
Abstract
Purpose:
The PRECEDE-PROCEED model (PPM) is a community-based participatory research (CBPR) framework for health promotion, yet the direct application of the PPM into practice is unclear. This paper describes how the PPM was adapted for the development and application of a pilot intervention study to promote outdoor physical activity (PA) in older adults (OUTDOOR ACTIVE). We illustrate the steps and adaptations we applied to put the PPM into practice and present the developed interventions.
Design:
The PPM was adapted by incorporating a socio-ecological model. This ensured the design of any resultant intervention would explicitly address multi-level determinants of physical activity. The list of possible program components to select from for the design of an intervention was also extended.
Setting:
Bremen, Germany.
Participants:
Participants in the intervention development were 924 noninstitutionalized older adults, aged 65-75 years (response: 25.2%), living in Bremen-Hemelingen, Germany. For implementation of the intervention and to ensure sustainability, several groups of stakeholders were involved throughout the process.
Methods:
A mixed method design was employed (e.g., focus groups, quantitative survey) to identify determinants. A round table and participatory workshops were held to involve the target group and community stakeholders in the design of an intervention using the adapted PPM model.
Results:
A conceptual model was developed illustrating the integration of a socio-ecological model into the PPM. The model received ecological validity, as it was affirmed by community stakeholders as an appropriate method for designing a community-level PA intervention. Target goals to address PA determinants were selected by target group members. An intervention to meet the goals was developed and implemented with target group input.
Conclusion:
The adapted PPM is a promising starting point for developing multi-level interventions. Steps should be taken to ensure all social groups are participating in the process and all levels of determinants are addressed.
Purpose
The proportion of older adults in Europe is increasing, raising the need for strategies to promote healthy ageing. 1 Meta-analytic evidence from longitudinal studies suggests that physical activity (PA) is an important contributor to healthy ageing 2 ; yet PA declines with age. 3 For example, more than 80% of older adults in Germany aged 60 to 79 do not meet World Health Organization (WHO) recommendations of at least 150 minutes moderate PA per week. 4
Increasing levels of PA through PA promotion programs, however, remains challenging which is reflected by highly heterogeneous effect sizes. 5,6 One promising approach for PA intervention development is community-based participatory research (CBPR), as it actively involves the community as well as communal stakeholders, 7 and therefore has the potential to reduce health inequalities. 8 This approach is considered to be particularly effective, if a socio-ecological model (SEM) is applied that takes into account the interplay of individual and environmental determinants of PA. 7
The PRECEDE-PROCEED model (PPM) 9 is a framework that helps identifying specific intervention targets, allows the integration of individual and environmental factors into one concise program, and includes consideration of organizational, administrative and policy aspects that might hinder or support the practical implementation of a program. Research using the PPM approach for development of PA interventions 10 -12 shows promising preliminary first results regarding outcome, as well as reach of the implemented programs. 13,14 However, the precise steps on how to apply the PPM are not outlined in detail: For instance, the PPM lacks a framework for the concrete development of the intervention. 12,15 Moreover, transfer of the PPM phases into action has been realized in different ways across studies since a comprehensive guide is missing, 16 underlining the need for methodological work in this field.
The present paper aims to describe how the PPM was adapted for the development and application of a pilot intervention study to promote outdoor PA in older adults (OUTDOOR ACTIVE). Specifically, we illustrate the steps and adaptations we applied to put the PPM into practice and present the developed interventions and their outcomes. The research project OUTDOOR ACTIVE is 1 of 5 subprojects forming the AEQUIPA (physical activity and health equity: primary prevention for healthy ageing; http://www.aequipa.de/) health promotion network. 17 The central aim of OUTDOOR ACTIVE is to promote outdoor PA in older adults, aged 65-75 years, applying a CBPR approach based on an adapted PPM. 9 In the first part of OUTDOOR ACTIVE (OUTDOOR ACTIVE pilot study, 2015-2018) this approach was further developed, made explicit, and applied in one community.
Approach
In the following, we describe the adapted PPM that we developed in the preparatory phase and that guided the OUTDOOR ACTIVE project. These adaptations were done such that the adapted PPM allows incorporating recent literature on determinants for physical activity.
In general, the PPM is carried out in 2 distinct steps: Firstly, the 4 PRECEDE phases serve as a thorough needs assessment and the development of an intervention program customized to the needs and situation of the community. Secondly, the 4 PROCEED phases comprise the implementation and evaluation of the developed intervention program. 9,16 In OUTDOOR ACTIVE, we extended the PRECEDE phases of the classical PPM regarding its underlying theoretical models. Consequently, we re-named some of the phases of the PPM to reflect these changes (see Table 1).
Adaptations and Application of the PRECEDE-PROCEED Model in OUTDOOR ACTIVE.
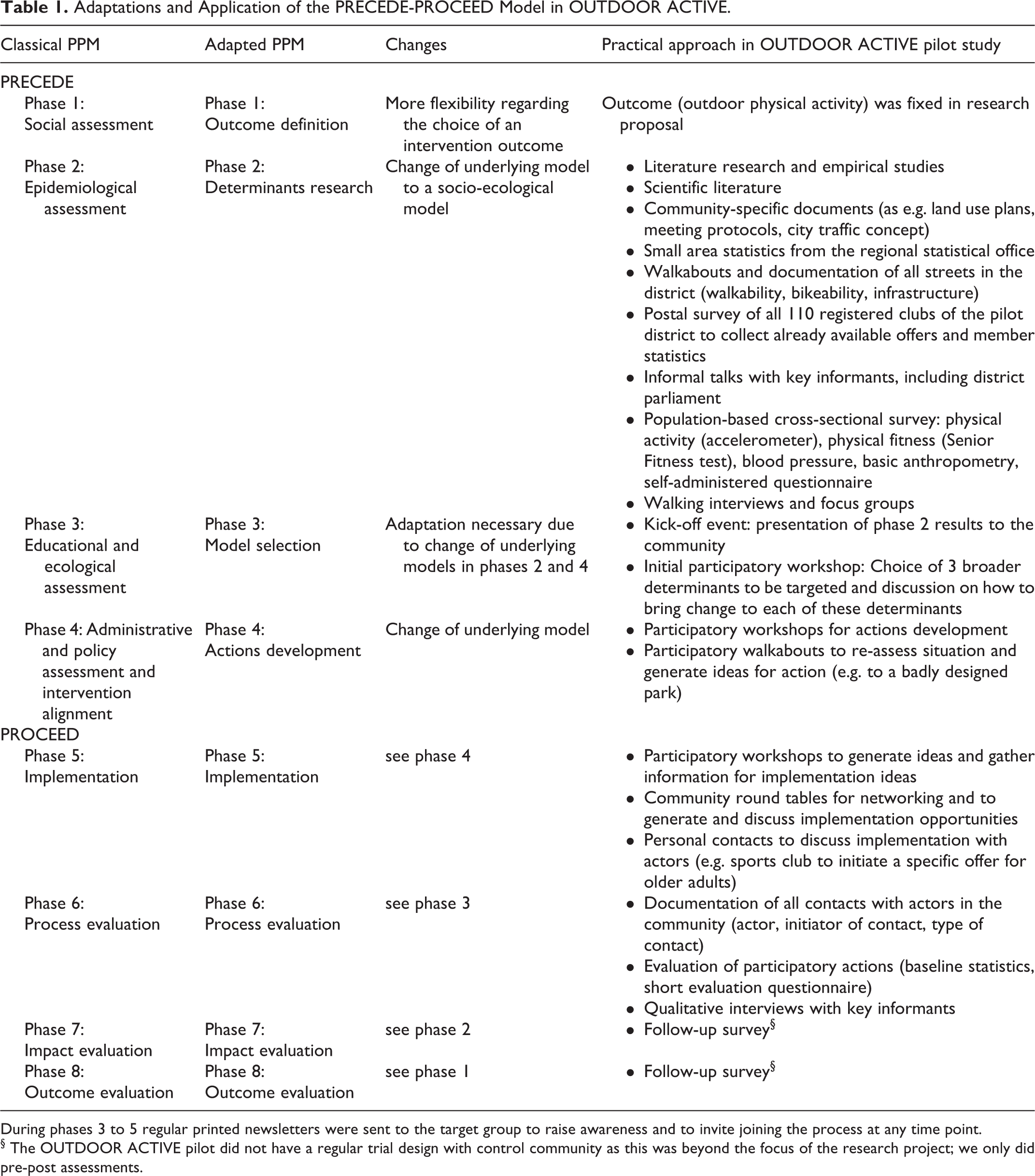
During phases 3 to 5 regular printed newsletters were sent to the target group to raise awareness and to invite joining the process at any time point.
§ The OUTDOOR ACTIVE pilot did not have a regular trial design with control community as this was beyond the focus of the research project; we only did pre-post assessments.
In the classical PPM approach, the intervention outcome is identified as part of the research process in phase 1. However, often the outcome has to be fixed in the research proposal and in this case the authors of the PPM suggest “to start in the middle of PRECEDE and work in both directions (p.86),” 9 which seems a somewhat unclear instruction. To improve clarity, we decided to keep the process of identifying the outcome completely in phase 1. This explicitly includes the classical approach of identifying the most dominant health problem that impacts the quality of life of the target population, but it also allows to choose the outcome solely based on own research findings or the literature. In OUTDOOR ACTIVE, the intervention outcome outdoor PA was fixed beforehand in the research proposal.
In phase 2 of the PPM approach, the main determinants of the selected health problem are identified. The most current version of the PPM distinguishes between behavior, environment, and genetics, a categorization that stems from the classical risk factor definition in epidemiology.
9
However, the PPM does not include all socio-ecological determinants, suggested by contemporary theory and research.
18,19,20
For example, interpersonal factors are missing in the list of determinants provided by the PPM. Taking into account more recent theoretical and empirical contributions with regard to determinants of health, we re-wrote the set of categories according to an integrated behavioral model.
21
Societal / structural factors, comprising organizational, institutional, or cultural factors Community factors, comprising the physical and social environment Interpersonal / household factors, comprising interactions between individuals All individual factors, except habitual factors Habitual factors, referring to all factors related to habit formation of an individual
All 5 categories presented in the previous list comprise elements that are fixed (e.g. age), coined “contextual factors” by Dreibelbis and colleagues, 21 and potentially modifiable factors. The extension of categories in phase 2 required re-writing of phases 3 and 4 because these could no longer be based on health behavior models alone. Moreover, we wanted to allow integration of modern health behavior models. 22 Models for phase 3 derive from a broader range of models as for instance health behavior models, policy models, or generic change models. 23 -26 Key is that the selected model is suitable for changing the selected determinant. Lastly, we extended the categories for phase 4 where the measures for the health program are developed and put into practice. Our approach relies on the Ottawa Charter of the World Health Organization 27 and the work of Whitelaw 28 to ensure that all elements of a health program are covered. The new categories are:
Development of
Building and implementing healthy
Re-orienting
Re-shaping
Building
Strengthening
Each selected determinant of phase 2 can now be translated into actions covering one or more of the generic categories of phase 4 by employing the model selected at phase 3. The adapted PPM, and its interrelation to SEM, is depicted in Figure 1.
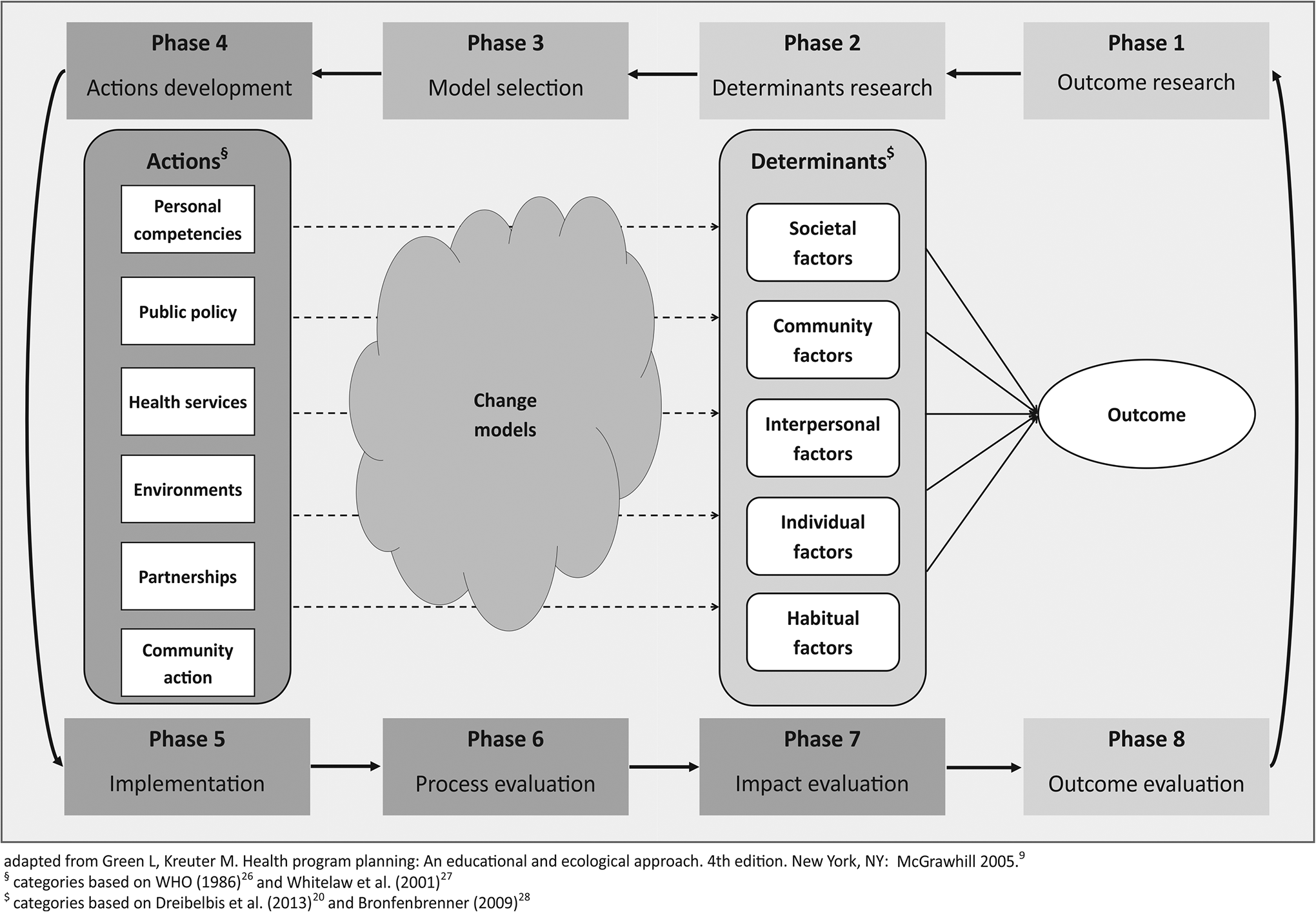
Adapted PRECEDE-PROCEED Model Used in OUTDOOR ACTIVE. The process starts with identification of the outcome (phase 1) and its main determinants (phase 2). One or more change model(s) are selected (phase 3) and actions for changing the determinants are chosen (phase 4). After implementation (phase 5), evaluation of the process (phase 6), impact (phase 7) and outcome (phase 8) take place. The cycle can be started again with the same or a different outcome.
Setting
Bremen is a commercial and industrial city of around 550,000 inhabitants located in the north-western part of Germany (former Federal Republic). The OUTDOOR ACTIVE pilot study was conducted in 1 of the 19 districts of Bremen, called Hemelingen, from 02/2015 to 01/2018. The pilot district Hemelingen currently has 42,415 registered inhabitants, 4,332 of these in the target age group of OUTDOOR ACTIVE, 65 to 75 years. Hemelingen consists of 5 sub-districts: Hastedt, Sebaldsbrück, Hemelingen (sub-district), Arbergen, and Mahndorf. Albeit directly bordering to each other, the 5 sub-districts are highly heterogeneous with regard to their history, socio-economic situation of their inhabitants, and their land use mix. Some key characteristics of the 5 sub-districts can be found in the supporting material (see S1 Table).
Participants and Method
A mixed methods approach was used in OUTDOOR ACTIVE (see Table 1).
We initially gathered district-specific relevant information from any existing available data (e.g. land use plans, meeting protocols, and traffic concepts). We obtained small area statistics from the regional statistical office to get
For phase 2, empirical data was collected using several approaches: To gather information on barriers and motivations for PA, 3 semi-structured
Additionally, 7 individual narrative
To document the built environment with regard to walkability, bikeability, presence of basic businesses (as e.g. shops), and infrastructure (as e.g. benches), the 383 streets in the pilot district were assessed on foot by observers using a
To explore sports opportunities and level of participation in the target group, a short questionnaire was mailed to all 110 registered clubs in the district to assess available offers with regard to physical activity and participation of the target age group. 36 of the registered clubs were not considered eligible (18 associations with corporate members, 14 regional clubs not operating in the district, 4 youth clubs), 38 of the remaining 74 clubs did respond (response proportion: 53%), of these 17 sports clubs. All eligible larger clubs (>99 members) responded to the survey.
To investigate associations with level of physical activity, behavior and attitudes we invited the full sample of 4,332 residents of the pilot district, aged 65 to 75 years to participate in a
Moreover, several
The AEQUIPA / OUTDOOR ACTIVE study was approved by the Ethical Board of the University of Bremen.
Results
Application of the Adapted PPM
The determinants for outdoor PA identified in our formative work described above (e.g. quantitative survey, focus groups) are depicted in Table 2. The research team grouped them into targets and non-targets. All societal determinants and those community determinants related to industry (noise and smell) or to citywide factors (traffic regulations) were categorized as non-targets. On the interpersonal, individual, and behavioral/ habit formation level, the following determinants were categorized as non-targets: a) determinants that were considered not changeable (age, sex, sports behavior in childhood), b) determinants that relate to a person’s own health or that of others (prevalent diseases, caring for others), c) composition of household and household activities (walking the dog and gardening), d) personal values, and e) income (unsatisfied with financial situation). This left 31 out of 53 identified determinants as optional targets for intervention development. Using this approach, we identified potential targets from all but the societal level. For the community level, only barriers were identified. These encompassed a perceived neglected neighborhood, especially in the Hemelingen sub-district (54.7% in this district reported littering and 54.1% fear of crime), barriers to active travel (lack of crossings, poor state of bike lanes); lack of free and non-committal offers and offers for health-impaired persons. Lacking infrastructure in the environment as e.g. public toilets and benches for talking to other people or for resting opportunities were repeatedly pointed out as being barriers to active travel. In the baseline survey, 18.4% of women and 11.1% of men reported urinary incontinence and 34.1% of women and 24.0% of men were restricted in their mobility. Less than good subjective health was reported by 23.6% of women and 18.3% of men.
Determinants Identified in Phase 2 in OUTDOOR ACTIVE.
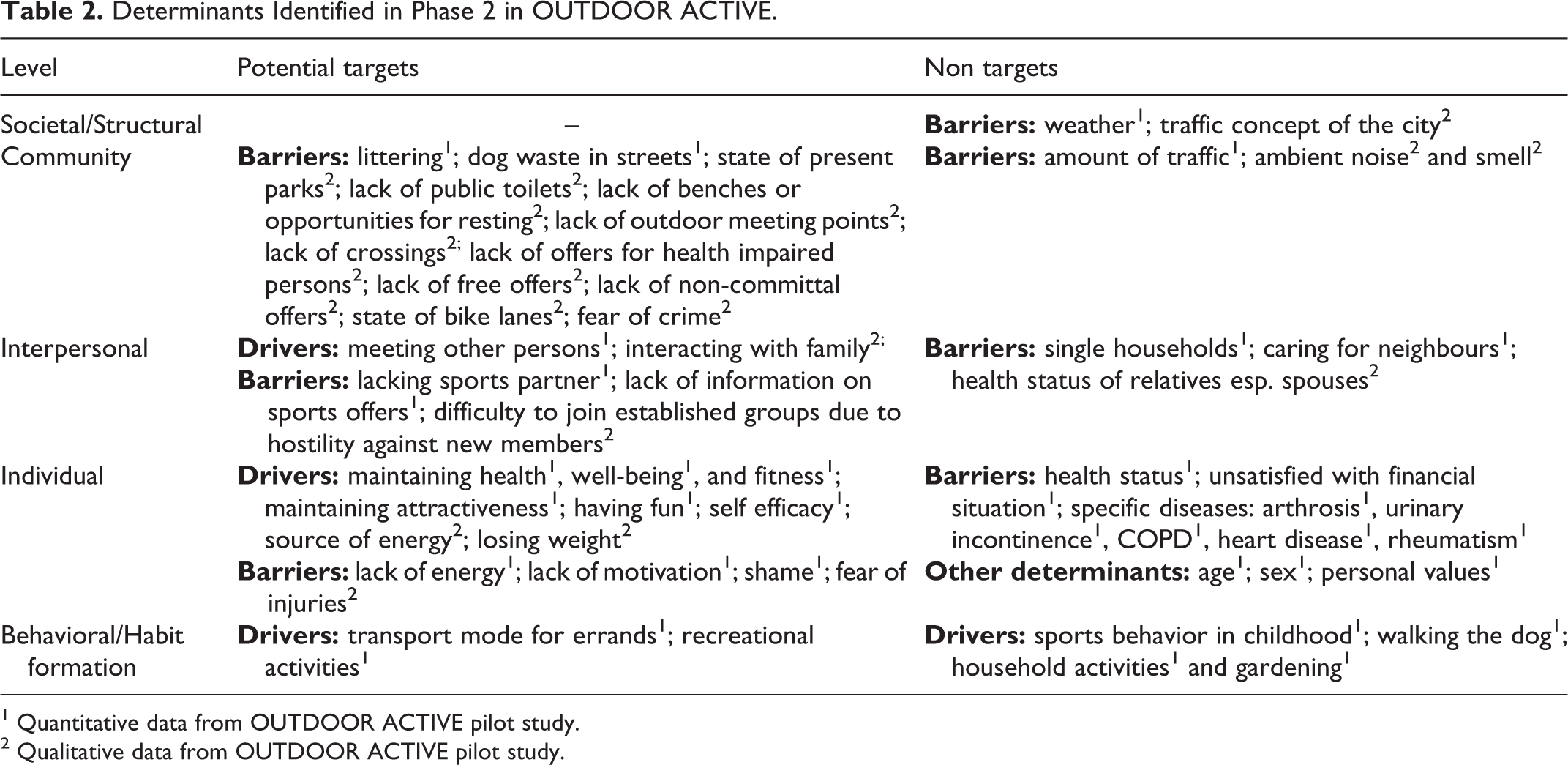
1 Quantitative data from OUTDOOR ACTIVE pilot study.
2 Qualitative data from OUTDOOR ACTIVE pilot study.
We identified several possible targets on the interpersonal level emphasizing the need for integrating this level into the PPM. An important driver is that sports activities and outdoor physical activities give opportunity for social contacts, which is especially important for those living alone (Women: 35.6%; Men: 12.8%). As one participant from a biking group puts it:
You want to socialize; everyone wants to be together, to exchange ideas. The physical activity on top is of course beneficial, that’s clear.
Barriers can also be found on the interpersonal level. Apart from lack of a sports partner and lack of information, we found interpersonal conflicts as one important barrier to joining existing groups:
I didn’t get warm there [the gymnastics club]. So I came in and hello, that’s the new one, but that was it. And you wouldn’t be talked to after that [..] I don’t think they even noticed that I stopped going there.
Another participant observed:
[..] I know, also from the sports groups here in Hemelingen, because I also worked as a trainer that cliques like to form and that they’re not always open to others.
As potential targets on the individual level, perceived positive benefits regarding health (89.6%), well-being (85.0%) and attractiveness (41.8%) were drivers for physical activity, whereas perceived lack of time (30.3%) and lack of motivation (13.2%) were among the barriers. Despite being in retirement, lack of time was not uncommon. A statement in one of the focus groups is typical for those participants that were more socially active:
That is just the pensioner’s life. Pensioners, they say, pensioners never have time and I really do, that’s really the case with me, so there’s always a lot going on.
Another important level was habit formation. Using the bike for errands (50.9% men and 47.1% women reported that the bike is their usual mode of transport for at least one destination) and regularly going for walks in the neighborhood are among the habits that lead to higher physical activity levels. One participant explains that he still goes on the daily walks he used to go with his dog:
And I also love to go for a walk. Until 2 years ago I also had a dog. He is no longer with us, but I still go for a daily walk [..] I love to do it.
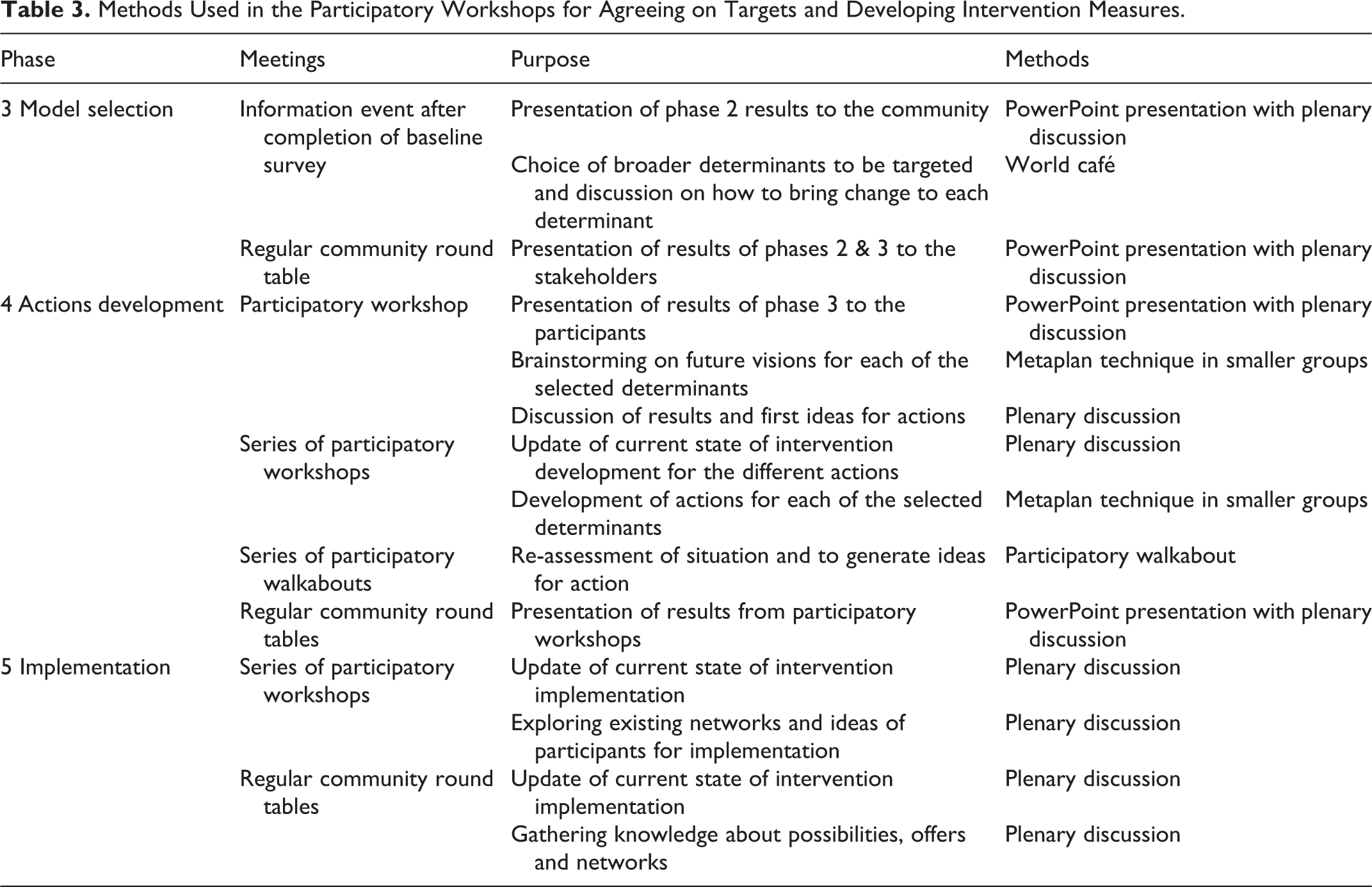
The process of agreeing on targets and developing intervention measures as well as the used methods are shown in Table 3. The results from phase 2 were presented to the community in an information event with 158 participants using a slideshow before conducting a world café 30 (see Figure 2). This method was used to narrow down the possible targeted determinants and to discuss ideas on how to address each PA determinant. It was then decided to conduct the participatory workshops of phase 4 in the 5 sub-districts separately, because of the huge response. The meetings focused on actions development, where the results from the initial workshop were presented and discussed using mainly the Metaplan technique 31 and group discussions. Moreover, knowledge and participants’ connections within the community, that could be helpful for the implementation of the intervention measures, were gathered. Participatory walkabouts were carried out to re-assess the situation and generate further ideas for action. The results from the participatory workshops were regularly presented to the community stakeholders during round tables. To develop ideas and gather information for implementing the intervention measures in phase 5, the Metaplan technique and group discussions were used as well.
Methods Used in the Participatory Workshops for Agreeing on Targets and Developing Intervention Measures.

Information Event in Phase 3, 09/26/16. Photograph taken by the OUTDOOR ACTIVE team, all participants gave consent to publish.
Eventually, 8 of the 31 generated targets for intervention development were chosen by the participants with no interference of the research team (see Table 4). Only barriers were chosen; 6 out of 12 on the community level (50%), 2 out of 3 on the interpersonal level (67%) and 0 out of 4 on the individual level (0%). Subsequently, intervention measures were developed with the participants, and ideas for their implementation discussed in the workshops as well as in the community round table. For ease of workflow, we decided to apply the same generic change model for all determinants, in our case the model by Kotter. 32 For the implementation, a descending order of priorities was applied. The first priority was to utilize existing stakeholders and infrastructures, for example by integrating measures, such as starting a Nordic walking group in an existing sports club. Second priority was to establish new structures or groups within the district as for example the OUTDOOR ACTIVE scouts, a group that was founded to tackle the littering problem of the district. Last priority was to implement the measure ourselves. One example is the organization of district walks which none of the stakeholders was willing to organize. In total, 14 intervention measures were developed and implemented (see Table 4). Of these, the majority (11 of 14: 78.6%) was on the community level, 2 measures dealt with the interpersonal level, and one concerned habit formation.
Intervention Measures Developed and Implemented With Participants.
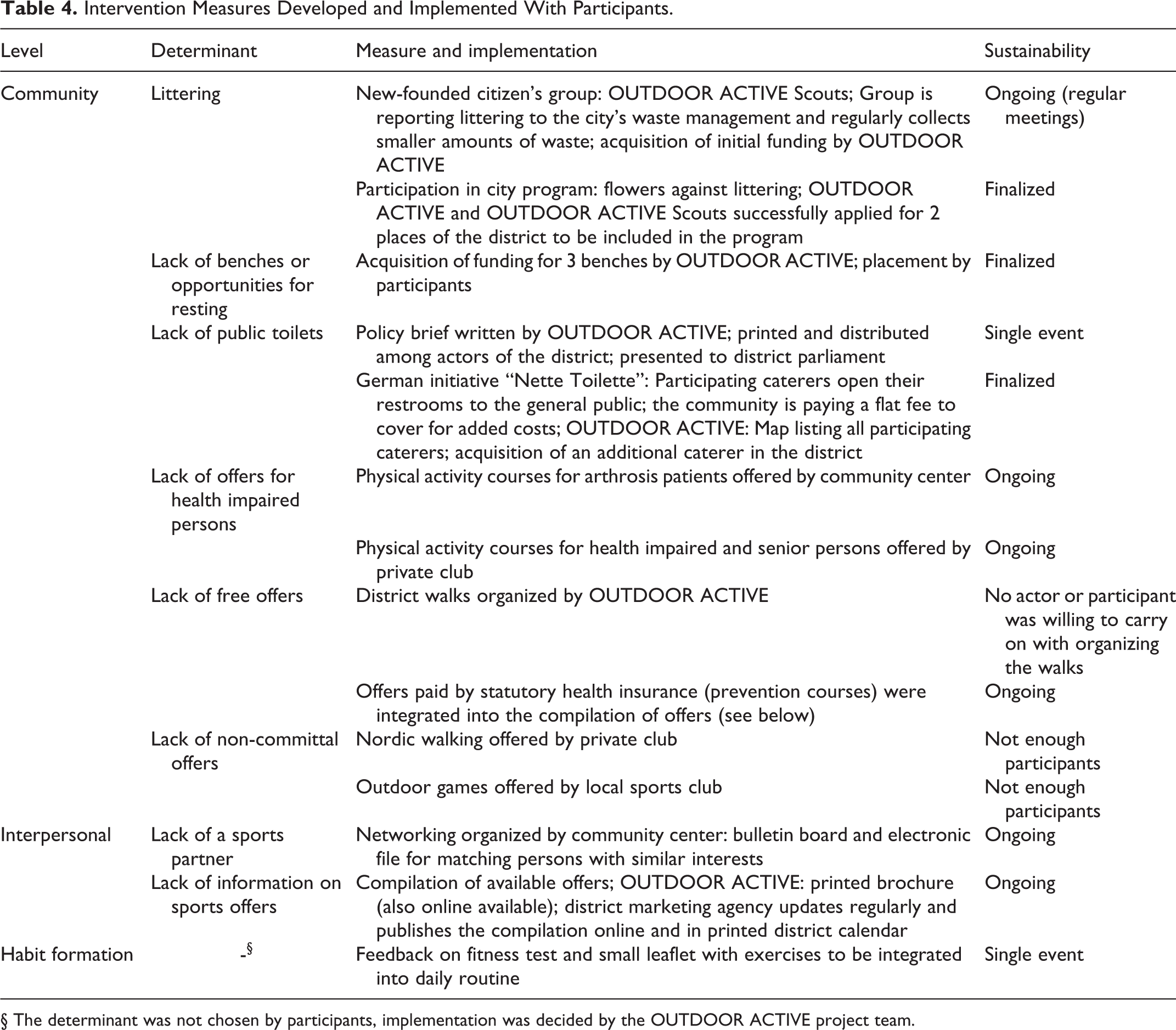
§ The determinant was not chosen by participants, implementation was decided by the OUTDOOR ACTIVE project team.
Discussion
Mounting evidence suggests that the PPM is a well-suited framework for the development of health interventions. 33 -36 While the PPM is a generic framework that can be applied flexibly, it does not provide clear guidelines regarding its translation into practice. 15 The aim of this paper was to illustrate how we adapted and applied the PPM to develop a physical activity intervention for older adults in a large pilot study and to present the results of this study. With regard to the PPM, we incorporated a socio-ecological model and adjusted the classical PPM accordingly. While the PROCEED step (phases 5 to 8) remained unchanged, we extended the set of categories for health determinants in phase 2 and made explicit that determinants have to be selected from the large range of possibilities for a specific program. Due to our extension of potential health determinants, we further generalized the model incorporated in phase 3 from a health behavior model to a broader range of models, so that, depending on the health determinant, a suitable change model can be chosen. If, for example, the aim is to change the speed limit in a district, a policy model which involves agenda setting and coalition building is more appropriate than a human behavior model. Lastly, we updated the list of action categories in phase 4 according to current WHO practice and further work by Whitelaw 27,28 (see Figure 1).
Applying the adapted PPM to develop a physical activity intervention targeted at 65-75 years-old residents of the OUTDOOR ACTIVE pilot community, a large heterogeneous district in Bremen, Germany, resulted in a set of 14 intervention measures from 3 of the 5 categories of determinants. Overall, our experiences with the adapted PPM have been very positive. The adapted PPM captured the wide range of determinants of outdoor PA in our sample and allowed for a nuanced categorization of potential intervention targets. We were successful in ensuring sustainability for most of the implemented intervention measures by utilizing existing clubs and infrastructures whenever possible. It worked in our favor that we were welcomed very generously in the community and that we had 3 years of time for the OUTDOOR ACTIVE pilot study, as our approach was time intensive. Especially establishing a good network within the community, which is a vital task for success, is time consuming and it also takes time to build trust. We visited all relevant local stakeholders to present and discuss the project, we presented several times to the district parliament, we engaged in existing local networks and activities, and we held contact to the local press. All empirical work, including the population-based surveys, and all participatory workshops were not done in the university but in the district (participatory workshops and focus groups) or even in each of the sub-districts (survey and walking interviews). Apart from lowering the barrier to participate the choice of locations also helped shifting power from researcher to participants. One participant stated during process evaluation:
That [participation in the survey] was a home game for me. It took place at our parish hall, where I totally feel at home.
Despite these positive experiences, we noticed a number of limitations when applying the adapted PPM. The selection of optional intervention targets from quantitative data was based on p-values. Thus, we might have missed determinants that are relevant for physical activity but that failed reaching statistically significance (false negatives).This might introduce bias, 37 however, since we also drew information from the qualitative studies, and included determinants that were mentioned in these studies, although they did not reach statistical significance in the quantitative study, the danger of omitting variables is reduced compared to purely quantitative studies.
Even though the sample of the survey was overall representative of the population of Hemelingen, and we thus got a clear and unbiased picture on the key determinants for physical activity in the age group 65 to 75 years, the participants of the intervention development and implementation in phase 3 to phase 5 were mainly outspoken and active members of the district (e.g. members of the church or politically active individuals). While these participants were very active and helpful during the workshops and beyond, helping us to get in contact to different stakeholders in Hemelingen, they only represented a small proportion of the population of Hemelingen. This is a common problem of participative research designs. 38
When selecting intervention targets, participants only chose targets on the community (e.g. littering, lack of free offers) and interpersonal level (e.g. lack of a sports partner). Determinants at the individual or behavioral/ habit formation level remained largely unaddressed. Considering that individual and behavioral/ habitual factors are important determinants of PA, 18 interventions should ideally include these determinants as well. Participants’ decision to focus on community-related and interpersonal determinants could have been affected by the design of the intervention. For instance, participants in the OUTDOOR ACTIVE pilot study decided upon intervention targets in a group setting. First of all, it might have been easier to find consensus on determinants at the community and interpersonal level. Second, it is possible that participants thought that they could work on individual and behavioral/ habitual factors themselves and perceived the group setting as a chance to tackle community-related and interpersonal determinants. As one participant put it:
OUTDOOR ACTIVE is not only about physical activity of older residents. It is about how we take care of our district and this is also a very important topic. (Workshop participant, OUTDOOR ACTIVE process evaluation).
Third, participants may felt hesitant to admit that individual and behavioral/ habitual factors had kept them from being physically active, as they might perceive these factors (e.g. lack of motivation) as a personal weakness they do not wish to deal with or share with others. Alternatively, they might have been worried that advocating for individual factors such as a lack of motivation as intervention target implies that others have the same issue.
Further research is necessary to gain insights into why participants focused on determinants at the community and interpersonal level and on participants’ decision process on intervention targets. Apart from investigating the underlying mechanisms, different practical approaches should be studied for this crucial point in the PPM process. One possibility is to bring the levels of determinants more actively into the discussion process, for example addressing them from community level to individual level.
Past research has highlighted a number of strategies that, while time intensive, may help to ensure that community members that belong to minorities or socially disadvantaged groups are better represented in CBPR projects. These include word-of-mouth recruitment and contacting potential participants from these groups multiple times through language-congruent members of the research team. 39 -41 Future research should further experiment with these possibilities. A different route might be to explore methods that do not require such a high level of language skill as e.g. the Metaplan technique is demanding. Possibilities comprise participatory walkabouts, community maps, community art or brick-building. 42 -45 These methods could also help give introvert characters a voice that would otherwise be silent at group meetings.
From our experiences, key to a successful CBPR approach are trust building and networking within the community. 8,46 Especially, gathering basic information and current administrational and political plans and topics of the district at the start of the study; this was an important step for gaining credibility within the pilot district when talking to stakeholders or participants. Moreover, this knowledge was important for ensuring sustainability of the implemented intervention measures. Equally important, researchers and practitioners have to be open to the process and its outcomes, and commit to the general rules of participatory research. This includes that researchers continuously critically reflect on their roles, which was a regular topic of discussion in our research team meetings.
Conclusion
In this pilot study, we adapted the PRECEDE-PROCEED model (PPM) to conform to modern theory. A socio-ecological model (SEM) was incorporated to ensure multi-level PA determinants were addressed, resulting in the list of possible program components to be extended to encompass components suitable for all levels of the SEM. The adapted PPM was applied to develop an outdoor physical activity intervention for older adults in an urban community in Germany, where interventions were developed on multiple levels. Future work should focus on involving all social groups in the process and addressing all SEM levels of PA determinants.
So What?
What is already known on this topic?
Developing effective PA promotion programs for older adults remains challenging. Health interventions employing community-based participatory research (CBPR) frameworks, such as the PRECEDE-PROCEED model (PPM) have provided some encouraging results. While the PPM is a widely used framework for health interventions, it lacks clarity regarding its translation into practice.
What does this article add?
This article illustrates how the classical PPM was adapted to incorporate modern theory on health determinants and health promotion practice. It showcases the practical application of the adapted PPM by presenting the OUTDOOR ACTIVE pilot study, a project that uses the adapted PPM to promote outdoor PA in older adults.
What are the implications for health promotion practice or research?
The adapted PPM is a promising starting point for developing multi-level interventions using a CBPR approach. In practice, steps should be taken to ensure all social groups are participating in the process and that all levels of determinants are addressed. Further research is needed on decision-making in such complex situations.
Supplemental Material
Supplemental Material, sj-pdf-1-ahp-10.1177_0890117120974876 - Promoting Physical Activity Among Older Adults Using Community-Based Participatory Research With an Adapted PRECEDE-PROCEED Model Approach: The AEQUIPA/OUTDOOR ACTIVE Project
Supplemental Material, sj-pdf-1-ahp-10.1177_0890117120974876 for Promoting Physical Activity Among Older Adults Using Community-Based Participatory Research With an Adapted PRECEDE-PROCEED Model Approach: The AEQUIPA/OUTDOOR ACTIVE Project by Karin Bammann, Carina Recke, Birte Marie Albrecht, Imke Stalling and Friederike Doerwald in American Journal of Health Promotion
Footnotes
Acknowledgments
We are grateful to our participants and local actors in Bremen-Hemelingen who supported the whole research team. We thankfully acknowledge the numerous valuable discussions with our colleagues from the AEQUIPA network, the reviewers of this paper, and other scientific colleagues.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the German Federal Ministry of Education and Research [01EL1422B].
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.