
Abstract
Purpose
To evaluate the implementation and effectiveness of the Carolina Heart Alliance Networking for Greater Equity (CHANGE) Program, an adapted evidence-based cardiovascular disease risk reduction intervention delivered by Community Health Workers (CHW) to rural adults.
Design
Hybrid implementation-effectiveness study with a pre–post design.
Setting
North Carolina Federally Qualified Health Center and local health department in a rural, medically underserved area.
Sample
Participants (n = 255) included 87% Non-Hispanic Black with a mean age of 57 years; 84% had diagnosed hypertension, 55% had diabetes, and 65% had hypercholesterolemia.
Intervention
A CHW-delivered, low-intensity, 4-month behavioral lifestyle intervention promoting a southern-style Mediterranean dietary pattern and physical activity.
Measures
We measured number and representativeness of participants reached and retained, intervention delivery fidelity, weight, blood pressure, and self-reported dietary and physical activity behaviors.
Analysis
Pre–post changes at 4 months were analyzed using paired t-tests.
Results
Study participants completed 90% of planned intervention contacts; 87% were retained. Intervention delivery fidelity measures showed participants receiving a mean of 3.5 counseling visits, 2.7 booster calls, and on average completing 1.7 modules, setting 1.8 goals, and receiving 1.3 referrals per visit. There were significant mean reductions in systolic (−2.5 mmHg, P < .05) and diastolic blood pressure (−2.1 mmHg, P < .01); the proportion of participants with systolic blood pressure <130 increased by 7 % points (P = .05), and diastolic pressure <80 by 9 percentage points (P < .01). Dietary behaviors improved significantly with average weekly servings of nuts increased by .5 serving (P < .0001), and fruits and vegetables by .8 daily serving (P < .0001). Physical activity also increased on average by 45 min./week (P < .001). Weight did not change significantly.
Conclusions
The CHANGE program showed both implementation and program effectiveness and adds to the evidence supporting CHW-delivered lifestyle interventions to reduce CVD risk among rural, Non-Hispanic Black, and medically underserved populations.
Keywords
In the US cardiovascular disease (CVD) is the leading cause of death, with the greatest CVD burden concentrated in the southeastern states.1,2 Within this geographic region, CVD rates are highest among those living in rural communities, those with lower socioeconomic status, Non-Hispanic Blacks, and Native Americans.3,4 Factors contributing to CVD risk in rural communities include consuming fewer fruits and vegetables,5,6 engaging in less leisure-time physical activity, 7 having higher rates of obesity, and having limited access to healthcare,8,9 relative to the US population as a whole. Economic burdens such as lack of insurance and higher rates of unemployment among rural residents also make it difficult to afford health care. In North Carolina (NC), approximately 4 million people, or about 40% of the population, live in one of the state’s 80 rural counties. 10 Despite the increased risk for CVD in rural Americans, few CVD risk reduction interventions are available for rural populations.11-13 This represents a missed opportunity to reduce health disparities by improving modifiable lifestyle behaviors among high-risk individuals.
While there has been some CVD risk reduction intervention research in rural settings,14-16 evidence gaps remain for studies with Community Health Workers (CHWs) among rural Non-Hispanic Blacks. Moreover, we know little about the effectiveness of adapting and implementing CHW-delivered interventions in rural settings, especially among underrepresented populations such as Non-Hispanic Blacks. To address this gap, we developed the Carolina Heart Alliance Networking for Greater Equity (CHANGE) intervention. 17 The CHANGE intervention adapts an evidence-based behavioral lifestyle intervention to reduce CVD risk 18 to be delivered by Community Health Workers (CHWs), defined as frontline public health workers who are trusted members of and/or have an unusually close understanding of the community served. 19 Although CHWs are recommended for delivery of interventions to prevent cardiovascular disease, there is insufficient evidence to guide implementation of CHW interventions in rural, medically underserved areas. We initially tested the feasibility of the CHANGE intervention in one rural, predominantly African American county. 20 The purpose of the CHANGE feasibility study was to assess implementation and effectiveness outcomes with a goal of identifying key refinements needed for more effective implementation of the CHANGE program in a larger study sample. Here, we report on the findings from this larger study testing the CHANGE intervention’s implementation and effectiveness in a sample of high-risk adults living in a second rural, predominantly African American county with a high rate of CVD mortality.
Methods
Design: We evaluated the implementation and effectiveness of the CHANGE program using a type 3 hybrid implementation-effectiveness design, 21 and a single arm, pre-/post-study design. In a type 3 hybrid design, the primary research aim is to determine the impact of an implementation strategy, with a secondary aim of assessing clinical outcomes associated with implementation. Type 3 hybrid designs are used in implementation studies when there are concerns that the intervention may not be delivered with fidelity in real world settings. In CHANGE, this hybrid design fits with the focus on implementation of an evidence-based intervention adapted for CHW delivery in rural public health settings and populations.
The University’s Non-Biomedical Institutional Review Board (IRB) approved and monitored the study. This phase of the study was approved in January 2016 and direct interaction with study participants ended in August 2019. Participants were recruited from a Federally Qualified Health Center (FQHC) and Local Health Department, and all participants provided written informed consent. Participants enrolled at the FQHC also provided consent for study staff to obtain CVD-related lab values from their medical record by signing a separate Health Insurance Portability and Accountability Act (HIPAA) consent form. No medical record information was gathered for participants enrolled at the local health department.
CHANGE Program Content. a
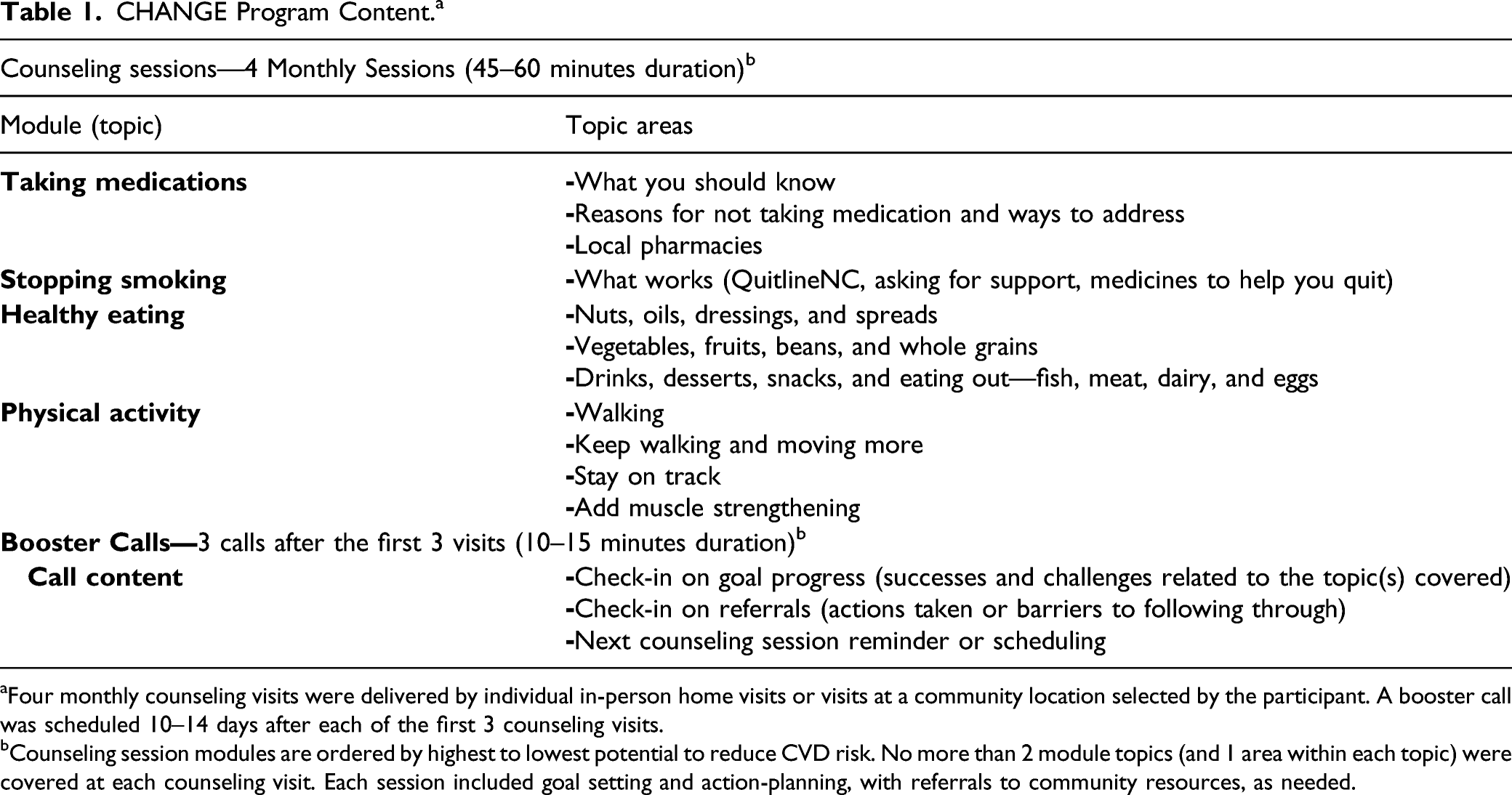
aFour monthly counseling visits were delivered by individual in-person home visits or visits at a community location selected by the participant. A booster call was scheduled 10–14 days after each of the first 3 counseling visits.
bCounseling session modules are ordered by highest to lowest potential to reduce CVD risk. No more than 2 module topics (and 1 area within each topic) were covered at each counseling visit. Each session included goal setting and action-planning, with referrals to community resources, as needed.
CHANGE is a low-intensity (short duration with limited contacts) behavioral lifestyle intervention targeting CVD risk reduction through dietary and physical activity behavior changes, smoking cessation, and medication adherence. (See Table 1 for program content, planned duration of sessions/calls, and order of topics according to CVD risk reduction potential.) The dietary pattern promoted is a southern-style Mediterranean dietary pattern (Med-South) that includes affordable and familiar foods such as peanuts/peanut butter, vegetable oils, and adapted recipes for traditional southern foods such as hush puppies, collard greens, and barbeque. Med-south dietary goals include nuts and beans 3 times/week, at least 7 servings/day of fruits and vegetables, and less than 1 sugar-sweetened beverage/day. The physical activity recommendation is the same as that for US adults—at least 150 minutes/week.
The intervention involved 7 contacts: 4 monthly in-person counseling sessions delivered in participants’ homes or at local venues selected by the participant, and 3 brief booster calls between counseling visits. At the first counseling visit, participants received a manual with the full program content and a resource guide with information on local resources for healthy food, places to be physically active, wellness classes, and medication assistance. To maximize the potential benefits of lifestyle changes, sessions were introduced to participants based first on the participant’s selection of the behavior they most wanted to change, then on the potential CVD risk reduction expected (highest to lowest) by making the behavior change. In a typical session, the CHW covered up to 2 topics related to the participant’s top priority (e.g., healthy eating) followed by a session on another topic (e.g., medication adherence). Each session included goal setting, action planning, and referrals to community resources, as needed.
Site, CHW, and Participant Recruitment: Our study sites included an FQHC and a local health department in Edgecombe County, NC. Edgecombe is a rural county located in the northeastern region of NC, with a population of about 51 000, poverty rate of 21%, and about 58% of the population self-identified as Non-Hispanic Black. 22 In 2021, Edgecombe County ranked in the least healthy quartile (0–25%) for health outcomes and health behaviors, among NC’s 100 counties. 23 Moreover, the county’s age-adjusted stroke, heart, diabetes, and CVD death rates are all higher than the state rates. 24
Inclusion criteria for enrollment included the following: living in or receiving medical care in the county, 18–80 years of age, and speaking English. Pregnant women were excluded or withdrawn, as pregnancy may account for observed changes in weight and blood pressure. The CHW at the health department recruited participants through community outreach, with recruitment tilted toward primary prevention of CVD. In contrast, the CHW at the FQHC recruited through the electronic health record system, with a focus on secondary prevention. Patients were targeted for participation if they were smokers or had uncontrolled diabetes (A1c greater than 8%), hypercholesterolemia (low density lipoprotein [LDL] greater than 130 mg/dL), hypertension (systolic blood pressure >140 or diastolic >90 mmHg), or a previous cardiovascular event. Patients with multiple CVD risks were prioritized.
Staff Training for Intervention Delivery: The research team conducted an intensive 4-day study training (estimated 20 hours) with the staff responsible for participant recruitment and intervention delivery (site supervisors and CHWs). Training sessions included the following content: study protocols, informed consent and participant confidentiality, participant recruitment, CHANGE intervention content, counseling principles (motivational interviewing and adult learning) and practice, community referral resources, and data collection methods.
Measures: Data collection included measures of both implementation and effectiveness outcomes; details have been published 20 and are briefly described here and below. CHWs collected all participant data at counseling visits along with implementation process data related to participant recruitment and program delivery. To assess the utility of specific participant recruitment strategies, a single item asked participants how they heard about the program. Delivery fidelity measures included documentation of participant attendance, efforts used to contact participants missing program sessions/calls, session content and duration, goals set and progress made toward reaching goals, and referrals made with outcomes of referrals. Eligibility screening data used to rank health center patients by CVD risk factors were provided to the study staff through a data sharing agreement.
Implementation Outcomes: Data were collected to assess reach and delivery fidelity. Reach data included the number, representativeness (race/sex), and retention of participants. Fidelity data included number of visits completed, goals set, referrals made to community resources, and disposition of referrals given (action taken and/or services received).
Effectiveness Outcomes: Program effectiveness measures included blood pressure, weight, and self-reported dietary and physical activity behaviors. Outcome measures were collected at the first and last intervention visits. Blood pressure (BP) measurements were taken with an automated BP machine (Omron HEM-907XL, Omron Healthcare, Lake Forest, IL). Three BP measurements (reported as an average systolic and diastolic value) were taken at 1-minute intervals after the participant was seated for 5 minutes. Weight (average of 2 measures) was assessed in pounds to the nearest 10th, using an electronic scale (Seca 874, Seca, Hanover, MD). Self-reported dietary behaviors were measured with items from 2 validated brief food frequency surveys measuring dietary fat quality 25 and estimated intake of fruits and vegetables. 26 A single item adapted from the 2 items used in BRFSS 27 was used to assess usual daily consumption of sugar-sweetened beverage consumption (“On an average day, how many 12-ounce servings of sugar-sweetened beverages do you drink with meals or in between meals? One regular can of beverage is 12 ounces.”). Self-reported data on physical activity behaviors was measured with the RESIDential Environment (RESIDE) survey 28 which was previously modified then validated in a sample of low-income women with overweight/obesity.
Statistical Analysis: Baseline sample characteristics were summarized using descriptive statistics such as means, percentages, and standard deviations. Analyses of participant outcomes and pre–post changes at 4 months were conducted using paired t-tests. We also assessed for group differences between males and females, and age as an independent predictor of pre-/post-changes, after adjusting for baseline sex, diabetes, hypertension, and education. Since intervention effectiveness outcomes were secondary aims in this study, we did not use any imputation methods to account for missing values but provide a description of those lost to follow-up. All analyses were conducted using SAS Version 9.4 (SAS Institute, Cary, NC).
Results
Participant Characteristics.
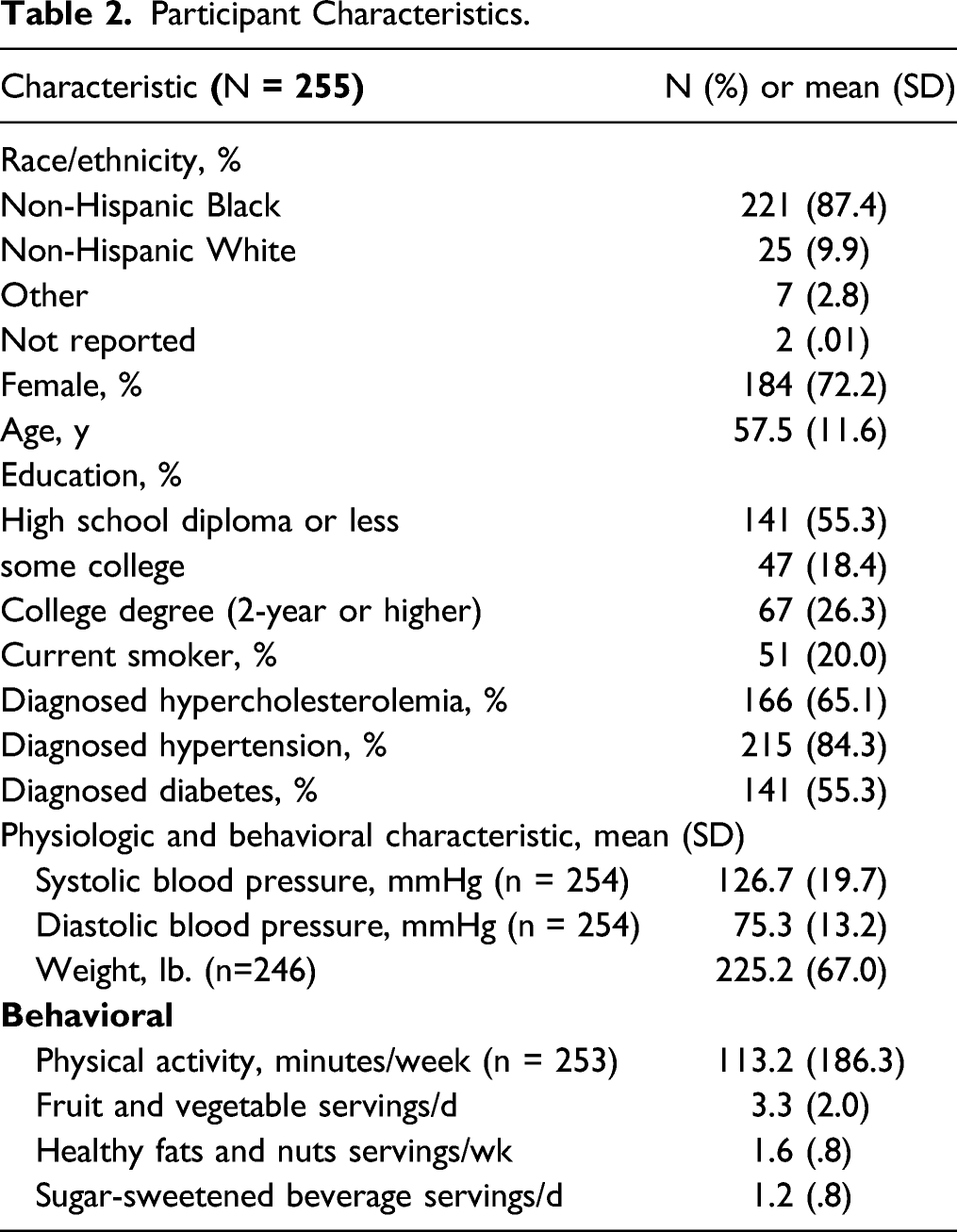
Figure 1 shows the flow of enrolled participants through the CHANGE intervention. Among the 255 study participants enrolled, 87% (222/255) were retained, and 13% (33/255) were lost to follow-up. Those lost to follow-up included 6 participants (15%) who could not be reached, and the remaining 28 (85%) were withdrawn from the study for the following reasons: unable to contact (43%), too busy/no time (32%), no longer interested (21%), and death (4%). Participants lost to follow-up differed significantly from those included in study analysis by age and hypertension diagnosis; no race/ethnicity differences were observed. Those lost to follow-up were on average younger (52 y vs. 58 y, P < .01), and included more participants not diagnosed with hypertension (39% vs. 12%, P < .0001). Participant flow diagram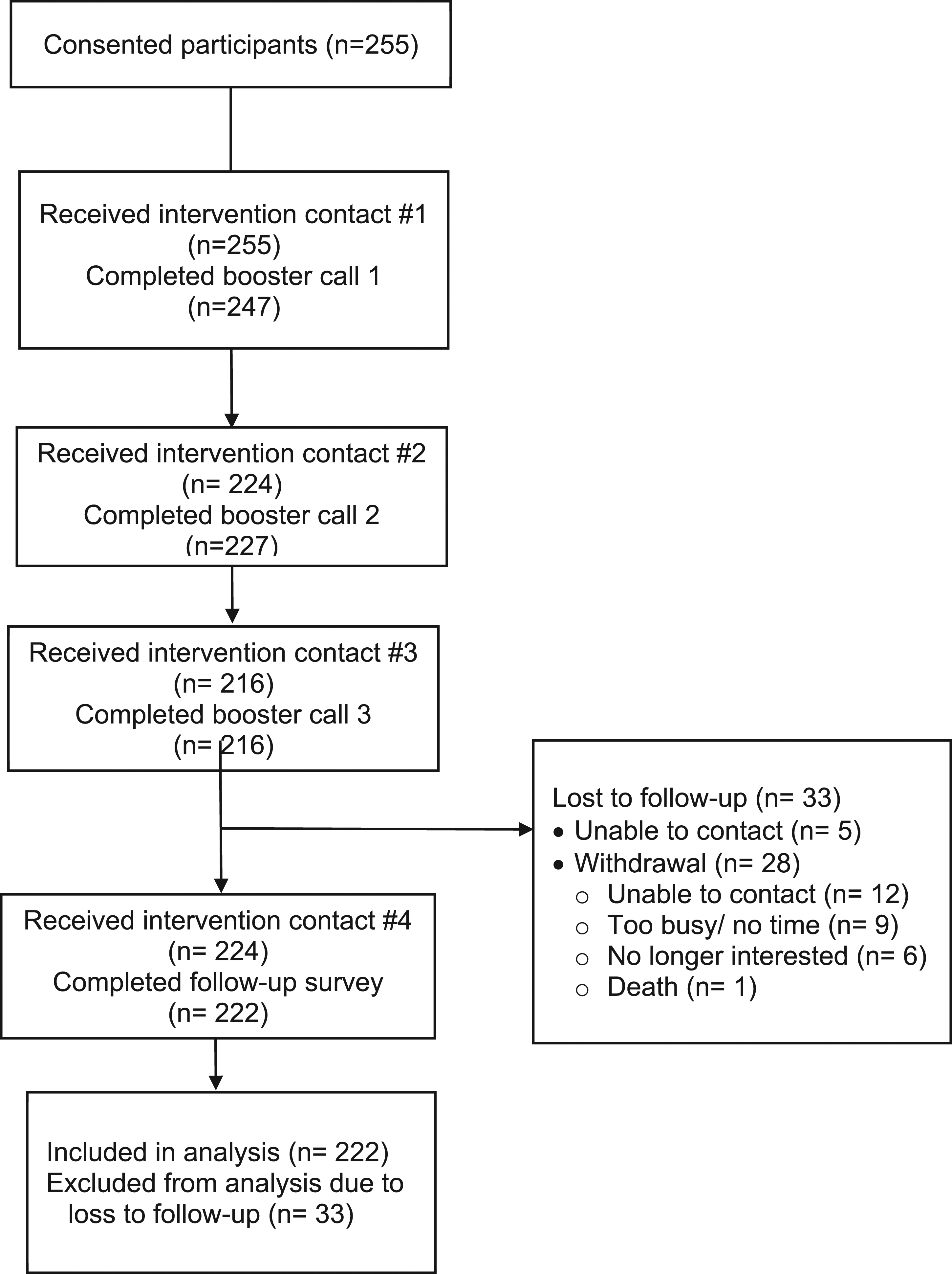
Study participants included 138 (54%) from the community health center and 117 (46%) from the local health department. The ratio of CHW to participants was 1:138 at the community health center where the CHW was full-time, and 1:58 for the two part-time CHWs at the health department.
Implementation Variables (N = 255).
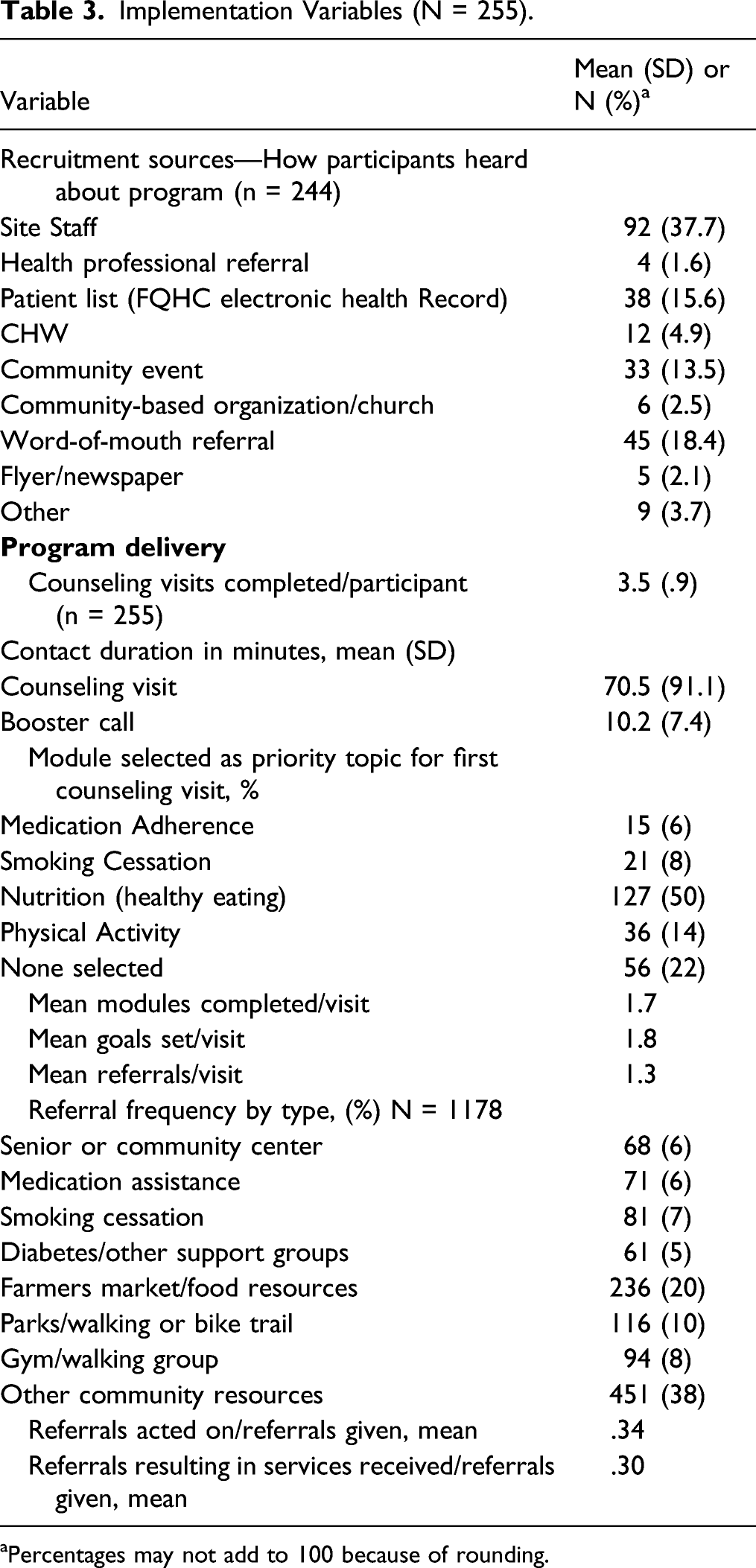
aPercentages may not add to 100 because of rounding.
Implementation of the CHANGE program, as measured by delivery fidelity, showed participants received 3.5 counseling visits on average, with average duration of 70 minutes and 2.7 booster calls on average, with average duration of 10 minutes. The proportion of planned contacts completed by each site differed slightly, with the health department participants completing 89% of all planned visits, while the health center participants completed 94%.
Participants could select the topic (module) considered their top priority and most participants (50%) chose “Healthy Eating” or did not select a priority topic (22%). Physical Activity was chosen by 14%, followed by Smoking Cessation (8%) and Medication Adherence (6%). The average counseling visit included discussion of about 2 topics and goals set, with about 1 referral made. Referrals were made to a variety of community resources, with food-related and physical activity resources accounting for the largest proportion of referrals (38% combined) among those specified. On average, participants given referrals attempted to follow-up on 34% of them and successfully accessed services for 30% of all referrals made.
Program Effectiveness Outcomes.
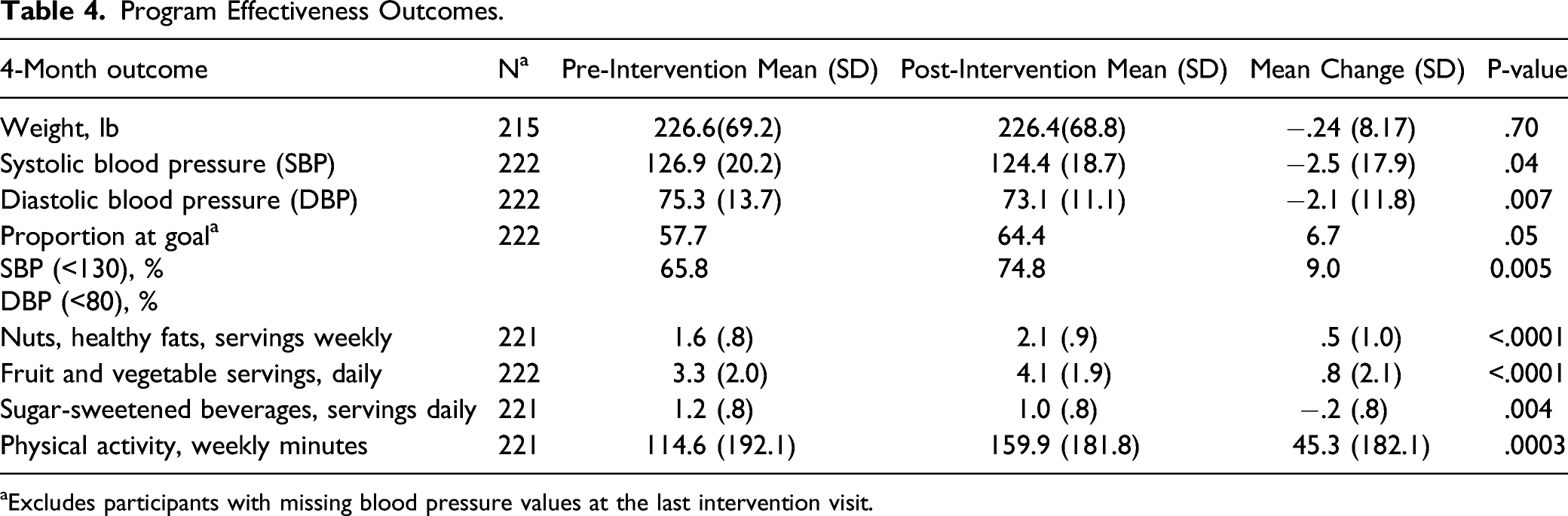
aExcludes participants with missing blood pressure values at the last intervention visit.
Discussion
Our findings demonstrate effectiveness in both implementation and effectiveness of the CHANGE intervention, and compared to our prior feasibility study, 18 several improvements in program implementation were observed. In the paragraphs that follow, we put our results in the larger context of lifestyle interventions and CHW-delivered CVD risk reduction interventions (which are recommended by the Community Preventive Services Task Force), 13 focus on the improvements in implementation effectiveness outcomes, and conclude with implications for future research.
CHW-delivered CVD risk reduction interventions are recommended by the Community Preventive Services Task Force, 13 but very few studies have included rural, diverse populations. The CHANGE study helps to fill that gap. The evidence forming the basis of the Task Force recommendation came from 31 evaluations of interventions including CHWs in different roles. Most (28 studies) were conducted in the US and in urban areas (22 studies), with only 4 studies in rural settings. Thirteen studies used a pre-/post-study design without a comparison group; 23 studies included adults 18–64 years with 5 studies including older adults; and 22 studies enrolled adults from underserved groups (defined as ≥75% African American, Hispanic, or low-income). Ten studies included study populations of more than 75% female while most were evenly distributed by gender. 13
In reviewing the studies included in the systematic review used by Community Prevention Task Force, 13 over one-third (39%) of all studies had follow-up rates of less than 80%. Our rate of 87% points to effective training and implementation procedures. Additionally, we were able to recruit and retain a large sample of rural, Non-Hispanic Blacks, while CHWs delivered the intervention with fidelity to protocols. We also observed program effectiveness outcomes that show promise and compare favorably with similar studies. Most of the CHANGE program content focused on dietary and physical activity behavior changes. From the studies summarized in the Community Prevention Task Force report, 13 we find that among the studies similar in design to CHANGE and delivered by CHWs, all studies reported significant improvements in nutrition and physical activity outcomes. More broadly, there is demonstrated effectiveness of lifestyle interventions among persons with CVD risk factors. 30
A closer look at our dietary outcomes as measured by self-reported fruit and vegetable intake shows that our mean increase of .8 serving per day (an increase of 24% from baseline), compares favorably with overall outcomes of increases between .1–1.4 servings per day (or a 9.7% to 59.3% increase from baseline) reported in reviews of lifestyle interventions designed to increase adult fruit and vegetable intake.30-33 If maintained, our reported increase in nuts intake is similar in magnitude to that observed in the PREDIMED trial’s nut arm where increased nut intake was associated with a 28% reduction in CVD events. 34 General improvements in healthy eating pattern by increased fruit and vegetable intake also contribute to systolic blood pressure reductions, 35 which in turn are associated with risk reductions for major cardiovascular events and all-cause mortality. 36 For our physical activity outcomes, comparing our mean increase of 45 minutes/week (or 40% of baseline) to other rural-based physical activity interventions, 12 we see that among the 8 studies included in this review, only 2 reported significant differences between study arms, and relative to controls the increase in physical activity was 15% 37 and 42% 38 of baseline values. The 40% increase from baseline in CHANGE is an encouraging outcome. The clinical relevance of these dietary and physical activity lifestyle changes is supported by meta-analysis of data showing significant risk reduction of 18% in fatal cardiovascular events among patients engaged in multifactorial lifestyle interventions. 39
When comparing our blood pressure outcomes to studies summarized in the Community Prevention Task Force report, 13 we find that among studies with a non-team-based care model and similar study designs (e.g., pre-/post-test without a comparison group), our outcomes are comparable or better. Defining blood pressure goal as < 130 for systolic and <80 for diastolic pressure, we observed with a 4-month intervention, a 6.7 (systolic) and 9.0 (diastolic) percentage point increase in the proportion of participants with blood pressure at goal. Similar studies in the Community Prevention Task Force report 13 found increases of 1.6 and 4.5 % points among studies that were 6 months or longer in duration. Our 4-month improvements in blood pressure control were much better by comparison. Changes in mean systolic and diastolic pressure in CHANGE were comparable to those reported by studies with a control or comparison group in the Community Prevention Task Force report. 13 Our decrease of 2.5 mmHg in systolic pressure was similar to the median 2.2 mmHg decrease reported (5 studies). Two studies similar to CHANGE found an increase of 2.3 and a decrease of 3.9 mmHg. For diastolic pressure, our 2.1 mmHg decrease is better than the median decrease of 1.3 mmHg reported by 5 studies with a control or comparison group, and an increase of .5 mmHg change in 1 study of similar design to CHANGE.
With the CHANGE study primarily focused on assessing the impact of implementation strategies, after the feasibility study we targeted refinements in 3 areas for this study: pre-implementation planning for staff turnover, CHW and supervisor training improvements, and integrating CHWs into the healthcare delivery team. Our pre-implementation refinements included hiring 2 part-time CHWs (20 hours/week) for the health department site rather than 1 full-time CHW (40 hours/week), to allow for better coordination of task coverage when a CHW took leave time or turned over. We also trained one of our University study staff to deliver the CHANGE program in the event of an emergency. Improvements in staff training involved the following: (1) refining the training content and approaches, (2) adding training specifically for the CHW supervisor, and (3) providing on-going training in the form of monitoring and feedback related to implementation and program delivery. These improvements were accompanied by full retention of our CHW staff.
Other refinements included incorporating regular site meetings between the supervisor and CHW into implementation protocols and regularly monitoring the data CHWs entered into the data management system. By improving implementation planning and staff training, we anticipated improvements in both program delivery fidelity and participant retention, and both were observed. In the feasibility study, 80% of planned contacts (counseling visits and booster calls) were completed; in this phase we completed 91% of planned contacts. Our participant retention showed even greater improvements, increasing from 72% to 87% (with lost to follow-up dropping dramatically from 28% to 13%). The last area of refinement was better integration of the CHW into the health care delivery team. At the FQHC site, the full-time CHW was directly engaged with the primary health care providers and behavioral health staff. With CHW supervision by a Care Coordination supervisor, there were more opportunities for the CHW and the health care delivery team to work together in patient referrals and follow-up.
The strengths of this study are represented by these improvements in both implementation and program delivery outcomes stemming from our ability to successfully refine the strategies used in the feasibility study. This improved study helps to fill a gap in CVD-risk reduction intervention research involving CHWs among rural, Non-Hispanic Black, and medically underserved populations. Moreover, in this study with a rural sample of mostly Non-Hispanic Black adults, we had very high rates of program uptake and study participant retention. One limitation of the initial feasibility study that remains in this study is that of our study design. With a single arm, pre–post study design we are limited in attributing the observed program effectiveness to the intervention itself. As previously mentioned, our focus was on implementation because the CHANGE intervention was adapted for CHW-delivery from an evidence-based intervention. Another limitation is the short study duration relative to behavior change outcomes. Without a follow-up maintenance phase, there is no evidence of how long improvements in behaviors or blood pressure were maintained. To this point, the Task Force identified as an evidence gap, evidence from programs evaluated over periods longer than 12 months. 13 Lastly, even though adults 18–80 years of age were eligible, we observed that those willing to volunteer were predominantly female and midlife in age. While we did not see any differences in program effectiveness by sex, the recruitment of men and younger adults to lifestyle intervention studies is area for improvement in future studies.
In summary, this study demonstrated that refinements to our initial implementation of the CHANGE program produced improvements in both implementation and program effectiveness and provide evidence supporting CHW-delivered lifestyle interventions to reduce CVD risk among rural, Non-Hispanic Black, and medically underserved adults. The potential for public health impact in CVD risk reduction and mortality is enhanced with the observed dietary changes consistent with the Southern-style Mediterranean dietary pattern promoted in the CHANGE program. Recent data from 2 large ongoing prospective cohort studies
40
support the benefits of increasing fruit and vegetable intake on mortality risk reduction and similar health benefits are observed with intakes consistent with a Mediterranean dietary pattern.
41
Moreover, our study findings have statewide implications for the role of CHWs and health promotion programs like CHANGE in North Carolina’s transformation of their Medicaid Program and integration of CHWs into the public health workforce while addressing social determinants of health. In July 2021, NC will begin the transformation of Medicaid from fee-for-service to managed care
42
and with it they will include opportunities to test and evaluate the impact of addressing non-medical drivers or social determinants of health, by providing evidence-based non-medical interventions targeting housing, food, transportation, and interpersonal safety to Medicaid enrollees with high needs.
43
A separate component of these healthy opportunities includes building infrastructure to develop and support the integration of CHWs in the healthcare workforce.
44
Our study findings provide timely and state-specific data to inform these efforts. Beyond the NC context, there are also implications for future research targeting strategies to scale-up these low-intensity behavioral lifestyle interventions in public health agencies. Our results combining lowering of blood pressure with improved dietary habits in a hard-to-reach rural, underserved population suggest that sustaining community-clinical linkages that support chronic disease management and promote health using scalable lifestyle interventions like CHANGE could have a significant public health impact among those at highest risk. Cardiovascular disease (CVD) risk reduction interventions delivered by Community Health Workers (CHWs) are recommended by the Community Preventive Services Task Force, but very few studies have included rural, racial, and ethnically diverse populations. Evidence gaps remain for implementation and effectiveness studies of CHW-delivered interventions in rural settings and among underserved Non-Hispanic Black populations. Using a hybrid implementation-effectiveness study design, we evaluated the implementation and effectiveness outcomes of a CHW-delivered, CVD risk reduction intervention in a sample of mostly Black adults living in a rural setting with high rates of CVD mortality. Our results in a hard-to-reach rural, underserved population suggest that sustaining community-clinical linkages that support chronic disease management and promote health using low-intensity, scalable lifestyle interventions delivered by CHWs could have a significant public health impact among those at highest risk.So What?
What is already known on this topic?
What does this article add?
What are the implications for health promotion practice or research?
Footnotes
Acknowledgments
We gratefully acknowledge our community research partners at Edgecombe County Health Department and OIC Family Medical Center, and the community members who decided to participate in CHANGE. The authors also acknowledge the assistance of the site staff (Karen Lachapelle, Cheryl Fisher, Brian Ellerby, Patricia Neville, Becky Hollis, Tisa Roberts, Bridgette Luckey, and Kim Barnette) and CHWs (Donia Simmons, Angela Heath, and Tanya Murray), and the IT staff at UNC Sheps Center (Jack Ward, Maria Tobin, and Gary Hunt).
Authors’ Contribution
Conception and design of the study (JL and SC); data acquisition (AB, AE, and SA); data analysis and interpretation (ZG, CS-H, and SC); drafting or substantively revising text (CS-H, JL, SA, and SC). All authors read and approved the final manuscript.
Declaration Of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Centers for Disease Control and Prevention grant U48/DP005017.
Clinical Trial Registration
ClinicalTrials.gov: NCT03582696.
Ethnical Approval
University of North Carolina at Chapel Hill, Institutional Review Board Application Approval–Application #15-2822.
Informed Consent
All participants provided written informed consent.