
Abstract
Purpose
The present study conducted a social media content analysis on videos describing the Mediterranean Diet (MedDiet) posted onYouTube.
Setting
YouTube TM online video sharing and social media platform.
Method
Three independent content experts evaluated 141 YouTube videos on the MedDiet in August 2020 utilizing standard rubric and protocol. Data abstracted include media source(s) of posted videos, and viewer exposure/engagement metrics. Information quality was measured by each content expert independently through use of the DISCERN instrument, a 16-item tool designed to assess reliability, dependability, and trustworthiness of an online source, scores were then aggregated for analysis.
Results
A majority of videos (n = 102, 72.3%) were educational in nature. A third of videos were less clear and less credible on information presented (n = 46, 32.6%). Most videos were posted by an individual (n = 79, 56%), and the majority of videos were rated as medium quality (n = 88, 62.4%). Overall level of user engagement as measured by number of “likes,” “dislikes,” and user comments varied widely across all sources of media. Exploratory correlation analysis suggests that the number of a video’s views, comments, likes, and dislikes are not correlated with quality.
Conclusion
Study findings suggest that MedDiet health promotion and education via YouTube has the potential to reach and inform clients; however, existing video content and quality varies significantly. Future intervention research focused on MedDiet should further examine possible predictors of high quality MedDiet content utilizing diverse online video sharing platforms.
Introduction
Globally, the number of Internet users has increased dramatically in the past decade, where, approximately two-thirds of the world’s population now has Internet access. 1 Currently, people with Internet access are able to produce and share health information via social media (Web 2.0); this is in stark contrast to the early Internet where people were only able to retrieve information.2,3 Social media is considered a highly important tool for communicating health information. 4 Coincidently, online health information (OHI) happens to be one of the most popular activities completed online.2,4 that the literature communicates that 79% of adults use the Internet as a source of health information. 5 Additionally, 24% of these users access the Internet to obtain food and nutrition information. 6 One of the most important factors affecting the reliability of food and nutrition information is the credibility of the online source. 7 Emerging research has examined the influence of health information in social media on health problems such as diabetes, cancer, Alzheimer’s disease, and hypertension among others.2,8-20 In the last few years, video-sharing social media has become more popular, with 72% of adults accessing video-sharing social media, including YouTube which is accessed by 63% of adult users. 4
YouTube (http://www.YouTube.com), first launched in 2005, is among the most utilized social media video sharing platforms on the Internet.2,21 Online public communication on YouTube occurs via interactions such as likes, dislikes, and comments to posted videos.2,7,22 YouTube also provides content in more than 80 different languages. 23 YouTube serves as a media channel for promoting education and awareness.9,16,24-26 On the other hand, it may provide invalid and misleading information.7,9 YouTube videos offer a variety of health information, which is not regulated in terms of the quality of the information provided, nor in the content itself. 27 Recent studies have reported YouTube videos are a poor source of medical information and have a high probability of propagating misleading information.2,27 Consequently, it is necessary that medical, and health information shared on YouTube be reliable to keep from misleading consumers. 6
The Mediterranean Diet (MedDiet) is the traditional dietary pattern associated with countries surrounding the Mediterranean basin.28,29 MedDiet consists of a high intake of fruits, vegetables, legumes, nuts, unrefined whole grains, liberal use of olive oil; moderate-to-high intake of fish; moderate intake of alcohol (primarily wine) through meals; low-to-moderate intake of dairy products; and low intake of red meats, poultry, saturated dietary fat, and sweets.30-32 Several studies have shown an inverse association between adherence to MedDiet and oxidative stress, cardiovascular diseases, depression, and several types of cancers.33-37 The sheer volume of information available on the Internet has led prior researchers to examine the quality of information communicated. 38 Not surprisingly, information related to MedDiet found on websites was overwhelmingly poor in quality. 6
We, therefore, build on prior research examining the potential of YouTube as a resource for health promotion. 39 The current study bridges an existing gap in the literature on the credibility and quality of information related to MedDiet on online video sharing platforms, specifically YouTube. The overarching purpose of the current review is to assess the quality (credibility and reliability) of MedDiet information available among videos posted online and hosted on YouTube. We also communicate YouTube’s potential for promoting healthy behaviors via MedDiet.
Methods
The current search and review was conducted in August 2020. Mediterranean diet related videos available on YouTube were systematically searched and examined utilizing standard procedures and DISCERN online video quality evaluation instrument.
Three independent raters searched using the following four search phrases – “Mediterranean Diet; Mediterranean-style Diet; Mediterranean dietary pattern; and Mediterranean Eating Pattern.” Cookies and cache were cleared by each rater prior to conducting search. Prior to abstracting data from search results, all raters checked for consistency of video results. The following criteria were followed in selecting videos for evaluation.
Inclusion Criteria
Utilizing search terms communicated above, MedDiet video results in the English language only, search periods between January 2010 – August 2020, and 100 top search results were included.
Based on previous studies,2,3,7,10,11,17,19 YouTube users characteristically only browse through the list presented of the first 60 to 200 videos. We sought to replicate end user experience and evaluate only the first 200 resulting videos fitting inclusion criteria. YouTube settings were adjusted to sort the videos based on the highest view count to the lowest. Video results were excluded if they did not meet the inclusion criteria. A total of 200 videos were collected. Duplicate video results and non-English videos were excluded from analysis. One hundred 41 videos met the criteria for analysis, and each video was evaluated independently by three independent raters from the study team.
The three independent raters are also nutrition experts. Each examined videos independently and collected data accordingly. For data congruency and reproducibility raters followed the same standard procedures and all used the DISCERN evaluation instrument. 38 The data collected were abstracted using the same objective criteria which included video titles, links, view count, number of comments, number of likes, number of dislikes, and video length. Evaluators classified the speakers featured in the video into 8 categories (Healthcare professional/dietitian/nutritionist, researcher, cook/chef, influencers/actor, personal trainer/coach, not available (N/A), and other). The type of the video was also classified based on three categories (educational, experience (by following MedDiet), and cooking show). The video source was reported based on type of source (for-profit organization, non-profit organization, and individual user). The videos were evaluated using the DISCERN instrument, developed for use in healthcare to judge the quality and reliability of health information. 38
DISCERN has been used previously in robust peer-reviewed literature,40-42 and consists of 16 questions, with each question on a continuous rating scale from 1 to 5 where 1 indicates No; 3 indicates partially and 5 indicates Yes on whether the video fulfills the item’s criteria; 2 and 4 are intermediates on the scale.
DISCERN consists of three categories; A.) evaluation of reliability, dependability, and trustworthiness of video (items 1-8); B.) quality of information presented (items 9-15); and, C.) overall quality of video (item 16). Of note, item 16 is completed separately and its rating scale is distinct to the prior items in the instrument. Item 16s rating scale is continuous from 1 to 5. Where one is defined as a low-quality video with ‘serious shortcomings’; 3 a moderate quality video with ‘some limitations’; and 5 a high quality or video that is a ‘useful source’. For this item, 2 (proximity to low quality) and 4 (proximity to high quality) are intermediates on the scale. To compute a DISCERN score and determine relevant quality level the sum of all 16 items is calculated. A DISCERN score has a total possible maximum score of 80 and minimum score of 16. It is important to note The DISCERN handbook provides little guidance on interpreting total DISCERN scores, and, to date, to our knowledge, no definitive subdivision of the DISCERN score has been formally agreed upon and published.38,43 Thus, for the current study we used the following 3 predetermined cut-off points to define video quality level; low quality: 15-37.6, medium quality: 37.7-58.9, and high quality: 59-80.
The reliability of the videos was determined by taking the average of the first 8 questions from (1 to 8), and the quality of the information was assessed based on the average of the questions from 9 to 15. For overall, quality assessed by item 16, the score obtained in the item served as the indicator (as a brief reminder - 1 is defined as a low-quality video with ‘serious shortcomings’; 3 a moderate quality video with ‘some limitations’; and 5 a high quality or video that is a ‘useful source’).
Each video was evaluated independently by 3 content experts. To prevent and reduce the introduction of possible bias, the mean score stemming from each of the 3 evaluations were calculated and recorded for each video.
All analyses were conducted in IBM SPSS version 25. The characteristics of videos (number of views, length in minutes, number of comments, number of likes, and number of dislike) were represented by using mean ±SD as well as minimum and maximum counts. Normal distribution of data was assessed by applying The Kolmogorov-Smirnov test. The associations between the quality of videos using the DISCERN instrument and speaker, type of message and source of information were tested using Chi 2 due to the data being categorical. Correlation between variables of quality assessments (performed with the DISCERN instrument) and the characteristics of the videos was tested using Spearman’s test as data were not normally distributed. Results were considered significant at P-value <.05.
Given the nature of this study, no ethical oversight or approval was found to be necessary and therefore not obtained.
Results
Characteristics of Videos on Mediterranean Diet (N = 141).
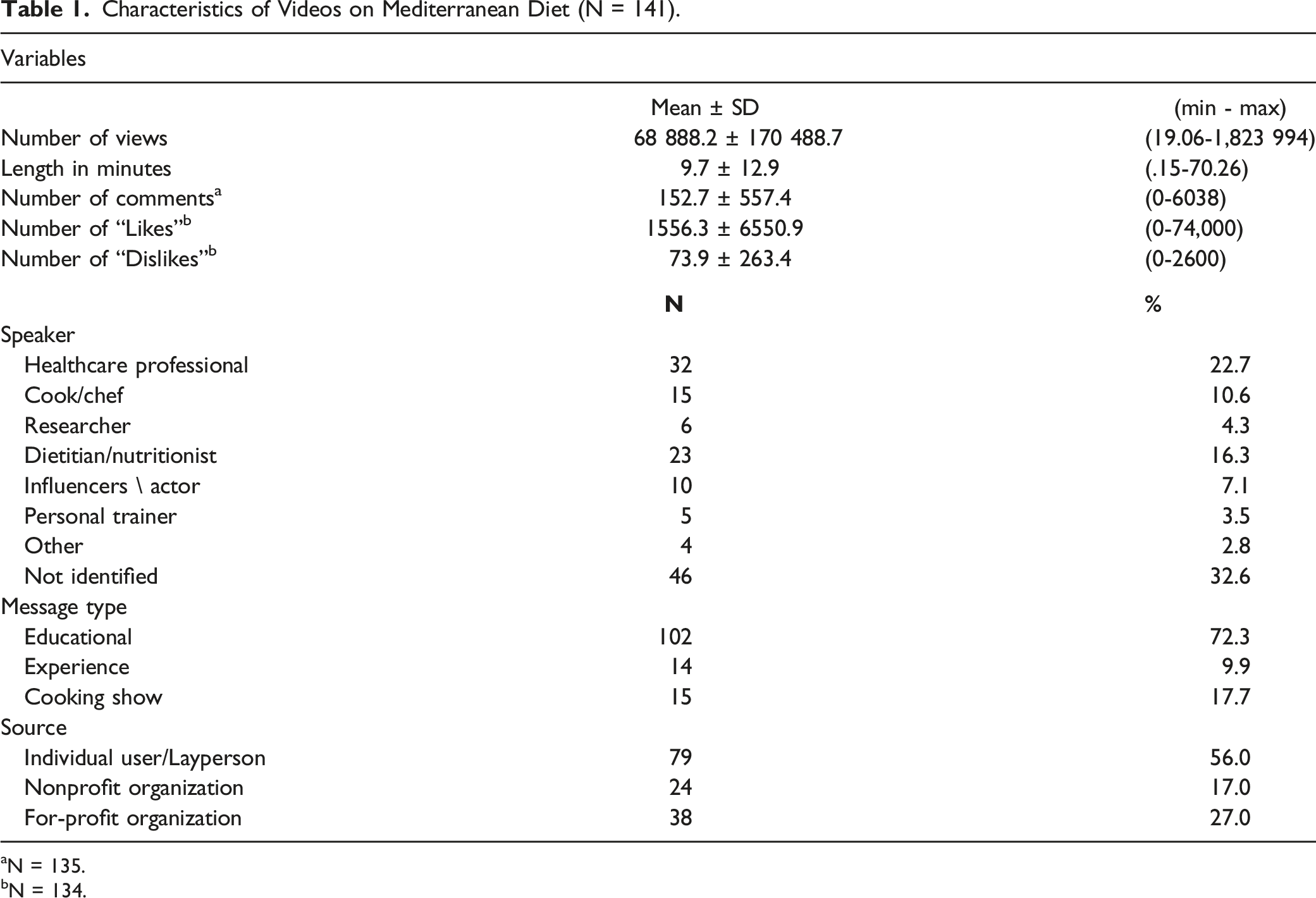
aN = 135.
bN = 134.
Quality Assessments of Videos (n = 141) Utilizing DISCERN Instrument Relevant to the Speaker.
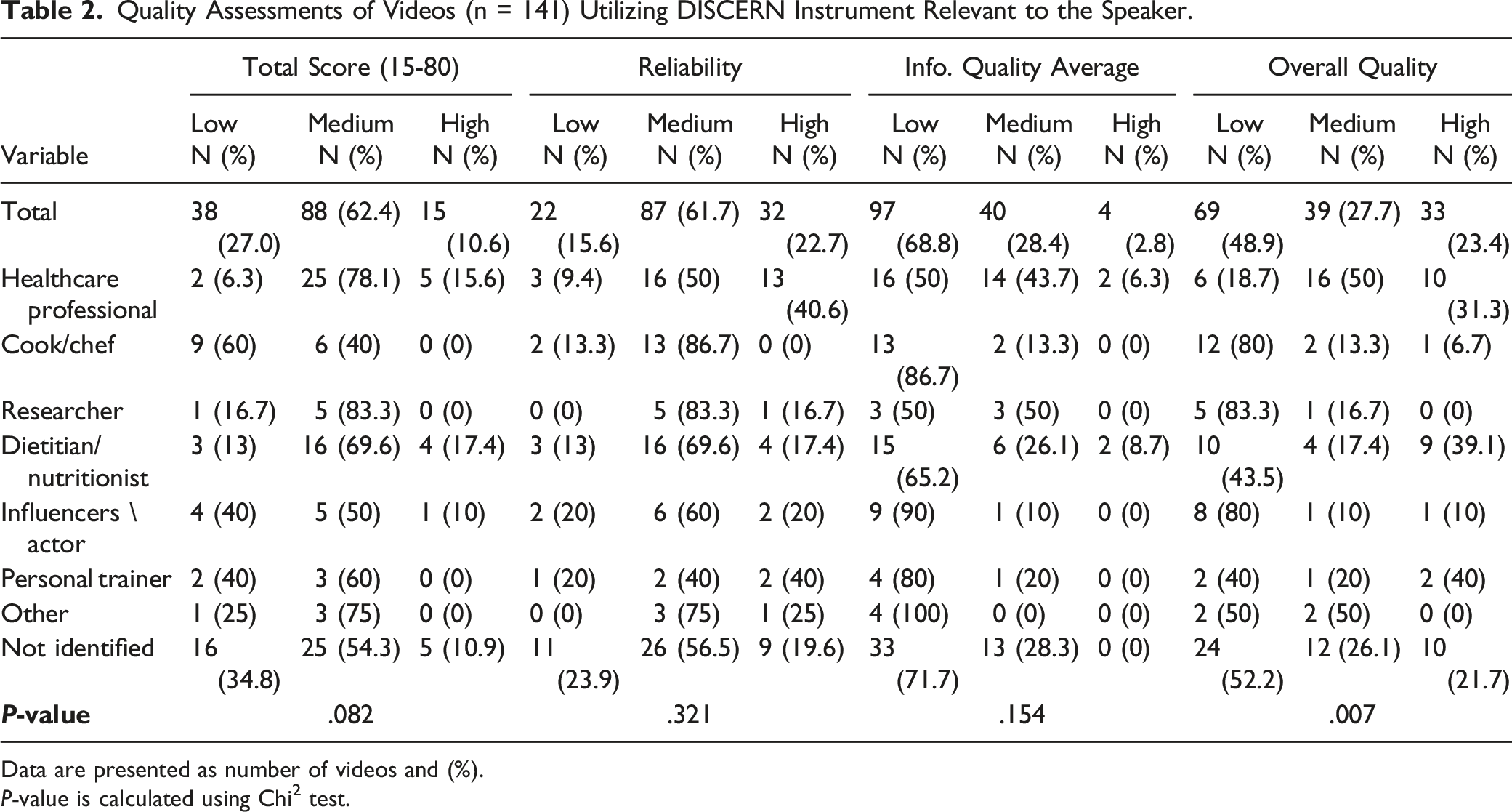
Data are presented as number of videos and (%).
P-value is calculated using Chi 2 test.
Quality Assessments of Videos (n = 141) Utilizing DISCERN Instrument Relevant to Message Type.
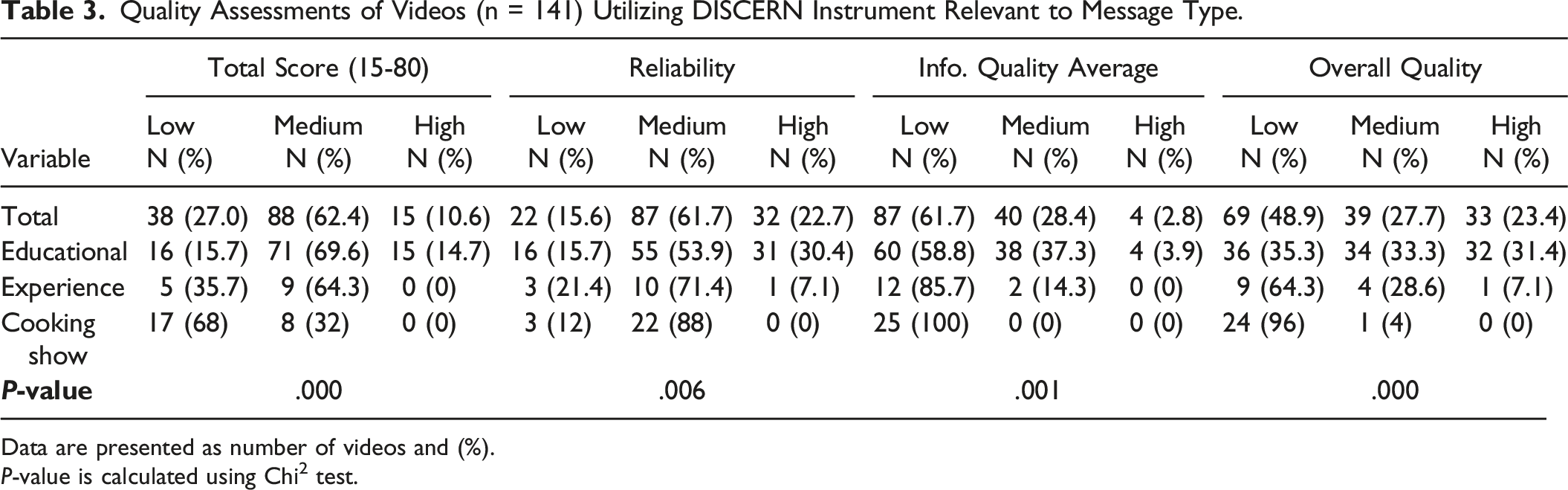
Data are presented as number of videos and (%).
P-value is calculated using Chi2 test.
Quality Assessments of Videos (n = 141) Utilizing DISCERN Instrument Relevant to Information Source.
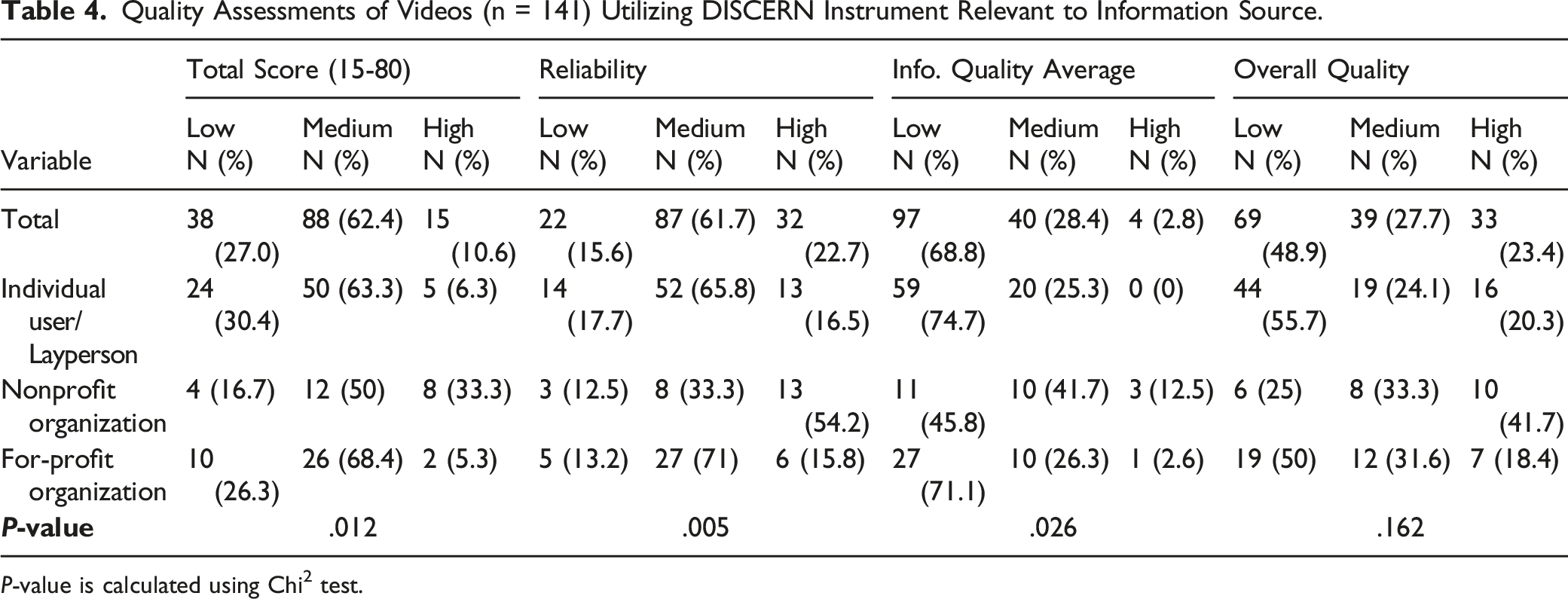
P-value is calculated using Chi2 test.
Correlation (Spearman’s rho) Between Quality Assessment Variables (Utilizing DISCERN instrument) and Video Characteristics.
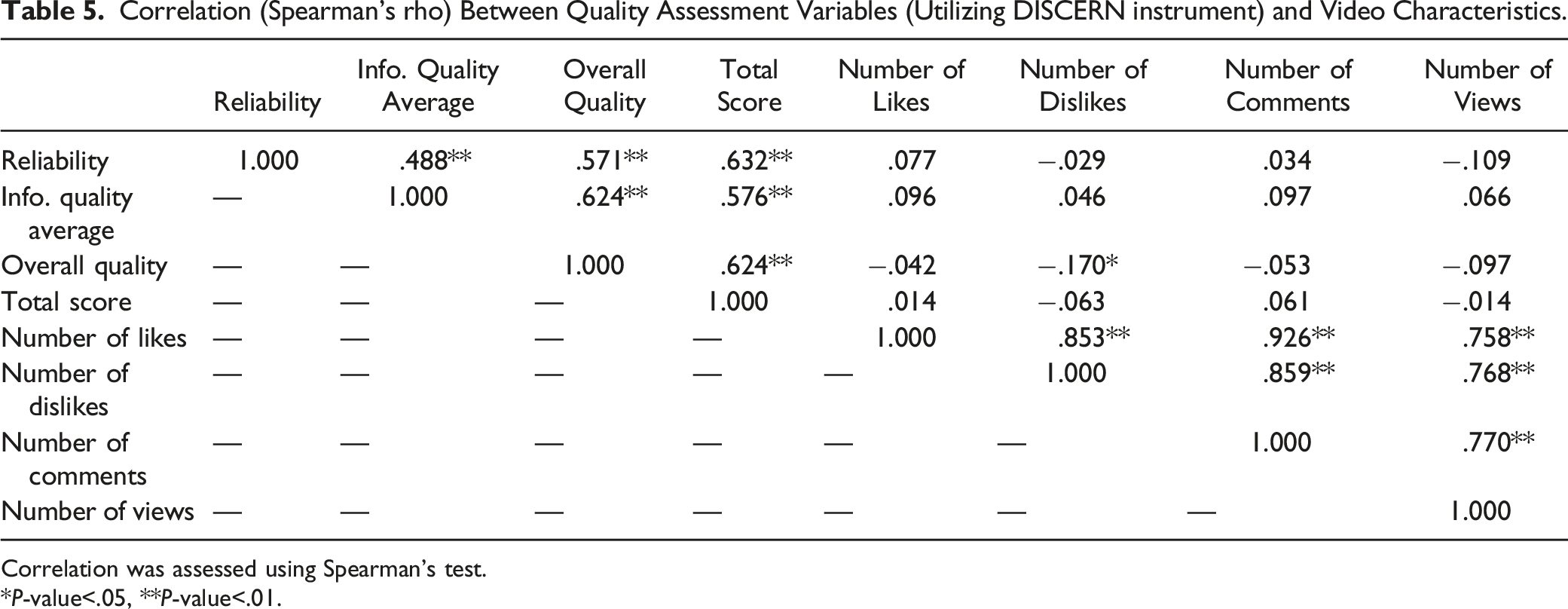
Correlation was assessed using Spearman’s test.
*P-value<.05, **P-value<.01.
Discussion
This research confirms both the variability in the quality of information provided on the Mediterranean diet and related health benefits in YouTube videos as rated by content experts researchers in the field, 6 as well as the lack of correlation between the health information quality of these videos and consumer response to said videos. Because of the unregulated nature of this forum, it is not surprising that there was little correlation between the researcher ratings of the videos using DISCERN and the video characteristics evaluated. The present research indicates that the number of views, likes, dislikes, and comments is not associated with, and should not be used as an indicator for quality of videos on the topics of MedDiet, and health; this mirrors prior findings among published studies on health information found on YouTube.10,44 These findings further communicate an area for concern for all health practitioners, as the videos that were assessed as lower quality were not correlated with consumer interactions which can result in amplifying the message of a video such as likes and views. While the significant yet weak negative correlation between overall video quality and the number of dislikes could be a promising trend, there is no indication that the number of ‘dislikes’ is due to the veracity of the information presented. eHealth literacy is defined as the ability to seek, find, understand, and appraise health information from electronic sources, and apply the knowledge gained to addressing or solving a health problem. 45 The findings highlight a need to increase consumer literacy about the reliability of video-based information in online forums such as YouTube. The researchers assessed MedDiet videos utilizing the DISCERN tool to determine overall video quality, with significant associations found between the type of professional presenting the information, however, the scores for reliability, information quality, and the total score were not significantly associated with the profession of the presenter. Because of the increasing role of the Internet and volume of healthcare information provided on platforms such as YouTube18,46 it is imperative that quality be a concern of professionals providing information in this format.47-49 While there was a significant association between MedDiet video source and DISCERN total, information quality, and reliability scores and it was determined that non-profit funded sources had the highest quality ratings compared to for-profit, and individual sources. In general, the distribution of quality scores was relatively wide and poorly correlated with the video characteristics. This finding is similar to other content analyses that have found a mixed quality of health information online and a lack of well-established guidelines for professionals on the best methods to deliver evidence-based information to consumers via the Internet.10,50,51
In reflecting on the current study’s findings on MedDiet, it is of interest how our results compare to videos for other health conditions. We acknowledge that further research is necessary to speak on findings relevant to multiple health conditions. Yet, in similar prior efforts, such as those by Stellefson et al, 14 on YouTube’s potential to reach and educate COPD patients, findings are astonishingly similar in the need to encourage researchers and practitioners to lead efforts on creating high quality educational materials respective to their field of expertise. 14
This study has some limitations. Selection of the videos was made using a limited number of key words; hence, some videos could have been missed. Additionally, YouTube is known to be a constantly changing platform which implies that the number of comments, likes and dislikes could change. Finally, only videos in English were evaluated, meaning videos in other languages could influence the findings of the current study.
Information on YouTube regarding MedDiet and health, as with other health information available on the platform, is varied in quality, and more work is needed to improve the quality of information provided in videos made on this topic. The highest quality videos reviewed were attributed to healthcare professional/dietitian/nutritionist; and, were categorized as educational, and provided by non-profit sources. The number of a video’s views, comments, likes and dislikes is not correlated with, and subsequently should not be used as a gauge for quality. Based on these findings, it is recommended that healthcare professional/dietitian/nutritionist, researchers, universities, and governmental and non-profit organizations should be encouraged to create evidence-based content that is of interest to viewers to help balance what clients, and their families may access on popular media sites and the Internet. Additionally, our findings speak to the need for eHealth literacy training to increase the public’s ability to seek, find, understand, and appraise health information from electronic sources and apply the knowledge gained to addressing or solving a health problem. The Mediterranean diet (MedDiet) is internationally recognized as an antiobesogenic dietary model. Social media is considered a highly important tool for communicating health information and serves as a channel for promoting education and awareness. This article assesses the quality of MedDiet information available on YouTube TM. This article also communicates YouTube’s potential for promoting healthy behaviors via MedDiet, thereby filling a gap in the scholarly literature with regards to the MedDiet’s visibility, credibility, and how information on this dietary pattern is portrayed on social media. Information on YouTube regarding MedDiet and health promotion, as with other health information available on the platform, is varied in quality, and more work is warranted to improve the quality of information provided in videos made on this topic. Findings also speak to the necessity for eHealth literacy training to increase the public’s ability to seek, find, understand, appraise, and apply health information from electronic sources.So What?
What is Already Known on this Topic?
What does this Article Add?
What are the Implications for Health Promotion Practice or Research?
Footnotes
Author Contribution
Research conception: BAE. Methodology: NB, MA, FA, AA, ED. Data collection: MA, FA, AA. Data collation: MA, FA, AA. Data analysis: NB, MA, FA, AA, ED. Data interpretation: BAE, EAC. Literature search: BAE, EAC. Manuscript drafting and revision, final approval: BAE, EAC, ED, NB.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.