
Abstract
Purpose:
To evaluate the effects of preconception care (PCC) consultations by change in lifestyle behaviors.
Setting and Intervention:
Women in deprived neighborhoods of 14 Dutch municipalities were encouraged to visit a general practitioner or midwife for PCC.
Sample:
The study included women aged 18 to 41 years who had a PCC consultation.
Design:
In this community-based prospective cohort study, we assessed initiation of folic acid supplementation, cessation of smoking, alcohol consumption, and illicit drug use.
Measures:
Self-reported and biomarker data on behavioral changes were obtained at baseline and 3 months later.
Analysis:
The changes in prevalence were assessed with the McNemar test.
Results:
Of the 259 included participants, paired analyses were available in 177 participants for self-reported outcomes and in 82 for biomarker outcomes. Baseline self-reported prevalence of no folic acid use was 36%, smoking 12%, weekly alcohol use 22%, and binge drinking 17%. Significant changes in prevalence toward better lifestyle during follow-up were seen for folic acid use (both self-reported, P < .001; and biomarker-confirmed, P = .008) and for self-reported binge drinking (P = .007).
Conclusion:
Our study suggests that PCC contributes to initiation of folic acid supplementation and cessation of binge drinking in women who intend to become pregnant. Although based on a small sample, the study adds to the limited body of evidence regarding the benefits of PCC in improving periconception health.
Purpose
Preconception care (PCC) aims to prevent biomedical, behavioral, and social risks from adversely affecting pregnancy by reducing these risks before conception. 1 For instance, lifestyle behaviors such as smoking and alcohol consumption as well as inadequate folic acid intake are associated with suboptimal embryonic development. 2 -4 Unfortunately, such behavior is widely prevalent among women in the preconception and early pregnancy periods. 5 -8 Prevalence of inadequate folic acid is around 39%, smoking 23%, and alcohol use 46%, based on a National Online Self-Reported Risk Assessment. 6
Preconception behavior interventions have focused on folic acid, smoking, and alcohol before with varying effectiveness, but little is known about actual behavior changes after a comprehensive PCC intervention in a general population of women planning pregnancy. 9 -12
In 2011, the Healthy Pregnancy 4 All program was launched to improve perinatal health and reduce related inequalities in the Netherlands. 13 Women were encouraged to visit a general practitioner (GP) or midwife for PCC. 14,15 The main objective of this study is to evaluate the effects of the program’s PCC consultations on lifestyle behaviors.
Methods
Design
A prospective cohort was designed to study the effect of the PCC consultations. 14 The PCC consultations were planned as 2 individual visits with an interval of 3 months. During the first visit, risk assessment was performed using a web-based questionnaire (including the domains lifestyle, medical, reproductive, and family history) and advice was provided according to the national guideline. 6,16 During the second visit, the identified risk factors and formulated plan were evaluated.
The primary outcome of the study was lifestyle behavior change assessed as 4 independent outcomes: initiation of folic acid supplementation, smoking cessation, reduction or cessation of alcohol consumption, and cessation of illicit drug use. In addition, subgroup differences were explored.
The study was conducted in 14 municipalities selected based on their relatively high perinatal morbidity and mortality rates. 13 A local outreach strategy for PCC was rolled out to promote uptake. This strategy consisted of invitation letters sent by municipal health services and GPs (including translations in 8 languages), as well as referral by youth health care professionals and health educators. 15 Preconception care was offered at participating GPs and midwifery practices. The GPs and midwives received a training as well as self-study material and protocols. 14
Sample
Women aged 18 to 41 years who made an appointment for a PCC consultation between February 2013 and December 2014 were eligible to participate in the study. In total, 587 PCC appointments were registered and 259 (44%) participants were included in the study after written informed consent. 15 Participant enrolment is described in detail elsewhere. 15
Measures
We collected baseline and follow-up measurements from questionnaires and blood samples. We dichotomized the outcomes and used the following definitions of preconception risk factors: No folic acid supplementation: self-reported “no” to folic acid use, <20 nmol/L serum folate, and <590 nmol/L erythrocyte folate.
17,18
Smoking: self-reported “current smoking” and cotinine levels of >25 µg/L (reference value used by the laboratory).
19
Alcohol consumption: self-reported drinking of “1 unit (glass) or more per week” and self-reported binge drinking of “>6 units per day in past 3 months,” carbohydrate-deficient transferrin (CDT) above the laboratory reference value of ≥2.2%, and one of the homologues of PEth above the lower limit of quantification of the laboratory, which was >6 µg/L for POPEth and PLPEth, and >3 µg/L for DOPEth.
20
Illicit substance use: self-reported “current use” or “use within the previous week.”
15
Analysis
We used descriptive statistics to show baseline characteristics of the participants. Within the total sample of women with follow-up data, we first tested whether there was ≥20% increase in self-reported folic acid intake and ≥5% decrease in self-reported smoking using the exact binomial test with a 1-sided significance level of .025, as specified in the published protocol. 14 An estimated sample size of 839 was calculated for the outcome folic acid intake and 687 for smoking cessation. In addition, all outcomes were analyzed paired for change between their prevalence at baseline and follow-up with the McNemar test.
Subgroup data are provided (Supplementary table) on the self-reported outcomes. Subgroups were based on baseline patient characteristics, self-reported pregnancy since PCC, and women who filled in the baseline questionnaire before the PCC consultation or later.
We used SPSS software for Windows, version 21, and statistical significance was accepted at .05 unless stated otherwise.
Results
Of the 259 participants, we collected 237 (92%) questionnaires and 186 (72%) blood samples at baseline. Follow-up data consisted of 177 (75%) questionnaires and 82 (44%) blood samples. The baseline characteristics of the 177 participants with both questionnaires demonstrate that the median age was 30 years; 68.8% reported Dutch ethnical background; educational attainment was 7.5% low, 33.9% intermediate, and 55.7% high (International Standard Classification of Education); 76.9% indicated a pregnancy intention within 6 months; 27.7% had been pregnant before; and 7.4% reported current or previous fertility treatment. Comparing complete cases with incomplete cases shows only more lost to follow-up among non-Dutch participants (46.6% Dutch vs the earlier mentioned 68.8%; Supplementary table). Considering the risk factors no folic acid supplementation, smoking, and alcohol consumption, 15.8% had no risk factor, 55.6% had 1 risk factors, 25.7% had 2 risk factors, and 2.9% had 3 risk factors.
Table 1 shows the primary outcomes. A significant increase in self-reported and biomarker (serum folate) established folic acid use was observed in the follow-up data, when compared to baseline use. In addition, 42.1% (24/57) of women who reported not taking folic acid at baseline had started taking folic acid at the follow-up measurement (binomial test ≤20%, P < .001). The percentages of smoking showed no change between baseline and follow-up, nor with the binomial test ≤ 5% (P = .736). Prevalence of reported binge drinking decreased significantly. Only a few participants reported illicit substance use at baseline and this showed no significant decrease at follow-up.
Prevalence of Preconception Risk Factors at Baseline (T1) and Follow-Up (T2).
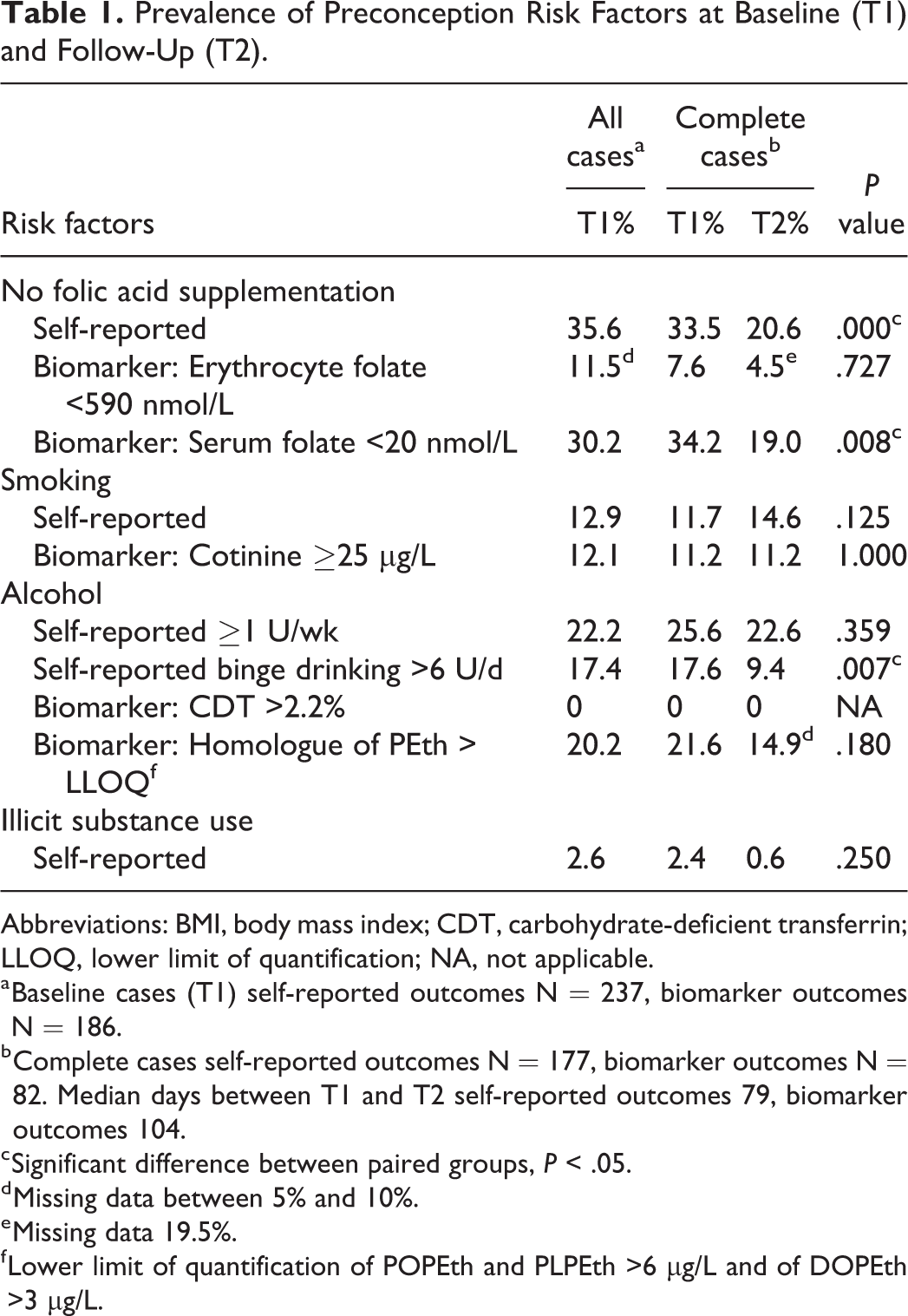
Abbreviations: BMI, body mass index; CDT, carbohydrate-deficient transferrin; LLOQ, lower limit of quantification; NA, not applicable.
a Baseline cases (T1) self-reported outcomes N = 237, biomarker outcomes N = 186.
b Complete cases self-reported outcomes N = 177, biomarker outcomes N = 82. Median days between T1 and T2 self-reported outcomes 79, biomarker outcomes 104.
c Significant difference between paired groups, P < .05.
d Missing data between 5% and 10%.
e Missing data 19.5%.
f Lower limit of quantification of POPEth and PLPEth >6 µg/L and of DOPEth >3 µg/L.
Exploratory analyses indicated that the prevalence of not using folic acid supplementation, smoking, and alcohol consumption varied across subgroups (Table 2). Possible associations with subgroups were inconsistent for the 3 risk factors analyzed.
Subgroup Analyses of Complete Cases for Self-Reported Data on No Folic Acid Supplementation, Smoking, and Alcohol Use.
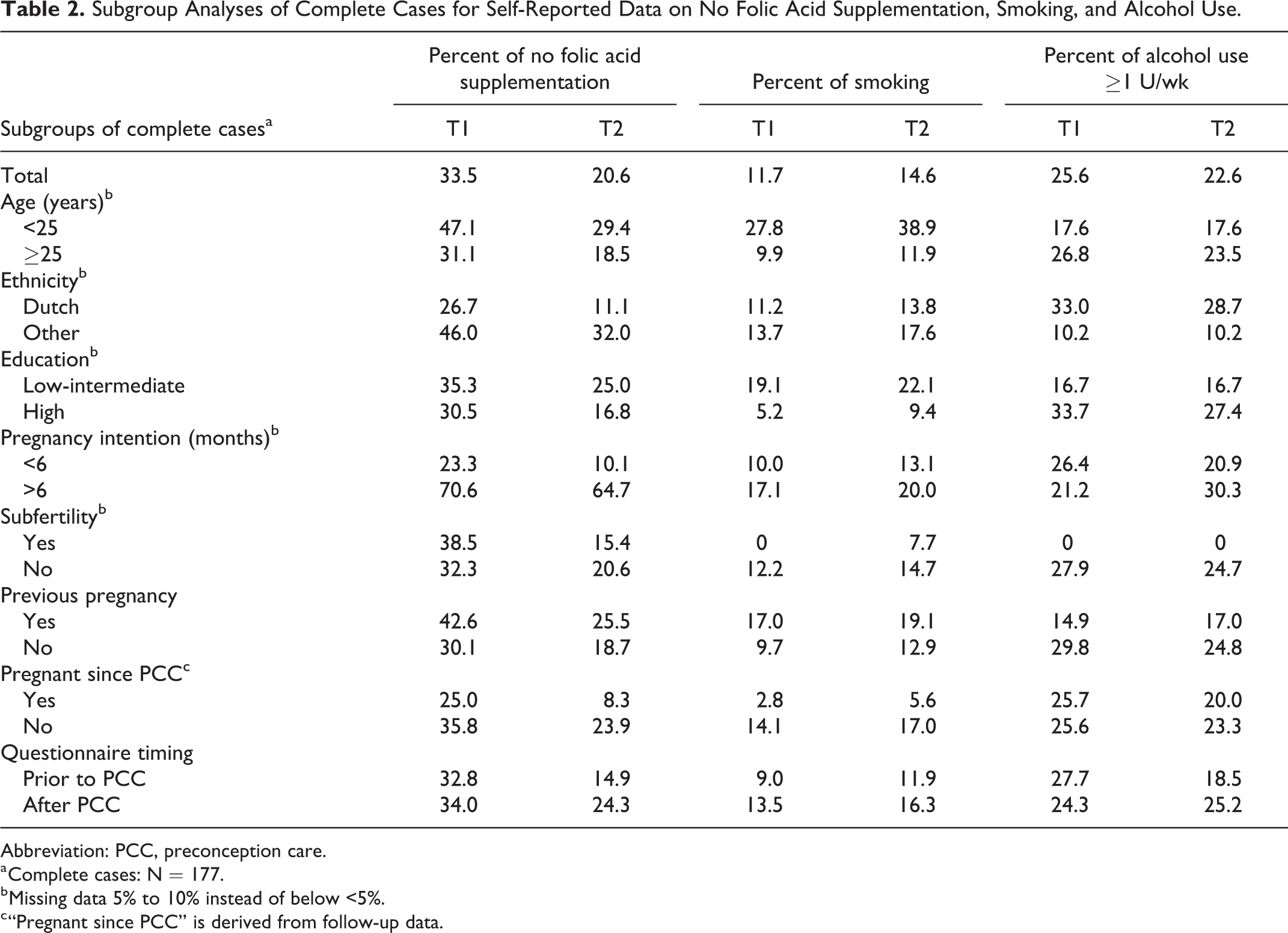
Abbreviation: PCC, preconception care.
a Complete cases: N = 177.
b Missing data 5% to 10% instead of below <5%.
c “Pregnant since PCC” is derived from follow-up data.
Discussion
Summary
This study has demonstrated that both self-reported and biomarker-confirmed folic acid supplementation increased at follow-up after PCC. Furthermore, self-reported binge drinking decreased. Our outcomes are largely in accordance with the few other studies involving multifactorial preconception health promotion interventions in a general population of women planning to become pregnant. Previous studies often showed a positive effect on initiation of folic acid and reducing alcohol consumption, but less effect on cessation of smoking. 17,21 -24 Changing an addiction such as smoking will require more effort than a single consultation.
The biomarker data mostly confirmed our results based on self-reported data. Nevertheless, using higher erythrocyte folate cutoff levels (900-1000 nmol/L) would probably have been more appropriate and given the same results as the other 2 folic acid outcomes. 25 There were no positive CDT levels, indicating no severe alcohol consumption. PEth is known to be better in retrospective monitoring (2-4 weeks) of moderate alcohol consumption. 20 PEth results suggest a reduction in positive cases in the period after PCC in line with less self-reported binge drinking.
Targeting high-risk neighborhoods, it was expected that the recruited study population would have higher baseline prevalences of behavioral risks. However, the prevalences we found were lower or similar to other cohorts. This might be explained by the fact that most women were actively preparing for pregnancy. 6 -8 It could also be that we did not sufficiently reach high-risk women, since even though we did reach a diverse population, the majority had a Dutch and high educational background. 15 Our exploratory findings on subgroup differences are also reported by other studies; characteristics such as younger age, ethnic minority background, lower educational attainment, and a previous pregnancy seem to be associated with no use of folic acid supplementation and with smoking. 6 -9,18,26,27
Strengths and Limitations
Strengths of the study are the real-time community-based approach and the assessment of biomarkers. Limitations include the smaller sample size than intended, 15 loss to follow-up, and the possibility of a Hawthorne effect, in which participation in a study stimulates positive outcomes. 28 In addition, variation in timing of questionnaire responses, potential differences in how the PCC consultations were delivered, and variation in pregnancy intentions provide challenges in assessing the actual effect of PCC.
Significance
Our study is one the few studies looking at actual preconception lifestyle behavioral change. The results suggest that a comprehensive PCC intervention has beneficial effects on initiation of folic acid supplementation and cessation of binge drinking in women who intend to become pregnant. Altogether, the need and potential for PCC have been illustrated, but challenges remain with regard to targeting high-risk women and attaining more improvement of health behaviors.
So What? (Implications for Health Promotion Practitioners and Researchers)
What is already known on this topic?
Lifestyle behaviors such as smoking and alcohol consumption as well as inadequate folic acid intake are associated with suboptimal embryonic development.
What does this article add?
This community-based study shows the effects of comprehensive preconception care (PCC) consultations in the general population. Preconception care contributes to initiation of folic acid supplementation and cessation of binge drinking in women who intend to become pregnant. To verify self-reported outcomes, it includes biomarker data.
What are the implications for health promotion practice or research?
It warrants implementation of a comprehensive PCC program for the general population to improve maternal and perinatal health.
Supplemental Material
Supplemental Material, sj-docx-1-ahp-10.1177_0890117120927287 - Change in Lifestyle Behaviors After Preconception Care: A Prospective Cohort Study
Supplemental Material, sj-docx-1-ahp-10.1177_0890117120927287 for Change in Lifestyle Behaviors After Preconception Care: A Prospective Cohort Study by Meertien K. Sijpkens, Sabine F. van Voorst, Ageeth N. Rosman, Lieke C. de Jong-Potjer, Semiha Denktaş, Birgit C.P. Koch, Loes C.M. Bertens and Eric A.P. Steegers in American Journal of Health Promotion
Footnotes
Authors’ Note
The study has been approved by the Medical Ethical Committee of the Erasmus Medical Center of Rotterdam (MEC 2012-425). All participants signed for informed consent.
Acknowledgments
The authors thank all healthcare professionals that were involved in the Healthy Pregnancy 4 All–related PCC services, all participating laboratories (in particular M. de Waart of the Erasmus MC), and all women who participated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Dutch Ministry of Health, Welfare and Sport (grant number 318 804) and National Organization for Health Research and Development.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.