
Abstract
Objective:
The purpose of this systematic literature review is to assess the factors associated with synergistic multisector alliances in the public health domain.
Data Source:
Articles in PubMed, CINAHL, Scopus, and Google Scholar between March 2009 and February 2019 were searched.
Study Inclusion and Exclusion Criteria:
Included alliances had a public health and behavioral focus, were from the public or private sector, and were multipartner and multisector, and from high-income countries. Public health research alliances were included, but clinical research alliances were excluded.
Data Extraction:
Data extraction included alliance description, alliance domain, country, single or multiple alliances, and the sectors included in the alliance. Two theoretical frameworks were used in data extraction.
Data Synthesis:
Data were coded according to 28 factors representing antecedents, management, and evaluation (Parent and Harvey model) and 3 output-specific factors (Bergen model).
Results:
A final 24 papers were included, of which 58% contained synergistic alliances. While almost all factors reportedly enabled synergy, some factors were more frequently associated with synergistic alliances, including clear purpose and positive coordination, information sharing, and evaluation of project outcomes. Complexity within some factors was also reported.
Conclusion:
The theoretical models were supported by the data. Public health alliances would likely benefit from incorporating factors identified as beneficial for synergy and from carefully considering the management of complex factors.
Keywords
Objective
The objective of this review is to provide evidence on how to create and maintain synergistic public health alliances. A synergistic alliance is greater than the sum of its parts, members achieve more together than they could do as individuals. 1 The necessity of this review was prompted by the creation of a strategic alliance to increase children’s vegetable intake. 2
An alliance is a form of partnership including two or more organizations, also commonly referred to as a coalition, network, consortium, or collaboration. 1 It is evident in available literature that alliances addressing public health are popular globally and are commonly used to connect diverse stakeholders with a mutual goal. 1,3 -9 Alliances of this nature may include members from private and public health, government, academia, advocacy, and industry. 1,3 -9
A search of recent literature identified previous reviews in the public health alliance domain (excluding commercial partnership models) and models potentially suitable for a theoretical framework. Although numerous literature reviews were identified, there were several limitations to their application, including lack of quality control, 4,9 restriction to one region, 5,10 lacking variety of stakeholders, 7 restricted focus of the alliances (eg, focused solely on physical activity), 6 and small sample size. 8,11
As none of the previous reviews suited the current objectives, a clear need for the current review was identified. Assessing the models for alliance evaluation, it was identified that many models lacked theoretical robustness due to limited evidence from application and many did not include multisector partnerships. A synthesis of the available models concluded that a hybrid of the Parent & Harvey model (see adaptation in Figure 1) 1 and the assessment of outputs from the Bergen model 3,9 was most suitable for purpose. The Parent & Harvey model was originally developed to assess alliances in the physical activity and sport domain. The apparent lack of conflict between private commercial interests (and sponsorship) and public health outcomes in the physical activity domain is analogous to the current vegetable domain. The Bergen model categorizes alliances into one of three output categories: synergistic (a greater or more productive outcome than could be achieved individually), additive (members achieve no more together than they would working individually), or antagonistic (members achieve less together than they would individually). 3
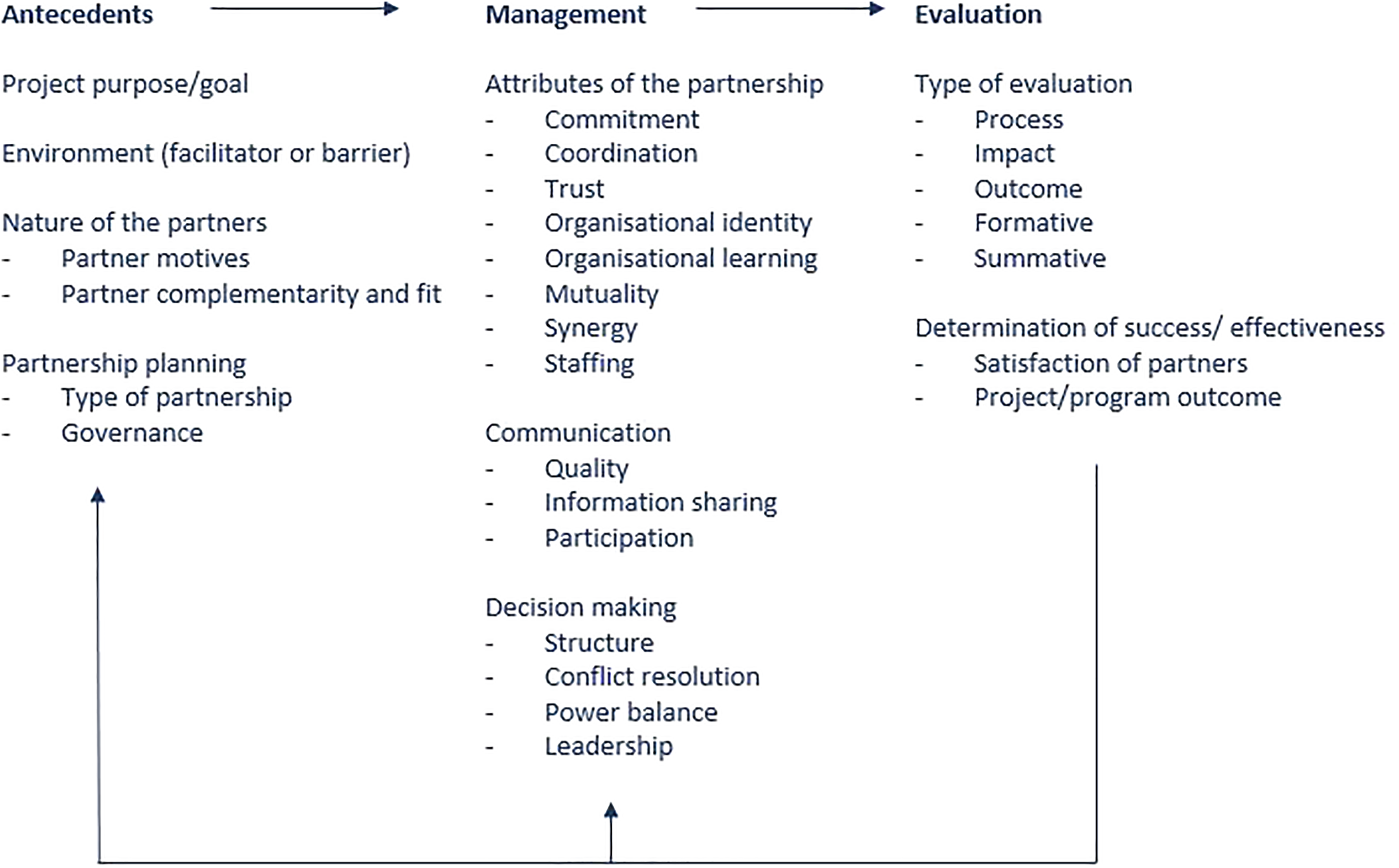
Adaptation of Parent and Harvey model for sport and physical activity community-based partnerships. 1,6 See Appendix A for definitions of each partnership attribute.
This article reviews the evidence for creating a synergistic public health alliance grounded in the Parent and Harvey, and Bergen models. The results of this review are applicable to a broad range of alliances in the public health domain.
Methods
Data Sources
The search was conducted in PubMed, CINAHL, Scopus, and Google Scholar (Google Scholar limited to first 200 results). A search of the published peer-reviewed literature was conducted between February and March 2019. Search terms were defined to retrieve academic papers describing the development, management, or evaluation of public health-focused alliances (see Table 1). Preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines were followed (see Figure 2 for PRISMA checklist).
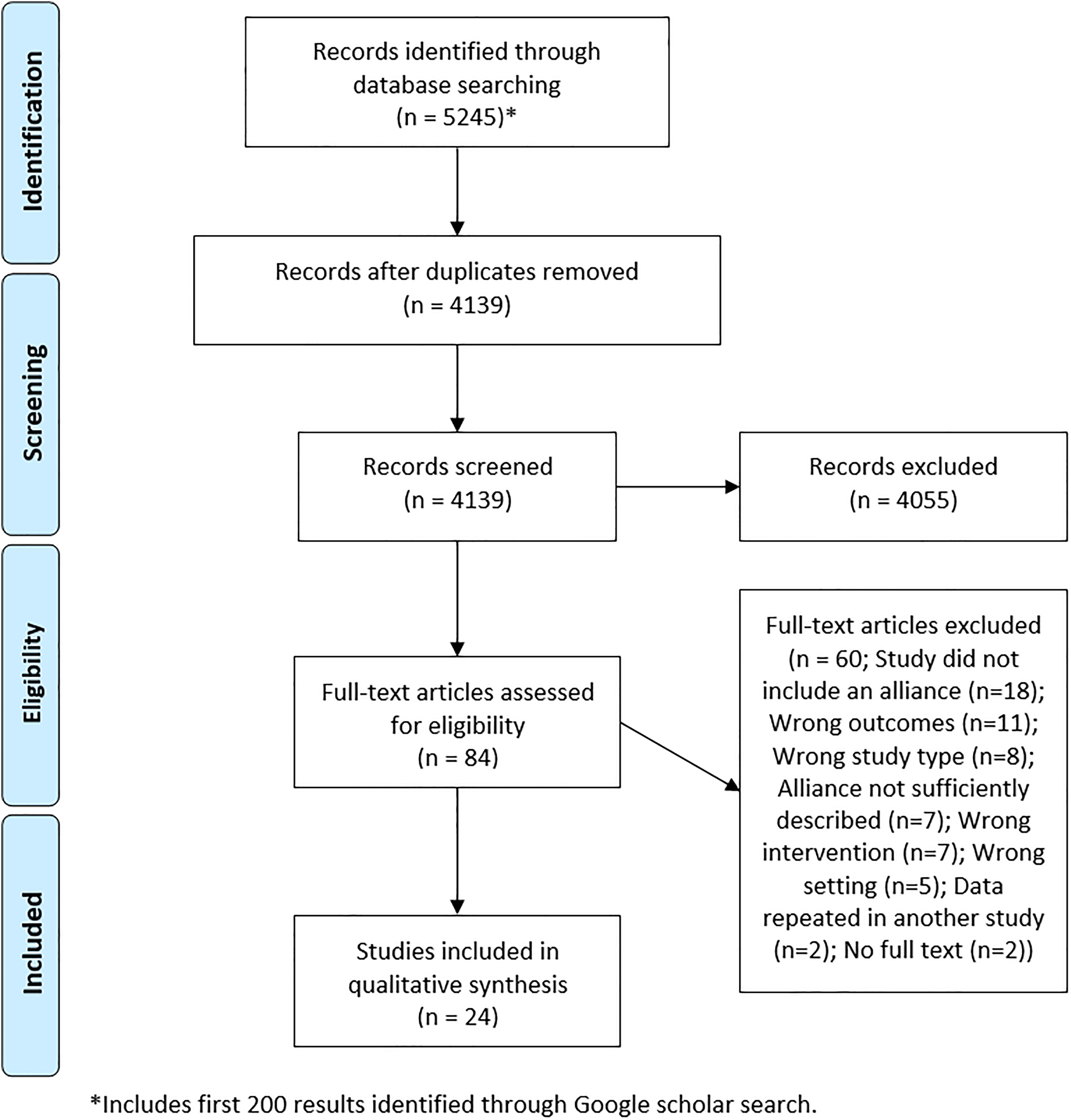
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) diagram.
Literature Review Search Terms.a
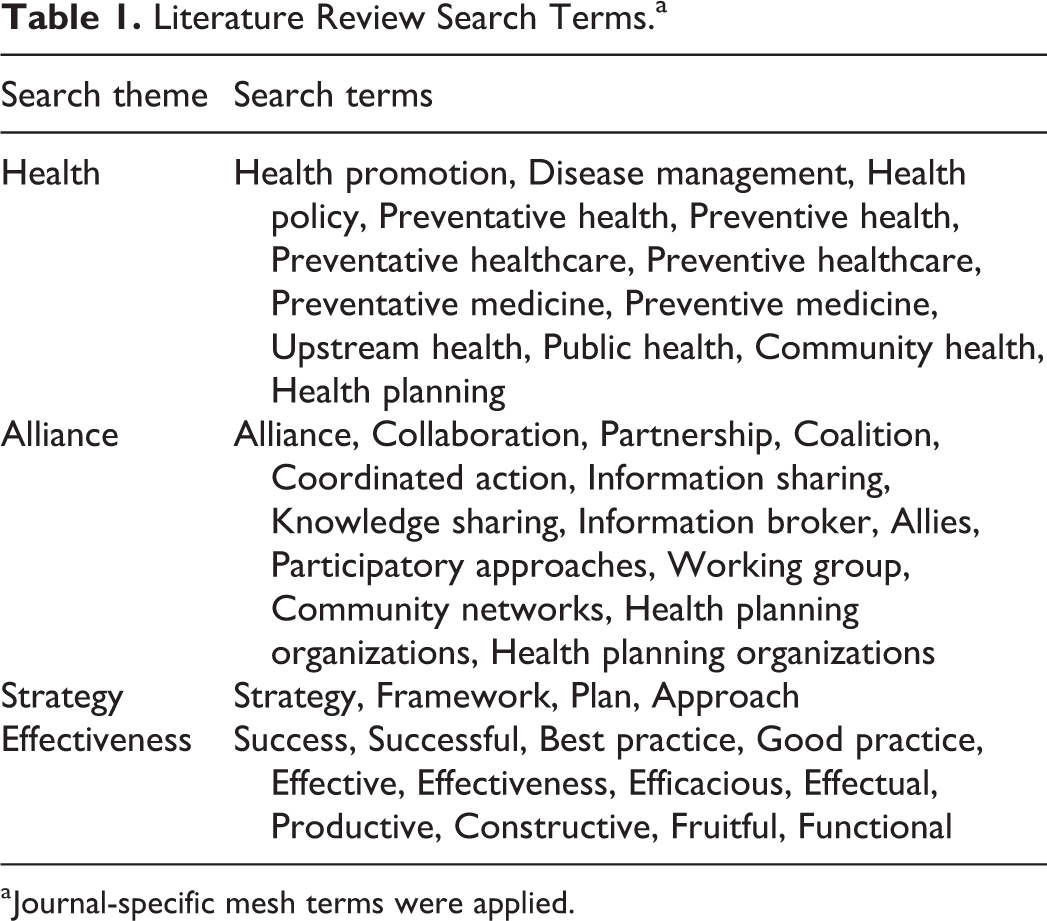
a Journal-specific mesh terms were applied.
Inclusion and Exclusion Criteria
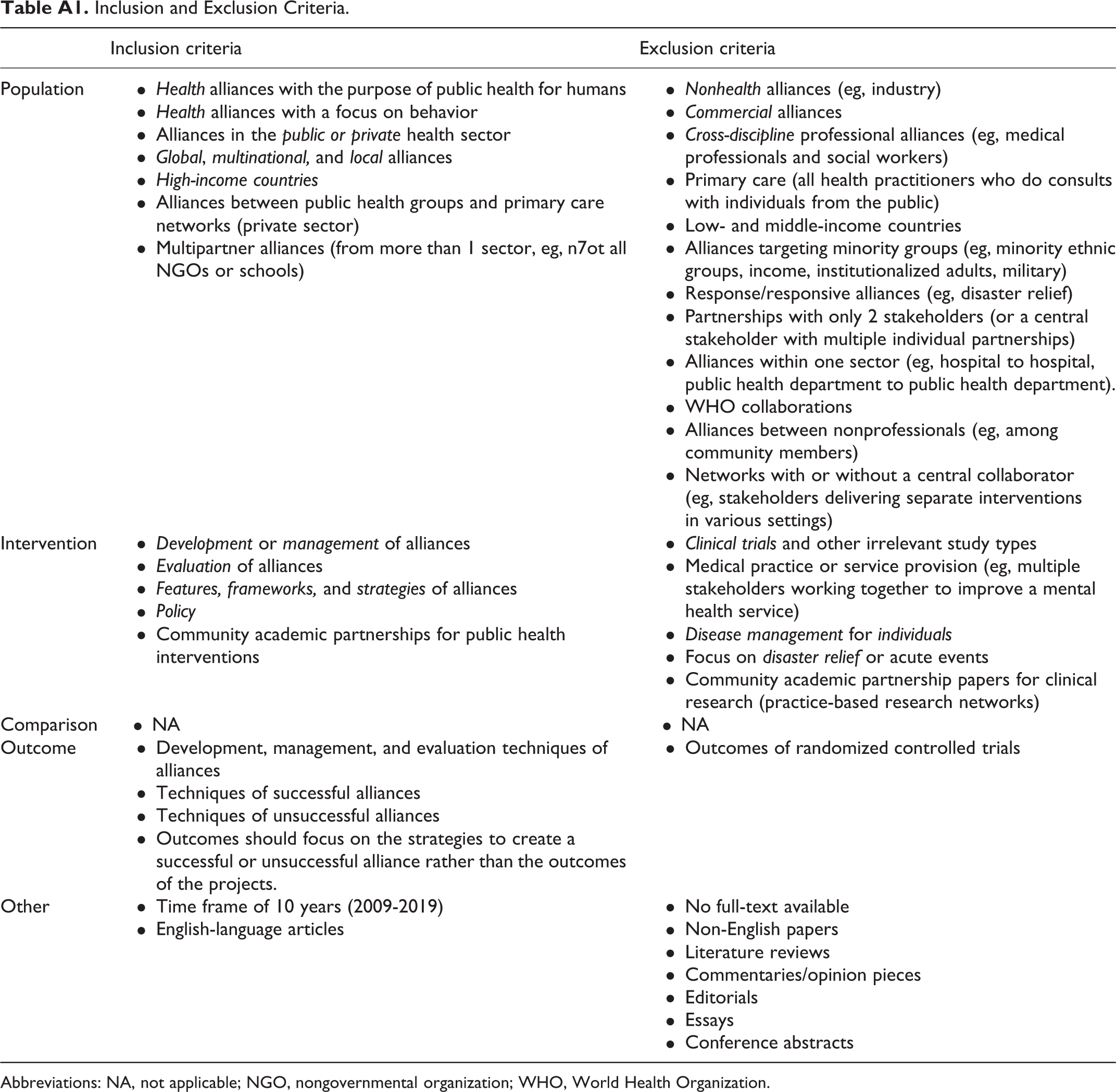
The inclusion criteria defined alliances with a public health focus and a behavioral focus, from the public or private sector and in high-income countries. Alliances had to be multipartner and multisector (i.e., minimum of 3 partners and 3 sectors). Alliances were defined as such to exclude two-way partnerships, as the focus was to determine which factors encouraged synergy in larger multistakeholder alliances. Community-Academic Partnerships for public health interventions were included, those for clinical research (i.e., practice-based research networks) were excluded (see Appendix A for full criteria).
Data Extraction
The initial search retrieved a total of 5245 papers, reduced to 4139 once duplicates were removed. The papers underwent title and abstract screening, before 84 full-text articles were assessed for eligibility and finally 24 papers were included for review (see Figure 2 for PRISMA diagram). Data were extracted by two coders who double-coded 20% of the literature to establish consistency, before adjusting the strategy to individually code and check the remaining papers.
Data Synthesis
The data were coded in line with the Parent and Harvey Partnership model, 1 and the Bergen model was used to code outputs. 3,9 The Parent and Harvey model describes alliances based on 28 factors within the categories of antecedents, management, and evaluation. Papers were coded as either positive (factor present and functioning well), negative (factor present and functioning poorly), positive and negative, neutral (factor present but functionality unclear), or not reported.
The Bergen model provides three output categories: synergistic, additive, or antagonistic. Where outputs were evident, papers were coded accordingly.
Results
Of the 24 papers, the majority were from the United States (67%), four (17%) from Canada, two (8%) from Australia, and two (8%) from Europe. The majority of the papers (79%) focused on a single alliance, two (8%) papers focused on multiple alliances with the same goal (e.g., an analysis of several alliances for increased physical activity) and three (13%) papers contained multiple alliances with the same goal and funding source (e.g., a national program which funded state-based alliances with individualized strategies).
The alliances included varied stakeholders. Alliances typically included a representative of research, community, and government, but extended to the following: private and public health organizations, academia, education, business/industry, community organizations, government and nongovernment departments, for-profit and not-for-profit organizations, and service providers such as mental health clinicians.
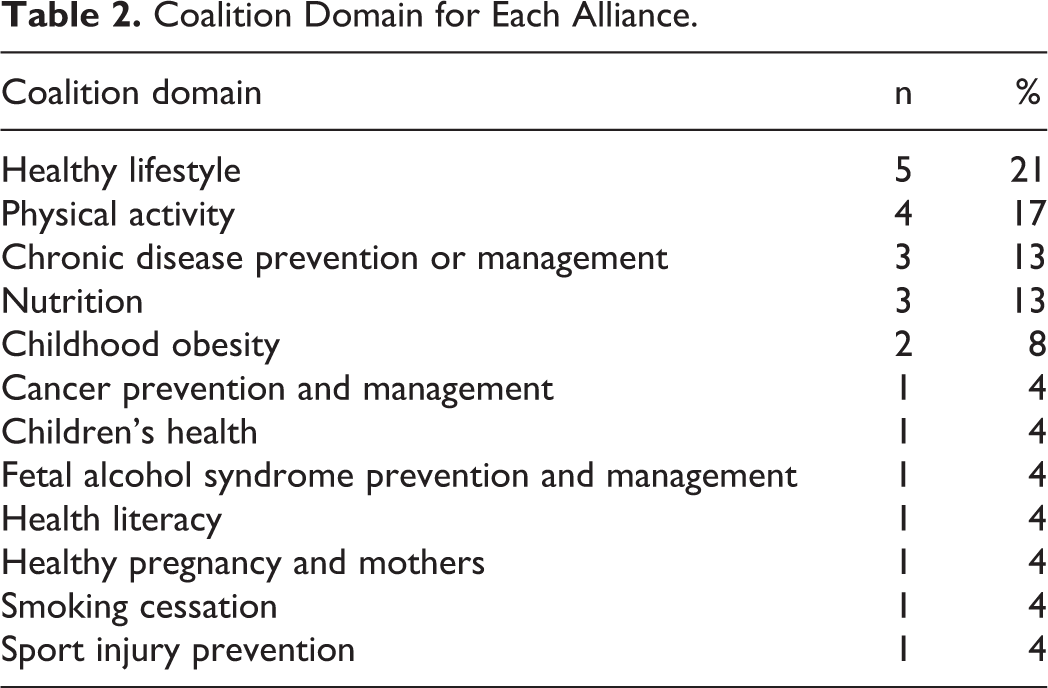
The most common alliance domains were healthy lifestyle (21%), physical activity (17%), chronic disease prevention or management (13%), nutrition (13%), childhood obesity (8%), and several singular domains (see Table 2). Successful alliances were distributed across a range of domains.
Coalition Domain for Each Alliance.
Model Attributes
Alliance outcomes reported were heterogeneous with no clear or common primary outcome, with most authors reporting some positive outcome; therefore, “outcomes” as a measure of categorizing success was not useful as a comparator. Additionally, the longevity of an alliance is dependent on both reaching alliance goals and partnership satisfaction. Only 37% of studies reported partner satisfaction, so another method was required to determine the alliance success. Therefore, the Bergen model of defining success (synergy) was used to determine which alliances were structured in a way that would lead to the highest likelihood of success.
In accordance with the Bergen model alliance outputs, fourteen (58%) papers included synergistic alliances, two (8%) were additive, none were antagonistic, and eight (33%) did not report the output in sufficient detail to be coded (see Appendix B for output definitions). There are insufficient data to make recommendations based on the two alliances with additive results, and we are unable to draw conclusions on the effectiveness of the uncategorized alliances (however, results for all papers are provided in Appendix C). The results presented below indicate which alliance attributes are common in synergistic alliances and can be used to guide the creation and management of public health alliances.
Antecedents
Project purpose
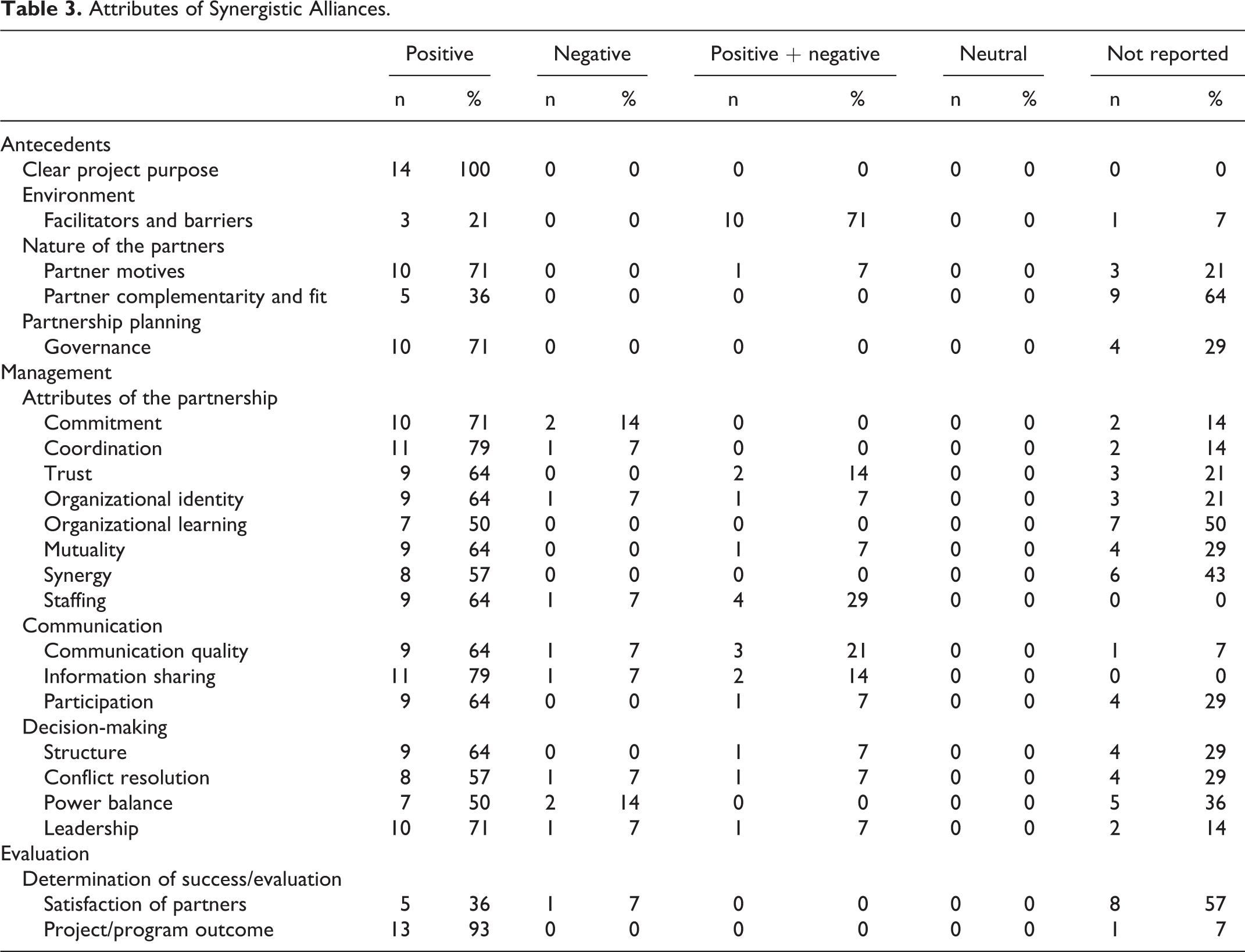
All synergistic alliances had a clear project purpose, which guided team members to work toward a common goal (Table 3). For example,
Attributes of Synergistic Alliances.
“promoting healthy lifestyles of those who live, work and visit Monroe County through community events, programs, and policies.” 12
The model identifies the value of a flexible purpose, which was evident in several alliances, for example, an alliance with smaller localized teams was given flexibility to develop community-relevant programs. 13
Some alliances created a goal prior to inviting members, while others worked as a group to define the alliance purpose. As having a clear project purpose was a consistent attribute of successful alliances, the notion of a flexible process personalized to the alliance is supported.
Environment
An analysis of the general and task (context-specific) environments was a key antecedent to an effective alliance. Ten (71%) of the synergistic alliances identified both barriers and facilitators, whereas 3 (21%) only reported facilitators. Common facilitators included receiving funding,
14
-21
alignment with political policies or goals,
15,18,21,22
and pre-established relationships between organizations or individuals in the alliance.
16,18,21
Common barriers included members travelling long distances for meetings,
13,14
limited funding or resources,
14,15,17,18,22
-26
and changes in politics/policies.
15,17
The economic environment, including alliance funding, was mentioned most frequently. The economic environment often acted as both a facilitator and barrier within one setting. Funding is evidently integral to the success of an alliance. “Good project management in maintaining this engagement and some seed corn funding also enabled people to put their ideas into practice which gave sufficient “quick wins” to keep the partnership interested.”
17
Nature of the partners
Positive partner motives were frequently reported (71%), while partner complementarity and fit were largely underreported (64%), with only five (36%) reporting positive complementarity or fit. The alliances with positive partner motives frequently reported clear actions taken to ensure aligned motives. “…partners developed partnership principles to determine how they would work together and an action plan to define the objectives, action steps to design, implement and evaluate the chosen interventions; and the outcomes of interest.”
14
Partnership planning
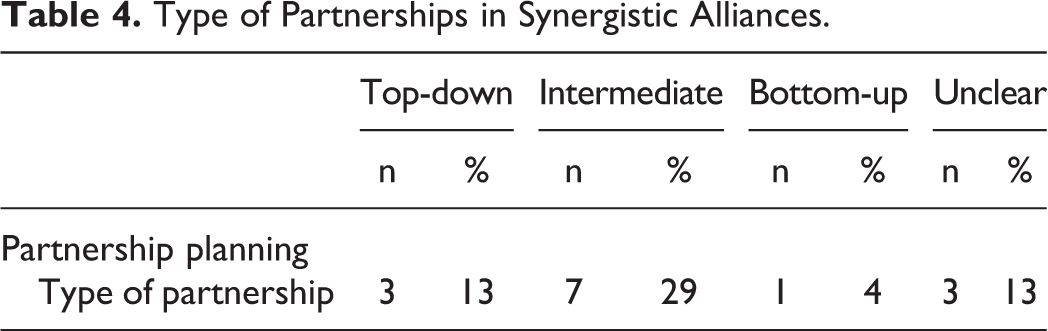
The type of partnership used by synergistic alliances varied (Table 4). Three (13%) synergistic alliances used top-down management approaches, seven (29%) used an intermediate structure, whereby members may provide input on the alliance, but there is a clear leadership structure, one (4%) alliance used a bottom-up approach, and three (13%) did not report the structure. Parent and Harvey state that the intermediate partnership is the ideal type of partnership for alliance success. 1 However, further evidence is needed to determine whether this is consistent and practical for all successful public health alliances.
Type of Partnerships in Synergistic Alliances.
Most synergistic alliances reported a positive governance structure (71%), with the remainder not reporting on governance (29%). It was common for alliances to include a governing body or steering committee. This may assist in providing clear leadership for alliances and should be considered when designing the structure of an alliance.
Management
Attributes of the partnership
The Parent and Harvey model includes eight management attributes (Table 3). Synergistic alliances tended to report positive attributes.
The majority of synergistic alliances reported that members were committed (71%). Alliance commitment was facilitated through a range of strategies, including partners signing contracts to state their role in the alliance,
13,21,23
ensuring a common motive,
15
shared leadership,
14
and enthusiastic members.
17,25
Issues around commitment centered around continuity of interest and willingness to commit: “Interest in participation by members of the research team waxed and waned depending upon the stage of the project and the compatibility of the research stage with academic and practice interests.”
18
“We recommend that other rural regional partnerships discuss how partners want to be engaged and what they value early in the partnership process.”
14
Almost one-third (29%) of synergistic papers reporting both positive and negative staffing attributes, for example, “Most also agreed that the partners had the necessary skills for collaborative action; administrative, communication, and decision-making structure of the partnership was as simple as possible; and that the relevant managers in each organization supported the partnership…. [However] Several respondents indicated confusion around why some participants—particularly those outside the direct sporting sector—were part of the partnership.”
22
Communication
Overall, communication was positively reported, with over 3-quarters of the synergistic papers reporting positive information sharing (79%), communication quality (64%), and participation (64%). Quality communication occurred during and between meetings. It was facilitated by creating time for one-on-one communication and networking, 14,19 having capacity-building activities to “break down silos,” 16 and circulating agendas before meetings. 22 Information sharing was facilitated by structured reporting processes via e-mail, text messages, events, or meetings. 14 -17,19,20,24 -26
Communication quality was commonly rated as positive and negative (21%), indicating greater complexity within this factor and the potential for it to be successful in some ways while falling short in other ways. Alliances may benefit from focusing on high-quality communication across all areas (eg, online and in-person, internally and externally facing).
Interestingly, as well as being commonly rated as positive and negative, information sharing and staffing were the only two attributes that were 100% reported, further highlighting that alliances consider these as particularly important. It is possible that other factors have similar complexities but were underrepresented in the results because their ambiguity prevented them being coded as positive and negative.
Decision-making
Most synergistic papers reported positive decision-making regarding structure (64%), conflict resolution (57%), power balance (50%), and leadership (71%). Some papers reported setting up structures or agreements to support positive power balance. “Key elements described in the participation agreement included partner representation in decision-making, meetings, administration of the grant, project funding, communication, a noncompete clause, conflict resolution, participation in projects, relevant industry guidelines, and project duration.”
23
Evaluation
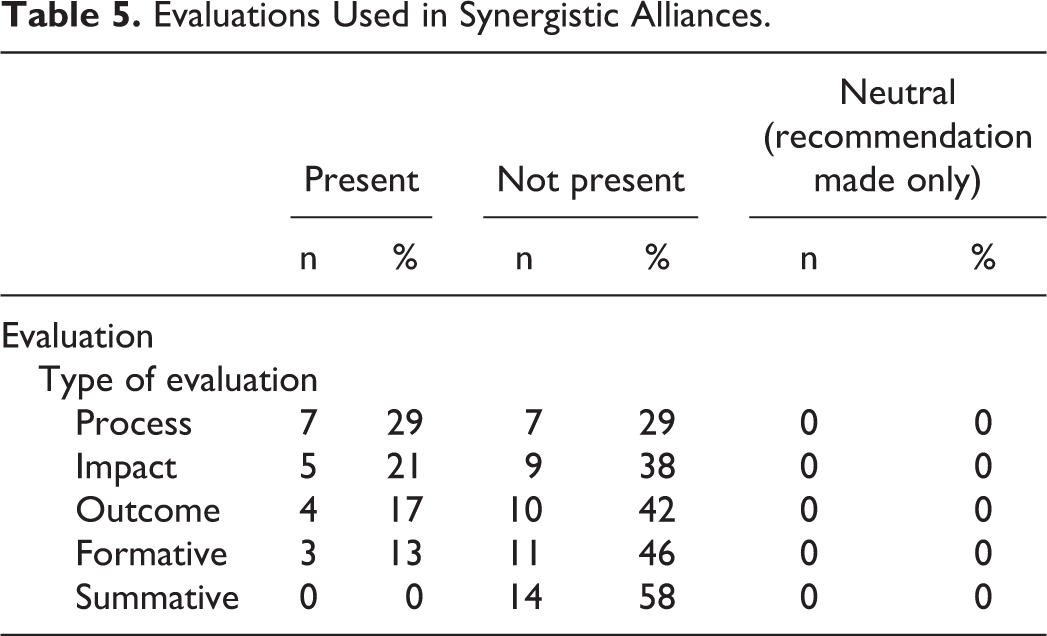
The Parent and Harvey model includes five methods of evaluation (Table 5). The most commonly used was process evaluation (29%), followed by impact (21%), outcome (17%), and formative evaluation (13%; see Table A1). None of the papers included a summative evaluation. While some of the papers classified as “additive” and “unclear” did not report on evaluation, all the synergistic papers reported some form of evaluation. Evaluations can provide critical feedback about the processes and satisfaction of partners in the alliance, as well as provide evidence for continued funding. “[The alliance] undertook a formative evaluation of the partnership by an external resource providing an invaluable midcourse adjustment of the overall project.”
23
Evaluations Used in Synergistic Alliances.
Another indicator of evaluation within the Parent and Harvey model is the determination of success or effectiveness. Satisfaction of partners was not highly reported (57% not-reported), and only 36% of synergistic papers reported that partners were satisfied.
Promisingly, 93% of synergistic alliances reported that they achieved their project outcome, with 1 (7%) paper not reporting the project outcome success. This suggests a high correlation between synergistic alliances and successful outcomes of alliances, highlighting the importance of creating a working environment that supports synergy.
Limitations
Study design
The alliances in this sample had diverse goals, structures, environments (geographically or politically), and evaluation techniques, which made data analysis challenging. It was not always clear whether long-term alliance goals were met, which limited the ability to conclude that alignment with the factors in the model leads to successful alliance outcomes. Therefore, this article highlights the key features required to make an alliance synergistic; however, there may be additional elements required to make the outcomes of the alliance successful. This means that the factors discussed are necessary but may not be sufficient for success.
Further to this, the papers used a variety of models to assess alliance effectiveness (eg, CBPR, RE-AIM, and DISC), meaning that some key concepts did not have an equivalent attribute in the Parent and Harvey model, despite their relevance.
There was also variation in study quality. Most papers clearly defined a data collection process that included surveys or focus group interviews, appropriately sampling a wide variety of alliance members. However, some papers failed to adequately describe their methodology; therefore, it was unclear whether member feedback was collected. Other alliances only surveyed the governing body, which may have led to positively biased results if the data were collected from a limited sample of highly engaged members.
Reporting bias is likely, as papers may have focused on successful alliance attributes, rather than attributes that were lacking or perceived as barriers. Publication bias is also possible, as successful alliances may have been more likely to be published, or to seek publication. In turn, this may have limited insights on antagonistic or additive alliances. Although this review provides an overview of the factors contributing to successful synergistic alliances, future reviews would benefit from analysis of negative attributes and barriers faced in unsuccessful alliances.
Model
Although the included alliances mapped well to the Parent and Harvey partnership model, there were several areas of partnership functioning that were not well represented. The model did not capture sustainability and forward planning, which featured in several alliances as a facilitator to success. 18 As such, an alliance may feature many of the factors outlined in the model but still lack the aptitude for success, or in this context, long-lasting behavioral changes.
Relationship building and efforts to foster a sense of community, belonging, or connection was also a theme across several alliances, 27 and although the elements of relationship building fit within the attributes leadership or trust, it was not represented by a clear factor. Introduction of relationship building as a factor could also extend to social skills development, social networking, and team building. 10
There was also a substantial emphasis on funding and access to resources in most of the included literature. Although the model captures this under facilitators and barriers, a separate and defined factor would emphasize the imperative role of funding.
As with other structural models, the authors are required to judge the level of intuition or definitiveness used in identifying factors to code. There are several factors within the Parent and Harvey model that may have been undercoded as it was not explicit in the text. For example, partner complimentary and fit was coded six times (25%); however, many papers included stakeholders from a wide range of settings and it is likely the stakeholders were sought in effort to draw different skills, knowledge, roles, and power to the alliance. The model would benefit from defining the factors to pick up on such nuances, for example, membership from at least three sectors (such as medical, government, and industry) being indicative of partner complimentary and fit. Another example is organizational learning. Some papers had clear progression, evolution, adaption to circumstances, and change over time, but it was not always explicitly acknowledged as organizational learning.
Finally, this article was limited to models for alliance evaluation and did not investigate other factors that are also likely to be important in creating successful alliances, such as stakeholder mapping, 28 and understanding the culture in which stakeholders operate. 29
Conclusions
The results indicate that synergistic alliances tended to have one or more of the following attributes: clear project purpose, effective coordination and information sharing, aligning partner motives, clear governance structures, committed partners, and effective leadership for making decisions. Although we cannot assume cause and effect, we recommend that these factors are prioritized when creating an alliance.
Reports on future alliances should consider alliance outputs, partner complementarity and fit, organizational learning, conflict resolution, and satisfaction of partners as they were underreported in the studies identified in this review. Reporting comprehensive evaluations on the alliance projects was also limited.
The objective of this review was to provide evidence on how to create and maintain successful public health alliances. The application of the Parent and Harvey model to 24 papers documenting public health alliances across a range of domains found evidence that all attributes in the model are likely to be critical. The heavy emphasis on funding and access to resources in most of the literature indicates that considering funding as a separate and individual factor would be valuable in an analysis.
The Parent and Harvey model did not capture all factors influencing the success of the alliances. Those omitted were sustainability and forward planning, relationship building, and efforts to foster a sense of community, belonging, or connection. Although captured partially in the model (leadership and trust), relationship building as a separate factor should be considered with possible extension to social skill development, social networking, and team building. 10 Thus, it is possible for alliances to feature many factors from within the model and simultaneously be lacking in other factors, which lead to lasting influence on success. Future studies should continue to expand on the Parent and Harvey model to ensure that it is a comprehensive model for capturing and describing successful alliances.
So What? (Implications for Health Promotion Practitioners and Researchers)
What is already known on this topic?
Previous systematic literature reviews partially assessed the success factors of public health alliances; however, they were limited due to lack of generalizability to health alliances in different countries and domains. The Parent and Harvey model 1 has demonstrated validity in analyzing physical activity and sport alliance success but had not been applied to other public health areas. 6
What does this article add?
This review found that the Parent and Harvey model could be successfully applied to a broad range of public health alliances, outside the sports domain. Furthermore, this review used the Bergen model to define alliances as synergistic, antagonistic, or additive 3,9 and thus provided a unique examination of the Parent and Harvey model in the context of alliance outputs.
What are the implications for health promotion practice or research?
The results demonstrate that almost all factors in the Parent and Harvey model play a key role in creating and sustaining a synergistic alliance. The findings further demonstrated that several factors, including clear project purpose, effective coordination and information sharing, aligning partner motives, clear governance structures, committed partners, and effective leadership for making decisions are most prominent in synergistic alliances. Alliances for health promotion can benefit from selectively prioritizing certain elements key to a success synergistic alliance.
Footnotes
Appendix A
Inclusion and Exclusion Criteria.
| Inclusion criteria | Exclusion criteria | |
|---|---|---|
| Population |
Health alliances with the purpose of public health for humans Health alliances with a focus on behavior Alliances in the public or private health sector Global, multinational, and local alliances High-income countries Alliances between public health groups and primary care networks (private sector) Multipartner alliances (from more than 1 sector, eg, n7ot all NGOs or schools) |
Nonhealth alliances (eg, industry) Commercial alliances Cross-discipline professional alliances (eg, medical professionals and social workers) Primary care (all health practitioners who do consults with individuals from the public) Low- and middle-income countries Alliances targeting minority groups (eg, minority ethnic groups, income, institutionalized adults, military) Response/responsive alliances (eg, disaster relief) Partnerships with only 2 stakeholders (or a central stakeholder with multiple individual partnerships) Alliances within one sector (eg, hospital to hospital, public health department to public health department). WHO collaborations Alliances between nonprofessionals (eg, among community members) Networks with or without a central collaborator (eg, stakeholders delivering separate interventions in various settings) |
| Intervention |
Development or management of alliances Evaluation of alliances Features, frameworks, and strategies of alliances Policy Community academic partnerships for public health interventions |
Clinical trials and other irrelevant study types Medical practice or service provision (eg, multiple stakeholders working together to improve a mental health service) Disease management for individuals Focus on disaster relief or acute events Community academic partnership papers for clinical research (practice-based research networks) |
| Comparison | • NA | • NA |
| Outcome |
Development, management, and evaluation techniques of alliances Techniques of successful alliances Techniques of unsuccessful alliances Outcomes should focus on the strategies to create a successful or unsuccessful alliance rather than the outcomes of the projects. |
Outcomes of randomized controlled trials |
| Other |
Time frame of 10 years (2009-2019) English-language articles |
No full-text available Non-English papers Literature reviews Commentaries/opinion pieces Editorials Essays Conference abstracts |
Abbreviations: NA, not applicable; NGO, nongovernmental organization; WHO, World Health Organization.
Appendix B
Attribute Definitions as Defined by the Coders, Using the Original Descriptions From the Models.
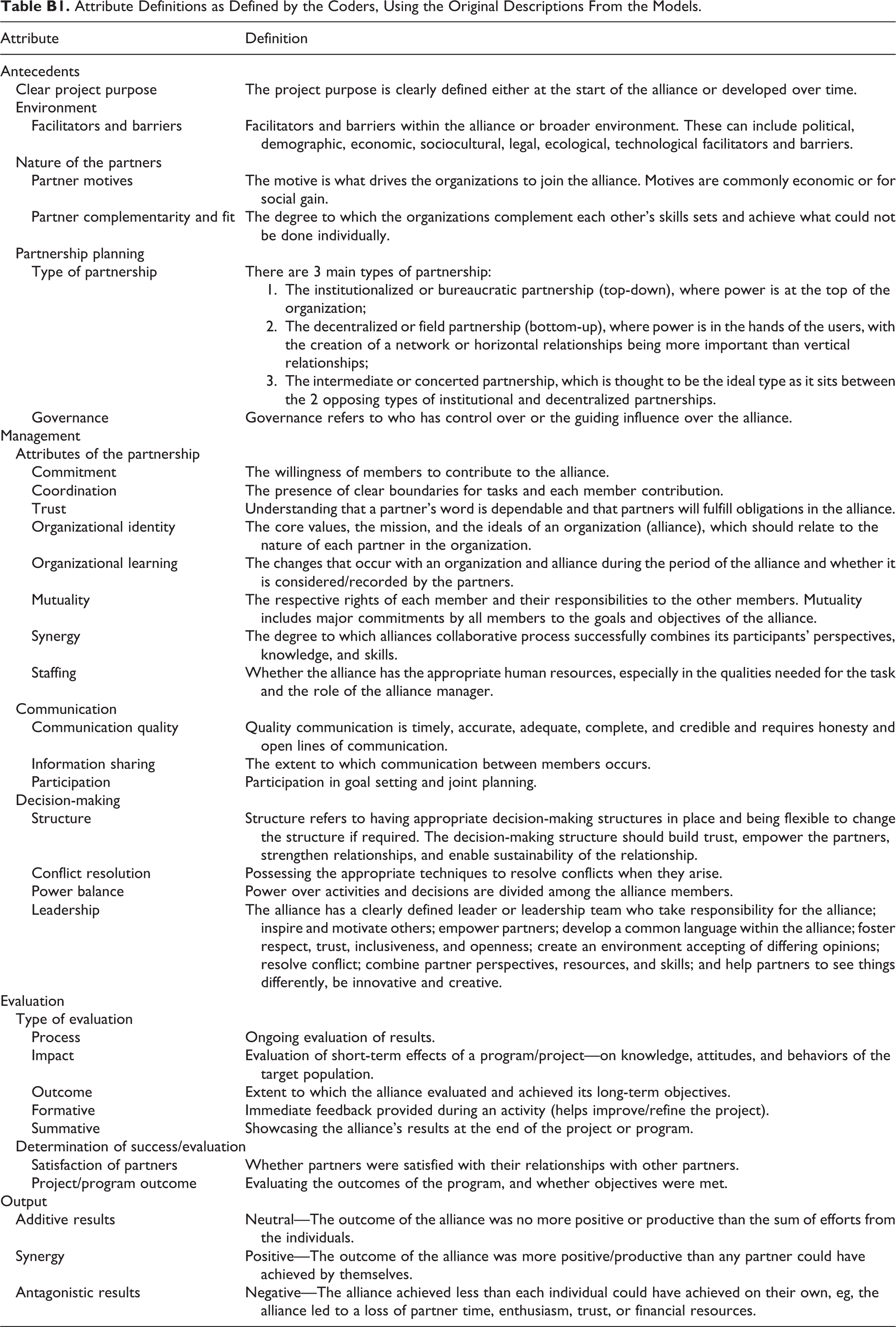
| Attribute | Definition |
|---|---|
| Antecedents | |
| Clear project purpose | The project purpose is clearly defined either at the start of the alliance or developed over time. |
| Environment | |
| Facilitators and barriers | Facilitators and barriers within the alliance or broader environment. These can include political, demographic, economic, sociocultural, legal, ecological, technological facilitators and barriers. |
| Nature of the partners | |
| Partner motives | The motive is what drives the organizations to join the alliance. Motives are commonly economic or for social gain. |
| Partner complementarity and fit | The degree to which the organizations complement each other’s skills sets and achieve what could not be done individually. |
| Partnership planning | |
| Type of partnership | There are 3 main types of partnership: The institutionalized or bureaucratic partnership (top-down), where power is at the top of the organization; The decentralized or field partnership (bottom-up), where power is in the hands of the users, with the creation of a network or horizontal relationships being more important than vertical relationships; The intermediate or concerted partnership, which is thought to be the ideal type as it sits between the 2 opposing types of institutional and decentralized partnerships. |
| Governance | Governance refers to who has control over or the guiding influence over the alliance. |
| Management | |
| Attributes of the partnership | |
| Commitment | The willingness of members to contribute to the alliance. |
| Coordination | The presence of clear boundaries for tasks and each member contribution. |
| Trust | Understanding that a partner’s word is dependable and that partners will fulfill obligations in the alliance. |
| Organizational identity | The core values, the mission, and the ideals of an organization (alliance), which should relate to the nature of each partner in the organization. |
| Organizational learning | The changes that occur with an organization and alliance during the period of the alliance and whether it is considered/recorded by the partners. |
| Mutuality | The respective rights of each member and their responsibilities to the other members. Mutuality includes major commitments by all members to the goals and objectives of the alliance. |
| Synergy | The degree to which alliances collaborative process successfully combines its participants’ perspectives, knowledge, and skills. |
| Staffing | Whether the alliance has the appropriate human resources, especially in the qualities needed for the task and the role of the alliance manager. |
| Communication | |
| Communication quality | Quality communication is timely, accurate, adequate, complete, and credible and requires honesty and open lines of communication. |
| Information sharing | The extent to which communication between members occurs. |
| Participation | Participation in goal setting and joint planning. |
| Decision-making | |
| Structure | Structure refers to having appropriate decision-making structures in place and being flexible to change the structure if required. The decision-making structure should build trust, empower the partners, strengthen relationships, and enable sustainability of the relationship. |
| Conflict resolution | Possessing the appropriate techniques to resolve conflicts when they arise. |
| Power balance | Power over activities and decisions are divided among the alliance members. |
| Leadership | The alliance has a clearly defined leader or leadership team who take responsibility for the alliance; inspire and motivate others; empower partners; develop a common language within the alliance; foster respect, trust, inclusiveness, and openness; create an environment accepting of differing opinions; resolve conflict; combine partner perspectives, resources, and skills; and help partners to see things differently, be innovative and creative. |
| Evaluation | |
| Type of evaluation | |
| Process | Ongoing evaluation of results. |
| Impact | Evaluation of short-term effects of a program/project—on knowledge, attitudes, and behaviors of the target population. |
| Outcome | Extent to which the alliance evaluated and achieved its long-term objectives. |
| Formative | Immediate feedback provided during an activity (helps improve/refine the project). |
| Summative | Showcasing the alliance’s results at the end of the project or program. |
| Determination of success/evaluation | |
| Satisfaction of partners | Whether partners were satisfied with their relationships with other partners. |
| Project/program outcome | Evaluating the outcomes of the program, and whether objectives were met. |
| Output | |
| Additive results | Neutral—The outcome of the alliance was no more positive or productive than the sum of efforts from the individuals. |
| Synergy | Positive—The outcome of the alliance was more positive/productive than any partner could have achieved by themselves. |
| Antagonistic results | Negative—The alliance achieved less than each individual could have achieved on their own, eg, the alliance led to a loss of partner time, enthusiasm, trust, or financial resources. |
Appendix C
Authors’ Note
All authors (B.W., K.A., and D.N.C.) made a substantial contribution to the concept or design of the work; acquisition, analysis, or interpretation of data; drafted the article or revised it critically for important intellectual content; and approved the version to be published. Each author has participated sufficiently in the work to take public responsibility for appropriate portions of the content. Bonnie Wiggins was the lead author and contributed to the design of the study, review of the literature, data extraction, synthesis of findings, and prepared, reviewed, and edited the manuscript. Kim Anastasiou contributed to the design of the study, review of the literature, data extraction, synthesis of findings, and prepared, reviewed, and edited the manuscript. David N. Cox conceived the idea to undertake the study, contributed to the design of the study, reviewed and chose the theoretical framework, and reviewed and edited the manuscript.
Acknowledgments
The authors thank the contribution of the Vegetable Intake Strategic Alliance (VISA) members, who provided feedback during the review process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project has been funded by Hort Innovation, using the vegetable research and development levy and contributions from the Australian Government. Hort Innovation is the grower-owned, not-for-profit research and development corporation for Australian horticulture.