
Abstract
Objective
American Indian and Alaskan Natives (AIAN) are regenerating cultural knowledge and practices to adapt westernized evidence-based interventions to address health concerns such as substance use. This study describes the process of selecting, adapting, and implementing motivational interviewing plus cognitive behavior therapy (motivational interviewing + Skills Training; MIST) for use in a combined substance use intervention with a rural, Northwest tribal community.
Methods
An established community and academic partnership worked together to make culturally mindful changes to MIST. The partnership incorporated community leaders/Elders (n = 7), providers (n = 9), and participants (n = 50) to implement an iterative process of adapting and implementing the adapted form of MIST.
Results
Key adaptations included presenting concepts grounded in tribal values, providing examples from the community perspective, and incorporating cultural customs and traditions. Overall, the MIST adaptation was favorably received by participants, and the adaptation appeared feasible.
Conclusions
Adapted MIST appeared to be an acceptable intervention for this Native American community. Future research should evaluate the interventions efficacy in reducing substance use among this and other Native American communities. Future clinical research should consider strategies outlined in this adaptation as a potential process for working with Native American communities to implement culturally appropriate interventions.
Keywords
Introduction
American Indians and Alaska Natives (AIAN) have garnered resiliency and wellness through traditional practices and knowledge guided by teaching from elders and spiritual leaders. 1 The practice of wellbeing is embraced through ceremony, language, and interwoven in community and cultural values. 2 For many tribal nations, these practices were suppressed through colonization including loss of ancestral homelands and language, and laws against cultural practices and forced assimilation polices. 3 Among some AIAN communities, substance misuse was associated with historical trauma, stressors from colonization, genocide, and continued social and economic inequalities,4-7 Despite high rates of abstinence, large, national surveys have shown that binge drinking rates were higher among AIAN than other ethnic/racial groups.8,9 The rates of alcohol-induced mortality are highest among AIAN men and women with 113.2 and 58.8 deaths per 100 000 residents, respectively. 10 Thus, having substance use disorder (SUD) treatments that are acceptable and efficacious for AIAN’s is of high public health import.
Although several SUD treatments have been identified as efficacious, 11 AIANs too often do not receive treatment and represent the highest rates of unmet treatment need for SUD in the United States of any ethnic group. 12 However, few research studies include meaningful numbers of AIAN13,14 and evidence-based intervention (EBI) have primarily been developed by and tested with predominantly white communities. 15 This lack of AIAN involvement in developing EBIs has resulted in high rates of observed attrition16,17 and providers who serve AIAN may be skeptical of EBI efficacy for AIAN given lack of representation. 18
Broadly, there is increasing evidence that EBI and cultural adaptation are complementary.19,20 Cultural adaptation can consist of surface level adaptations that increase the intervention fit through changes to setting, means of delivery, or materials to have them be a better fit for the target population.21,22 Deep structural adaptations may include incorporating cultural theories of change, beliefs about symptom origins, and considerations regarding the historical, cultural, or environmental context.21,22 However, if the adaptation dilutes core elements of the treatment this can decrease intervention effectiveness. 19 There are a few studies of SUD treatments which have examined adapted treatments specifically for AIAN communities, incorporating traditions and values of the tribes.23,24 This includes interventions that incorporate ideas around cultural identity and religiosity, content on historical trauma, and AIAN beliefs about healing practices. 15 The goal with culturally tailored interventions is to increase appeal, efficacy, and engagement among AIAN communities thereby reducing SUDs.25-27
Two SUD interventions with wide empirical support are motivational interviewing (MI) and cognitive-behavioral therapy (CBT, or skills training). 28 MI is client-centered and focuses on increasing motivation to change SUD through empathy, supporting autonomy, and exploring connections between changing substance use and values or goals. 29 CBT for substance use is rooted in learning theory and trains individuals in skills to refuse substances, identify triggers for use, and addressing those triggers through problem solving, mood management, or coping skills. 30 These approaches can be combined within a single intervention31,32 to capitalize on interventions reducing ambivalence towards change (MI) while unlearning negative patterns of substance use (CBT).
Research has already begun on adaptations of MI for AIAN.33,34 Meta-analyses indicated larger effect sizes for MI among ethnic minority populations, including AIAN, than Caucasian samples, and interventions that include MI are more effective than other types of interventions with AIAN individuals. 35 In a small randomized controlled trial specifically examining adapted empirically supported treatments for SUDs for AIAN adults, investigators worked closely with a Southwestern United States tribe to adapt MI combined with the Community Reinforcement Approach (CRA) for AIAN.23,24 Culturally adapted MI plus CRA was found to be as efficacious and as acceptable as a traditional SUD program, demonstrating the promise of this type of approach. Thus, blending MI with CBT, while adapting both, appears promising to address SUD among AIAN communities.
One important area to address in treating SUD among AIAN communities is the overlap with exposure to traumatic events and the presence of PTSD symptoms, 36 as well as with risk behaviors such as high risk sexual behaviors. 37 Given elevated social-behavioral risk stemming from lack of access to care, poverty, and other forms of instability compared to other communities in the US,38-40 it is not surprising that AI show disproportionately high rates of psychopathology associated with trauma exposure including high rates of PTSD, substance use and HIV risk.41,42
Although integrated treatment for PTSD and SUD is recommended when both are present, studies have demonstrated that treating SUD alone can also have beneficial impact on PTSD symptoms. 43 Manualized SUD interventions do appear to reduce symptoms of PTSD similarly to coping-based treatments intended to address PTSD.44,45 Integrated or combined PTSD/SUD treatments tend to be lengthy (20-25 sessions) with low treatment completion rates. Due to low rates of treatment completion among AIAN for lengthier trauma-focused treatments 46 and fewer treatment resources in tribal communities, brief, targeted SUD interventions with potential for downstream effects on PTSD could be ideally suited for AIAN communities. Manualized SUD treatments are widely available and delivery does not require counselors to be cross-trained in PTSD and trauma, thus further increasing potential viability and feasibility in AIAN communities.
The purpose of this paper is to describe our work culturally adapting MI/CBT (MI + Skills Training; MIST) for use with a rural, Northwest tribal community. The parent trial is ongoing and aims to evaluate whether addressing trauma or substance use among AIAN are the most effective methods for decreasing SUD, PTSD, and HIV-risk behaviors. 47 This paper includes a description of the MIST intervention, the adaptation process via consultation with tribal elders and members of the community review committee (CRC), qualitative data from in-depth interviews with AIAN patients and counselors, and quantitative data summarizing acceptability of the adapted intervention.
Methods
Intervention
The MIST Curriculum was delivered by local counselors, conducted in up to six, 90-120 minute sessions, and to consist of 1-2 sessions of MI and 4-5 sessions of skill building (CBT). Six sessions was predetermined as the intervention length based on findings from a prior trial with this community in which average session attendance was 6.1 sessions 48 . Longer session length was also recommended to allow more time for relationship and skill building.
Four MI core principles guided the intervention: (1) Express empathy, understanding how the client views their substance use and experiences; (2) Support self-efficacy, clients are responsible for choosing and carrying out actions to change while counselors support clients' belief in their abilities to change; (3) Roll with resistance, counselors do not confront clients but support them in developing their own solutions to self-defined problems; and (4) Develop discrepancy, counselors help clients examine discrepancies between their current behavior and future goals and values. The MI manual used was based on a manual already adapted for American Indians. 34
Cognitive Behavioral skills content was adapted from treatment manuals from prior efficacy trials.49-52 These manuals were chosen because they were written to be approachable with reduced technical jargon. The MIST Skills include setting substance use goals for treatment, identifying substance use triggers, and preparing for lapses or high-risk situations. Clients are taught how to identify how mood is related to substance use and new coping skills to address high-risk situations. Other modules assist clients in refining communication skills and increasing social supports. In each session clients identify thoughts and feelings that continue “unhelpful” substance use behaviors and develop new thought patterns to aid in behavior change. The main goal of MIST is to engage clients, and evoke from the client their own reasons for change. Once motivation to change is solidified, the client identifies goals and learns skills to address maladaptive substance use patterns.
Setting
The study was designed and conducted in full collaboration with a Pacific Northwest tribal nation 47 partnering with two behavioral health clinics: a tribally-operated clinic on the reservation and a privately-operated nonprofit in the adjacent town.
Participants
Study inclusion criteria were AIAN age 16 and older residing in and around tribal lands, with past year substance use and at least sub threshold trauma symptoms as measured by the PTSD checklist for the DSM-5. 53 Participants had to be willing to receive either a substance use treatment or an exposure-based PTSD treatment. Informed consent was obtained in-person utilizing a process where participants reviewed consent and were offered opportunities to ask questions. Participants were recruited throughout the community by advertisements in local newspapers and flyers distributed throughout the community, study personnel held booths at key community events, and counselor referral. We recruited 50 participants who were randomized into the MIST condition (13 males, 37 females; Age in years: Mean = 36.0, SD = 13.9) and 39 (78%) received therapy. Most (90%) were members of the participating tribe. Participants were slightly older than the general population served by the tribal behavioral health agency (average age: 32.3 years), likely due to the fact that 36.7% of their clients are under the age of 16 and eligibility for the study required participants to be at least 16 years old. The study recruited fewer males as compared to the client population at the tribal behavioral health agency (42%), but participants were similar on race/ethnicity. Of those that received the intervention, 52.6% (n = 20, 16 females, 4 males) responded to the debrief qualitative interview conducted by phone or in-person. Most participants (n = 39, 78%; 29 females, 10 males) responded to the post-intervention quantitative survey regarding therapeutic expectations, acceptability, and satisfaction. Of the 39 participants who completed the post-intervention quantitative survey, 34 participants received therapy. The post intervention survey was administered to all participants regardless of whether they received care.
Behavioral health counselors
Included nine providers serving the tribal community (1 male, 8 female, 4 American Indian, 1 Puerto Rican, 4 white). Counselors attended a 3-4 day MIST training conducted by DW and DK. The training included didactic content, experiential exercises, and opportunities to practice intervention implementation through role-plays and observation. Weekly, group consultation was offered via telephone. Debriefing interviews 18 months after training assessed counselors’ experience delivering MIST. On average counselors saw four clients each (range from 0–10).
Cultural Adaptation Process
The grant submission was supported by the tribal council via a tribal resolution. The tribe delegated IRB review of the study protocol to the University (IRB #00001359; clinical trials #NCT03112369) and maintained community oversight through the CRC and monthly written reports to the tribal council.
Community voice was paramount throughout curriculum development. We followed a three-step iterative process allowing for feedback from our CRC, counselors, and AIAN client participants. The CRC was comprised of seven individuals enrolled in the participating tribe including traditional healers, tribal leaders, Elders, and service program managers.
Adaptation Process
Step 1, began with the investigators drafting an initial manual by removing jargon, and reviewing each element to obtain feedback from the CRC and counselors on potential adaptations. The treatment was structured to eliminate between session homework and to have session handouts act as a guide for both counselor and client for session content. Although homework is a common feature of CBT, community feedback on a separate trauma treatment project suggested limiting homework. 46 Thus, no homework was assigned. Instead, clients were offered paper copies of worksheets to take home and encouraged to practice skills during the week. Verbal content on the worksheets was limited to be facilitative of visual learning. Handouts for each session included an agenda of the session topics, a “breaking it down” worksheet which reviewed a substance use event or urge to use in the past week, a handout that described key didactic points from the skill, and worksheets to practice the skill. A side benefit of increased handouts was to assist the counselor in maintaining focus on content and decrease the preparation time needed for each session.
In Step 2 we held five monthly two-hour meetings with the CRC and three one-hour meetings with counselors. We invited feedback on the procedures for honoring the voices and experiences of AIAN clients, selection of content for the five skill building modules, and cultural images. The tribe had a preexisting document that identified and described nine core tribal “Virtues”. We sought feedback on the incorporation of these Virtues within MIST. The MI component had already been adapted with American Indian communities; 34 however, we reviewed the cultural appropriateness of MI for the tribal community we were working with and it was determined no changes were required. The CRC identified and the counselors confirmed five CBT skills as most salient for the community: (1) Goal setting and substance use triggers; (2) Getting and increasing positive support (3) Relapse prevention; (4) Communication; and (5) Negative moods. Manual length was seen as acceptable and readability statistics (Flesch reading ease 65% and Flechkincaid grade level 7.8) suggested that the subject matter and reading level required minimal changes. The focus instead, was on cultural inclusion in language, indigenous imagery, and relevant examples.
Language revitalization was reflected with the incorporation of the Nine Virtues of Níix Ttáwaxt, guided by the CRC to insure their appropriateness. 54 These virtues function as ‘ideal rules for proper conduct’ in health and wellbeing. The virtues refer to the sacredness of youth and family and the importance of guidance and growth within the tribe’s culture (Supplementary Table 1). The Virtues were originally written down by a tribal elder, and although more virtues exist, these nine have been publicly shared and used in education and health care curricula. 54 Permission from the elder who published the virtues was obtained for use within the manual. One to two virtues were selected that were consistent with the theme of each session. Virtues were discussed at the beginning of each session by the counselor and client and connected with the module.
Indigenous cultural images
The medicine wheel, mountains, and hawks were incorporated into the manual and materials. The medicine wheel, is a symbol of harmony with balanced and peaceful interaction among all living beings on earth and represents self-development. By utilizing this circular format, the idea of “balance” that is integral to indigenous communities, was represented within the curriculum. Although, the medicine wheel is not a foundation to this tribe’s culture, the CRC acknowledged there are many other tribes residing on the reservation that do use the medicine wheel. Mountains located in the community reflect important tribal traditions of hunting, root gathering and the teachings of the elders. Hawk imagery and examples were incorporated because of their importance within community traditions as a symbol of seeing the “big picture”.
Module selection: Within MIST, the initial skill session focuses on goal setting (renamed as “personal vision”) and treatment rationale. Clients choose the order skills are conducted, thus affirming client autonomy and control.
Step 3 consisted of final manual adaptations based on counselor input. Counselors provided input during their training and a 6-month follow-up to clarify concepts, offer concerns with regard to the material, and fine-tune the application of virtues and service delivery procedures. Within the communication skills module, counselors who were members of the tribe suggested that “assertive” communication was not a good cultural fit because it can be perceived as aggressive and inconsistent with how tribal members communicate, particularly with elders. The term “assertiveness” was re-named to “honoring your vision” and the language describing the skill changed to emphasize the intention of communication that is clear, respectful and honest to the client with regard to their substance use goal. This was consistent with two of the tribe’s virtues (Kwy’āātimt‘ (honesty) and Itm’āāksha (careful in speech, peaceful; see Supplementary Table 1) reviewed at the beginning of the session. For behavioral activation/pleasant activity scheduling, a range of traditional practices were added as examples one could engage with as alternatives to substance use and a means for addressing mental health concerns.
Client quantitative measures: This 5-minute self-administered assessment was conducted post intervention (6-weeks). If this assessment was not completed, the items were presented again at the 3-month follow-up assessment. This survey included 14 items rated on a 10-point scale (from 0 not at all-9- extremely) that assessed therapy expectations, counselor satisfaction, and acceptability of therapy format. 55 Two open-ended questions asked clients what they liked and what they would change to make it better. The first and second authors independently analyzed these two questions.
Counselor post-training quantitative measures
The motivational interviewing knowledge and attitudes test (MIKAT) was used to assess MI knowledge and nine true/false questions assessed CBT skills knowledge. 56 CBT items included: “Role-plays are basic techniques used to teach skills within sessions.” And “Identifying substance-free alternative behaviors to cope with depression can help clients use less.” On a 10-point scale, six items assessed beliefs about MIST efficacy, i.e. confidence in treatment success, in reducing symptoms in various domains and likelihood to recommend MIST to their other clients.
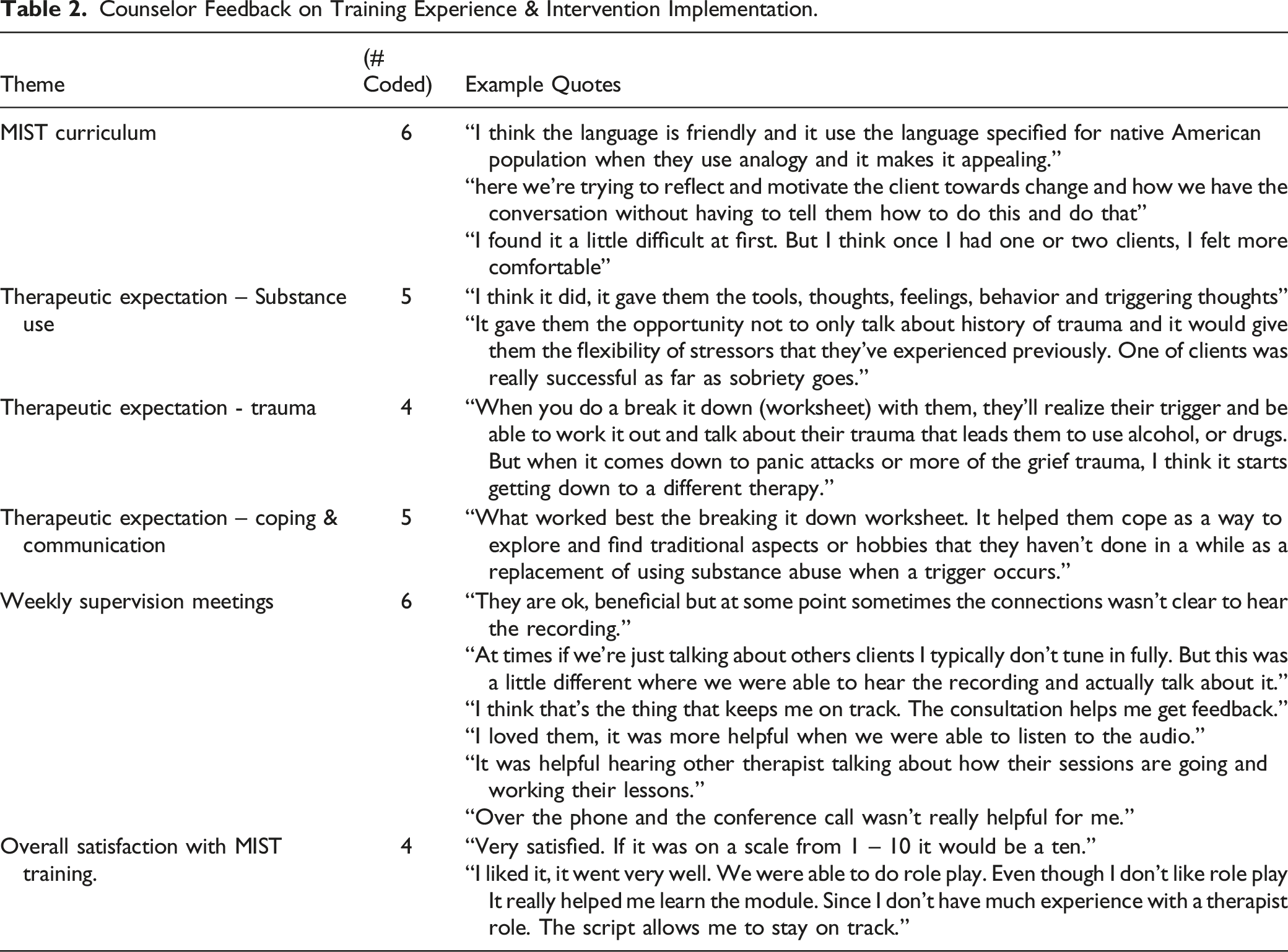
Counselor six-month follow up qualitative measures
In a semi-structured interview six MIST counselors were asked: how satisfied they were with the therapy; what they liked and disliked; and whether they thought therapy helped their clients in several domains. Additional items sought feedback on the usefulness of the weekly supervision meetings and initial training. Other questions assessed satisfaction with counseling process logistics and invited other suggestions. Responses were summarized under each item and comments in support for and areas of improvements are presented.
Procedures & Analysis
The quantitative data was analyzed using all available responses to provide frequencies and central tendencies. Qualitative interview and survey data was coded for pre-determined themes. Participant views were intended to contextualize the quantitative findings on intervention feasibility and acceptability. Qualitative interviews were transcribed and hand coded by two independent coders, analyzed using color blocking, and entered into excel. Participant quotes were categorized into the following categories by the first author: (1) therapist style, (2) therapy approach, (3) client outcomes and (4) cultural fit of treatment. These themes and client quotes were analyzed to identify concerns and suggestions for future practice, and potential training needs for counselors.
Results
Client quantitative data on intervention acceptability and satisfaction
Therapy Expectations
Of the 39 participants, 88%, reported MIST to be logical (70%), and that it would be effective at reducing trauma symptoms (72%), substance use-related concerns (79%), and risky sexual behaviors (77%). Participants also expected the treatment to help with other personal problems (77%) and would recommend the treatment to a friend (75%).
Counselor Satisfaction
Participant ratings on counselor satisfaction were high, with 77% of participants rating their counselor as able to understand their problems to a good or excellent degree. Similarly, participants felt their counselor was respectful (82%), knowledgeable about how to help (82%), used time wisely (82%), and they could share their thoughts, concerns or questions (80%).
Therapy Format Satisfaction
Participants were highly satisfied with the range of topics covered in therapy (77%). More than half rated satisfaction with the therapy dose (66%) and the materials used during sessions (66%) as “good” or “excellent”.
Open response questions
Several themes emerged from the question “What did you like about the therapy you received?” Most commonly, participants liked being able to express themselves without being judged (n = 6) and learning healthy ways to cope (n = 6). Learning new ways to think about problems or substance use triggers (n = 5), communication skills (n = 3) and feeling understood (n = 3) were also reported. Other participants cited appreciation for cultural flexibility “I admired my counselor so much... she even let me pray before session” and format “I liked how it was formatted so that the counselor can put in an easy way to explain it to me so I can understand.” With regard to changing or adding to the therapy, 25 participants reported they would add or change “nothing” to the therapy. The most common change desired was the therapy should be longer (more time in session or greater number of sessions, n = 3), however, at least one participant stated “Maybe I thought six sessions were too much”. Two participants suggested less emphasis on printed materials and completion of worksheets.
Client Qualitative Responses
Themes from participant interview data illustrated both strengths of and suggestions for improvement in the four pre-identified areas. Table 1 presents illustrative quotes for each theme. Overall, client comments suggested more aspects of the intervention that were appreciated and fewer suggestions for improvement. For “therapist style” several participants discussed how “comfortable” the sessions were and how it was easy to discuss topics with their counselor. “Native Americans, I just feel like we are just at the bottom of the pole when it comes to psychotherapy and you know nobody wants to listen to our problems, nobody wants to listen to what we have to say……..I don’t want to go to a different program because I appreciate this one so much….” “It was one of the few times I felt comfortable talking things out.” Illustrative quotes for each coded theme. Participant identifiers (P1, P2, P3, etc.) are used to indicate quotes attributed to each participant.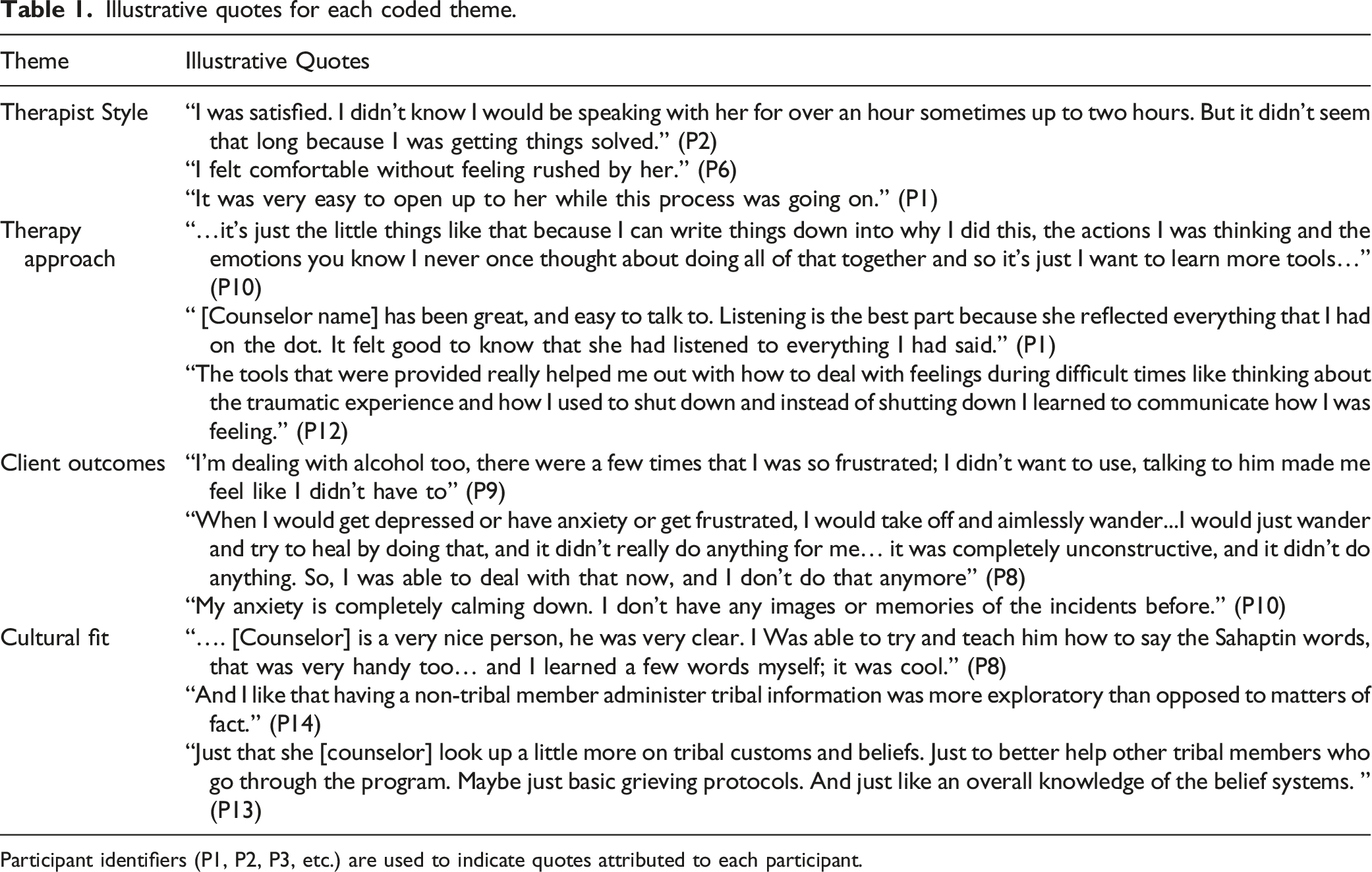
With regard to “therapy approach” several indicated high satisfaction with the communication skills modules, worksheets, and counselor use of reflective listening (which translated into the participants feeling heard and understood). “It was one of the few times where I felt comfortable talking things out.” “How they listened to me when I was talking”. “…. and she basically let me have control to figure things out on my own with her support”. “She actually went through the steps with me and helped me understand how I can talk to somebody in my family without pointing fingers and saying this is so-n-so's fault.”
Areas identified for improvement included treatment length (desire for more sessions), and less reliance on the manual and worksheets by the counselor.
For “client outcomes” participants indicated MIST was helpful generally and a few noted it was specifically helpful with addressing substance use. Less feedback was received on the “cultural fit” of the intervention. One participant noted that non-native counselors could benefit from increased education on cultural practices and traditions (specifically on death and grieving). The majority of comments referring to the use of the Virtues were positive, valued as they were developed by their own tribal elder, and perceived their inclusion as a strength. Acknowledgment of MIST increasing interest in other cultural activities and appreciation for the culturally significant healing tools (i.e., smudge stick, sweat grass, candles) were evident.
Counselor assessment
Counselor Feedback on Training Experience & Intervention Implementation.
Discussion
More culturally adapted evidence-based SUD treatments are needed for AIAN populations. This study adds to the literature as it describes the process of working with one AIAN tribal community to adapt a combined MI and CBT treatment for substance use, eliciting and integrating feedback from the CRC, providers, and participants. Overall, community responses to the intervention were quite positive. Most were likely to recommend the treatment to a friend, suggesting their strong belief in the efficacy of the treatment. Participants were confident that MIST could not only assist them with their substance use (which the intervention targeted), but also with co-occurring concerns such as symptoms of post-traumatic stress or high-risk sexual behavior. This speaks to the applicability and credibility of the skills modules selected by the community. The acceptability of cultural adaptation of evidence-based practices for Native American communities is consistent with other research specific to MI and behavioral treatment for substance use.23,24 Although counselor and participant evaluations of the MIST intervention were favorable, further research will need to evaluate whether the intervention is effective in addressing substance use, as well as the other behavioral health issues reported by this population.
Format of the intervention including dose and materials were also rated highly by most participants. Treatment length was informed by previous work in the community that suggested a six session intervention would be more acceptable than a longer treatment. 42 Most participants did receive treatment (77.5%), and coupled with little feedback requesting fewer sessions suggests six sessions were adequate for most. A future treatment adaptation might involve “add-on” sessions for those who wish for additional support, skills training, or specific content such as trauma-related work.
Despite high acceptance of the number and length of sessions, 90–120 minute sessions may be difficult to implement under “real world” conditions. Longer sessions can add implementation barriers as reimbursement for longer psychotherapy sessions tend to be low, no-shows or late cancellations are even more detrimental to clinic productivity, and clinic productivity indices may not adequately reflect counselor time for longer sessions. Session content however, was easily adjusted to be broken into two 60 minute sessions when it was impossible for a client to stay for 90–120 minutes.
Quantitative and qualitative data found counselors were perceived to be helpful. MI emphasizes active listening, a warm and empathic approach, supporting client autonomy, and valuing the client’s experience. This way of being with clients appears to be highly valued by this population as specific comments identified the counseling style as helpful. Themes from the qualitative data emphasized the experience of being “understood”, “comfortable”, listened to, and guided rather than directed or told what to do as aspects of the treatment clients appreciated. Some client comments spoke to this directly. Also, the nonjudgmental nature of the intervention was experienced as positive. These aspects of MI may be especially effective for populations who often feel like their voices aren’t heard or have had experiences of being unfairly judged.
Process interviews identified several strengths of the communication module, dealing with negative moods, and problem-solving components of the intervention. Skills that addressed triggers for substance use were noted as especially helpful. These skills modules required few content adaptations although Tribal specific imagery and examples were incorporated. For example, in the relapse prevention module a list of community specific activities (sweat lodge, beading, gathering berries, learning native language or dance) are listed as alternative activities to substance use. However, the basic content of the modules remained similar to the original and adaptations to increase cultural relevance were relatively easy to implement. Each session began with a tribal value and discussion of how the teaching of the day related to that value. This centering of session content on core values and beliefs of the community may have negated the need for dramatic changes to the skill content and suggests that adapting such interventions for other communities might be achievable with a modest amount of effort.
Working with the community throughout the adaptation process garnered several benefits. Content was selected and endorsed by the community as having relevance to its members. Opening the skills training sessions with tribal values honored language revitalization and squarely focused the session content with its’ intersection of cultural values. It was obvious to the client that this was an intervention adapted with community input with the explicit incorporation of tribal values, language and imagery used throughout potentially contributing to high acceptance rates of the intervention.
The findings should be understood with the following caveats. Just over half of participants completed the qualitative interview to discuss strengths and limitations of the intervention. This could have skewed our findings positively, as it is possible that the participants who were most favorable towards the intervention were those who completed the interview. However, 78% of participants completed the quantitative surveys and those results mimicked the interviews. As stated above, session length of 90–120 minutes may be a barrier to implementation of MIST in its present form. However, given the acceptability of this format among participants, and the reasons for doing so (allowing for greater warm up time with the counselor, inclusion of cultural activities if participant desires, and community recommendation of fewer sessions), future research should evaluate dosing schedules for efficacious treatments to assess the optimal length and number of sessions. Longer sessions allow for more content to be delivered in fewer sessions. Barriers to attending treatment in this population may suggest that more content in fewer sessions is ideal for accessing a therapeutic dose of intervention. Additionally, although MIST is a treatment for SUD, not all participants had SUD. This may speak to the applicability of the skills sessions outside of an SUD treatment context and the potential for this intervention as a transdiagnostic approach. This is not surprising since CBT is an effective intervention for many behavioral health issues but the particular formulation of this adapted CBT approach may have increased generalizability across presenting concerns. Future outcome data will illuminate whether the treatment is effective in reducing substance use, trauma symptoms or high-risk sexual activity. AIANs represent the highest rates of unmet treatment need for substance use disorder (SUD) in the United States of any ethnic group. Evidence-based interventions (EBIs) have primarily been developed by and tested with white communities. The few studies of SUD treatments which have examined adapted treatments for AIAN communities, incorporating tribal traditions and values offer encouragement. This article describes an iterative process for culturally adapting two EBIs for SUD with a Pacific Northwest tribe. Qualitative and quantitative data report input and reactions from a community advisory board, practitioners serving the community and participants. The goal with culturally tailored interventions is to increase appeal, efficacy, and engagement among AIAN communities thereby reducing SUDs. Findings suggest a method for adapting interventions with AIAN communities that lead to high acceptability.So What
What is already known on this topic?
What Does this Article add?
What are the implications for health promotion practice or research?
Supplemental Material
Supplemental Material - A Community Engaged Approach in Adapting Motivational Interviewing and Skills Training for Native Americans With Experiences of Substance Misuse
Supplemental Material for A Community Engaged Approach in Adapting Motivational Interviewing and Skills Training for Native Americans With Experiences of Substance Misuse by Denise Walker, Cynthia Pearson, Angelique Day, Michele Bedard-Gilligan, Kathryn Saluskin, David Huh, and Debra Kaysen in American Journal of Health Promotion
Footnotes
Acknowledgments
We would like to acknowledge Robin Pebeahsy and Lucy Smartlowit-Briggs for contributions to project set up and implementation and valuable insights on working with this community. We would also like to acknowledge Patricia Whitefoot, Willow Howard, Anita Mendoza and Diane Pebeahsy for their guidance and leadership serving as the study community advisory members.
Author Contributions
Denise Walker contributed to the conception of the study design, acquisition of data, interpretation of data and led the writing of the manuscript. Cynthia Pearson contributed to the conception of the study design, acquisition and interpretation of data and writing and review of the manuscript. Angelique Day contributed to the analysis and interpretation of the data and manuscript review. Michele Bedard-Gilligan contributed to the conception of the study design, acquisition and interpretation of data and writing and review of the manuscript. Kathryn Saluskin contributed to acquisition of data and review of the manuscript. Debra Kaysen contributed to the conception of the study design, acquisition and interpretation of data and writing and review of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a grant from the National Institute on Mental Health Disparities (1R01MD011574-01; PIs: Pearson & Kaysen). The grant submission was supported by the tribal council via a tribal resolution. NIMHD had no role in the study design, collection, analysis, or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Ethical approval
This study conforms to the ICMJE ethics guidelines for human subjects research and received IRB approval from the University of Washington. The tribe delegated IRB review of the study protocol to the University of Washington (IRB #00001359; clinical trials #NCT03112369) and maintained community oversight through the CRC and monthly written reports to the tribal council.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.