physical, and environmental barriers impacted PA engagement.43-45 Women reported limited PA due to a lack of motivation, being too tired, “not feeling like it”, and feeling drained from obligations related to work, church, and family. This aligns with the Giscombe Superwoman Schema which states that AAW describe their gender role as an obligation to put others needs before their own, suppress emotions, resist being vulnerable or dependent, and succeed despite limited resources. 46 Therefore subscribing to Superwoman Schema or being a “Strong Black Woman” can be a detriment to overall health, and promote unhealthy coping strategies. 47 Similarly, role strain stress caused by the unique intersectionality AAW experience has also been shown to be a significant contributor to low levels of PA. 48
Societal weight bias is a well-documented phenomenon which is also thought to be a barrier to PA engagement.49-53 Individuals may be stigmatized for having a larger body size than the local population they inhabit consequently creating a viscous cycle of discrimination and obesity. However, this population of rural AAW with severe obesity is situated in North Carolina where, according to 2021 Behavioral Risk Factor Surveillance System(BRFSS) reports, 68.2% of the population had overweight or obesity. 54 This percentage increases when looking at just AAW (77.8%), 54 and even more so when factoring in a rural location. 55 The intersectionality of being African American, female, living in a rural area, and having severe obesity is an underexplored area of weight bias research.56,57 There is currently no evidence that weight bias is internalized in this specific population where obesity is more normative.
Additional barriers to PA engagement are AAW beliefs that their health conditions will worsen with increased PA. 58 Adults with obesity and musculoskeletal pain have also been shown to have an increased fear of movement. 59 Rosic and colleagues 60 showed that in women under age 40y with BMI 30.0 to 76.6 kg/m2, low PA was correlated with greater fear of falling. Chronic pain has also been associated with lower levels of PA as BMI increases. Relative to adults with normal weight, those with overweight reported 20% greater rates of recurring pain, 68% for people with Class 1 obesity, 136% with Class 2 obesity, and 254% among those with Class 3/severe obesity. 61
Other barriers identified by AAW to engaging in PA include a lack of PA role models they can identify with, limited or unclear PA advice from healthcare providers,43,44 and environmental factors such as lack of sidewalks and overall safety concerns. 45
Implications for Weight Loss Interventions Targeting African American Women With Severe Obesity
As we consider our study results related to PA, and the existing research on treatment disparities and limited weight loss interventions among AAW with Class 3 obesity, there are several important implications we see for future research focused on AAW with Class 3 obesity in a rural setting, particularly in the Southeastern US. These implications do not include a dietary component, but it should be noted here that no weight loss intervention would be effective without a dietary component that addresses caloric intake, diet quality, and the cognitive, environmental, and social factors that impact eating behaviors. Implications for the PA component of an effective weight loss intervention include: utilizing a physical therapy model, a multi-disciplinary team-based approach, and a stress-management focus.
Physical Therapy Model
Benefit may be drawn from the cardiac rehabilitation/physical therapy model. In this model, participants engage in structured supervised exercise almost daily. Two observational studies were found that utilized this technique in combination with dietary and psychological counseling.62,63 The populations were largely female with obesity averaging around Class 2. These programs yielded significant weight and BMI reductions. Given the importance of PA in women with severe obesity, as evidenced by our findings, incorporating daily structured sessions may be important in future interventions. Further, it may be beneficial to use the structured supervised exercise time to address underlying musculoskeletal complications which may be limiting exercise capacity in severe obesity.62-64
Multi-Disciplinary Team-Based Approach
Future studies may benefit from a multi-disciplinary team approach to address the multiple factors influencing weight loss; specifically, an exercise physiologist may strengthen intervention designs, strategies, and implementation. For example, in a non-surgical weight loss program for individuals with severe obesity, clinically significant weight loss was achieved with a team approach consisting of a physiotherapist, clinical nurse consultant, gastroenterologist, and psychiatrist. 65 In another metabolic rehabilitation program for individuals with severe obesity, the patient care team included a dietician, diabetes educator, psychologist, physiotherapists, exercise physiologist, and endocrinologist to address long term diabetes management. 66 Both studies yielded significant weight and BMI reductions.
Stress Management Focus
Research suggests stress experienced in rural communities differs from that in urban communities due to both types of stressors and availability of resources for prevention and coping. 67 Including culturally appropriate stress management in weight loss programs designed for AAW with severe obesity living in rural communities may augment weight loss for this population. A recent weight loss intervention study using mindfulness, a stress management coping strategy, found less weight regain among participants self-described as members of racial/ethnic groups, compared to their white counterparts; 68 thus, demonstrating the efficacy of this approach.
Study Limitations
This exploratory study aims to fill an important research gap specific to rural AAW with obesity but, it is not without several limitations. We did not adjust our significance level to account for multiple comparisons made and some findings found to be statistically significant at an alpha of .05 may not have been significant at a more stringent adjusted level. That said, our significant findings regarding PA were significant at a level that would not be affected by such adjustments. The cross-sectional nature of this research also means we cannot address the temporal link between exposures and outcomes. The surveys used, while validated, were not validated in rural, Southeastern Black US populations. Although this limitation is not unique to our study, it could potentially impact our ability to accurately assess factors important to tailoring interventions for this population subgroup. Our PA measure was validated in a low-income Southeastern US population. 24 Additionally, the number of psychosocial measures was limited in our efforts to reduce participant burden; this resulted in important measures of perceived stressors, environmental barriers, and household factors related to obesity not being measured. Because this is a moderately sized convenience sample in a limited geographical area, caution must be taken in generalizing the findings to AAW in other parts of the US.
Conclusions
Behavioral weight loss intervention research among rural AAW is limited, 10 and our study addresses this research gap with findings from a sample of rural women with severe obesity.8,9 Combining these findings with the available research among AAW with severe obesity, we have identified several implications that can inform future research specific to this high risk sub-group. These findings and our proposed strategies of using a physical therapy model to improve PA behaviors, addressing stressors, and a team-based care approach, can inform much needed behavioral lifestyle intervention research targeting AAW with severe obesity. If we consider that a greater proportion of AAW already live with severe obesity and the projections of increased prevalence, there is a level of urgency for research to address prevention and treatment of severe obesity using innovative and culturally appropriate strategies.
Footnotes
Acknowledgments
We gratefully acknowledge our Community Advisory Committee who provided helpful guidance with this project and to our study participants, whose willing participation made this study possible.
Author Contributions
Authors’ contributions are as follows: conception and design of the study (CS-H, AA, TK); data acquisition (CS-H, DB, AA, TK); data analysis and interpretation (CS-H, CA, DB, RA, HS); drafting or substantively revising text (CS-H, CA, RA, HS). All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by National Institutes of Health (NIH) grant 5P50 HL105184 to the University of North Carolina Center for Health Promotion and Disease Prevention (HPDP) with subcontract to the Brody School of Medicine, East Carolina University. Other support was provided by Centers for Disease Control and Prevention (CDC) cooperative agreement No. U48/DP001944 to HPDP (a CDC Prevention Research Center).
Ethical Approval
University of North Carolina at Chapel Hill, Institutional Review Board Application Approval – Application #10-0395.
Informed Consent
All participants provided written informed consent.
Clinical Trial Registration
ClinicalTrials.gov: NCT01433484.